
Abstract
Introduction:
Benign prostatic hyperplasia (BPH) mainly leads to lower urinary tract symptoms (LUTS) in aging men. The present study investigates the role of cholecalciferol, Silymarin, and their combined administration in patients with BPH suffering from LUTS.
Methods:
This double-blind, randomized, controlled trial enrolled 80 participants (50–80 years) diagnosed with BPH, from March 2019 to March 2020. Based on serum 25-(OH) vitamin D levels we formed subgroups, each receiving specific interventions. Measurements of International Prostate Symptom Score (IPSS), Maximal Urinary Flow Rate (Q-max), Prostate Volume (PV), Post-Void Residual (PVR), and Prostate-Specific Antigen (PSA) were recorded at baseline and following 3 months of follow-up.
Results:
Participants with serum concentration of 25-(OH) vitamin D below 20 ng/ml simultaneously received cholecalciferol and Silymarin that significantly improved IPSS, irritation, obstruction, PV, and PVR. In those with concentrations ⩾20 ng/ml, a single use of Silymarin significantly reduced IPSS, irritation, obstruction, and PVR. Adjustment of confounding variables revealed independent and significant effects of both cholecalciferol and Silymarin on PVR, IPSS, and obstruction. Cholecalciferol also improved irritation, while Silymarin reduced prostate volume. These findings highlight potential therapeutic benefits for BPH-associated LUTS, encouraging further exploration and clinical consideration.
Conclusions:
In this investigation, combination therapy with cholecalciferol at 50,000 IU/w for 8 weeks and Silymarin at a dosage of 480 mg for 3 months resulted in a notable improvement in the IPSS score, PV, and PVR, as well as both irritative and obstructive symptoms. However, the total PSA and free PSA amounts did not reach a significant difference.
Keywords
Introduction
Benign prostatic hyperplasia (BPH) is a histological description reflecting the excessive proliferation of glandular epithelial cells, smooth muscle, and connective tissue that occurs in the transition zone of the prostate. According to autopsy data, the histological changes suggestive of BPH in elderly males begin approximately at 40–45 and rise consistently with age, reaching 60% at age 60 and 80% at age 80. 1 BPH should be distinguished from benign prostatic enlargement, which refers to the condition of the enlargement of the prostate gland. In contrast, lower urinary tract symptoms (LUTS), including irritative symptoms such as frequency, nocturia, and urge urinary incontinence, and obstructive symptoms like reduced flow, hesitancy, and the feeling of incomplete emptying, frequently cause individuals to seek medical treatment.2,3 LUTS due to BPH affects up to 50% of men over age 50 and up to 80% of men over age 80. 4
Androgens and estrogens are mainly associated with the pathophysiology of BPH. Development of BPH requires the regulatory action of androgen signaling through androgen receptors, while estrogen receptors, including (Alfa and Beta) can stimulate or inhibit prostatic proliferation, respectively.5,6 Chronic inflammation has recently been considered a significant variable in the emergence of BPH. In BPH, higher amounts of pro-inflammatory cytokines, including interleukins (IL-1, IL-2, IL-4, IL-6, IL-7, IL-8, IL15, and IL-17), are secreted by prostate stromal and epithelial cells compared to normal prostates. Also, the role of growth hormones (COX-2, TGF-beta, and FGF-2) and oxidative stress has been established recently.7–10 The underlying etiology of BPH seems to involve altered gene expression (BCL-2 and BCL-XL), affecting apoptosis and proliferation, culminating in decreased cell death rate and enhanced proliferation. 11
Treatment options available for the BPH/LUTS patients include pharmacological intervention (anticholinergics, alpha-blockers, low-dose daily Tadalafil), minimally invasive procedures (photoselective vaporization, laser enucleation, water vapor thermal therapy), and surgery. 12 BPH is a chronic and progressive condition manifesting with a wide range of symptoms, from LUTS to potential kidney damage, increasing with. 13 At the same time, since the incidence of this disease increases with age among societies and also considering the fact that the number of older people in the world will increase in the coming decades, management of this entity will become one of the challenges of healthcare providers in the coming years. On the other hand, current pharmacological interventions are frequently associated with adverse effects such as headache, dizziness, xerostomia, gynecomastia, and sexual dysfunction. The administration of herbal medicines in the management of BPH achieved prominence due to adverse effects of conventional treatments. 14 Meanwhile, vitamin D has been identified to play a crucial role in regulating gene transcription influencing the expression of antimicrobial peptides and inflammatory mediators. 15 Besides, vitamin D appears to exhibit an inhibitory effect on BPH by modulating the proliferation of prostate stromal cells. 16 In the recent study published by Yeo et al., 17 they showed that the administering vitamin D supplements effectively inhibited the growth of prostate volume and improved LUTS symptoms.
On the other hand, Silymarin, currently used as a medication for several chronic hepatic conditions, comprises seven flavonolignans and one flavonoid. 18 Various studies have also demonstrated the antioxidant, anti-inflammatory, pro-apoptotic, and antiproliferative effects of Silymarin. Besides acting as a selective ER β-agonist, Silymarin has been shown to stimulate the cyclin-dependent kinase inhibitors p21 and p27 in a prostate cancer cell line, leading to cell cycle arrest.19–22
Limited studies investigated the therapeutic role of Silymarin, cholecalciferol, and their combined administration on improving LUTS in BPH patients. Hence, we aimed to perform a double-blind, controlled clinical trial to evaluate the efficacy of mentioned therapeutic approaches in BPH patients suffering from LUTS.
This double-blind, controlled clinical trial aims to assess the therapeutic efficacy of Silymarin, cholecalciferol (vitamin D), and their combined administration in individuals diagnosed with benign prostatic hyperplasia (BPH) experiencing lower urinary tract symptoms (LUTS). The study intends to investigate the impact of these interventions on prostate volume, LUTS severity, and potential improvements in overall patient well-being.
