
Abstract
Although BCG use as an anticancer drug was nearly abandoned due to the poor results in most tumors, in 1976 Morales reported a relevant reduction in recurrence with intravesical BCG in few patients affected by NMIBC. Since then BCG was globally accepted as an empirical and effective therapy in treating Tis and preventing recurrence of intermediate and high risk NMIBC. Forty-eight years after Morales’ report, although some open questions remain object of debate, we have been able to find answers to many doubts improving BCG activity and toxicity. We better select patients undergoing BCG and many trials have indicated the best dosage and schedule. Moreover, we are able to better identify the patient unresponsive to BCG who might benefit of a timely radical cystectomy. We are also aware of the difficulties and toxicities that can be encountered with BCG use in every-day clinical practice. Research is ongoing to obtain genetically modified BCG to increase its efficacy and reduce toxicity. Moreover, the combination of BCG with other immunotherapeutic drugs given intravesically or systemically, first immune checkpoint inhibitors, is under study to obtain a response in patients unresponsive or intolerant to BCG. Almost 50 years after Morales publication, intravesical BCG remains an inalienable tool against NMIBC
Introduction
The story
Bacillus Calmette Guerin (BCG) vaccine was used for the first time in 1921 to prevent tuberculosis. In 1929, Pearl, 1 detecting at autopsy a lower incidence of cancer in patients affected by tuberculosis supported that it could induced immunity against cancer. In 1924, Lewis and Loomis 2 demonstrated an immune response with high antibody production in guinea pigs receiving intraperitoneally bovine tubercle bacillus.
In the following years, BCG antitumor activity was investigated in several tumors as melanoma, leukemia, colon, lung and ovarian cancer. Nevertheless, the promising results obtained in animal models and in phase I-II clinical studies were not confirmed by large randomized study and BCG use as an anticancer drug was nearly abandoned. 3 In 1976, Morales et al. 4 reported in nine patients affected by recurrent NMIBC a relevant reduction in recurrence with the use of intravesical BCG. The Armand Frappier strain supplied in 6-vials package was used and the AA empirically decided to give six instillations with a weekly schedule due to outpatients office organization. Each instillation used one vial of 120 mg containing 8 × 108 CFU. At that time BCG was also administered percutaneously on the idea it could enhance immunoreactivity. Two subsequent randomized controlled trials confirmed the superiority of BCG versus TUR alone in terms of recurrence rate.5,6 Since then, BCG became a globally accepted effective treatment in preventing recurrence of NMIBC. In “80s, several multicenter phase II and III trials with different schedules, dose and routes of administration were performed. The higher efficacy of intravesical BCG given according to Morales” report was confirmed. The oral administration of BCG, after the preliminary promising results, was not anymore used.7,8 The intradermal concurrent sensitization was abandoned since no benefit in comparison with intravesical BCG alone emerged in randomized trials.
Morales again, in 1980 9 reported the anticancer activity of BCG in 7 patients affected by vesical carcinoma in situ (Tis). The ablative, and not only prophylactic, efficacy of BCG against bladder cancer was later confirmed by several controlled studies. 10 At that time the mechanisms of action of BCG were unknown. . . . .
Mechanism of action of BCG
The mechanism of action of intravesical BCG is not completely understood. Ratliff et al. 11 in 1987 demonstrated that an intact immune system is necessary for the antitumor action of BCG, since athymic mice were unable to develop an antitumor response. Jackson and James in 1994, reported that the immune response consisted of an inflammatory infiltrate and the secretion of cytokines. Tumor cell apotosis was induced by CD8 T cells through the recognition of intracellular adhesion molecule (ICAM) and major histocompatibility complex (MHC) II. The CD4 T cells secreted cytokines leading to the maturation of cytotoxic T cells or more specific activated killer cells (BAK). The BAK would be capable of differentiating between normal and tumor cells. Only live BCG organisms can induce BAK cell activity. Thus, attenuated BCG is necessary to generate an increased cellular expression of ICAM 1 and MHC II, involved in antigen presentation and lymphocytes killing activity. Moreover, some studies suggested that BCG might also affect the tumor growth rate. Probably the two mechanisms are synergic to obtain a complete BCG clinical efficacy. 12 BCG has been recently found to increase the expression of PD-L1 on tumor cell surface, providing a possible new sight on BCG activity. 13
Back to the present
After 48 years since the report of Morales et al., 4 although some questions remain object of debate, we have been able to find an answer to many of them and to better manage BCG activity and toxicity.
Which are the main questions on BCG in clinical practice when dealing with an intermediate or high risk NMIB? Probably, the following questions and doubts are the first arising in our mind: Can we correctly select patients to be treated with BCG? Are we able to predict BCG response? Do we use the correct dose and schedule? Is BCG surely superior to intravesical chemotherapy? Does BCG prevent progression and improve survival ? Are all BCG strains equal? When should we consider a patient unresponsive to BCG? How to increase BCG efficacy? Any benefit in combining BCG with other agents? How does BCG perform in real world practice? Can we prevent or reduce BCG toxicity? What beyond BCG?
