
Abstract
Introduction:
We present our initial experience with robot-assisted reconstructive surgeries with the Da Vinci Xi robotic system for benign ureteric pathologies.
Materials and methods:
This is a retrospective review of prospectively collected data of patients who underwent robot-assisted reconstructive procedures for benign diseases of the ureter at our department from April 2018 to November 2022. Demographic and perioperative details were recorded. Patients were followed up and surgical success was evaluated on the basis of symptomatic, functional, and radiological improvement.
Results:
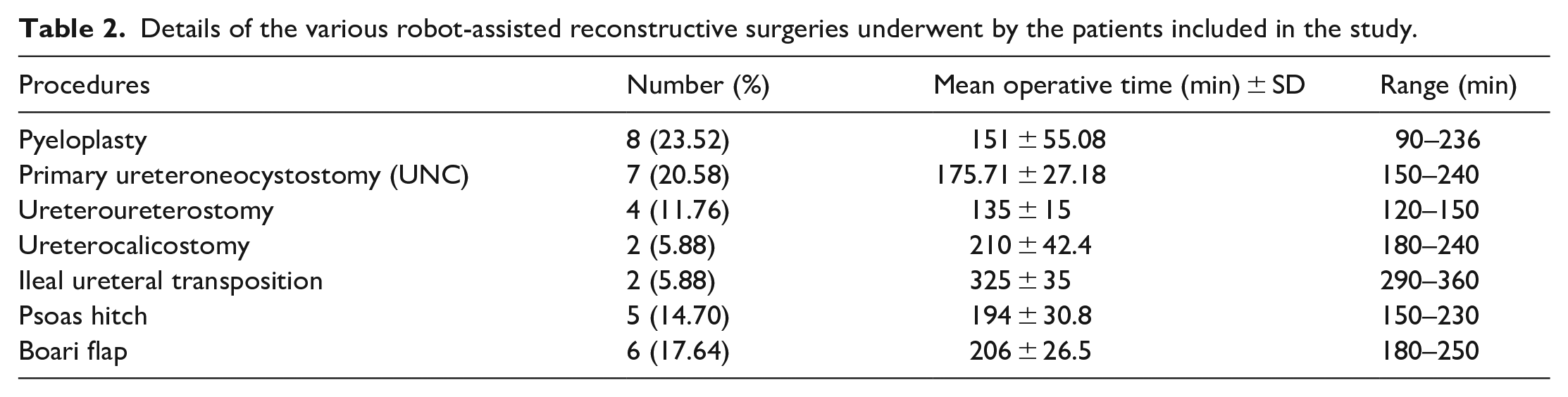
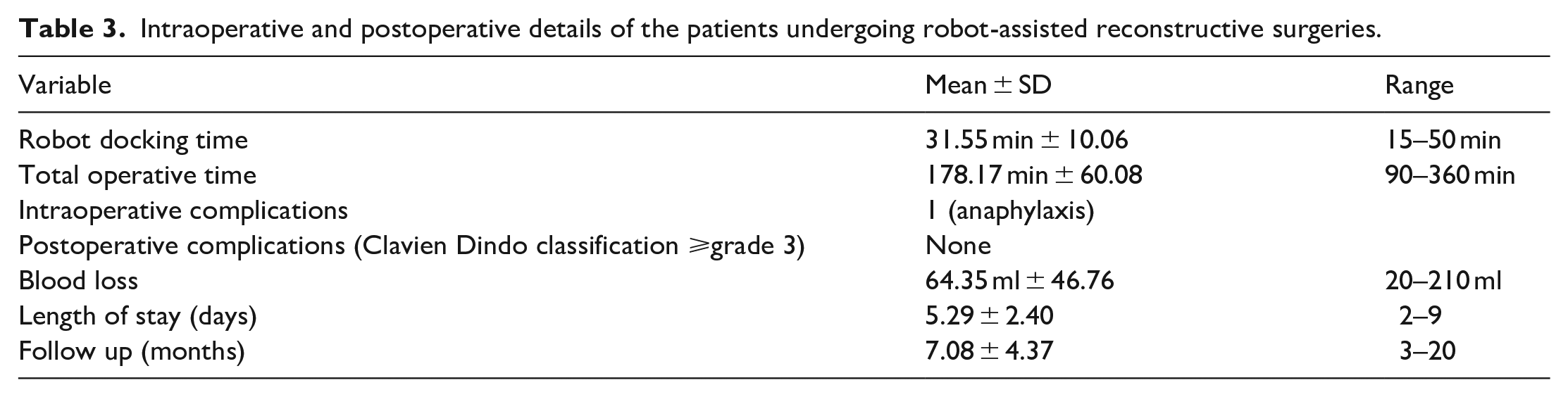
A total of 34 patients underwent robot-assisted reconstructions for benign ureteric pathologies by various techniques. Mean age, body mass index (BMI), hospital stay and follow-up duration were 36 years, 24.1 kg/m2, 5.29 days, and 7.08 months respectively. Procedures included pyeloplasty in eight, primary ureteroneocystostomy (UNC) in seven, Psoas hitch UNC in five, Boari flap UNC in six, Ureteroureterostomy in four, ureterocalicostomy in two and ileal ureteral transposition in two patients. Mean docking time, total operative time, and estimated blood loss were 31.5 min, 178 min, and 64.3 ml, respectively. All patients had radiologic or functional improvement on follow-up after 6 months.
Conclusion:
Robot-assisted reconstructive surgery for benign ureteric and bladder pathologies imparted excellent short-term outcomes without major complications with all the advantages of a minimally invasive approach.
Keywords
Introduction