Methods
Study volunteers and inclusion/exclusion criteria
Recruitment was carried out between March 2019 and March 2020 at the Booali Hospital, University-based Hospital of Islamic Azad University of Medical Science (Tehran, Iran). From the 120 participants, 80 healthy patients were allocated. The remaining 40 participants were excluded due to various reasons, such as not meeting the inclusion criteria, failing to provide written informed consent, or having conditions listed in the exclusion criteria. All subjects were relatively healthy but suffered from both LUTS and BPH. The inclusion criteria for participation in the study were the known cases of BPH, based on clinical and paraclinical findings by a urologist, including patients undergoing treatment with tamsulosin 0.4 mg/day for at least 3 months, these patients were referred to our study from another medical practitioner, and they had been prescribed tamsulosin as part of their ongoing management, aged 50–80 years, an International Prostate Symptom Score (IPSS) greater than 8, a total serum Prostate Specific Antigen (PSA) concentration <4 ng/ml, and providing written informed consent to participate in the study. 23 The exclusion criteria were comprehensive to ensure the selection of appropriate participants for the study. Kidney dysfunction was one of the key exclusion factors, defined as an estimated glomerular filtration rate (eGFR) of less than 60 ml/min/1.73 m² or the presence of chronic kidney disease. Patients diagnosed with prostate cancer, indicated by elevated PSA levels (>4 ng/ml), abnormal digital rectal examination findings, and confirmed by prostate biopsy, if necessary, were also excluded. Urinary tract obstruction, defined as a condition causing significant blockage of urine flow and confirmed by imaging studies or clinical findings, was another exclusion criterion.
Bladder dysfunction characterized by neurogenic bladder, overactive bladder, or underactive bladder, diagnosed through urodynamic studies, was grounds for exclusion. Additionally, patients with perineal damage, referring to any trauma or injury to the perineal region that affects normal urinary or reproductive function, were not included in the study. To ensure the participants had a sufficient degree of obstruction that could be objectively measured and potentially improved by the interventions, those with a maximum urinary flow rate (Q-max) of less than 15 ml/s were excluded.
Other exclusion criteria included urinary retention, liver problems, active infection, incontinence, urinary tract stones, a history of urethral stricture, partial prostate removal, prostatitis, presence of hematuria, cystoscopy, pelvic or urological surgery, diabetes, neurological diseases including Parkinson’s disease, spinal disk defects, heart failure, pelvic radiotherapy, psychiatric disorders like severe depression and schizophrenia, and tuberculosis. Patients with a history of using drugs such as anti-depressants, antihistamines, vasoconstrictors, diuretics, narcotics, metronidazole, Yohimbine, anticholinergics, alcohol and caffeine consumption, and PDE5 inhibitors were also excluded from participation.
Furthermore, individuals with 25-(OH) vitamin D levels greater than 100 ng/ml were not eligible for the study. Non-compliance with the prescribed treatment regimen during the study period and unwillingness to cooperate were additional grounds for exclusion. These stringent criteria were set to maintain the integrity of the study and ensure the safety and reliability of the results.
Silymarin, cholecalciferol, and placebos
The Silymarin capsules, branded as “Liversil,” were produced by Rose Pharmed Pharmaceutical Company. Each capsule contained 300 mg of milk thistle herb, equivalent to 240 mg of Silymarin. Cholecalciferol pearls, with a dosage of 50,000 IU, were produced by Zahravi Company. Additionally, the placebos used in the study were designed to resemble the Silymarin capsules and Cholecalciferol pearls in appearance and organoleptic characteristics. These placebos were manufactured by the Industrial Laboratory of the Faculty of Pharmacy at Tehran University of Medical Sciences to ensure they were identical in appearance to the actual medications.
Study design and patient allocation
The study was a pilot stratified, randomized, double-blind, placebo-controlled clinical trial with an add-on design and was conducted according to the guidelines laid down in the Declaration of Helsinki. With a cut-off point of 20 ng/ml for Vit D, 20 ng/ml or above are adequate and less than 20 ng/ml was considered low. Patients were classified into two groups based on serum 25-(OH) vitamin D (n = 40 for each of them) with forty packets inside each group’s box, containing cards with codes similar to those on drug or placebo packages. The allocation to vitamin D groups was based on eligibility, with one packet randomly selected for each participant by a researcher. The study employed a double-blind procedure, validated by a blinding assessment conducted throughout the duration, where both participants and investigators guessed their group assignment to ensure integrity.
From the start, patients were accidentally formed equal groups of 40 patients with low vitamin D level and 40 patients with high vitamin D level. Each group was divided into two sub-group. The method of randomization was conducted using a computer-generated simple randomization method, with allocation concealed through opaque, sealed envelopes opened at the time of assignment. subgroups A and B had adequate Vit D level (25(OH)D ⩾ 20 ng/ml) and subgroups C and D had low Vit D level (25(OH)D < 20 ng/ml). Trial had an allocation ratio 1:1 for each sub-group. Researchers independently conducted randomization for the patient grouping and examining the inclusion criteria for the study. Finally, 68 participants completed the study. Subgroup A (n = 15) received tamsulosin 0.4 mg/day and two placebos, the first every 12 h for 3 months and the second every week for 8 weeks. Subgroup B (n = 17) received tamsulosin 0.4 mg/day, Silymarin 240 mg every 12 h for 3 months and the placebo every week for 8 weeks. Subgroup C (n = 16) received tamsulosin 0.4 mg/day and a placebo every 12 h for 3 months and cholecalciferol 50,000 IU/w for 8 weeks. Subgroup D (n = 20) received tamsulosin 0.4 mg/day, Silymarin 240 mg every 12 h for 3 months and cholecalciferol (50,000 IU/w) for 8 weeks. Sometimes to enhance understanding, we avoided using group abbreviations and provided a detailed explanation of the administrated treatment. All participants were evaluated for total IPSS, peak flow rates (Q-max), prostate volume (PV), post-void residual (PVR), and serum amounts of total/ free PSA and 25-(OH) vitamin D that were measured at the beginning of the study and day 90 (Figure 1). On the first day, eligibility check, demographic and medical history taking, a thorough physical examination, abdominal sonography and uroflowmetry, laboratory tests, and IPSS were evaluated. Patients underwent second (day 1), third (week 4), and fourth (week 8) out-patient visits, during which abdominal sonography and uroflowmetry, laboratory tests, and IPSS were done again. A fifth and sixth visits were also done in weeks 12 and 13, respectively. Patients were all assessed for drug adverse effects at every visit after taking pills. After treatment no adverse effect was reported.
