
Abstract
Introduction:
Urogenital fistula is a physically, socially and psychologically devastating condition for the patient. In developed countries, these fistulae are typically related to gynecological surgery, pelvic pathology like malignancy or post radiation therapy. In contrast, classical teaching is that urogenital fistulae in the developing countries like India are usually associated with prolonged labor and obstetric complications. This retrospective study conducted at a tertiary care health Institute shows a paradigm shift in epidemiology, etiology and management of genitourinary fistulae in India in recent times.
Methods:
This retrospective study included patients undergoing surgical repair for various genitourinary fistulae at our institute from 2016 to 2022. Epidemiology, etiology, site, size and number of fistulae, clinical presentation, and management records of these patients were recorded and reviewed retrospectively.
Results:
In our study, the mean age of the patients was 38.4 ± 10.2 years. Vesicovaginal Fistula (VVF) was found to be most common fistula in the study population (87.5%) followed by vesicouterine (7.1%) and urethrovaginal fistula (5.4%). The causes of genitourinary fistula were iatrogenic (73.2%), carcinoma of cervix (16.1%), obstructed prolonged labor (7.1%), and genitourinary tuberculosis (3.57%). Among the 48 vesicovaginal fistulas that underwent surgery, 45.8% were treated using a transvaginal approach, 29.2% were managed through a laparoscopic transabdominal repair, and 25% were addressed using a robotic approach. Recurrence occurred in 7.1% of the operated patients.
Conclusion:
Enhanced healthcare services in the country have contributed to a decrease in the incidence of obstructed labor, subsequently reducing related injuries. Iatrogenic injuries resulting from gynecological surgeries and carcinoma cervix have given rise to more complex fistulas, necessitating the implementation of advanced treatment strategies.
Introduction
Genitourinary (GU) fistula refers to an abnormal communication between genital, and urinary tracts resulting in continuous incontinence or cyclical hematuria. Any part of the urinary system that is, ureter, bladder, urethra may communicate with any part of the genital system (uterus, vagina). Vesicovaginal fistula (VVF) is the most common genitourinary fistula 1 and this condition leads to lot of anxiety, and morbidity in afflicted women. VVF is the commonest type of genitourinary fistula which occurs following gynecological procedures (reported incidence: 0.8 per 1000 procedures). 2 In the developing countries, obstructed labor accounts for 97.0% ofVVF. 3
The reported occurrence of ureteral injuries following gynecological procedures ranges between 0.50%–14.0%. 4 The etiology and incidence of GU fistula varies geographically. In developed countries, these fistulae are typically related to gynecological surgery, pelvic pathology for example, malignancies or radiation therapy. 5 In contrast, classical teaching is that urogenital fistulae in the developing countries like India were usually associated with childbirth. 6 Recently, in our clinical practice, we have observed a paradigm shift in epidemiology, etiology and management of genitourinary fistulae. With improvement in obstetric care in India there has been a decrease in incidence of obstructed labor and associated genitourinary fistulae. Also, increase in hysterectomies and other pelvic surgeries have changed the epidemiology of GU fistula in our country. Other notable causes, leading to increasing incidence of GU fistula include radiation-induced and advanced pelvic malignancies such as bladder, rectal, and cervical tumors and their treatment.7,8 In underdeveloped nations, prolonged obstructed labor constitutes the most common etiology of Genitourinary fistula (= 90%), especially in Sub-Saharan African countries.9,10
Treatment approaches have also been showing changing trends including conservative management for small fistulae to surgical ones for large and complex fistulae. There is currently no gold standard technique for the management of genitourinary fistula. Traditionally fistula repair was carried out by either transabdominal or transvaginal approach with success rates ranging from 50.0% to 100.0%. 11 In the past, open transabdominal trans vesical was the main approach because of the familiarity of urologists to anatomy but was associated with significant morbidity to the patient. Nowadays, more and more of these fistulae are being operated with minimally invasive approaches like laparoscopic, robotics and transvaginal route.
