
Abstract
Background:
Urinary tract infection (UTI) is humans' second most common bacterial infection. Indiscriminate use of antibiotics is a common practice in underdeveloped and many developing countries that often leads to the emergence of resistant microorganisms to one or several of these agents with gradual narrowing of scope for effective molecules to combat bacterial infections including UTIs. As a common practice, empirical antimicrobial treatment is initiated before the laboratory results of urine culture are available which may lead to the emergence and spread of antimicrobial-resistant strains. Therefore, this study was conducted to identify the common bacterial uropathogens associated with urinary tract infection and their susceptibility to antibiotics.
Objectives:
This study aims to analyze the prevalence of culture-positive isolates and determine the susceptibility patterns of bacterial uropathogens to antibiotics at GAMBY Teaching General Hospital, Bahir Dar, Ethiopia.
Methods:
An institution-based retrospective study was conducted at GAMBY Teaching General Hospital (GTGH) for patients who had UTIs, from November 1, 2015, to December 30, 2021 G.C. Antimicrobial sensitivity tests were done using the disc diffusion technique as per the standard of the Kirby-Bauer method.
Results:
A total of 1,714 urine samples were processed. Of the total urine samples collected, 974 (56.8%) were from women and 456 (26.6%) revealed a positive culture. Among the positive isolates, the gram-negative was 340 (74.6 %), which makes it the most prevalent type. E. coli, 276 (60.5%) and S. saprophyticus, 78 (17.1%) were the two most prevalent uropathogens isolated. The highest percentage of susceptibility to antimicrobial agents was seen with nitrofurantoin 338 (91.4%), Clindamycin 72 (83.7%), Norfloxacin 244 (79.2%), and Cefoxitin 22 (78.6%). Ampicillin 48 (100%), Piperacillin 6(100%), Cefixime 6 (100%), Clarithromycin 6 (100%), Amoxicillin 96 (96%), Amoxicillin/clavulanic acid 242 (89.6%), and Penicillin 12 (85.7%) had the highest percentage of resistance among all isolates to the antimicrobial agents.
Conclusions and recommendations:
Urinary tract infections are mostly caused by Gram-negative bacteria predominantly in females and Escherichia coli is the most common isolated bacteria. Nitrofurantoin, Norfloxacin, cefoxitin, and clindamycin are considered appropriate antimicrobials for the empirical treatment of urinary tract infections. The majority of uropathogens were resistant to antibiotics commonly used in clinical practice. The resistance pattern to all of the microorganisms incriminated showed there was a progressive increment of resistance to the common antibiotics over the study period. Empirical treatment of UTIs should be guided on the newer culture and sensitivity pattern and more importantly, prescriptions should be revised following the culture and sensitivity results.
Introduction
Urinary tract infection (UTI) is the second most common bacterial infection in humans, 1 which occurs mainly in hospitals and communities. 2 It usually occurs when bacteria from the digestive tract or vagina adhere to the opening of the urethra and begin to multiply within the urinary tract involving the kidneys, ureters, bladder, and urethra. The predominant causative agents are Gram-negative bacteria. 3 It is the inflammatory disorder of the urinary tract caused by abnormal growth of pathogens and presented with symptoms of fever, dysuria, urgency, urinary frequency, pyuria, flank pain, and/or lower abdominal pain. Involvement of the upper urinary tract sometimes results in permanent scarring of the kidney. It accounts for the majority of the reasons for hospital visits globally 4 and 35% of nosocomial infections which is the second most common cause of bacteremia in hospitalized patients.
Urinary tract infection (UTI) is caused by the invasion of the pathogen in the urinary system that can manifest as symptomatic or asymptomatic bacteriuria. 5 Nearly 10% of people will experience a UTI during their lifetime 6 and a common chief complaint observed in health care, and nowadays, UTIs are serious public health issues and are responsible for nearly 150 million cases every year. Worldwide, up to 8.1–10.5 million ambulatory visits for UTIs are recorded each year.7–10
UTIs are caused by uropathogens. Escherichia coli remains the predominant uropathogen (80%–90%) and Staphylococcus saprophyticus accounts for (10% to 15%) of acute UTIs. 11 Escherichia coli is the most common gram-negative bacterial pathogen causing a diverse range of clinical diseases that affect all age groups, and Staphylococcus saprophyticus is the most common gram-positive bacteria which primarily affects sexually active young females. Other causative agents include Enterococcus, Proteus spp., Pseudomonas aeruginosa, and Klebsiella pneumonia contribute to UTIs.2,12,13
UTIs can be associated with variable complications; such as morbidity, reduced quality of life, absence from work, and costs of services. However, infections can ascend and sometimes progress to pyelonephritis, bloodstream infection (BSI), and other severe complications in the absence of effective therapy. Failure of antibiotic therapy for uncomplicated UTIs is detrimental from a public health perspective because subsequent antibiotic prescriptions could lead to antibiotic resistance, drug-related adverse events, and increased healthcare costs. Worldwide, it is estimated that 150 million UTIs occur yearly which results in more than 6 billion dollars in direct healthcare cost.14,15 About 700,000 deaths are recorded annually due to antimicrobial resistance (AMR), based on a published survey, and it has been estimated that if appropriate monitoring and preventive steps are not taken, AMR will become one of the major causes of death among hospitalized or non-hospitalized patients in developing and industrialized countries. 16 Indiscriminate use of antibiotics is a common practice in underdeveloped and many developing countries that often leads to the emergence of resistant microorganisms to one or several of these agents with gradual narrowing of scope for effective molecules to combat bacterial infections including UTIs. As a common practice, empirical antimicrobial treatment is initiated before the laboratory results of urine culture are available which may lead to the emergence and spread of antimicrobial-resistant strains. Factually, antimicrobial resistance is one of the principal causes of treatment failure in infectious diseases and a great concern for UTIs. Although there are few research findings present to indicate the resistance profiles in Ethiopia, there is still insufficient information about the prevalence of UTI-related bacteria and their antibiotic susceptibility pattern in the Amhara region, especially in private settings, which is our main study area. Therefore, the current study aimed to measure the prevalence of infections by uropathogenic bacteria and their sensitivity patterns to the currently used antibiotics in the province of GAMBY Teaching General Hospital.