The merits of robot-assisted laparoscopic surgeries over classical laparoscopic and open approaches are already well-established in adults as well as the pediatric population.1,2 Traditionally, the comparison between these three modalities has shown equivalence in long-term results and superiority of the robotic approach in the length of hospital stay and postoperative pain.3,4 Ureteric reconstructive surgeries are no exception to these. Moreover, the additional advantage offered by the robotic approach in ureteric surgeries is the better point of technique, where better access to the deep pelvis and dexterity of instruments facilitates precise mucosa-to-mucosa anastomosis with better preservation of vascularity, leading to reduced recurrence rates and ultimately better outcomes. In the ever-evolving line of surgical robots, the DaVinci Xi robotic system has many advantages over previous models.5,6 In addition to a laser-guided port positioning system and many new safety features, much of the Xi system’s kinematic structure has been redesigned. In comparison to the older Si system, the newer Xi features smaller, thinner robotic arms with redesigned joints that enable a greater range of motion, longer instrument shafts to give greater operative reach and all 8 mm ports including the camera port. With the added advantages of Xi robotic system over preceding models, the majority of procedures can be performed with a single docking. 7 We are presenting our initial single institution experience with Da Vinci Xi (Intuitive Surgical, Sunnyvale, CA) surgical system in performing robot-assisted reconstructive surgery of the ureter using different approaches, depending upon the pathology. We will discuss surgical indications, peri-operative and post-operative outcomes as well as some technical considerations regarding the surgeries performed.