In this short review we will try to travel through the topics that have been the target of so many papers and scientific meetings over the last 50 years.
Can we correctly select patients to be treated with BCG? Are we able to predict BCG response?
Main questions dealing with BCG are: are we able to select high-risk patients who might benefit from BCG treatment? Are we able to predict BCG response since we are aware that delaying radical surgery can worsen patients’ survival?
In the past two decades many models has been introduced to stratify the risk of recurrence and progression for NMI bladder cancer patients. We can include the European Organisation for Research and Treatment of Cancer (EORTC) risk calculator 14 and the Club Urologico Espanol de Tratamiento Oncologico (CUETO) risk classification system 15 as the most used, although many other models have been proposed.16,17
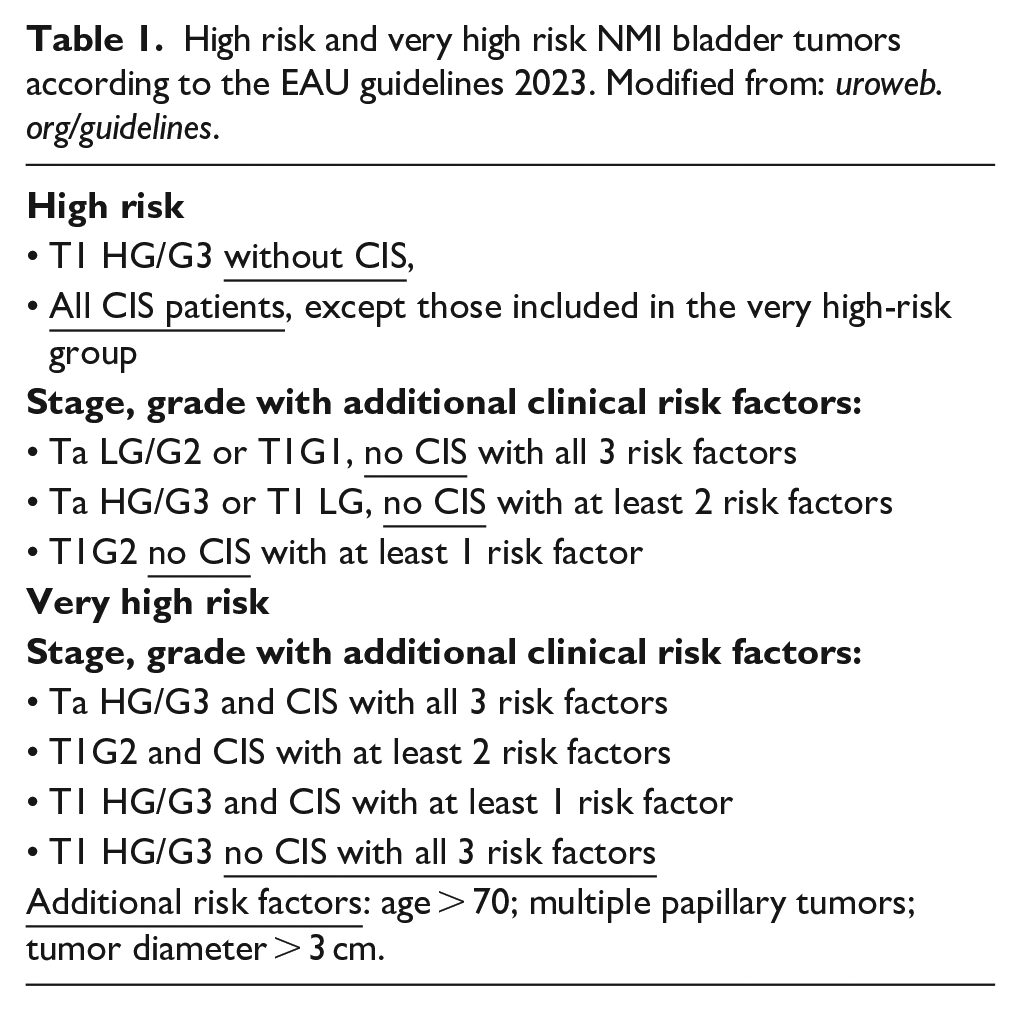
Up-today, pathological and molecular markers have failed in predicting BCG response. However, a category of “very high-risk” patients has been identified according to clinical and pathological factors as concomitant Tis, multiple and/or greater than 3 cm lesions, age ⩾ 70 years. The first indication for this category is not BCG but radical cystectomy and full-dose BCG with maintenance for 1–3 years should be offered only to those patients refusing or unfit for radical surgery 18 (Table 1). We must be aware of these recommendations and we should dedicate a sufficient time of our daily activity to adequately inform the patient, although it is not always easy in clinical practice.
High risk and very high risk NMI bladder tumors according to the EAU guidelines 2023. Modified from: uroweb.org/guidelines.