Materials and methods
This retrospective study was conducted in GAMBY Teaching General Hospital (GTGH) after ethical approval was received from GAMBY Medical and Business College from November 1st, 2015 to December 30th, 2021. The hospital is located in Amhara regional state, Bahir-Dar, Ethiopia. It is found 567 Kilometers away from the capital city, Addis Ababa. The Hospital has been providing specialty and sub-specialty services including Neurology, Neurosurgery, Ophthalmology, Dermatology, Hepatobiliary, Urosurgery, orthopedics surgery, and psychiatry, and has been giving specialized medical, gynecological/obstetrical, and surgical treatment to about 100,000 patients in the OPD and 19,000 patients in the general and private wards every year. The hospital has more than 70 beds, which are actively giving services; including an intensive care unit, hemodialysis, and emergency services. Blood, stool, urine, body fluids, and sputum specimens from outpatients and inpatients are collected on-site at a centralized collection center by laboratory personnel and have been giving services to more than 100,000 clients per year.
The laboratory has a department of Serology, Immunology, Parasitology, Hematology, infertility testing, oncology, and microbiology. It can provide, blood culture, stool culture, urine culture, semen culture, throat culture, eye discharge culture, ear discharge culture, genital discharge culture, and pus or wound culture services. It has a patient waiting area, Specimen collection with two rooms, Processing and organizing, and a tracking system with sufficient manpower. The laboratory has integration with the hospital information system with an active network system including the machines which are linked with the laboratory information system.
All patients who were seen at GAMBY Teaching General Hospital (GTGH) from November 01, 2015, G.C. to December 30, 2021, G.C. were included in the study. The study included both male and female outpatients and inpatients who presented with UTI symptoms and signs such as fever, dysuria, urgency, urinary frequency, pyuria, urine color or odor change, and flank pain or lower abdominal pain. Immediately following proper collection, each sample was sent to the laboratory for further processing. For bacterial culture and colony counts; Blood agar, MacConkey agar, Mueller-Hinton agar, and Nutrient agar (Oxoid Ltd., Basingstoke, Hampshire, England) were used. Urine specimens were cultured for isolation of the microbial agents of UTI on blood and MacConkey agar media. Petri dishes containing approximately 15 ml of blood agar and MacConkey agar media were prepared in a total sterile condition and were preserved at 0 - 8°C. The samples were plated out on MacConkey and blood agar media and incubated overnight at 37ºC17–19 Samples were then plated out on nutrient agar and Mueller-Hinton agar media for colony count. Growth of 105 colony-forming units (CFU)/mL was considered a positive urine culture in females while the growth of 103 colony-forming units (CFU)/mL was considered positive in male patients. 18 Samples that showed pure growth of isolate in a count of ⩾105 colony forming units (CFU) per milliliter of urine in females or ⩾103 CFU in males after overnight incubation were considered to indicate significant bacteriuria. 20 The characteristic bacteria on the culture media were aseptically isolated and subjected to microscopical and appropriate biochemical tests for proper identification. Uropathogens were isolated and identified according to NCCLS standard morphological, cultural, and biochemical methods. 19 Each batch of the culture media used was tested for sterility. Standard control strains of E. coli ATCC 25922 and S. aureus ATCC 25923 were used during culturing and antibiotics susceptibility testing as a control throughout the study.
Kirby-Bauer disc diffusion assay on Muller Hinton agar was carried out to determine the antimicrobial susceptibility profiles. 20 The panel antimicrobials included amoxicillin: 30 mg, gentamicin: 10 mg, cefotaxime: 30 mg, nalidixic acid: 30 mg, ciprofloxacin: 5 mg, ofloxacin: 5 mg, norfloxacin: 10 mg, erythromycin: 15 mg, cloxacillin: 5 mg, vancomycin: 30 mg, nitrofurantoin: 300 mg and tetracycline: 30 mg.
According to the report, the susceptibility testing was done on Mueller-Hinton agar (Oxoid Ltd. Basingstoke, Hampshire, England) using disk diffusion (Kirby Bauer’s) technique. This method was done according to the Clinical and Laboratory Standards Institute (CLSI) guidelines to determine the susceptibility of UTI agents. 21 The diameter of the zone of inhibition produced by each antibiotic disk was measured using engineer calipers. The result was interpreted as susceptible or resistant to the antibiotic agent used, depending on the length of the zone of inhibition produced compared to the standard length. 23 Multiple antibiotic resistance index (MAR) (number of antibiotics to which test isolate displayed resistance divided by the total number of antibiotics to which the test organism has been evaluated for sensitivity) for each test isolate was calculated as recommended by Krumperman. 24
The collected data were sorted in the prepared format. The laboratory result of the study was categorized based on age groups and sex. Isolates prevalence rate calculations, frequency distributions, susceptibility patterns, and other descriptive statistics were computed and reviewed. Percentages and ratios were calculated in tables. SPSS version 26 computer software package was used for data analysis. The chi-square test (χ 2 ) was used to measure the association and a P value less than .05 was considered statistically significant (p < .05).