Material and methods
This is a retrospective review of prospectively collected data of patients who underwent robot (Da Vinci Xi, Intuitive Surgical, USA) assisted reconstructive procedures for benign pathologies of the ureter in our department, from April 2018 to November 2022. We analyzed pre-operative and peri-operative data such as age, sex, BMI, clinical presentation, etiopathogenesis, American Society of Anaesthesiologists (ASA) score, side of ureteric pathology, estimated blood loss (EBL), surgical technique, robot docking time, total operative time, intraoperative complications, length of hospital stays (LOS), postoperative complications according to Clavien Dindo classification, and outcome. Preoperative evaluation included imaging in the form of intravenous urography (IVU), computed tomography urography (CTU), magnetic resonance (MR) urography, voiding cystourethrogram (VCUG) tailored according to pathology. Retrograde ureterogram (RGU), antegrade ureterogram (where percutaneous nephrostomy (PCN) was present) were also done to delineate ureteric and bladder anatomy. Whenever required we performed cystoscopy and ureteroscopy to further delineate anatomy. Diuretic renogram was performed in patients with suspected pelvi-ureteric junction (PUJ) obstruction and where renal unit was not visualized or showing very poor function. Sterile urine was confirmed before surgery. We included cases of pyeloplasty for secondary PUJ obstruction, ureterocalicostomy (UCS), ureteroureterostomy (UUS), ureteroneocystostomy (UNC), ileal ureteric transposition, psoas hitch and boari flap. Patients with a prior history of pyeloplasty were excluded from the analysis. Patients who had at least 3 months follow-up period were selected for this study. During the follow-up period, patients underwent renal function testing, urinalysis and renal ultrasound. A diuretic renogram was done in patients who underwent pyeloplasty and CTU was done in other patients post ureteric reconstruction to evaluate postoperative drainage and improvement. Surgical success was determined on the basis of clinical, functional and/or radiological improvement.
We present a brief description of each reconstructive procedure, the patient characteristics, the peri-operative data, 6-month postoperative complications and the results of follow-up.
Surgical techniques
Based on the pathology, definitive surgery was planned. Ureteroureterostomy (UUS) was used in patients with short-length mid-ureteric strictures. Primary ureteroneocystostomy (UNC) with or without Psoas hitch or Boari flap was done for lower ureteric pathologies depending upon the stricture length. In two patients with upper ureteric stricture and a non-dilated pelvis, ureterocalicostomy (UCS) was performed.
Patients were positioned according to pathology with proper strapping and padding of all pressure points. We used a Veress needle for pneumoperitoneum creation in all cases and surgeries were performed via a transperitoneal approach. Robotic ports were placed in a linear configuration positioned with minimum 6–8 cm spacing. For pyeloplasty and UCS, patients were placed in lateral decubitus position at 45°–60° without any table flexion to avoid tension over anastomosis and compression of the opposite kidney. Three 8 mm robotic ports were placed in a straight line over the midclavicular line at a distance of 8 cm each (Figure 1(a)). One 12 mm assistant port was placed in triangulation with the first and second robotic ports in the supraumbilical region. In ureteroureterostomy, patient positioning and port placement were similar to UCS except we used only three robotic arms instead of four. In ileal ureteric interposition, two assistant ports of 12 and 5 mm were placed medially between the first and second robotic ports and third and fourth ports respectively, and the rest of the port placement and patient positioning were the same as in pyeloplasty. In primary UNC and psoas hitch, the patients were put in a moderate to steep Trendelenburg position with legs spread at 50°–60° and slightly flexed at the knee. The robot was positioned at the foot of the table between the patient’s legs. All four, 8 mm robotic ports were placed in a linear configuration approximately 5–7 cm above the umbilicus with the fourth port placed opposite to the diseased ureter. An assistant port of 12 mm was placed in the flank area (Figure 1(c)). In Boari flap reconstruction, four robotic ports were placed in an oblique direction with an assistant port as shown in Figure 1(b).