Although advances have occurred in the understanding of etiopathogenesis, diagnosis, and management of GU fistula, it still poses challenges to the treating surgeon because of the controversies regarding the optimum time of repair and the ideal surgical approach. This retrospective study conducted at a tertiary care health institute shows a paradigm shift in epidemiology, etiology and management of genitourinary fistulae in India in recent times.
Material and methods
This study includes all female patients undergoing Genitourinary fistula repair at our Institute from 2016 to 2022. After obtaining institutional ethical clearance (Certificate clearance number- AIIMS/IEC/2020/3105), patients with written informed consent were enrolled for the study. Epidemiology, etiology, site, size and number of fistulae, clinical presentation, diagnostic modalities, and management records of these patients were recorded and reviewed retrospectively.
All the patients were evaluated and details on demography, etiology, history, clinical examination, baseline investigation, ultrasonography abdomen, computed tomography (CT) urography, treatment and outcomes were recorded. Cystoscopy was done to know the site, size and number of fistulae, and the condition of surrounding mucosa. Vaginoscopy was done to know about vaginal capacity and mucosal integrity.
The route and type of surgical repairs were individualized according to the classification of fistulae and accessibility of the fistula tract. All the patients were followed up at least for a period of 6 months. The cure rate per repair and overall success rate of various surgical approaches were analyzed. VVF’s were approached either by Transabdominal or Transvaginal approach.
Transabdominal repair was done for complex and supra-trigonal fistulas. Transabdominal approach included either laparoscopic or robotic repair. Robotic repair was preferred because of the complexity of the fistulae, which included recurrent, supra-trigonal, multiple fistulae. Surgeons’ preference was also one of the contributing factors for determining the use of robot for VVF Repair.
After repair, the bladder was drained by a suprapubic and a urethral catheter, along with a drain in the peri-vesical space for 3–4 days. Catheters were removed after 3 weeks. The transvaginal route was preferred for simple and small trigonal fistulas. Martius flap was used as interposing tissue.
Ureterovaginal fistulae were repaired by ureteroneocystostomy (With or without Psoas hitch) using Modified Lich-Grégoire technique over a double J (DJ) stent. Urethrovaginal fistula were repaired transvaginally (with Martius flap/ layered closure). Vesicouterine fistula was repaired by transabdominal hysterectomy and layered closure of bladder with omentum as interposing tissue followed by continuous bladder drainage for 3 weeks.
Statistical analysis
Microsoft Excel was used in creating the database and producing graphs, while the data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 23 for Windows. Mean and standard deviation (SD) were used to describe quantitative data meeting normal distribution. Continuous two independent groups were compared by parametric independent Student’s t test, this was used. Discrete (categorical) groups were compared by chi-square (χ2) test was used. A p value less than 0.05 was considered statistically significant.
Results
A total of 56 patients underwent genitourinary fistula repair in our institute and the mean age of patients was 38.4 ± 10.2 years. Comorbidities included diabetes (3.6%) and hypertension (19.6%). Recurrent fistulas were observed in 12.5% of cases and 20 (35.7%) patients had complex fistula that included fistula greater than 4 cm, recurrent fistula, fistula involving urethra or due to genitourinary tuberculosis. (Table 1)
Patients Characteristics.