Do we adopt the right schedule and the correct dose?
In other words, can we reduce doses and instillation number? Can we avoid maintenance or reduce it? Its monthly maintenance of similar efficacy when compared to the Southwest Oncology Group (SWOG) schedule? Can we reduce BCG dosage to lower toxicity?
The first randomized trials failed in demonstrating the increase of prophylactic efficacy of maintenance schedule when compared to induction alone. This was probably due to the low statistical power and poor design.19,20 In 2001 the results of a SWOG randomized controlled trial showing the superiority of maintenance versus induction alone were published. The maintenance schedule consisted of 3 weekly instillations at 3 and 6 months, then every 6 months up to 3 years. This was the first trial to state the need of maintenance in intravesical immunotherapy 21 The recurrence free survival increased from 36 to 77 months. Conversely, it must be mentioned that only 16% of the patients completed the 3-year maintenance schedule. These results were confirmed 11 years after by Hinotsu et al. 22 in a trial comparing epirubicin induction, BCG induction and BCG induction plus maintenance. Not only BCG induction resulted more effective than chemotherapy, but also BCG maintenance resulted clearly superior to induction alone. In 2004, Böhle and Bock 23 presented a metanalysis confirming with high statistical significance the benefit of maintenance in RFS (p < 0.0001). Malmström et al. 24 in 2009 published an individual patient data meta-analysis of the long-term outcome of randomized studies comparing intravesical mitomycin C versus BCG for MIBC. The study including 2820 patients showed that MMC induction plus maintenance was more effective than BCG induction alone and that BCG induction plus maintenance was more effective than both regimens reducing recurrence by 32% compared to MMC (p = 0.0001).
On the other hand, a CUETO multicenter randomized study did not find any difference in terms of recurrence and progression between BCG induction alone and maintenance with single full-dose BCG instillation given every 3 months for 3 years. 25 This maintenance schedule, however, was different from that adopted in the SWOG study. Although the latter maintenance protocol is considered the standard, the maintenance with monthly instillations is also widely used. Evidence comparing the two maintenance protocols is limited. Recently, Nurminen et al. 26 compared the two maintenance schedules in 723 patients, of whom 545 (75%) and 178 (25%) received maintenance according to the monthly and SWOG protocols, respectively. No significant statistical difference emerged between the two groups in terms of 5-years recurrence-free survival rates (65% vs 71%, p = 0.370), and of 5-yr progression-free survival rates (89% vs 91%, p = 0.240), respectively. Thus, according to this study monthly maintenance seems a comparable alternative to the SWOG protocol.
A recent international randomized trial (Nimbus) 27 compared the 1-year SWOG schedule with a reduced induction (one instillation every other week for 6 weeks) and a reduced maintenance schedule (one instillation at week 1 and 3, at 3, 6, and 12 months), in other words 15 versus 9 cycles. The trial was interrupted due to a significant increase of the recurrence rate at 1-year in the reduced schedule arm (27% vs 12%).
If a complete response is not achieved after the first induction cycle can obtain it after a second 6-week cycle in up to 30% of patients. 28 However, it is important to consider that patients failing more than two courses of BCG have a 50% risk of metastatic bladder cancer. 29
In meta-analysis published in 2022, 30 low-dose BCG revealed a lower efficacy in preventing recurrence when compared to the standard dose, without any significant difference in progression, cancer-specific survival and overall survival. Low-dose BCG showed a better outcome in terms of adverse effects and withdrawal rates. A further meta-analysis in 2023 confirmed that standard dose of BCG has a higher oncological activity in intermediate and high-risk NMIBC patients. 31 Nevertheless, lower dose BCG schedule can be adopted in patients showing toxicity at standard dose or in case of BCG shortage.
Is BCG superior to intravesical chemotherapy?
BCG resulted to be superior to chemotherapy, including Mitomycin C, Doxorubicin and Epirubicin, in preventing recurrence and progression of Tis and intermediate-high risk NMIBC in several randomized trials and meta-analysis if maintenance regimen is adopted. Intravesical chemotherapy significantly reduces recurrence, but not progression.32–34 A Cochrane Systematic review published in 2020 and including 12 randomized controlled studies comparing BCG versus MMC in almost 3000 patients with intermediate and high-risk NMIBC suggested that BCG, compared to MMC, reduces the risk of recurrence over time but may increases the risk of serious adverse events. In this review both BCG and MMC showed no influence progression free survival and overall survival. 35
Does BCG prevent progression and improve survival?
A meta-analysis on nine randomized studies comparing BCG and MMC 23 showed that progression was significantly reduced only in studies adopting BCG maintenance. Also the above cited individual patients data meta-analysis by Malmström et al. 24 found that BCG with maintenance but not BCG induction alone could reduce progression compared with MMC. The EORTC trial 30911 comparing epirubicin and BCG, both with maintenance, at a follow-up of more than 9 years demonstrated that BCG significantly improved recurrence-free-survival (p < 0.0001), metastatic progression (p = 0.046), specific and overall survival (p = 0.023). 33 Spencer et al. 36 in a retrospective study on almost 24,000 patients showed that BCG reduced mortality with a 13% benefit in survival at 10 years. Progression and survival benefit of BCG were confirmed by a similar, even if smaller, study. 37
Are all BCG strains equal?