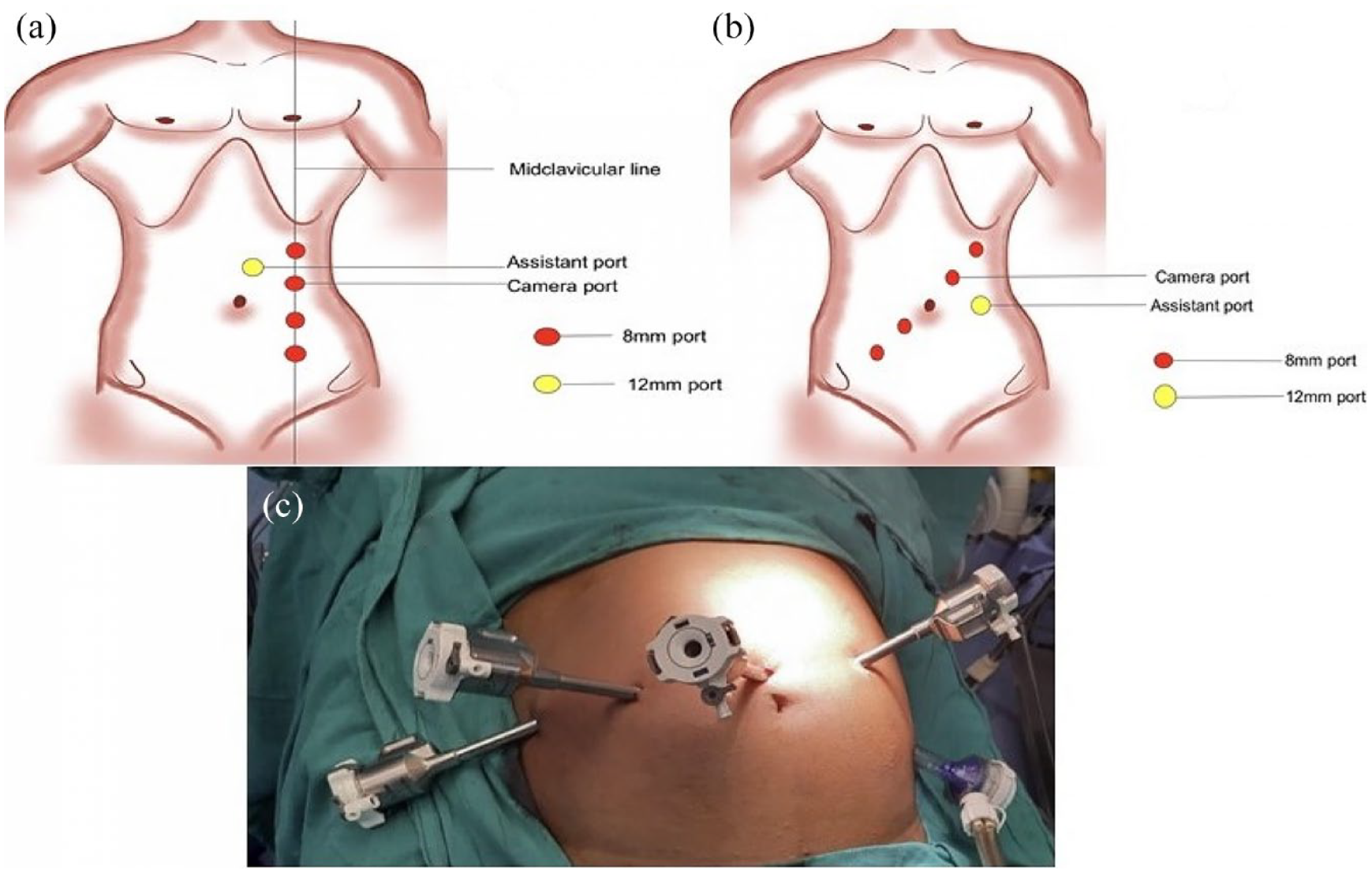
Port placement for robot-assisted procedures using Da Vinci Xi robotic system: (a) left pyeloplasty, ureterocalicostomy and ureteroureterostomy, (b) Boari flap reconstruction, and (c) ureteroneocystostomy and psoas hitch.