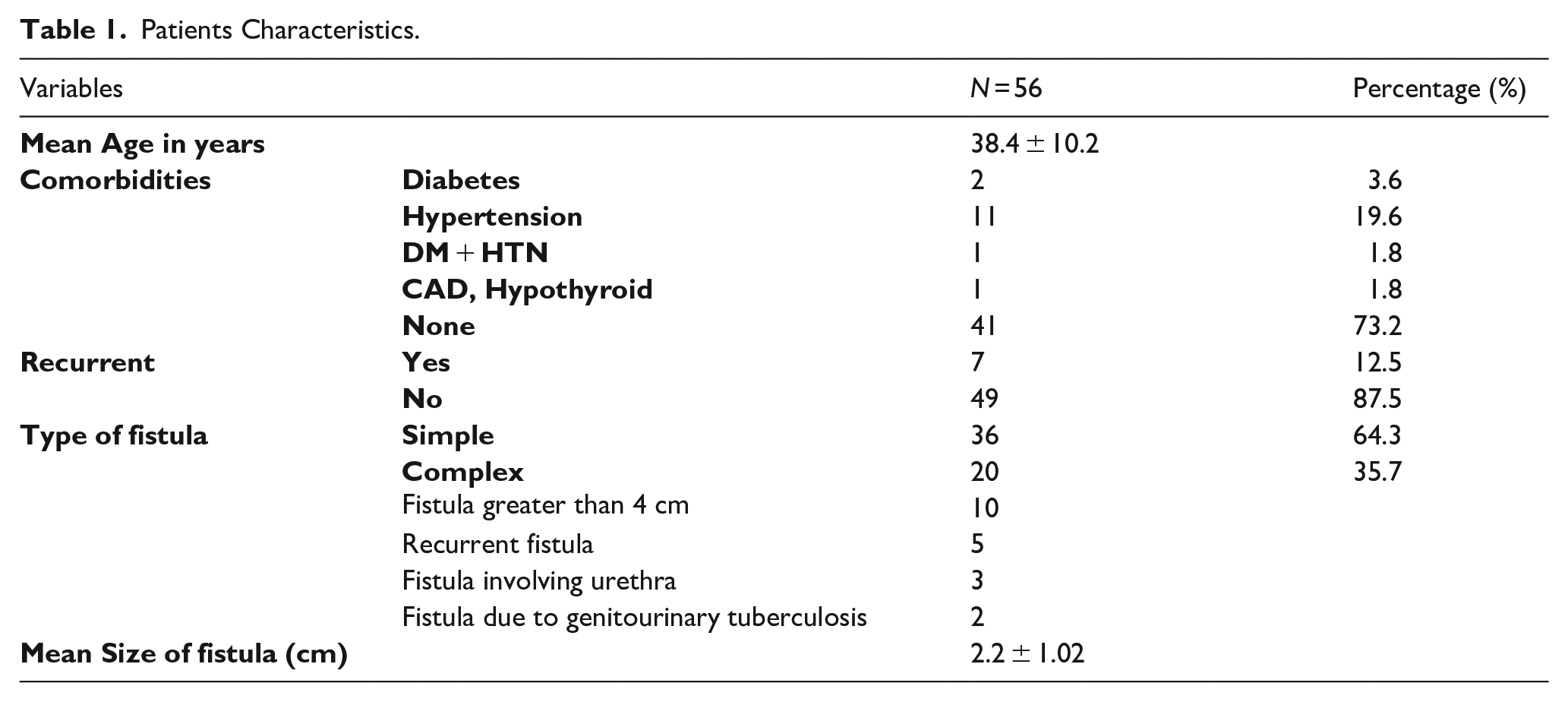
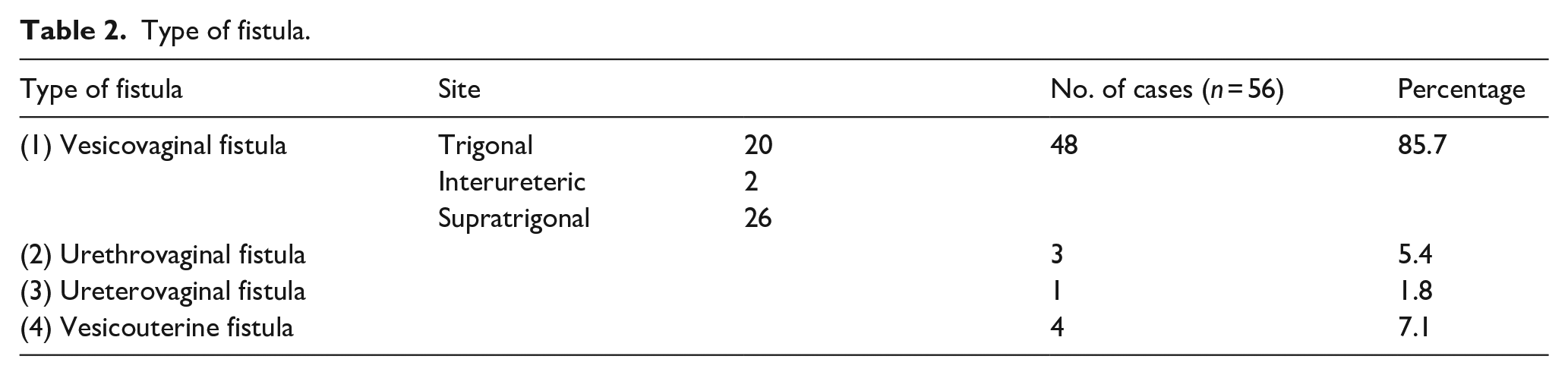
Table 2 shows that VVF were the most prevalent type (85.7%) of fistulas, with trigonal being the most common subtype. This was followed by vesicouterine (7.1%) and urethrovaginal fistula (5.4%). As shown in Table 3, etiology of GU fistula mostly constituted iatrogenic injury due to gynecological surgery such as abdominal hysterectomy (60.7%) and cesarean section (12.5%). Carcinoma of cervix was the next common etiology (16.1%).
Type of fistula.
Causes of genitourinary fistula.
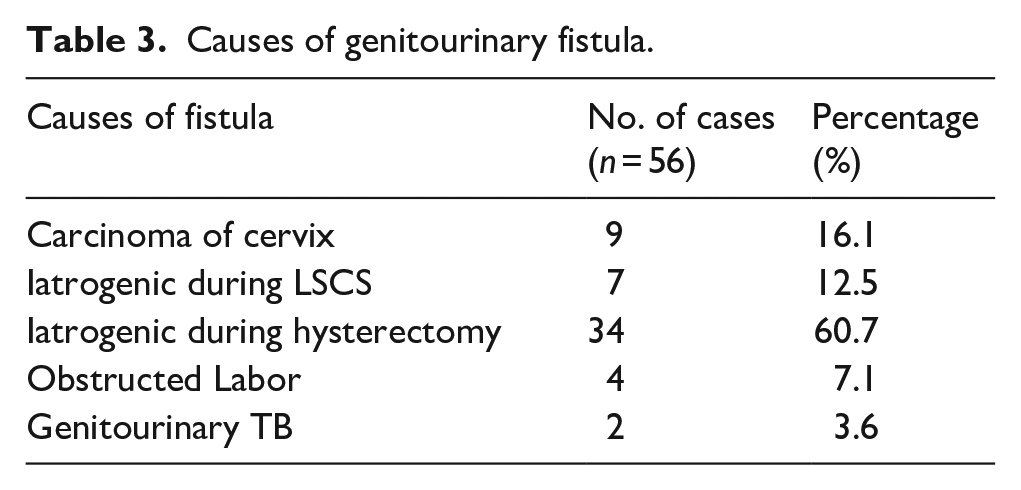
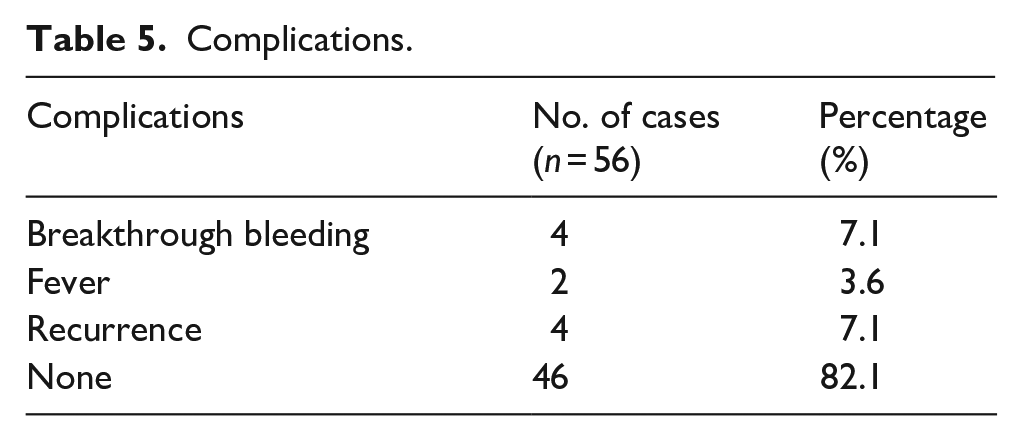
Table 4 shows that among the 48 VVF patients who were operated, transvaginal repair was done in 22 and transabdominal approach was used in 26 patients. Among transabdominally operated VVF repairs, 12 patients had robotic repair and 14 underwent laparoscopic repair. All recurrent fistulae were operated with robotic surgery only. Overall complications included breakthrough bleeding (7.1%), fever (3.6%), and recurrence (7.1%). 82.1% experienced no complications as shown in Table 5.