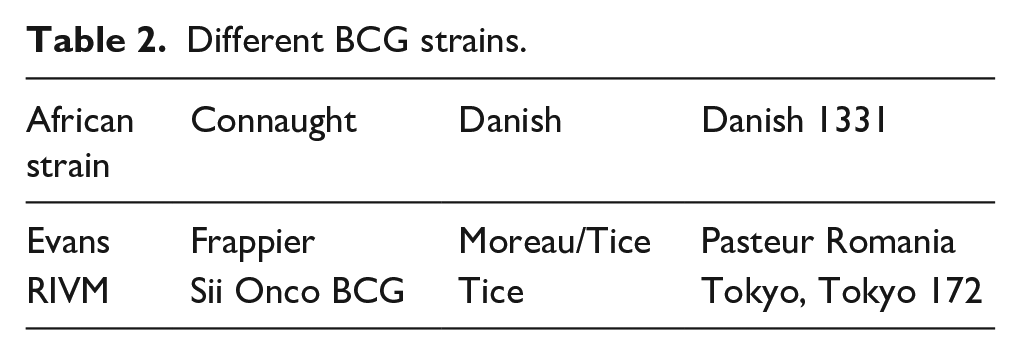
Genetic differences classify BCG strains into different substrains (Table 2). The large variability in BCG strain genetic profiling is conferred by serial laboratories passages. The BCG strain used by Morales came from the Institute Armand Frappier in Montreal. The BCG-Connaught strain derived from this strain although it is not anymore produced. Other commonly used strains are the “Tice strain” and the “RIVM strain.” Uncertainty exists in the literature whether the various strains of BCG have identical immunotherapeutic efficacy and identical clinical effectiveness. This data might represent a bias when comparing clinical studies adopting different strains of BCG. The interaction between genetic differences and immuno-reactivity for clinical outcomes was tested only by few small studies. Higher levels of IL-6 and IL-8 have been detected with BCG-Connaught and BCG-Russia, probably inducing a more robust immune response. 38 Birkhaeuser et al. 39 showed a statistically significant advantage in 5-year recurrence free survival in favor of Connaught compared to Onco-Tice. Witjes et al., 40 found a significantly longer time to first recurrence on Connaught as compared with Tice in patients undergoing an induction-only schedule. On the opposite when the sub-group of patients undergoing maintenance was analyzed, Tice revealed a long-acting efficacy contrasting a decrease in the immune response over time demonstrated by BCG Connaught. In a meta-analysis including 62 studies, 15,412 patients and 10 different BCG strains no single strain resulted superior to another in terms of recurrence free survival and recurrence rate. Although the study do not analyzed progression and cancer-specific survival due to the low numbers, it highlighted potential benefits from the genetically different BCG RIVM, Tice and Tokyo 172, supporting the adoption of these strains in BCG trials. 41
Different BCG strains.
When should we consider a patient unresponsive to BCG?
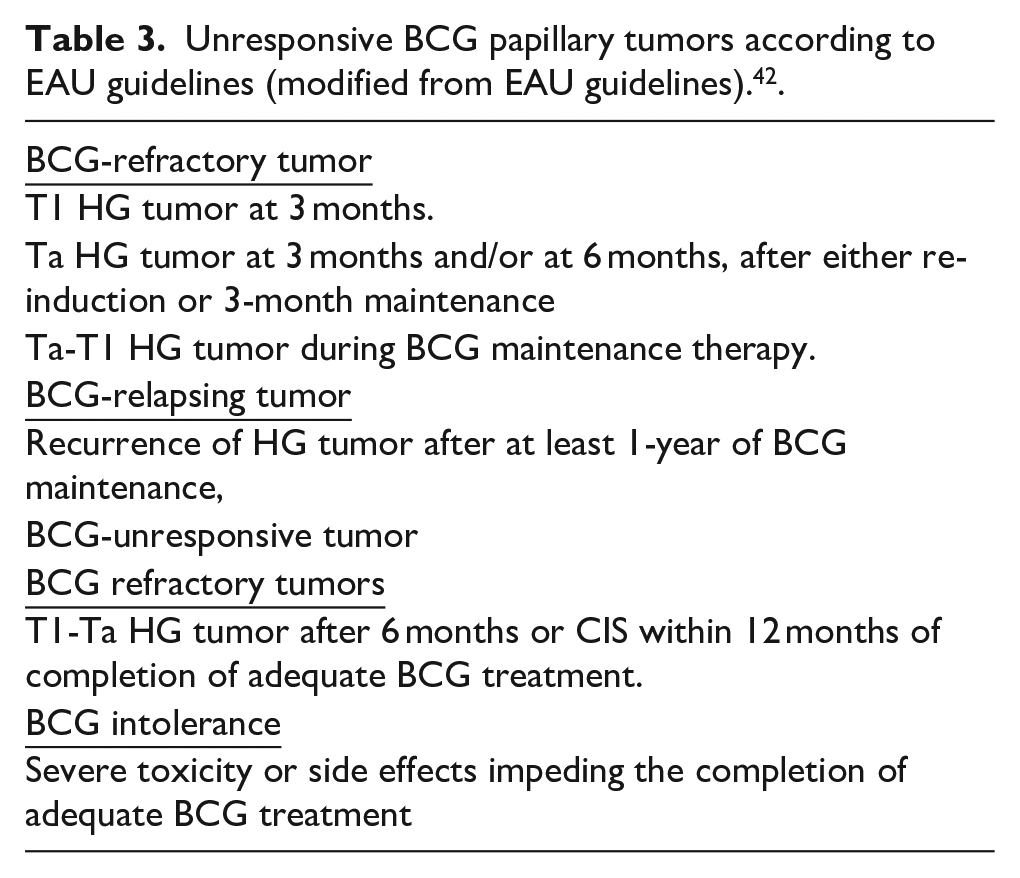
The complete response to BCG induction could be a delayed one. In a SWOG study on the role of BCG maintenance, 24% of the patients with a persistent CIS at 3 months after induction showed a complete response at 6 months without further treatment. 21 An adequate BCG treatment should include at least 5 doses of the induction course plus at least 2 out of 6 doses of a second induction course or 2 out of 3 doses of maintenance therapy. Patients who have not received an adequate BCG treatment should be not necessarily classified as BCG unresponsive. It is the same for patients who have responded and then recurred more than a year later. Moreover, low-grade tumors occurring during or after BCG treatment are not considered a BCG failure. BCG refractory CIS is defined as failure to achieve complete response following adequate induction. BCG relapse is defined as recurrent malignancy within 1 year of adequate BCG.
The different categories of BCG-unresponsive papillary tumors according to EAU guidelines 42 are reported in Table 3.
Unresponsive BCG papillary tumors according to EAU guidelines (modified from EAU guidelines). 42 .
How to increase BCG efficacy? Any benefit in combining BCG with other agents?
The EORTC-GU (European Organization for Research and Treatment of Cancer -Urological Group) in 1996, obtained a complete response rate of 50% in a marker lesion study adopting three weekly instillations of MMC followed by six weekly instillations of BCG. 43 The response rate was not higher than that expected with BCG alone a subsequent meta-analysis in 2012 concluded that adding sequential chemotherapy to BCG with maintenance had no benefit on recurrence or progression. 44 A later randomized phase 2 trial on TIS in which three weekly instillations of MMC were followed by six weekly instillations of BCG and maintenance of one MMC instillation and two BCG instillations according to SWOG schedule showed no benefit in terms of efficacy with the combination compared to the BCG arm. 45
In spite of sporadic studies showing some advantages of a sequential combination of chemotherapy and BCG versus BCG alone, nowadays no guideline advocates its adoption. 46 A Cochrane systematic review in 2017 analyzed five studies, including 1231 patients randomized between intravesical BCG with IFN-α (sequential or alternating combination) versus intravesical BCG alone. The analysis found very low-quality evidence showing no clear difference in recurrence and progression between the two groups. When an alternating schedule, and not a sequential, was adopted, the combination showed a higher probability of recurrence compared with BCG alone. Moreover, a subgroup analysis on recurrence in relation to IFN-α dose showed an advantage from a lower-dose IFN-α (6–10 MU) compared with a higher dose (50 MU). 47
How does BCG perform in real world practice?
BCG treatment efficacy and tolerability in NMIBC patients differ in the real world, with better results in patients completing maintenance BCG. There is a need to better understand the factors associated with BCG use and discontinuation. A systematic review on real clinical world showed that less than a quarter of studies report that the high-risk patients received BCG maintenance therapy. 48 In the EORTC trial 30962, comparing one-third versus full dose BCG and 1- versus 3-year maintenance in intermediate and high-risk NMIBC no difference in toxicity emerged between the 4 arms, demonstrating that toxicity was independent from both dose and treatment duration. 49 In this study, only 60% and 36% of patients randomized to receive 1-year and 3-year maintenance completed the treatment, respectively. Although in the past BCG toxicity was identified as a primary factor, in recent international trials BCG-related toxicity accounts for less than 10% of drop-outs. So far, the causes for the BCG maintenance interruption remain under debate.
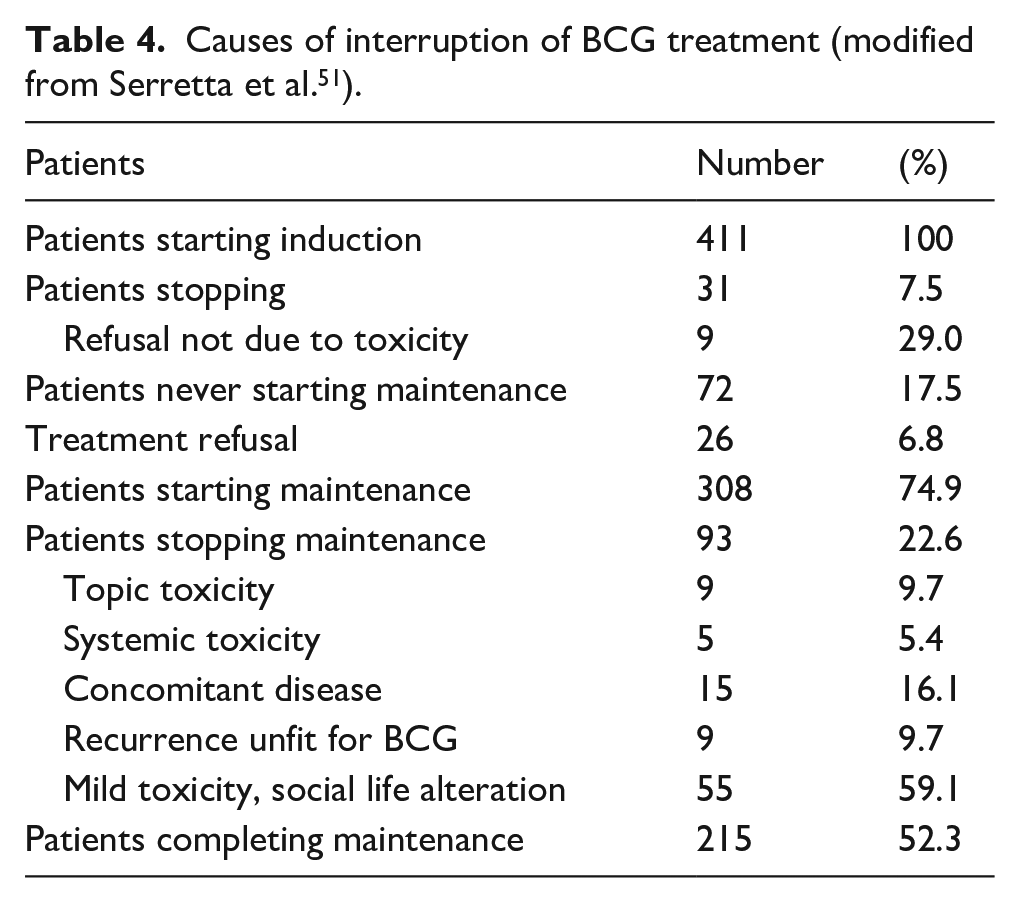
Di Gianfrancesco et al. 50 showed that a tailored instillation procedure may reduce BCG discontinuation and side effects in patients with severe functional impairment. Serretta et al. 51 out of 411 patients undergoing intravesical BCG with 1-year maintenance, reported that 215 (52.3%) only completed 1 year of treatment. In their study, toxicity requiring treatment interruption was recorded in 25 (6.1%) patients only (Table 4). The poor patient’s adherence to BCG treatment was found to be multifactorial and mainly due to personal difficulties related to the prolonged duration of the treatment, to grade-I toxicity underestimated by the urologists and to the limited patients’ awareness of the therapeutic value of maintenance to prevent recurrence and progression. The AA proposed a structured periodical counseling and a timely recognition and therapy of mild but persistent symptoms, that could significantly ameliorate patients’ acceptance of BCG maintenance.
Causes of interruption of BCG treatment (modified from Serretta et al. 51 ).
Can we prevent or reduce BCG toxicity?