After port placement for the respective surgery, the robot was docked with instruments. For pyeloplasty, the colon was reflected at the line of Toldt. After dissecting the ureter and renal pelvis, the renal pelvis was transected at the level of the pelvi-ureteric junction. The ureter was spatulated and Anderson Hynes dismembered pyeloplasty was performed with Vicryl (Ethicon, Somerville, NJ) 4-0 round-bodied sutures over a Double J (DJ) stent. While performing UCS, the ureter was identified and traced proximally up to the strictured area, keeping the peri-adventitial tissue intact. The kidney was mobilized and the lower pole was accessed. Parenchyma over the lower pole was resected to access lower pole calyces. Then the ureter was ligated and transected below the stricture segment. Ureter was spatulated laterally and anastomosis was done with opened dilated lower pole calyx over a DJ stent. The renal capsule was then loosely approximated over the cut surface of the parenchyma followed by perinephric fat covering.
While performing a ureteroureterostomy, the ureter and gonadal vein were identified and dissected. Once identified, the stricture was directly transected. Scar tissue was then subsequently resected until a healthy tissue margin was identified with well-perfused, normal-appearing tissue. The distal ureter was spatulated laterally and the proximal ureter medially. These two ends were anastomosed in a tension-free manner.
In Primary UNC, the posterior peritoneum over ipsilateral iliac vessels was incised and the ureter was identified. Ureteric mobilization was done till the pathologic segment, preserving adventitia. The strictured part was dismembered up to the proximal healthy segment. The distal unhealthy part was clipped with Hem-o-lok® clip or ligated with a trans-fixation suture. At this point, dissection of the bladder is completed to allow for adequate mobilization of the bladder, which is imperative for a tension-free anastomosis. In six patients primary UNC was feasible, however, one patient required ureteric tapering as the ureter was hugely dilated.
For performing the psoas hitch, the dissection and transection of the ureter just above the strictured segment were done, the psoas tendon was located and the overlying tissue was cleared. Vicryl 3-0 suture was placed through the tendon in a longitudinal fashion and through the superior and ipsilateral wall of the bladder in a figure-of-eight fashion. Further bladder mobilization was achieved by freeing the bladder superiorly from the peritoneum. Periodically filling and emptying the bladder via a Foley catheter helped in determining whether or not sufficient mobilization had been achieved to reach the transected ureter. The proximal healthy part of the ureter was spatulated. Detrusorotomy was done using electrocautery on the partially filled bladder. A submucosal tunnel of adequate length was created by blunt and sharp dissection. The mucosa was opened at the distal end of the tunnel. The spatulated ureter was sutured to the bladder mucosa. The Detrusor muscle was buttressed over the ureter forming a submucosal tunnel using 3-0 Vicryl sutures by the Lich-Gregoir technique.
While performing a Boari flap, the ureter was mobilized and dismembered at the strictured part. The spatulation of the proximal healthy ureter was done and the urinary bladder was mobilized. In our series, as we could bridge the gap between the ureter and bladder, we did not ligate the contralateral superior vesical pedicle. A wide-based C-shaped flap of length sufficient to bridge the gap between the ureter and bladder was elevated from the anterior surface of the moderately filled bladder preserving the blood supply (Figure 2(a)). Marking of this flap was done before incising, taking care not to fall short and avoiding ischemia at the tip of the flap. Mobilized bladder flap was then anchored to the ipsilateral psoas muscle (Figure 2(b)). The spatulated ureter was anastomosed to the apex of the elevated bladder flap in a refluxing type anastomosis. A ureteric stent was placed, the remaining bladder flap was tubularized and the bladder defect was repaired with a 3-0 Vicryl suture (Figure 2(c)).

Intraoperative images showing Boari flap ureteroneocystostomy: (a) wide based C shaped flap marked, (b) spatulated ureter anastomosed to apex of the flap, and (c) flap tubularized over DJ stent.
In performing ileal ureteric transposition, the length of stricture and condition of the remnant ureter were noted after dissecting the ureter and lower pole of the kidney. The ileal segment corresponding to the length of the strictured part isolated 20 cm from the ileocolic junction was sutured to the proximal and distal ends of the ureter.