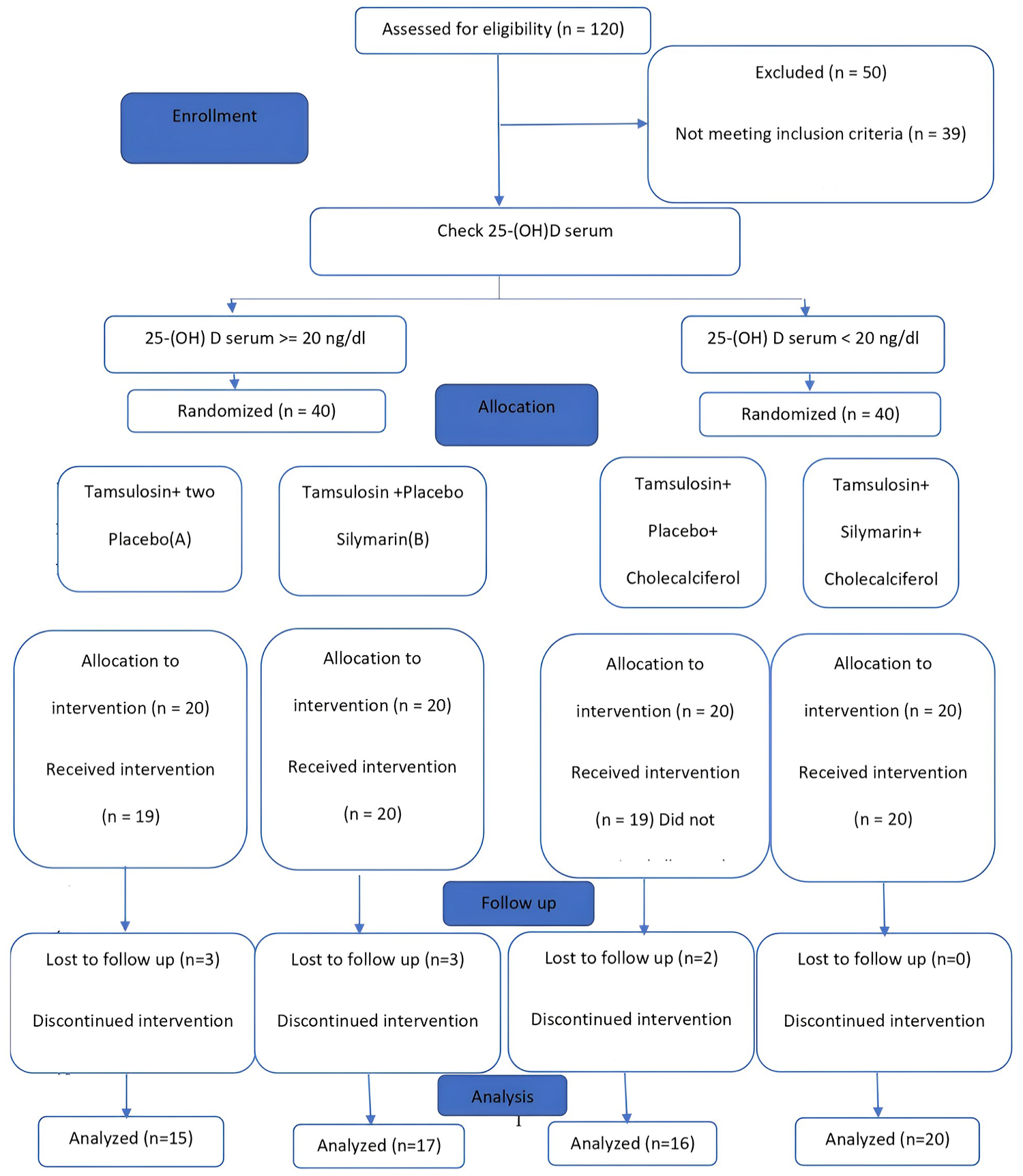
Consort chart.
Sample size
We conducted a sample size calculation using G*Power software, initially planning for a study design involving comparisons between groups using a one-way ANOVA framework, considering fixed effects, main effects, and interactions. 24 However, the study ultimately involved comparisons between two groups rather than multiple groups, which are typically analyzed with methods like t-tests or Mann-Whitney U tests. The calculation assumed a significance level (alpha) of 0.05 and a power (1-beta) of 0.80. Factoring in an expected dropout rate of 20%, we estimated a total sample size of 72 participants, with 15 participants per group.
Primary outcome
The primary outcome of the study was the change in the International Prostate Symptom Score (IPSS) from baseline to the end of the study period. Secondary outcomes included changes in peak flow rates (Q-max), prostate volume (PV), post-void residual (PVR), and serum levels of total/free PSA and 25-(OH) vitamin D.