Results
Incidence and sex /age group distribution of UTIs
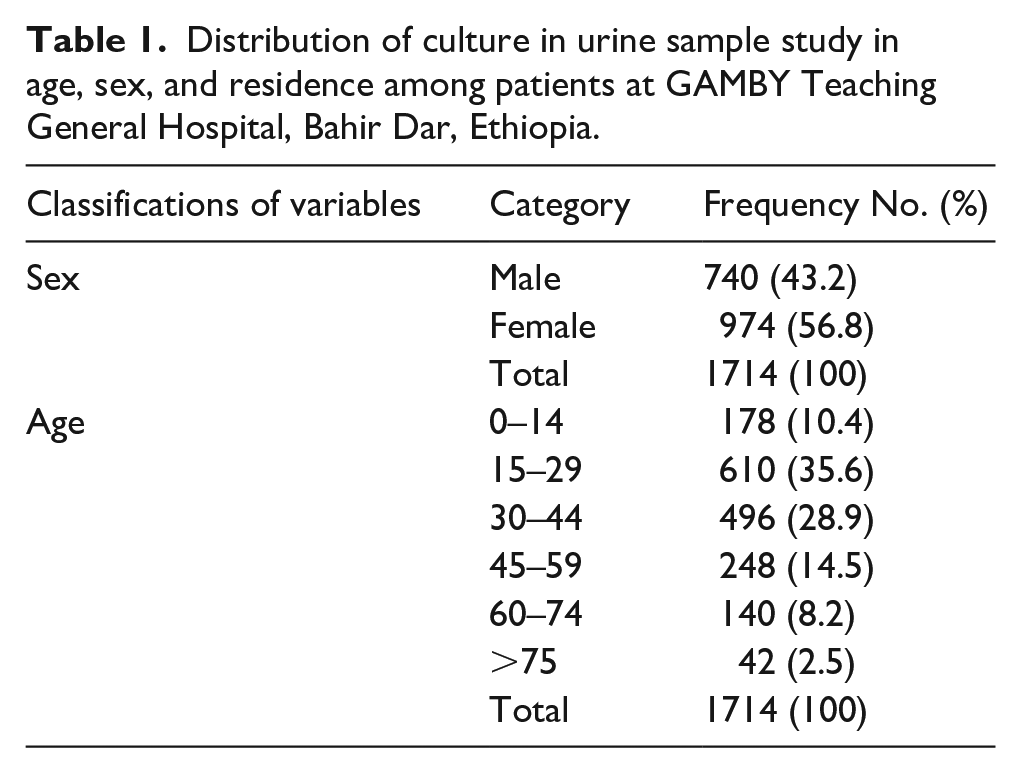
A total number of 1714 patients’ urine samples were conducted for culture and antimicrobial susceptibility tests. Of the 1714 urine samples, 740 (43.2%) were male and 974 (56.8%) were Female with a male-to-female ratio of 1:1.31. The results according to age range from a minimum of 3 days and a maximum of 96 years. The mean age of the patients was 34 + 0.6. The majority (35.6%) of patients were 15–29 years of age followed by 30–44 years of age (28.9%). The least age group was over 75 years of age (2.5%) as shown in (Table 1).
Distribution of culture in urine sample study in age, sex, and residence among patients at GAMBY Teaching General Hospital, Bahir Dar, Ethiopia.
Clinical presentations
Even though some patients’ clinical presentation was not thoroughly documented, the most common clinical presentations found among patients with UTIs were as follows: increased urinary frequency in 1230 (82%) of patients, subjective fever was seen in 980 (70%) of patients, pain during micturition in 720 (48%) of patients, and suprapubic pain or flank pain was seen in 360 (40%) of patients. Urine color changes to cloudy or bloody and urine odor changes were not documented. The urine dipstick testing which was done on all patients showed positive urine white blood cells (sex difference considered, i.e., 2-5 or more WBCs in males and more than 10 WBCs in females) in 1500 (94%) of patients, urine blood cells were found in 660 (44%), and urine nitrates were positive in 1456 (90%) of patients. Urine leukocyte esterase was not documented. The systemic findings like leukocytosis, objective fever, and raised CRP and/or ESR were not documented either.
Isolation and identification of Uropathogens
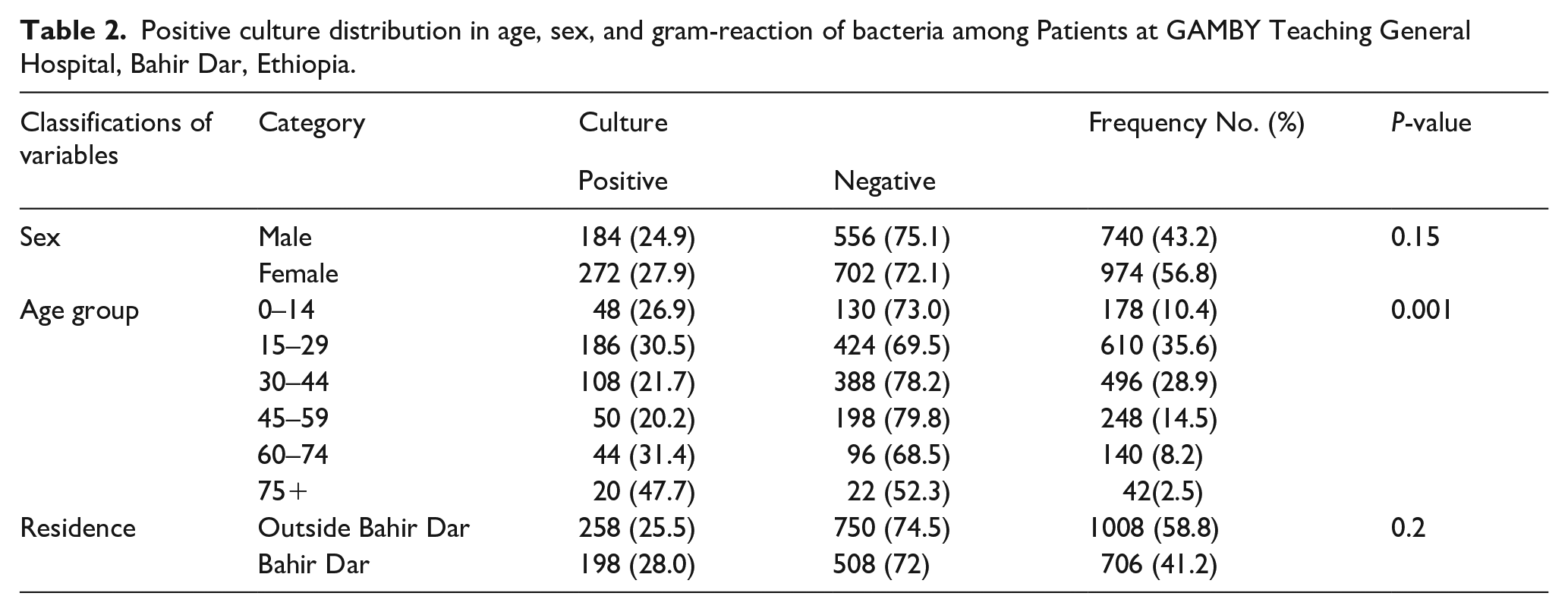
The overall number of UTI patients with culture-positive urine samples was 456 (26.6%), whereas 1258 (73.4%) were culture-negative. Among culture-positive urine samples, there were 116 (25.4%) Gram-positive isolates and 340 (74.6%) Gram-negative isolates, which was the most prevalent isolated strain. Analysis of culture-positive infection with regards to the age groups affected showed that major incidence was recorded in the age group between 15 and 29, which was 186 (40.8%); followed by age between 30 and 44, 108 (23.7%), and the third was between age 45 and 59, 50 (11%). The least culture-positive infection was seen in the age group above 75, which was 20 (4.4%).