Postoperative care
The ureteric stent was removed within 3–8 weeks following surgery. Complications were recorded according to the Clavien-Dindo grading system. Follow-up scheduled at 3 months post-procedure was done with standard imaging techniques as per the procedure (CT urogram or renogram as described above). Subsequent follow-up protocol included three monthly visits for 1 year and annually, thereafter. Surgical success was defined by improvement in symptoms, improvement in renal function and resolution/improvement in the severity of hydronephrosis.
Results
A total of 34 patients were included in the study. Demographic parameters and etiologies of the patients are shown in Table 1. The most common symptom at presentation was flank pain. We had eight patients with secondary PUJO, which developed after percutaneous nephrolithotomy in all of them. All patients undergoing robot-assisted surgeries had successful outcomes, however, one patient developed anaphylactic shock after induction, so surgery was abandoned and carried out after proper precautions later. The mean robot docking time (±SD) was 31.55 (±10.06) min and the mean total operative time (±SD) was 178.17 (±60.08) min. The mean blood loss (±SD) was 64.35 (±46.76) ml, the mean hospital stay (±SD) was 5.29 (±2.40) days and the mean follow-up (±SD) was 7.08 (±4.37) months. Tables 2 and 3 summarize the details and outcomes of the patients who underwent various robot-assisted reconstructive procedures. Five patients developed urinary tract infection which was managed with antibiotics according to urine culture and sensitivity. One morbidly obese female (BMI – 44.4) who underwent left Boari flap reimplantation developed numbness in her left upper limb which required physiotherapy along with analgesics. No patient had a Clavien-Dindo grade 3 or higher complication. At a mean follow-up of 7.08 months, all patients were asymptomatic and doing well with stable renal function tests. All patients showed either stable or improving renal function on follow-up imaging.
Patient demographics and etiology of the patients included in the study.
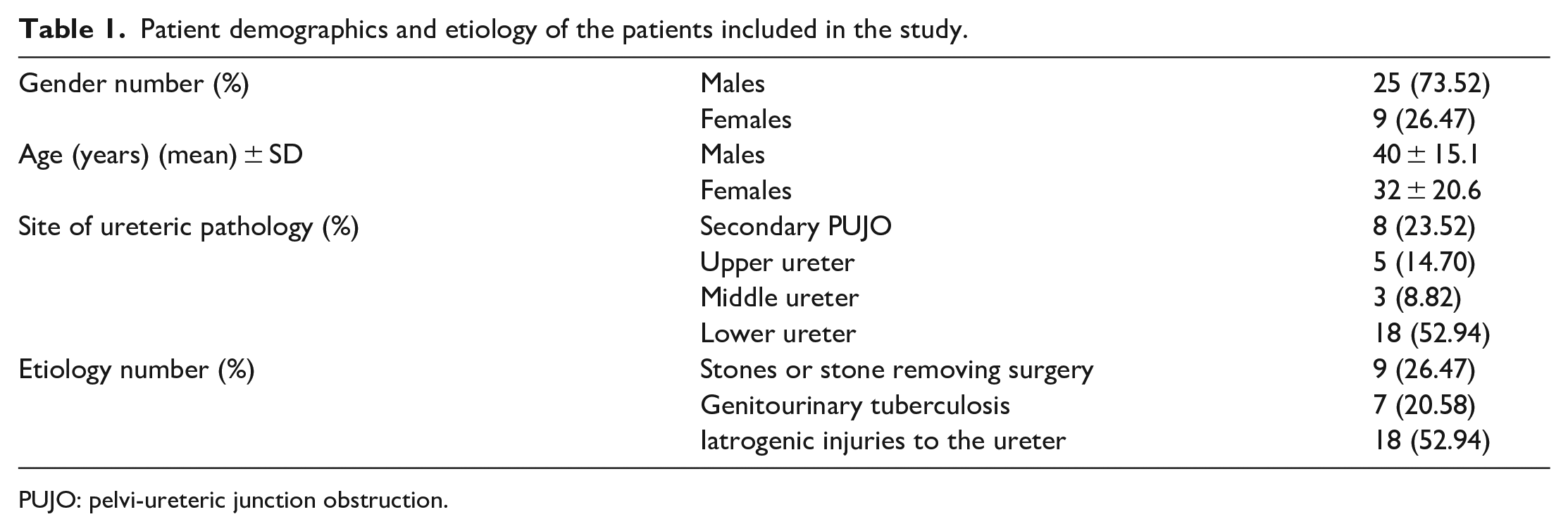
PUJO: pelvi-ureteric junction obstruction.