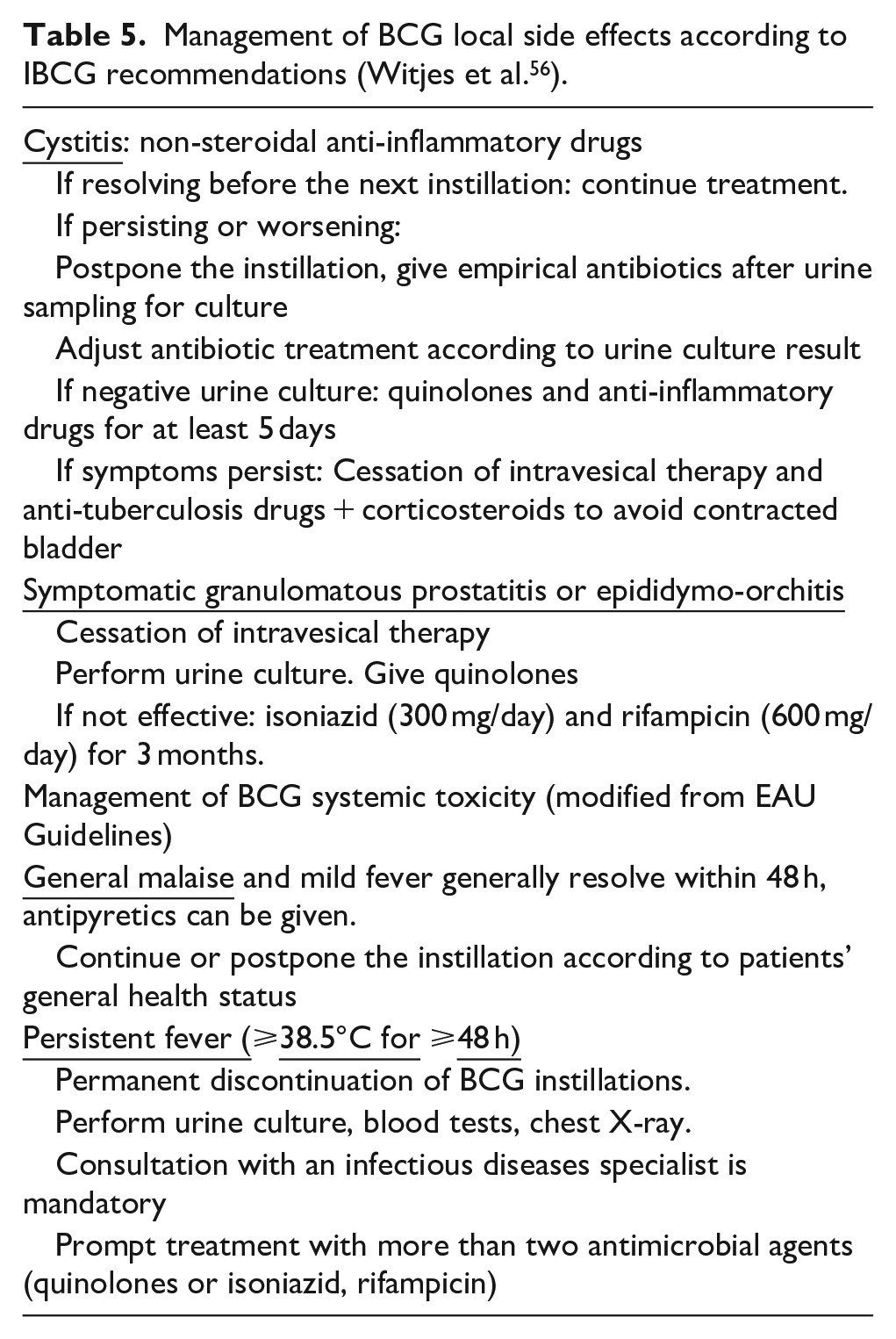
The analysis of the side effects occurred in the EORTC study comparing one-third dose with full dose BCG and 1 year with 3 years maintenance provided useful recommendations on BCG toxicity. Out of 1316 patients, 63% reported local and 31% systemic side effects. 52 The most frequent local side effect is BCG-induced cystitis, occurring in more than 30% of the patients while the most frequent systemic side effect is general malaise occurring in up than 15%–20% of patients. Severe side effects are rare and have been reported as BCG infection or immune reaction in any organ, often with very unusual symptoms and signs. The incidence of clinical significant BCG infection has been reported in 1% of patients and maintenance is not associated with an increased risk of toxicity. 53 Major complications often appear after accidental systemic absorption of the drug. Thus, contraindications of BCG instillation should be strictly respected. Absolute contraindications of intravesical BCG are an interval less than 2 weeks after TURB, gross hematuria, traumatic catheterization, symptomatic urinary tract infection. BCG should be used with caution in immune-compromised patients. The presence of leukocyturia, micro-hematuria or asymptomatic bacteriuria is not a contraindication for BCG and antibiotic prophylaxis is not necessary in these cases. A study failed in demonstrating the prophylactic activity of isoniazid against local or systemic toxicity, 54 while a prospective but small study showed that ofloxacin given shortly after BCG instillation could reduce the incidence of moderate-to-severe side effects. 55 The urologist must inform the patient and his general practitioner that many complications can occur late, also after years from the end of the treatment. In conclusion, the incidence of local or systemic side effects and the most severe toxicity can be prevented or reduced adopting all the possible cautions. The prompt recognition at first occurrence permits their effective treatment in almost all cases. The management of the toxicity of BCG should be based on the recommendations of the International Bladder Cancer Group (IBCG) 56 (Table 5).
Management of BCG local side effects according to IBCG recommendations (Witjes et al. 56 ).