The rate of culture-positive isolation among females was 272 (27.9%) and among males was 184 (24.9%). Among the culture-positive samples found, female patients constituted 59.7% and male patients constituted 40.3%. The age group 75 and above had the highest ratio of culture-positive UTIs from the total number of patients in that age group (47.7%), followed by 60–74 (31.4%) and 15–29 (30.5%) as shown in Table 2.
Positive culture distribution in age, sex, and gram-reaction of bacteria among Patients at GAMBY Teaching General Hospital, Bahir Dar, Ethiopia.
According to the relative organism proportion of culture-positive UTI isolates, E. coli was found in 276 (60.5%) culture-positive cases and was the most prevalent isolated bacteria; followed by S. saprophyticus, which is responsible for 78 (17.1%) culture-positive cases. Other less common organisms found were as follows: S. aureus was found in 30 (6.6%) cases, Citrobacter Spp was found in 30 (6.6%) patients, and Klebsiella spp was found in 30 (6.6%) cases as shown in Table 3.
Bacterial isolates from urine samples of patients with UTI among Patients at GAMBY Teaching General Hospital, Bahir Dar, Ethiopia.
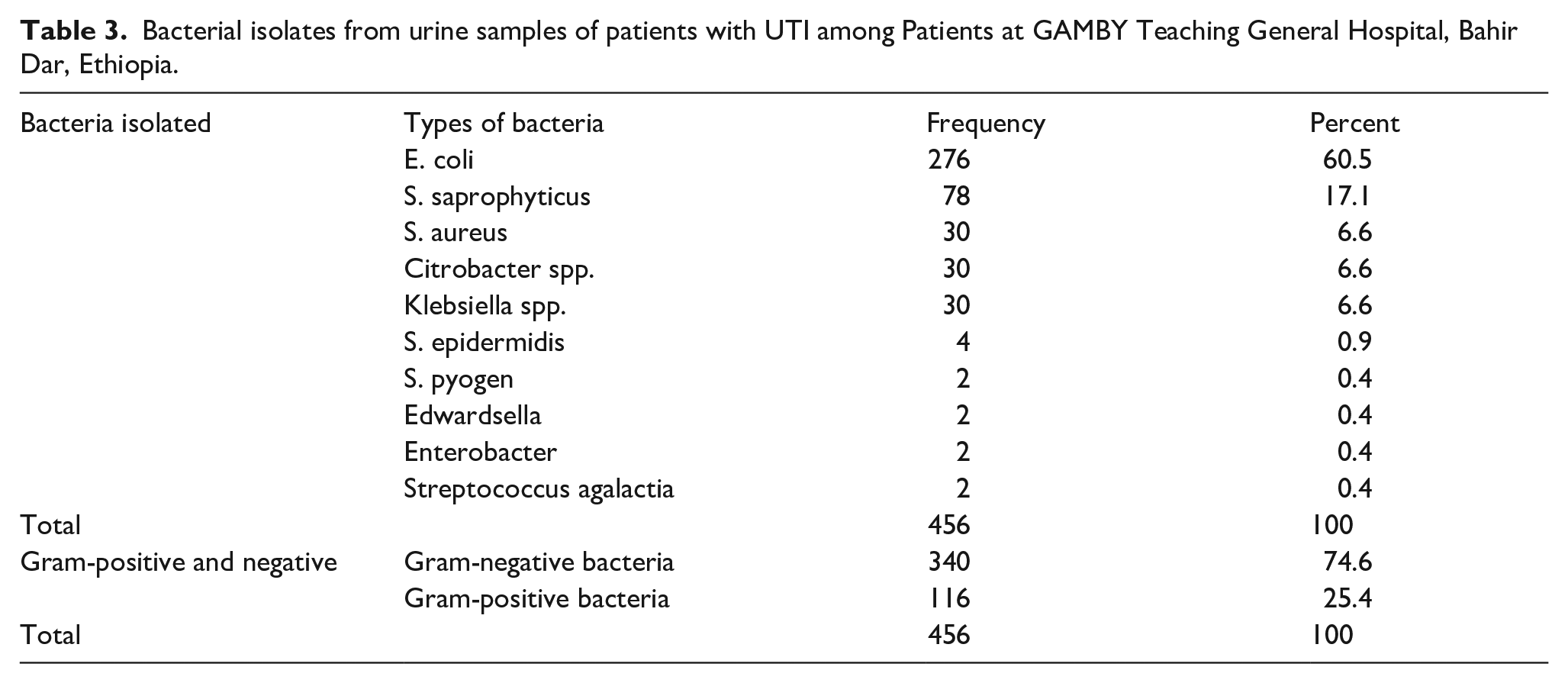
The prevalence of culture-positive UTI due to S. pyogen and Citrobacter were higher in males than in females, but the prevalence of UTI due to S. saprophyticus, E. coli, Enterobacter Spp, and Klebsiella spp, S. epidermidis, Edwardsella, S. aureus, and streptococcus agalactia is higher in women than in men. 340 (74.6%) of isolated bacteria were Gram-negative, while 116 (25.4%) were Gram-positive.