Details of the various robot-assisted reconstructive surgeries underwent by the patients included in the study.
Intraoperative and postoperative details of the patients undergoing robot-assisted reconstructive surgeries.
Discussion
Except for primary PUJO, most ureteric strictures are acquired and usually are iatrogenic. 8 Widespread use of upper urinary tract endoscopy has resulted in an increased incidence of ureteric strictures. The incidence of ureteric stricture formation related to upper tract endoscopy varies between 1% and 11%.9,10 In our cohort of patients also, the most common cause of stricture formation was the endoscopic treatment of stone disease. Clinical presentation of ureteric strictures varies widely ranging from mild hydroureteronephrosis (HDUN) to complete loss of renal function. Patients may remain asymptomatic or present with flank pain, sepsis, and recurrent pyelonephritis.
Indications for intervention include symptomatic ureteric stricture, the need to rule out malignancy and obstruction which may threaten a patient’s renal function. Depending upon the stricture location and length, various surgical options are present. 11 We evaluated all our patients thoroughly and the best option was chosen based on the site of injury. Two patients had long segment ureteric defects not amenable to other techniques, ultimately requiring ileal ureteral interposition.
With the relative immaturity in robotic ureteric reconstruction literature, limited number of studies exist that directly compare robot-assisted laparoscopy to open surgeries or pure laparoscopy.12–15 These studies reported no significant difference in operative time, but significantly lower hospital stay in robotic arm as compared to open and laparoscopic arm.12–15
The superiority of robot-assisted laparoscopic pyeloplasty (RALP) over conventional laparoscopic pyeloplasty (LP) in terms of less surgeon fatigue, shorter learning curve and the upper hand in dealing with redo and complex cases is already well known, though results are similar in both. 16 RALP offers better exposure to ureteropelvic junction and facilitates quicker endosuturing. 16 Here we are reporting data of eight patients with secondary PUJO undergoing RALP by Da Vinci Xi surgical system, without significant postoperative complications, despite being a relatively new center.
After Yohannes et al. published the first case of robot-assisted laparoscopic ureteric reimplantation for a left distal ureteric stricture, an increased number of cases were reported using robotic technology in direct ureter reimplantation or Boari flap, with or without psoas hitch.9,10,13,17 Baldie et al. in 2012 published results from 16 robotic surgeries for mid and distal ureteric strictures, and concluded that the results of the robotic management of mid and distal ureteric strictures are comparable to laparoscopic repair. 13