Assessment of LUTS
The volunteers completed the IPSS questionnaire. In addition to the total IPSS score, irritation and obstruction were assessed separately. Uroflowmetry and Q-max were measured. For increasing result reliability, the test was repeated for urinary volumes below 150 cc, PVR was assessed with an abdominal probe at 3.5–5 MHz, and volumes less than 30 ml are clinically insignificant. PV was calculated using the formula for a prolate ellipsoid (width × length × height × 0.523). Normal prostate volume was considered 20 cc.
Laboratory tests
PSA total and PSA free in serum were determined using the electrochemiluminescence method on two occasions. The patients were structured to abstain from ejaculation or sexual intercourse 24 h before the test.
Ethics approval
The study received ethical approval from the biomedical research ethical committee at Islamic Azad University of Medical Science under the reference number IR.IAU.TMU.REC.1398.170. The trial was conducted in accordance with the guidelines specified in the Declaration of Helsinki. All participants provided written informed consent before participating in the study. The trial was registered with the trial registration number IRCT20200906048641N1.
Statistical methods
Data analysis was performed using SPSS version 20.0 (SPSS Inc., Chicago, IL). To assess the statistical normality of numerical variables, the Smirnov-One-Sample-Kolmogorov test was utilized, and it was found that the distribution of the data was skewed. Therefore, the mean and standard deviation were used for describing numerical data, while for describing qualitative data, frequency and percentages were employed. The Mann-Whitney U test was used to compare two groups for numerical variables, and for nominal variables, Pearson’s chi-square test and Fisher’s exact test were utilized. To compare the four subgroups for numerical and ordinal variables, the Kruskal-Wallis test was applied. Pearson’s chi-square and Fisher’s exact tests were used to compare nominal variables. A multiple linear regression model with an interaction term was employed to examine the interaction effect between the two interventions, cholecalciferol (vitamin D) and Silymarin, as well as the influence of confounding variables. Significance levels below 0.05 were considered statistically significant for result interpretation.
Results
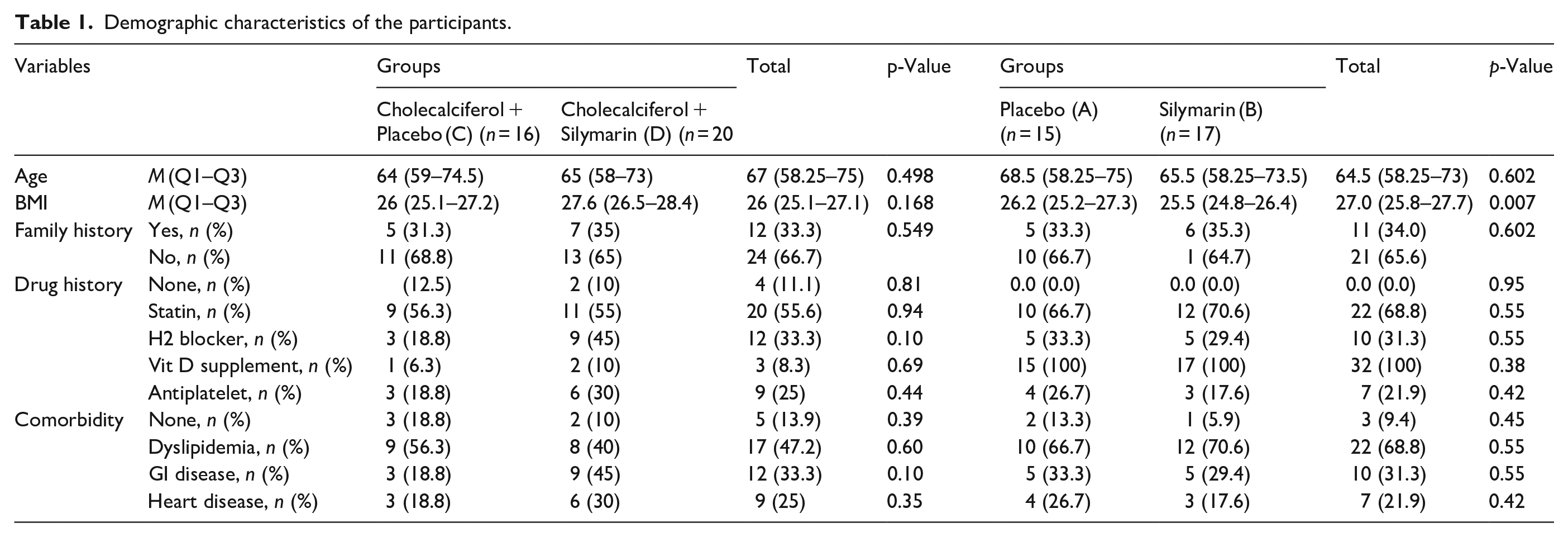
A total of 68 individuals were enrolled and distributed across four distinct intervention groups: Placebo (A, n = 15), Silymarin (B, n = 17), Cholecalciferol + Placebo (C, n = 16), Cholecalciferol + and Silymarin (D, n = 20). The analysis focused on key variables such as age, BMI, family history, drug history, and the prevalence of comorbidities within each group. Median values and interquartile ranges (Q1–Q3) were utilized to provide a comprehensive overview of the central tendencies of age and BMI. Additionally, the presence or absence of family history, drug history, and comorbidities, including dyslipidemia, gastrointestinal disease, and heart disease, were documented. The age distribution did not show significant disparities between the groups. The differences in age, BMI, presence of a positive family history, drug history, and prevalence of comorbidities were not statistically different between the groups (p = 0.498). However, the cholecalciferol + Silymarin group showed a significantly higher BMI than the cholecalciferol + placebo group (p = 0.007) (Table 1).