Antibiotic susceptibility pattern
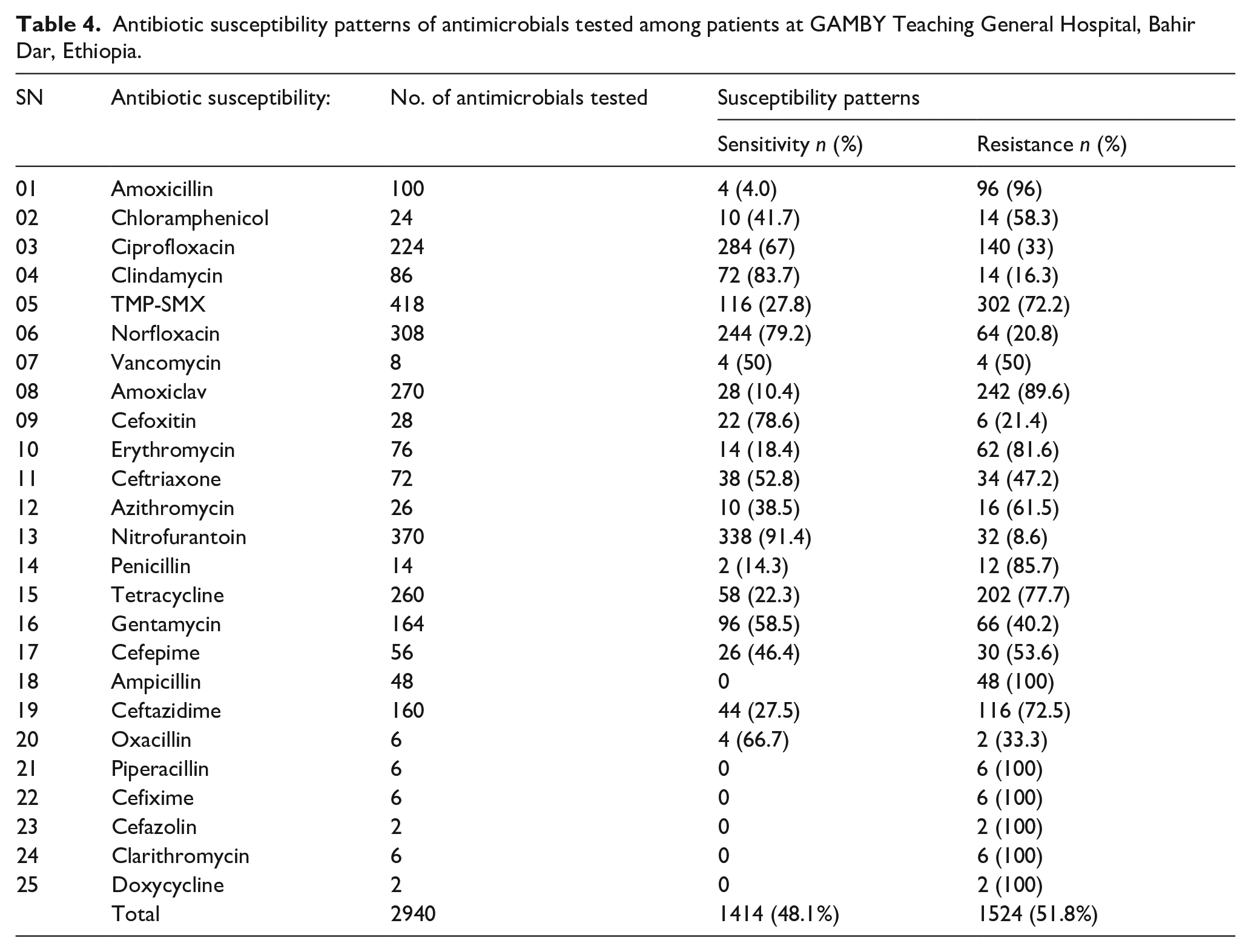
The susceptibility pattern of microorganisms that grew in our laboratory to different antimicrobial agents showed the following patterns: sensitivity to Nitrofurantoin was seen in 338 (91.4%) cultures tested, sensitivity to Clindamycin was seen in 72 (83.7%) cultures tested, sensitivity to Norfloxacin was seen in 244 (79.2%) cultures tested, sensitivity to Cefoxitin was seen in 22 (78.6%) cultures tested, sensitivity to Ciprofloxacin was seen in 284 (67%) cultures tested, and sensitivity to Oxacillin was seen in 4 (66.7%) cultures tested. The International guideline of uncomplicated UTI management recommends to use of Nitrofurantoin, TMP-SMX, and Fosfomycin as a first-line empiric treatment. However, testing for sensitivity of Fosfomycin was not done because it was not available in our institution and it was not practiced readily. As for TMP-SMX, our study showed a significant resistance 302 (72.2%) which is different from what the guidelines state. Even though further study will be needed to analyze why such a significant difference exists one likely reason might be due to the irrational use of this antibiotic. As our study showed above, Nitrofurantoin by far (91.4%) was the most important antimicrobial agent to which microorganisms were sensitive, and growth on the culture media was significantly inhibited.