In cases with upper ureteric obstruction with a small intrarenal pelvis and dilated lower pole calyces, UCS is a good option and only a few cases have been described in the literature of robot-assisted UCS.18,19 In our experience, UCS was successful in both the patients, including a 9-year-old female. Casale et al. performed robotic ureterocalicostomy in nine pediatric patients with successful outcomes and concluded that it is a good option in patients with recurrent PUJO and in cases with difficult access to PUJ, such as in intrarenal pelvis. 18
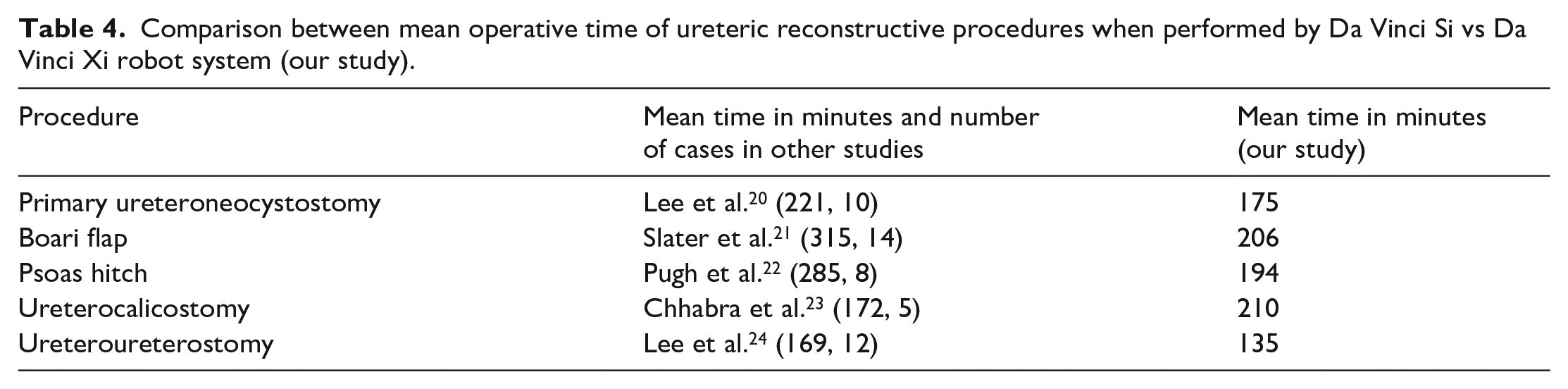
The mean operative timings of various surgeries of reconstructive urology in our study where Da Vinci Xi was used were comparable or lesser than the timings of similar surgeries done in other robotic surgical series where Da Vinci Si systems were used (Table 4).20–24 This can be attributed to following advantages of Da Vinci Xi over Da Vinci Si robotic system6,25:
Better vision due to new vision architecture with chip-at-the-tip technology, auto 3D calibration and auto white balance.
Faster docking with laser guided port placement and boom mounted robotic arms.
Reduced operative time due to torpedo-shaped robotic arms mounted on a rotation beam, providing better range of motion and less collision between arms.
Better efficiency in pelvic surgeries due to longer instruments.
Time-saving due to single docking and single robotic port placement while performing simultaneous upper and lower urinary tract surgeries.
Ours is a new center where the Xi robot was procured, and surgeries started. The existing surgeons were already experts in laparoscopy, which aided in the rapid adoption of the robotic system to our setup. 26 This, in turn, led to comparable operative and docking times, compared to established centers with good outcomes for patients undergoing robotic ureteral reconstructive surgeries.
Comparison between mean operative time of ureteric reconstructive procedures when performed by Da Vinci Si vs Da Vinci Xi robot system (our study).
Limitations of our study include its retrospective nature, small sample size and a mean follow-up duration and the BMI range may not be generalizable. Although our study concluded that robot assisted reconstructive surgery imparted excellent outcomes without major complications, it is not a comparative study with open or laparoscopic surgery, and therefore its advantages over the other approaches cannot be commented upon.
Conclusion
Robotic platforms have provided an impetus for innovation in surgical techniques while keeping in mind patient’s safety and postoperative outcomes. Our initial experience in aforementioned robot assisted surgeries with Da Vinci Xi system imparted excellent outcomes without major complications. For a surgeon without extensive laparoscopic experience, robots provide a comfortable ergonomic platform for working in the deep pelvis and is a great option for patients undergoing various urologic reconstructive procedures.
Footnotes
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by all the authors. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This is a retrospective observational study. The Institute Ethics Committee of AIIMS Jodhpur, India has approved the study.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent to publish
The authors affirm that all consents required for publishing this article have been taken.