Demographic characteristics of the participants.
Patient with 25-(OH) vitamin D levels < 20 ng/ml:
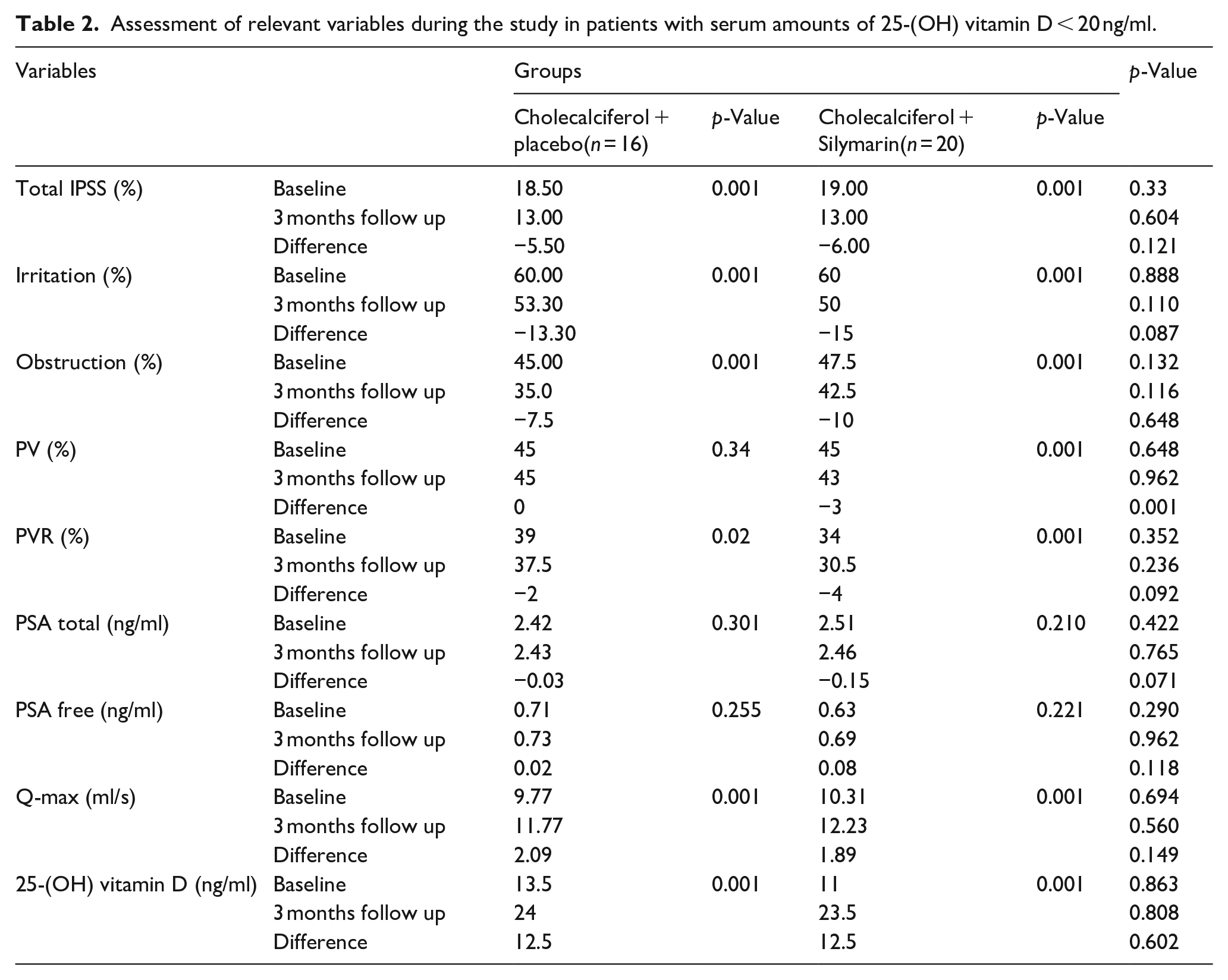
The cholecalciferol + Silymarin (n = 20) subgroup revealed significant improvements over 3 months. Total IPSS decreased from 54.28% to 41.42% (p = 0.001), indicating an amelioration in overall urinary symptoms. Irritation (60%) and obstruction (47%) also showed consistent reductions, with decreasing values to 50% and 42%, respectively. In the mentioned subgroup, PV (45%) and PVR (34%) reduced to the amounts of 43% and 30.5%, correspondingly (p = 0.001). Both total PSA and free PSA levels showed no significant changes, with marginal variations of −0.15 (p = 0.071) and 0.08 (p = 0.118), respectively. Significantly, in the subgroup cholecalciferol + placebo (n = 16), there was a significant rise in 25-(OH) D levels from 13.5 at baseline to 24 (p = 0.001), indicating a possible correlation between vitamin D and LUTS improvement (Table 2).
Assessment of relevant variables during the study in patients with serum amounts of 25-(OH) vitamin D < 20 ng/ml.
Patient with 25-(OH) D levels ⩾ 20 ng/ml:
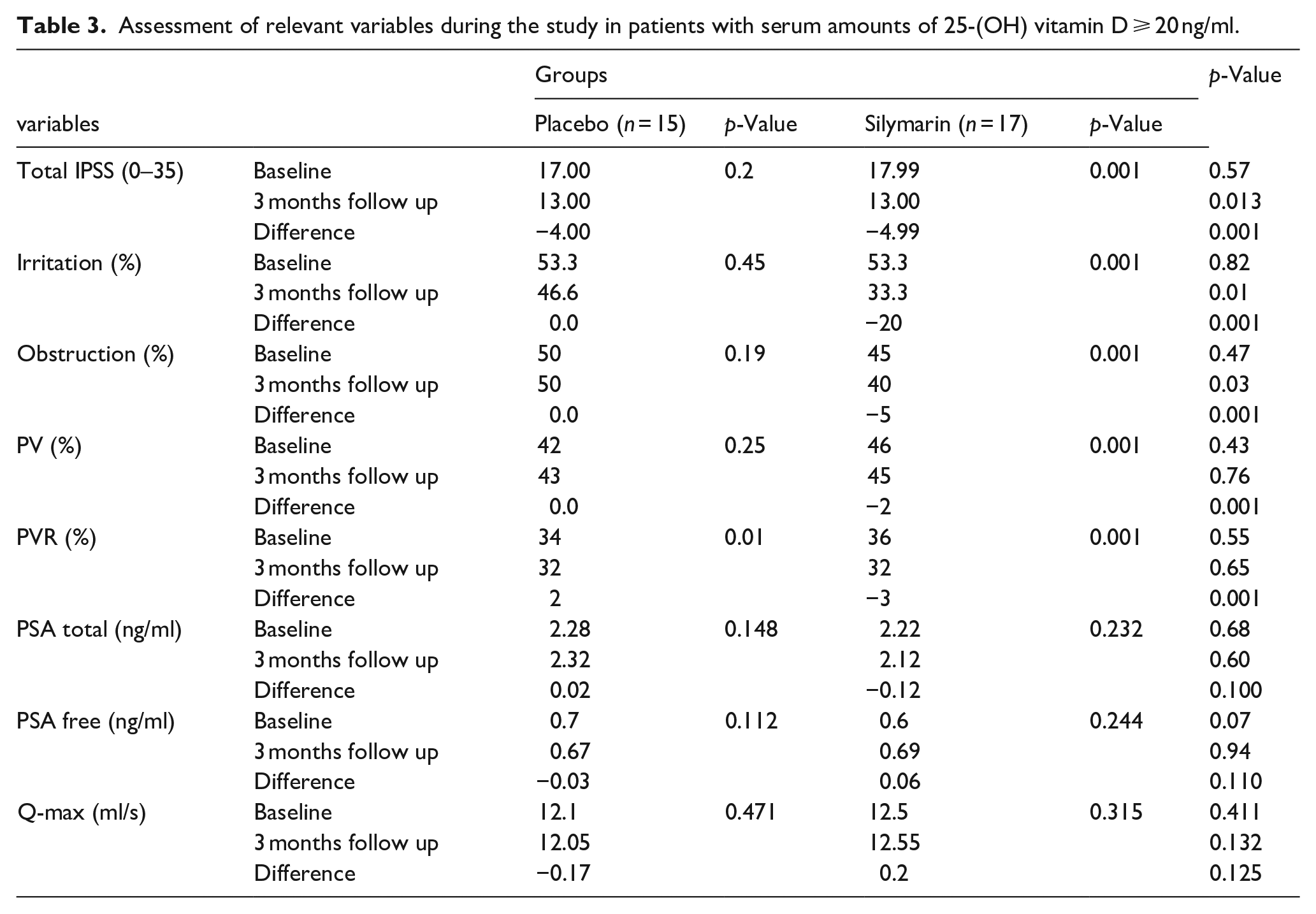
Over the 3-month follow-up, the placebo (n = 15) and Silymarin (n = 17) subgroups demonstrated changes in key parameters. IPSS had a baseline value of 48.57% for the placebo group and 51.42% for the Silymarin group. The placebo group maintained its baseline score during the follow-up, while the Silymarin group substantially reduced to 37.14 (p = 0.013). Similar trends were observed for irritation (53.3%) and obstruction (45%), reaching 33.3% (p = 0.001) and 40% (p = 0.001), respectively, which indicate significant improvements in the Silymarin group compared to the placebo group. Additionally, PV remained relatively stable, while PVR decreased by 3 (p = 0.001) in the Silymarin group. There were slight variations in total PSA and free PSA, with differences of −0.12 (p = 0.100) and 0.06 (p = 0.110), respectively, in the Silymarin group. Furthermore, Q-max exhibited no significant differences between the two groups over the follow-up period (Table 3).
Assessment of relevant variables during the study in patients with serum amounts of 25-(OH) vitamin D ⩾ 20 ng/ml.
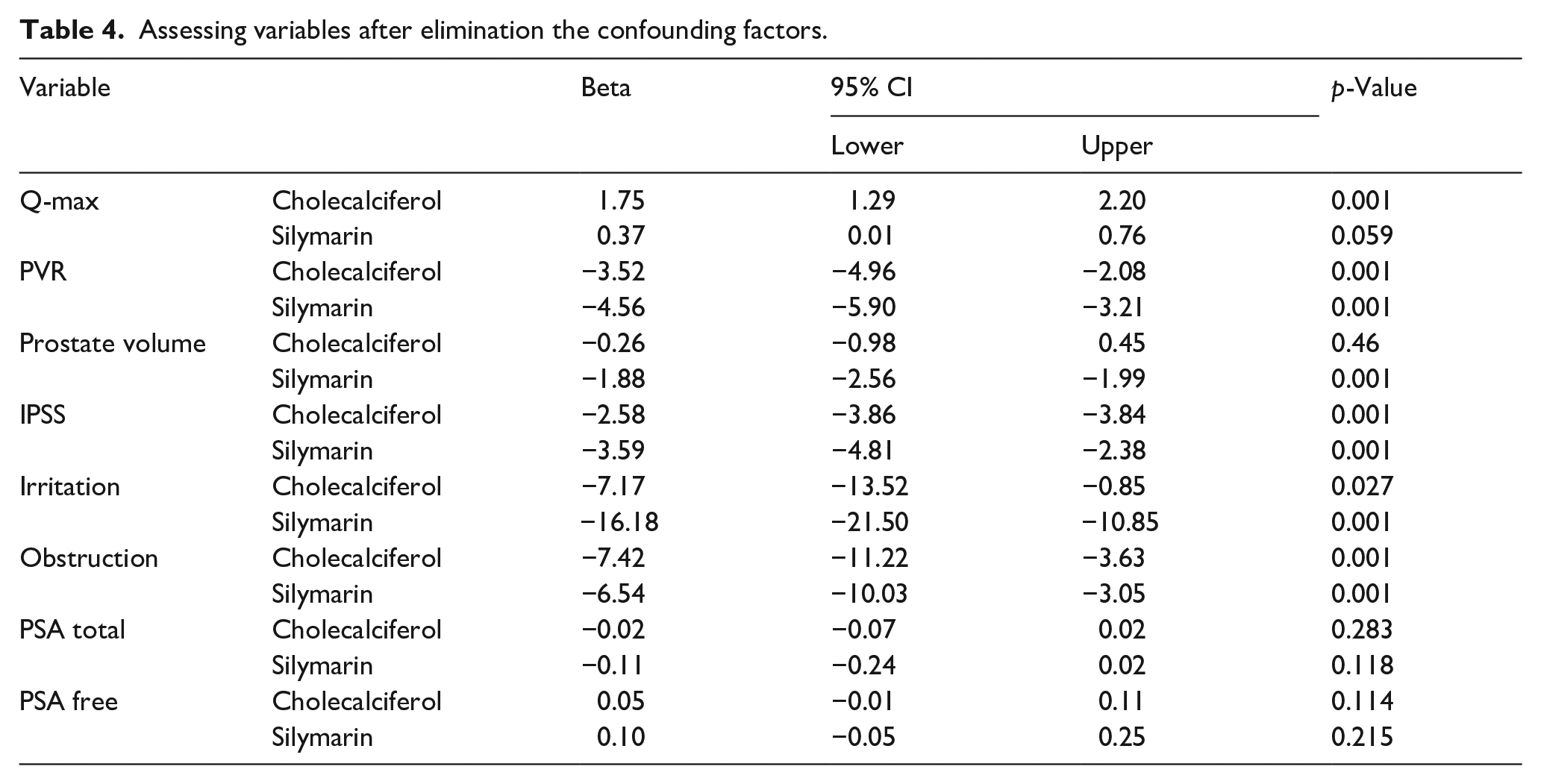
Assessment following the elimination of the confounding variables emphasized that PVR, IPSS, and obstruction showed significant improvement with simultaneous administration of cholecalciferol and Silymarin (p = 0.001). Irritation followed the same pattern for a single consumption of cholecalciferol (p = 0.027) or Silymarin (p = 0.001). PV exhibited a significant reduction with the use of Silymarin (β = −1.88, p = 0.001), and Q-max was only reduced with cholecalciferol consumption (β = 1.75, p = 0.001). However, total PSA and free PSA exhibited no significant changes with a single or combined consumption of cholecalciferol and Silymarin side effects were not observed in any of four groups in the entire study (Table 4).
Assessing variables after elimination the confounding factors.
Discussion
Benign prostatic hyperplasia (BPH) is a prevalent disease among males, exhibiting a high incidence, tending to increase with advanced age.1,25 LUTS resulting from BPH impact approximately 50% of males aged 50 and older, with prevalence increasing to almost 80% among those aged 80 and beyond. 4 The burden of BPH is increasing significantly in many regions across the globe, with a particular emphasis on low-income and middle-income countries. From 2000 to 2019, reported prevalence of benign prostatic hyperplasia increased from 51.1% to 94.01% of old men worldwide. 26 On the other hand, conventional treatments cause unwanted adverse effects, decreasing quality of life, including headache, dizziness, xerostomia, gynecomastia, and sexual dysfunction. 14 Since limited research has been conducted on the effects of Silymarin drug therapy on the LUTS in patients with BPH, and while the results of the previous studies on the correlation between vitamin D concentration and the severity of LUTS are controversial
Our investigation indicated that individuals with a serum 25-(OH) vitamin D amounts below 20 ng/ml exhibited a statistically significant lower Q-max and more prevalent irritation symptoms in comparison to patients with a serum 25-(OH) vitamin D level above 20 ng/ml. After administration of cholecalciferol at the dosage of 50,000 IU/w for 8 weeks, patients experienced improvements in total IPSS, obstruction, irritation, PVR, and Q-max.
A well-established correlation has been identified between the presence of inflammation and proliferation of the prostate tissue and the severity and progression of BPH. Prostate inflammation causes bladder irritability and altered detrusor muscle function, resulting in increase of urinary frequency and urgency. On the other hand, previous investigations have demonstrated induction of collagen expression and fibrotic tissue production following prostatitis, culminating in enhancement of urinary tract resistance.7,9,27
Anti-inflammatory effects of vitamin D are assumed to be reached through the regulation of expression of interleukins (including IL-10, IL-17A, IL-8, and IL-6), TGF-β, signaling NFK-β, inhibition of the prostaglandin pathway (reduction in expression of PG receptor and COX-2), and increase in expression of PGDF-15. 28 Furthermore, vitamin D receptor agonists seem to decrease the expression of active myofibroblasts such as Desmin and Smoothelin. 29
An investigation conducted by Haghsheno et al. 30 performed a cohort of 155 males with an average age of 72.76 years, revealing a significant inverse relationship between serum vitamin D concentrations and prostate volume and development of BPH in both type 2 diabetic and non-diabetic patients. However, In the present investigation, we found no significant correlation between elevated serum amounts of vitamin D and the values of PV. Although Haghsheno did not assume an exact cut-off value for vitamin D concentration, the inconsistency could arise from age distribution discrepancies and the methodology employed between the studies.
Previous studies conducted by Zhang et al. 31 and Elshazly et al. 32 showed that people with vitamin D deficiency had significantly higher IPSS and PV and lower Q-max. Findings were consistent with our study except for significantly decreased PV values.
In a cohort investigation, Yoo et al. 33 found no correlation between vitamin D serum concentration and PVR, PV, total IPSS, and total PSA in BPH patients. Consistent with our findings, this investigation reported no correlation between vitamin D, PV, or total PSA. Contrary to this, after 8 weeks of cholecalciferol at 50,000 U in patients with 25-(OH) vitamin D < 20 ng/ml, total IPSS, and PVR showed a significant reduction, and patients experienced improvement. Besides, a single dose of cholecalciferol (200,000 U) was prescribed to patients with serum levels of 25-(OH) vitamin D < 20 ng/ml.
A similar study carried out in Iran by Zendehdel et al. 34 found a reduction in IPSS score, PV, and total PSA levels, regardless of age or presence of diabetes. This study confirms our findings of significant IPSS score improvement. However, our study found no significant reduction in serum PSA amounts and PV after 8 weeks of cholecalciferol 50,000 U in patients with 25-(OH) vitamin D < 20 ng/ml. In this study, participants aged over 50 with asymptomatic to mild symptoms of LUTS with no inclusion or exclusion limitation in terms of PSA concentrations were investigated. Also, the vitamin D prescription was once every 2 weeks for 6 months. In contrast, our study included participants aged 50–80 with total serum PSA amounts < 4 ng/ml of moderate-to-severe symptoms treated with tamsulosin for at least 3 months. The vitamin D prescription was every 2 weeks until 8 weeks.
Our findings indicate that the administration of Silymarin at a dosage of 480 mg for 3 months as an add-on treatment along with the primary treatment resulted in a notable improvement in the IPSS score, PV, and PVR, as well as both irritative and obstructive symptoms. Prostate epithelial cells express ER-β, while stromal cells express ER-α. Prostate stromal cell proliferation is induced by estrogen (estradiol) through ER-α, while ER-β is responsible for the hormone’s anti-inflammatory and antioxidant effects. The ER-α/ER-β ratio increases in people with BPH. 6
Atawia et al. 22 found that testosterone-induced BPH of male rats given 50 mg/kg Silymarin for 2 weeks increased ER-β and decreased ER-α expression. Silymarin downregulates PCNA, upregulates P21 expression, and increases prostate tissue Bax/Bcl-xl ratio and 3-Caspase activity, modulating the cell cycle and apoptosis. Also, Silymarin reduces oxidative damage by downregulating NFK-B expression in rats with BPH. Another study conducted by Atawia et al. 35 demonstrates that Silymarin’s anti-inflammatory effects are revealed through the reduction in expression of inflammatory mediators like IL8, IL6, NFKB, COX2, and INOS. Also, histopathological changes due to inflammation, including hyperplasia and collagen deposition, have been shown to be reduced by Silymarin.
In 2013, Vostalova et al. 24 evaluated the effects of a Silymarin-selenium combination (Silymarin at a dose of 570 mg/day) for 6 months in BPH/LUTS patients with PSA < 2.5 who did not use any medication. The results showed significant improvement in total IPSS, PVR, Q-max, and total PSA, and no significant side effects were observed in the long-term use. Consistent with our findings, this study found that Silymarin significantly improved total IPSS and PVR. However, in our investigation, Silymarin had no beneficial impact on Q-max or total PSA. The study population, Silymarin dose, duration of treatment, and ethnic composition may contribute to the discrepancy between their findings and ours.
Similar to every other study, our investigation possesses both merits and limitations. The limitations include small number of participants and the lack of conducting rectal prostate ultrasonography. However, the lack of such diagnostic modulation was mainly due to the discomfort experienced by patients undergoing rectal ultrasonography. On the other hand, the utilization of this combination therapy represents a novel approach, mainly due to the limited availability of similar studies investigating the potential impact of Silymarin on BPH in males.
Conclusions
Vitamin D appears to have anti-inflammatory effects in the prostate, bladder, and urinary tract tissues. Reducing inflammatory mediators prevents fibroblast proliferation, minimizes urinary tract resistance, and improves detrusor muscle function. Consequently, cholecalciferol 50,000 U within 8 weeks, along with the primary treatment, could alleviate LUTS/BPH patients with a serum concentration of 25-(OH) vitamin D < 20 ng/ml. On the other hand, the estrogen-modulating actions of the Silymarin medication resulted in PV reduction and improvement in urinary tract resistance, all of which contribute to a reduction in LUTS symptoms. Therefore, an administration dose of 480 mg of Silymarin may be beneficial in alleviating LUTS/BPH. Eventually, we have shown that combination therapy with cholecalciferol at 50,000 IU/w for 8 weeks and Silymarin at a dosage of 480 mg for 3 months resulted in improvement in the IPSS score, PV, and PVR, as well as both irritative and obstructive symptoms. However, the total PSA and free PSA levels remained constant.
Footnotes
Acknowledgements
None.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of ethics
Written informed consent was obtained from all.
Ethical consideration
The study received ethical approval from the biomedical research ethical committee at Islamic Azad University of Medical Science under the reference number IR.IAU.TMU.REC.1398.170. The trial was registered with the trial registration number IRCT20200906048641N1. Informed written consent was obtained from the participants. The authors confirm the availability of, and access to, all original data reported in this study. All human subjects provided written informed consent with guarantees of confidentiality. The authors are employed at an academic or research institution where research or education is the primary function of the entity.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author, upon reasonable request.