On the contrary, the resistance pattern of all isolates to the antimicrobial agents was as follows: resistance to Ampicillin was seen in 48 (100%) cultures tested, resistance to Piperacillin was seen in 6 (100%) cultures tested, resistance to Cefixime was seen 6 (100%) cultures tested, resistance to Clarithromycin was seen in 6 (100%) cultures tested, resistance to Amoxicillin was seen in 96 (96%) cultures tested, resistance to Amoxicillin/clavulanic acid was seen in 242 (89.6%) cultures tested, resistance to Penicillin was seen in 12 (85.7%) cultures tested, resistance to Erythromycin was seen in 62 (81.6%) cultures tested, resistance to Tetracycline was seen in 202 (77.7%) cultures tested, resistance to Ceftazidime was seen in 116 (72.5%) cultures tested, and resistance to Co-Trimoxazole was seen in 302 (72.2%) cultures tested. The percentage of pathogens resistant to antimicrobial agents varied between (100 %) and (20.8%) while the susceptibility of pathogens varied between (91.4%) and (0%) as shown in Table 4.
Antibiotic susceptibility patterns of antimicrobials tested among patients at GAMBY Teaching General Hospital, Bahir Dar, Ethiopia.
As shown in Table 5, E. coli showed the lowest percentage of resistance to Nitrofurantoin 236 (3.4%), Cefazolin 22 (9.1%), Amoxicillin/clavulanic acid 180 (11.1%), Cefixime 22 (18.2%), and Erythromycin 18 (22.2%). The highest resistance was seen to Penicillin 6 (100%), Doxycycline 2 (100%), Oxacillin 2 (100%), Ampicillin 34 (100%), Penicillin 6 (100%), Amoxicillin 72 (97.2%), Norfloxacin 212 (79.2%), Clindamycin 8 (75%), Co-Trimoxazole 256 (70.3%), Tetracycline 154 (75.3%), and Ceftazidime 116 (74.1%).
Antibiotic Susceptibility of UTI Isolated bacteria among patients at GAMBY Teaching General Hospital, Bahir, Ethiopia.
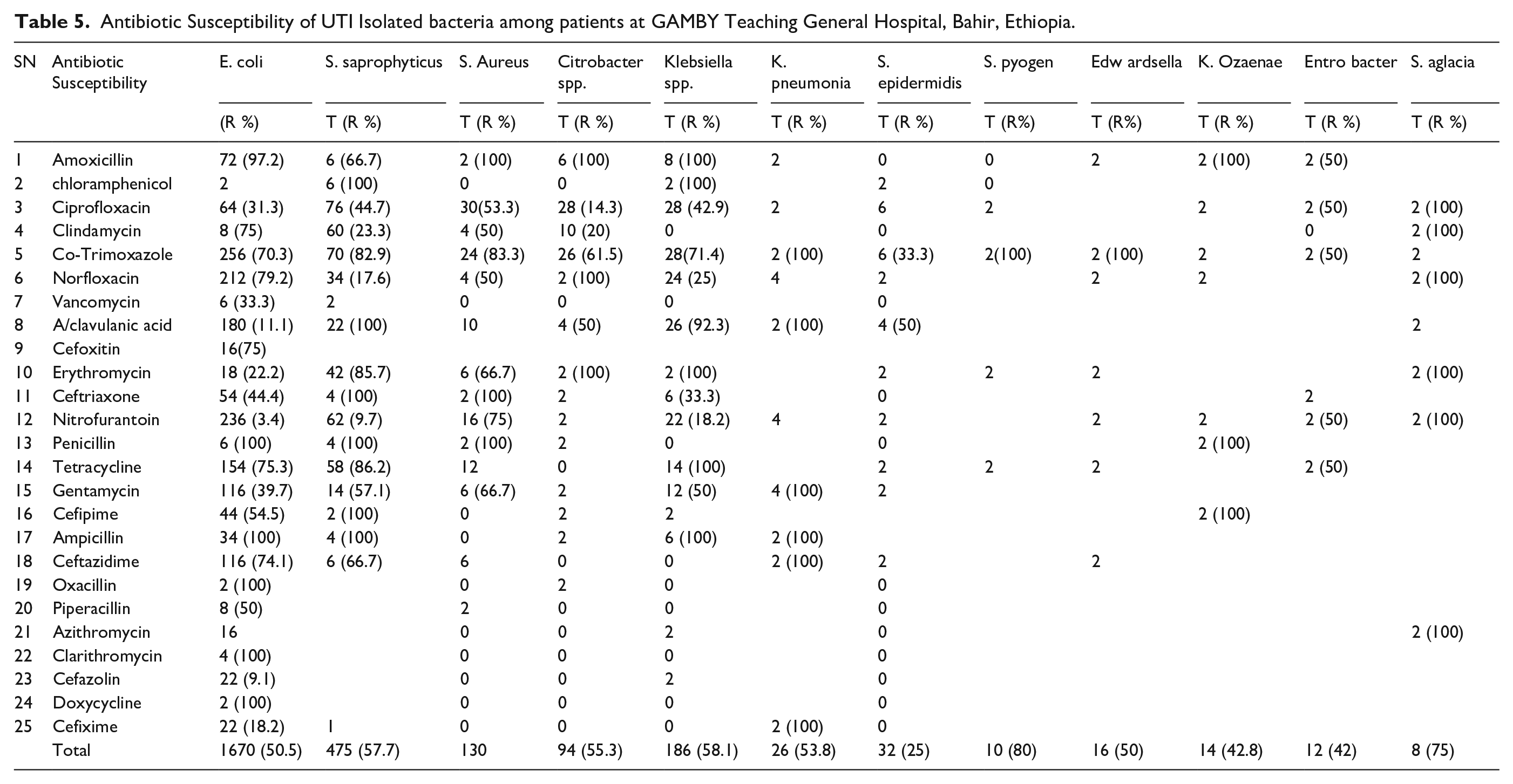
S. saprophyticus showed the lowest percentage of resistance to Nitrofurantoin 62 (9.7%), Norfloxacin 34 (17.6%), and Clindamycin 60 (23.3%). The highest resistance was seen to chloramphenicol 6 (100%), Amoxicillin/clavulanic acid 22 (100%), Cefepime 2 (100%), Ampicillin 4 (100%), Co-Trimoxazole 70 (82.9%), Erythromycin 42 (85.7%), Tetracycline 58 (86.2%), and Ceftazidime 06 (66.7%).