Management of fistula.

Complications.
Among our operated patients, those patients who experienced a recurrence underwent repeat VVF repair, with three of them being done with transabdominal approach, while one patient with concurrent cervical cancer received transvaginal repair. Out of 4 cases that recurred, two patients had diabetes and a BMI > 30, one had previously failed fistula repair, and the remaining one case had history of radiotherapy for carcinoma cervix.
Discussion
Genitourinary fistulae represent a significant maternal morbidity from obstructed labor in developing nations. The socioeconomic impact, along with the recognized morbidity of these fistulae, has prompted campaigns across developing countries to increase awareness and allocate resources for preventive and treatment services. In industrialized nations, obstetric causes of genitourinary fistulae have been virtually eliminated and are resultant from complications of pelvic surgery, radiation, trauma or malignant disease. 12
Our findings were in accordance with
In the past, obstetric complications like prolonged obstructed labor, coupled with a lack of medical attention, were more common causes of GU fistula, especiallyVVF.14,15 In developed countries, with much better obstetric facilities, the causative factors of GU Fistula are mostly associated with gynecologic and pelvic surgery, especially hysterectomy, occurring in 1 in 1800 hysterectomies.14,16 Similar results were reported by another study by
In our study we found that only 7.1% patients had obstructed labor as the cause of GU fistula. However, iatrogenic injury due to gynecological surgery such as hysterectomy (60.7%) and cesarean section (12.5%) were found to be the most common causes. Carcinoma of cervix was the next common etiology (16.1%). Another recent study of Pakistan by
In our study we found that 7.1% patients had recurrence post VVF surgery. Two patients had diabetes and obesity. Poor glycemic control may be the potential reason behind poor healing of the repair and leading to give way of sutures and hence recurrence. In one of the recurrent cases, radiotherapy was given for carcinoma cervix. Radiotherapy causes fibrosis of the vaginal tissue hence making suturing difficult. Remaining patient was a recurrent case with fistula size more than 2 cm and was operated by robotic transabdominal approach. These complex recurrent fistulas pose a great challenge to the operating surgeon. Increased fibrosis, dense adhesions and complex anatomy make suturing difficult and subsequently increase the chances of recurrence. There exist substantial evidence demonstrating that obesity is associated with a number of post operative complications. Specifically in relation to the wound healing, explanations include inherent anatomic features of adipose tissue, vascular insufficiencies, cellular and composition modification, oxidative stress, alterations in immune mediators and nutritional deficiencies. 19 These factors likely played a significant role in the unsuccessful repair observed in our study.
According to
Conclusion
Genitourinary fistulas are a debilitating problem in females but a comprehensive approach regarding diagnosis and treatment can cure these patients. Enhanced healthcare services in the country have contributed to a decrease in the incidence of obstructed labor, subsequently reducing related injuries. Iatrogenic injuries resulting from gynecological surgeries and carcinoma cervix have given rise to more complex fistulas, necessitating the implementation of advanced treatment strategies.
Footnotes
Contribution details
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.