Beyond BCG
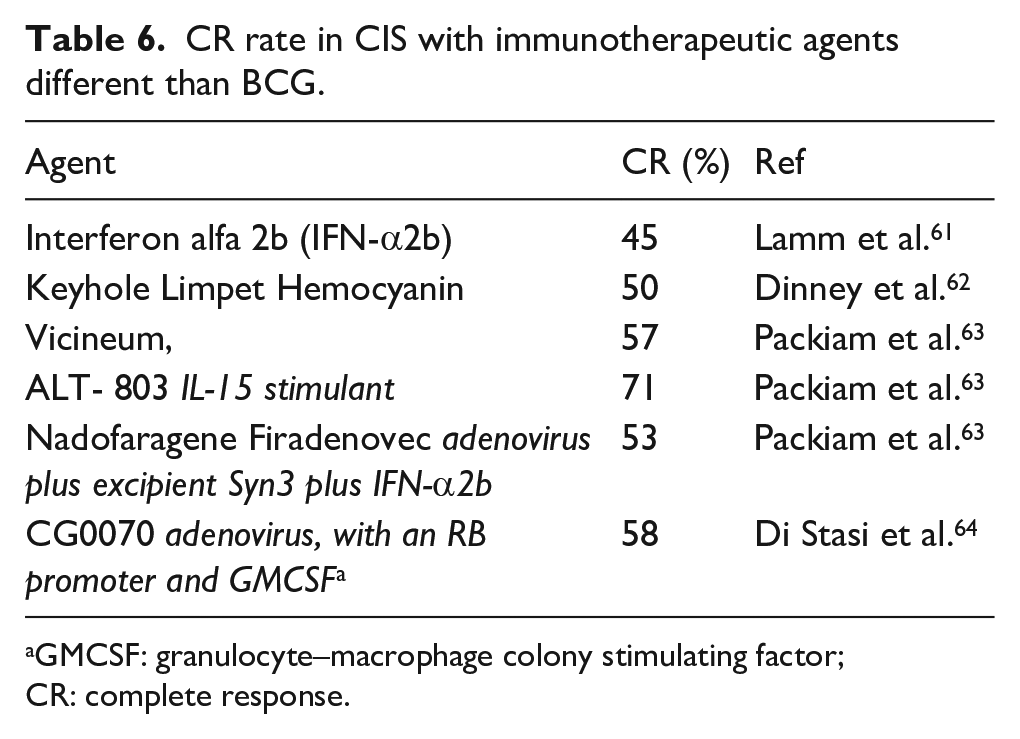
Research is ongoing to obtain genetically modified BCG (recombinant BCG) to reduce toxicity and increase the immune response57,58 Recently, a recombinant BCG (VPM2001) demonstrated at 5 years a complete response of 49% in bladder cancer patients not responding to standard BCG. 3 If the expectations will be fulfilled recombinant-BCG could help for the chronic supply shortage. Promising results were obtained in patients affected by BCG resistant NMIBC with MCNA (Mycobacterium Cell wall Nucleic Acid). It is composed of Mycobacterium phlei cell wall fragments complexed with active DNA characterized by both an immunotherapeutic and direct cytotoxic activity. 59 Many other immunotherapeutic agents have been object of investigations to improve the outcome of patients who are intolerant or resistant to BCG. 60 Some preliminary results are encouraging but further studies are needed. Moreover, the results are difficult to interpretate since some studies were conducted on naïve NMIBC, Tis in most of the cases, while others on NMIBC refractory to BCG60–63 (Table 6). Several studies have been conducted on device-assisted intravesical chemotherapy delivering, with promising but not yet conclusive results.64–66 In the last decade intensive research has been developed on immune checkpoint inhibitors. 67 The results of the SWOG S1605 phase 2 trial on systemic atezolizumab monotherapy in BCG-unresponsive NMIBC has been recently presented. 68 Particularly, in the subgroup of patients with carcinoma in situ (CIS), systemic atezolizumab monotherapy resulted in 3 and 6-months CR rates of 43% and 27%, respectively. At 12 months the 56% of the patients maintained a complete response with a complete response rate of 20%. Similar results were obtained with pembrolizumab monotherapy. 69 However, the results of systemic immune checkpoint inhibitor monotherapy do not reach the complete response rate of 50% at 6 months and 30% at 12 months considered “clinically significant result” in BCG unresponsive CIS according to the IBCG. 70 Thus, the only way to obtain useful results with the immune checkpoint inhibitor therapy in BCG-unresponsive CIS could be the combination with other treatments, first of all BCG itself, and many trails are ongoing.
CR rate in CIS with immunotherapeutic agents different than BCG.
GMCSF: granulocyte–macrophage colony stimulating factor; CR: complete response.
Conclusion
Since 1976, BCG represents a cornerstone in the prevention and therapy of NMIBC, thanks to the intuition and pioneering work of Morales. After almost half century we have the answers to many questions and we are able to better manage BCG intravesical treatment. Nevertheless, the way forward for NMIBC treatment is rapidly evolving. Several clinical trials are ongoing with new drugs, first of all with the immune checkpoint inhibitor administered alone or, better, in combination with BCG. At the present, BCG remains an essential and irreplaceable tool for the treatment of intermediate and high risk NMBC.
Footnotes
Acknowledgements
To Prof. Michele Pavone-Macaluso to whom I owe all my knowledge on bladder cancer.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.