S. aureus showed the highest percentage of resistance to Penicillin 2 (100%), Ceftriaxone 2 (100 %), Amoxicillin 2 (100%), Co-Trimoxazole 24 (83.3%), Nitrofurantoin 16 (75%), and Gentamycin 6 (66.7%).
Citrobacter spp. showed the highest percentage of resistance to Amoxicillin 6 (100%), Norfloxacin 2(100%), Erythromycin 2 (100 %), and Co-Trimoxazole 26 (61.5%).
Klebsiella spp. Showed the highest percentage of resistance to Amoxicillin 8 (100 %), Chloramphenicol l2 (100%), Erythromycin 2 (100%), Tetracycline 14 (100%), Ampicillin 6 (100 %), and Amoxicillin / clavulanic acid 26 (92.3%).
K. pneumonia Showed the highest percentage of resistance to Co-Trimoxazole 2 (100%), Amoxicillin/clavulanic acid 2 (100%), Gentamycin 4(100), Ceftazidime 2 (100), and Cefixime 2 (100).
S. pyogen Showed the highest percentage of resistance to Co-Trimoxazole 2 (100%).
K. ozaena Showed the highest percentage of resistance to Amoxicillin 2 (100 %), Cefepime 2 (100%), and Penicillin 2 (100%).
S. agalactia Showed the highest percentage of resistance to Ciprofloxacin 2 (100%), Clindamycin, 2 (100%), Norfloxacin 2 (100%), Erythromycin 2 (100%), Nitrofurantoin 2 (100%), and Azithromycin 2 (100%).
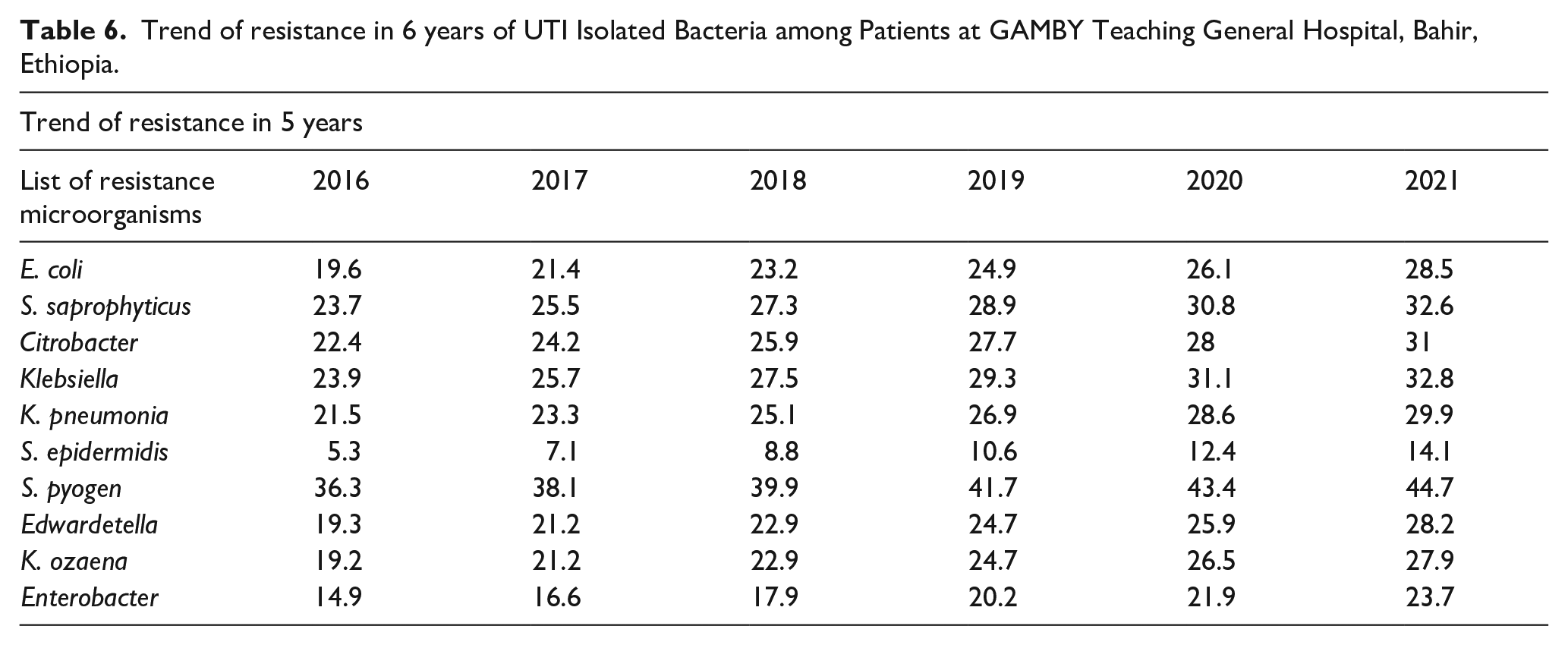
As the data in Table 6 shows, the trends of antibiotic resistance over the past 5 years were increased in each of the microorganisms that was found to cause UTIs. The data clearly stated that the increment of the resistance patterns was significant. In the two most important causes of UTI, E. coli and S. saprophyticus, the average resistance pattern was increased from 19.6 to 28.5 and 23.7 to 32.6 respectively.
Trend of resistance in 6 years of UTI Isolated Bacteria among Patients at GAMBY Teaching General Hospital, Bahir, Ethiopia.
Discussion
Urine culture was one of the most commonly requested specimens for culture and antibiotic sensitivity testing from our hospital's outpatient, inpatient, and emergency departments. This suggests that UTI is a common health problem in our setup.
Our study revealed that the prevalence of Uropathogens was 26.6%. Other studies showed an approximate result in Bahir Dar, Ethiopia with a prevalence of 30.5% whereas in the nearby town, Gondar, the prevalence was found to be 52.8 %.17–19 The most similar finding was found in Northern Ethiopia where the prevalence was found to be 28.5%. 20
The largest number of culture-positive patients were females 272 (59.6%). Their higher tendency to acquire this infection is mainly due to the anatomical proximity of the genital area and the anal region and the urethra is shorter and more radially transversed. 21 In the study area, females had more UTIs than males as was found in similar studies.
Considering the age groups tested, the highest prevalence was found in the age group between 15 and 29, 186 (40.8%) as most of the research was done on UTI. This is mainly because this age group is sexually active, which is one of the most important risk factors for developing an infection. 22 Approximately 60% of women will develop at least one symptomatic UTI during their lifetime, with higher rates of infection observed among sexually active females. 23
Among the uropathogens detected, the predominant type was Gram-negative bacteria, which accounted for 74.6 % of cases followed by Gram-positive bacteria (25.4%). E. coli was by far the most frequent Gram-negative strain identified (60.5%), followed by Citrobacter spp. (6.6%), and Klebsiella spp. (6.1%). Among Gram-positive isolates, S. saprophyticus (17.1%) was the most frequently isolated strain followed by S. aureus (6.6%). The prevalence was comparable to other studies done in different countries. All of the three most common causes of UTI in our study were biofilm producers. Biofilm is an extracellular material that increases the chance of surface attachment and decreases immune control thereby increasing the chance of multidrug-resistant strain. S. Saprophyticus is one of the most common gram-positive biofilm-producing uropathogens and biofilm production is one of the reasons for the higher resistance to the common antimicrobial available in our setup.
In our study, E. coli was found to be responsible for 60.5% of the cases among the culture-positive UTIs. This finding was lower as compared to the study done in Kenya (62%), Tanzania (66.7%), Uganda (70.8%), and India (69.23%).24–27 Moreover, lower frequencies were found in Riyadh Region (43.63%) and Taipei (41.2%).
The prevalence of S. saprophyticus in this study (17.1%) was higher than the finding in Northwest Ethiopia (12.6%). 28 Other comparative studies showed different frequencies such as Southwest Ethiopia (14.3%), 29 Northeast Ethiopia (23.07%), 30 Nigeria (30%), Southern Ethiopia (32.6%), 31 and Ethiopian Public Health Institute (52.4%). 30
In our study, the prevalence of S. aureus was 30 (6.6%). A similar finding was found among Pregnant Women in North West Ethiopia (8.6%). 32 Other comparative studies showed different frequencies such as Gondar 10 %, 33 Eastern Ethiopia (11.1%), 34 Southwest Ethiopia (17.9%), 35 and Gondar Hospital 18.0%, 36 and a much higher frequency is found in Felege Hiwot referral hospital, Ethiopia (61.9%). 37 Generally, the incidence of UTIs due to gram-positive uropathogens has been increasing and it is partly because of the increased unsafe sexual activity in young females and initiation of sexual activities at a younger age. The increased genitourinary procedures for diagnostic and treatment purposes in both sexes also contribute to the higher prevalence of gram-positive related UTIs.
Nitrofurantoin (91.4%), Clindamycin (83.7%), and Norfloxacin (79.2%) were among the antimicrobials to which the uropathogens showed susceptibility. Of the three drugs, Nitrofurantoin (91.4%) was the most frequent drug to which the uropathogens showed susceptibility. Our study showed a lower rate of susceptibility pattern in Northwest Ethiopia (97.7%) 38 and Addis Ababa, Ethiopia (100%). 39
The resistance patterns of all isolates to the antimicrobial agents were: Ampicillin 48 (100%), Piperacillin 6 (100%), Cefixime 6 (100%), Clarithromycin 6 (100%), and Amoxicillin 96 (96%).
Limitations of the study
This study may not represent the general population of Bahir Dar and because of the nature of the study, different risk factors responsible for anti-microbial resistance were not analyzed. In addition, only those commonly used antibiotics in the institution were tested. Hence, it didn’t include all the standard antibiotics recommended in the management of UTIs. The study also lacks further analysis of the prevalence of ESBL.
Conclusion
The prevalence of UTI in the study area was 26.6%. E. coli was the highest responsible pathogen (60.5%) among the culture-positive isolates. Females had a higher 272 (59.6%) prevalence of UTI than male counters 184 (40.4%). Almost all isolates were sensitive to nitrofurantoin 91.4%, and most of the isolates were sensitive to Clindamycin 83.7%, Norfloxacin 79.2%, and Cefoxitin 78.6%. Higher resistance was observed in Ampicillin 100%, Piperacillin 100%, Cefixime 100%, Clarithromycin 100%, Amoxicillin 96 96%, Amoxicillin/clavulanic acid 242 (89.6%), Penicillin 85.7%, and Erythromycin 81.6%.
Footnotes
Acknowledgements
The authors are grateful to GAMBY Medical and Business College for their permission to conduct the study in GAMBY Teaching General Hospital and support for culture media, biochemical tests, and antibiotic discs. We are sincerely grateful to the leadership commitment of the organization as a whole and in the department of medical laboratory. We are also grateful to all the staff of the medical laboratory department for their contribution with regard to sample collection, processing, analysis, and reporting.
Abbreviations
UTI, Urinary tract infection, ATCC, American Type Culture Collection; HMIS, Hospital Management Information System; CLSI: Clinical and Laboratory Standards Institute.
Author Contributions
All authors made a significant contribution to the work reported; in the conception, study design, execution, acquisition of data, analysis and interpretation, drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article was submitted; and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The data used and/or analyzed during the current study are available from the corresponding author and could be forwarded upon request (Adugna Tasew: