
Abstract
Purpose:
A retrospective study was performed to identify potential metabolic abnormalities and inflammatory abnormalities associated with benign prostatic hyperplasia (BPH) secondary to bladder calculi.
Materials and Methods:
This study enrolled 646 patients with bladder calculi between 2008 and 2022, including 314 patients with benign prostatic hyperplasia (BPH) and 332 without BPH. Demographic characteristics, serum biochemical parameters, prostate volume, maximum bladder calculus diameter, and randomized urinary metabolic profiles were compared between the two groups.
Results:
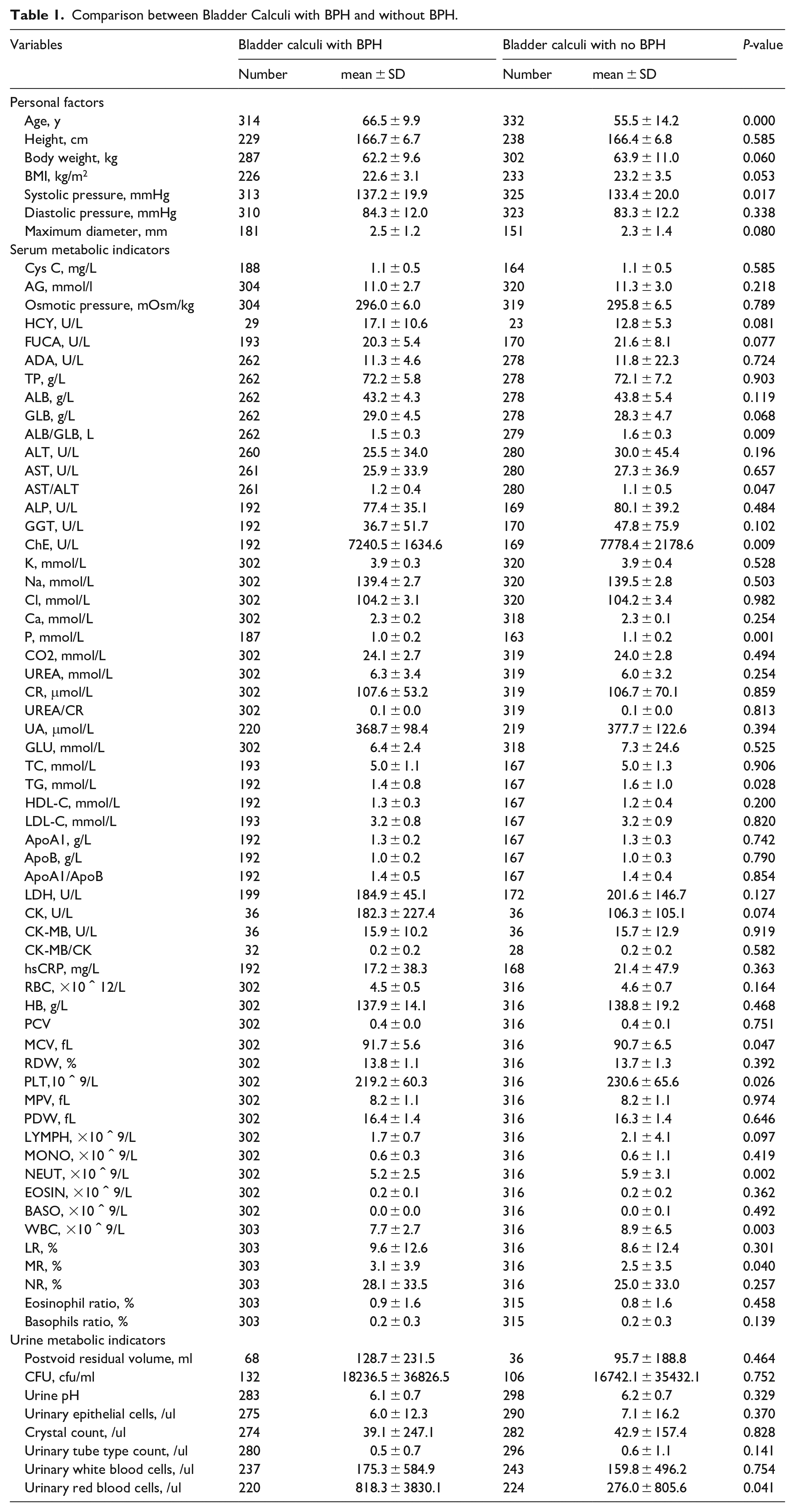
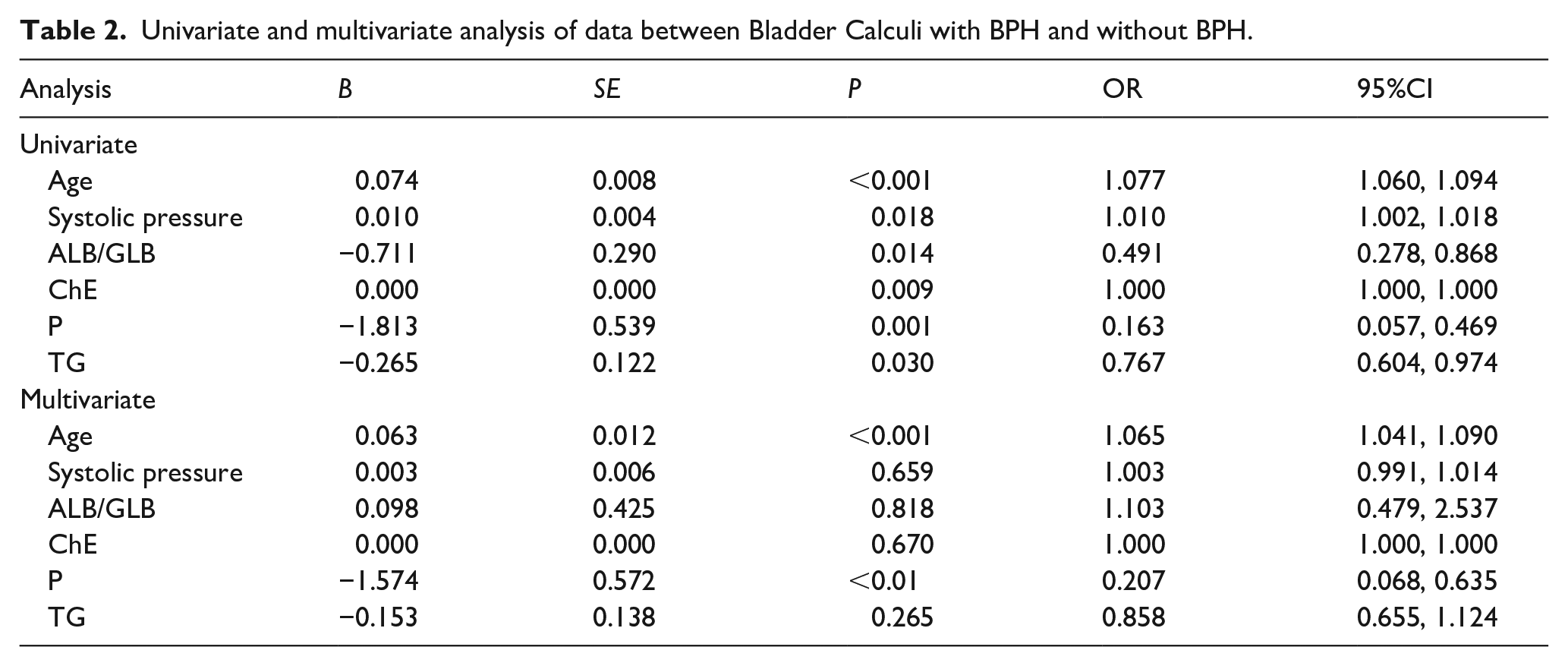
BPH was associated with increased aspartate aminotransferase/alanine aminotransferase (mean 1.2 vs 1.1, P < 0.05), lower cholinesterase (mean 7240.5 vs 7778.4, P < 0.01), increased systolic pressure (mean 137.2 vs 133.4, P < 0.01). Patients with BPH were significantly older and had higher systolic blood pressure compared to non-BPH patients. BPH group exhibited significantly lower levels of albumin/globulin ratio, cholinesterase, phosphorus, triglycerides, platelet count, neutrophil count, and white blood cell count, while demonstrating higher aspartate aminotransferase/alanine aminotransferase ratio, mean corpuscular volume, monocyte ratio, and urinary red blood cell count. Prostate volume was proportional to body weight and crystal count. Lower phosphorus (OR = 0.207; 95%CI = 0.068, 0.635; P < 0.01) and higher age (OR = 1.065; 95%CI = 1.041, 1.090; P < 0.001) were associated with BPH.
Conclusions:
Advanced age was identified as a significant risk factor for prostate hyperplasia in patients with bladder calculi, whereas elevated phosphorus levels emerged as a protective factor. The pathogenesis of BPH secondary to bladder calculi appears to be multifactorial, primarily influenced by metabolic abnormalities and inflammatory processes. These findings provide valuable insights for the clinical assessment and management of BPH secondary to bladder calculi.
Introduction
Benign prostatic hyperplasia (BPH) has historically been associated with bladder calculi,1,2 which incidence was 3% to 10% in patients with BPH.3–5 As common conditions in urological practice, 5 bladder calculi and BPH would lead a decreased quality of life.6,7 Currently, most of the literature has explored the risk factors of bladder calculi following operation for BPH. And it was generally accepted that bladder calculi were affected by BPH.1,3,4 Childs et al. prospectively analyzed the metabolic differences of patients with bladder calculi secondary to BPH and found that metabolic abnormalities (lower urinary pH and magnesium, and higher uric acid supersaturation) could result in BPH patients suffering from bladder calculi. 3 However, the metabolic factors and inflammatory factors leading to BPH have not been well explored, especially in patients secondary to bladder calculi. Recently, multifactorial aetiology of bladder calculi questioned the conventional belief that bladder calculi are the primary indication for prostatic surgery.5,6,8,9 Whereas the formation of BPH secondary to bladder calculi was complex and multifactorial for a unique group of patients with abnormal urinary microenvironment, inflammatory indicators, and metabolism.1,10–14 The hormone abnormalities that interacted with inflammatory indicators were not sufficient to explain the pathogenesis of BPH. 10 On the contrary, it was the additive effect of potential inflammatory and metabolic abnormalities that contributed to BPH in patients with bladder calculi. Hence, patients with bladder calculi with and without BPH before treatment or surgery were retrospectively compared to identify potential metabolic abnormalities, personal factors, and inflammatory abnormalities.
Methods
Study population
We designed a retrospective study, from September 2008 to July 2022. A comparative analysis was performed on 646 patients diagnosed with bladder calculi, with or without BPH. They were categorized into 2 groups: Group 1 had BPH, and Group 2 did not. All procedures performed in the study conformed to the 1964 Declaration of Helsinki and its subsequent revisions, or similar ethical standards. The primary aims were to identify serum, urinary metabolite, and inflammatory differences in the BPH group.
Inclusion criteria and exclusion criteria
Patients older than 18 years old were enrolled if they were diagnosed with bladder calculi at our hospital. Exclusion criteria: patients were excluded if they had a confirmed neurogenic bladder, bladder foreign body, or history of other lower urinary calculi (e.g. ureteral calculus).
Clinical data
After enrollment, demographic and clinical information was collected retrospectively, including medical history (urinary condition, complicated diseases), personal habits (smoking status), maximum diameter of bladder calculi, prostate volume, postvoid residual volume, random urine composition (urine pH, urinary epithelial cells, crystal count, urinary tube type count, urinary white blood cell et cetera), serum electrolytes and metabolites such as potassium (K), sodium (Na), and lactate dehydrogenase (LDH). The total prostate volume and the maximum diameter of bladder calculi were measured on patients in the supine position by the same physician using transabdominal ultrasonography. The above clinical data were collected preoperatively and pretreatment.
Statistical analysis
Statistical analysis was performed using SPSS, version 26. Data are presented as the mean ± standard deviation (SD). Continuous variables were compared across study groups using the Student t test or the Mann–Whitney U test. A multivariate logistic regression analysis model was used to further analyze the factors with statistical differences in single factor analysis. Tests were two-sided and considered significant at P < 0.05. Pearson correlation analysis was adopted for correlation analysis of measurement data.
Ethics and regulatory oversight
As a retrospective analysis of treatment data, prospective design and registered clinical trials were not included in this study. The government also did not convene a data security monitoring committee to oversee the study.
Results
This study enrolled 646 patients with bladder calculi, patients with BPH were classified as Group 1 (n = 314) and patients without BPH were classified as Group 2 (n = 332). Table 1 compares the differences between the urine metabolic indicators, serum metabolic indicators, and personal conditions of two groups. Obviously, Group 2 had a lower age, maximum diameter of the bladder calculi, systolic pressure. Comparing with Group 2, urinary red blood cells of Group 1 were higher. However, in comparison of the number of inflammatory indicators between the two groups, Group 1 presented with higher monocyte ratio (MR), mean red cell volume (MCV) and lower blood platelet count (PLT), neutrophil count (NEUT), white blood cell count (WBC). On the other hand, Group 1 showed lower albumin/globulin (ALB/GLB) ratio, cholinesterase (ChE), phosphorus (P), and triglyceride (TG) among blood component content. In contrast, Group 1 showed higher aspartate aminotransferase/alanine aminotransferase (AST/ALT) ratio (Table 1). Univariate and multivariate analysis showed that age was an independent risk factor for prostate hyperplasia in patients with bladder calculi, while P was an independent protective factor (Table 2). As the remaining data were not significant or of little practical significance, they were not described in detail.
Comparison between Bladder Calculi with BPH and without BPH.
Univariate and multivariate analysis of data between Bladder Calculi with BPH and without BPH.
Correlation analysis of metabolic markers and basic information
To assess the concordance in values between indicators more formally, we used the Pearson correlation coefficient to describe the correlation of some indicators (personal factors, serum electrolytes, colony-forming unit (CFU), urine pH, urine composition). In Figure 1, we visualize the results of this analysis via a clustered correlation heatmap.
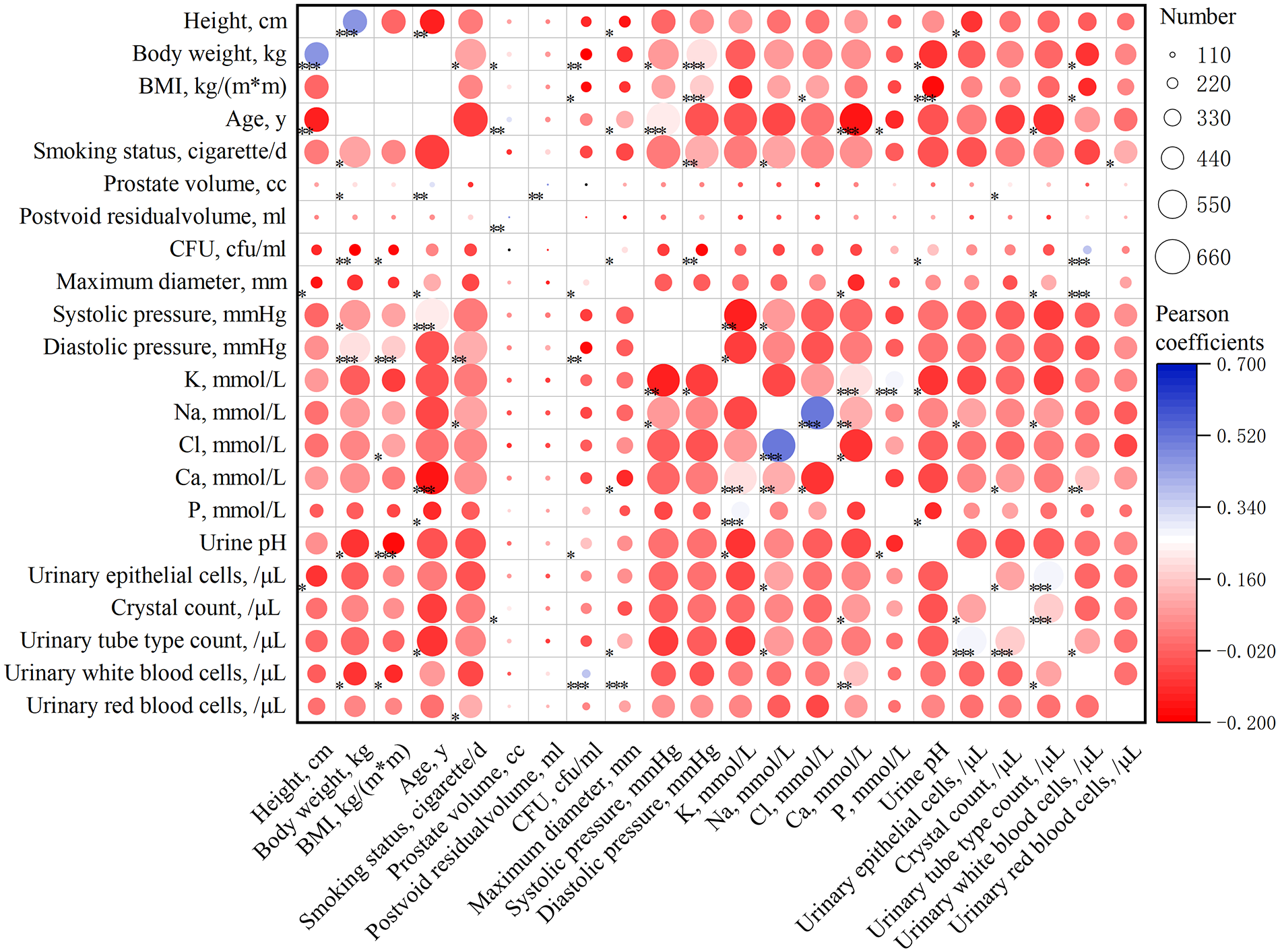
Correlation analysis of metabolic markers and basic information.
Shown is a clustered correlation heatmap of consistency in values between indicators. The color coding depicts Pearson coefficients. Blue represents a positive correlation, while red represents a negative correlation. As the color becomes darker, the correlation between indicators becomes stronger. The size of the bubble describes the number of cases analyzed. A “*” indicates a P-value less than 0.05, “**” indicates a P-value less than 0.01, and “***” indicates a P-value less than 0.001 (Figure1).
Correlation analysis of urine metabolism indices
To visualize the variables of interest, the associations are presented by graphs. Urine metabolism index, urine pH and urinary white blood cells were included to explore the potential metabolic abnormalities of urine components. The results showed a consistent negative correlation, although the Pearson coefficients of urine pH with body weight, body mass index (BMI), K and P were different. Urinary white blood cells, between which and calcium (Ca) there existed a positive correlation, was otherwise negatively correlated with body weight (Figure 2).
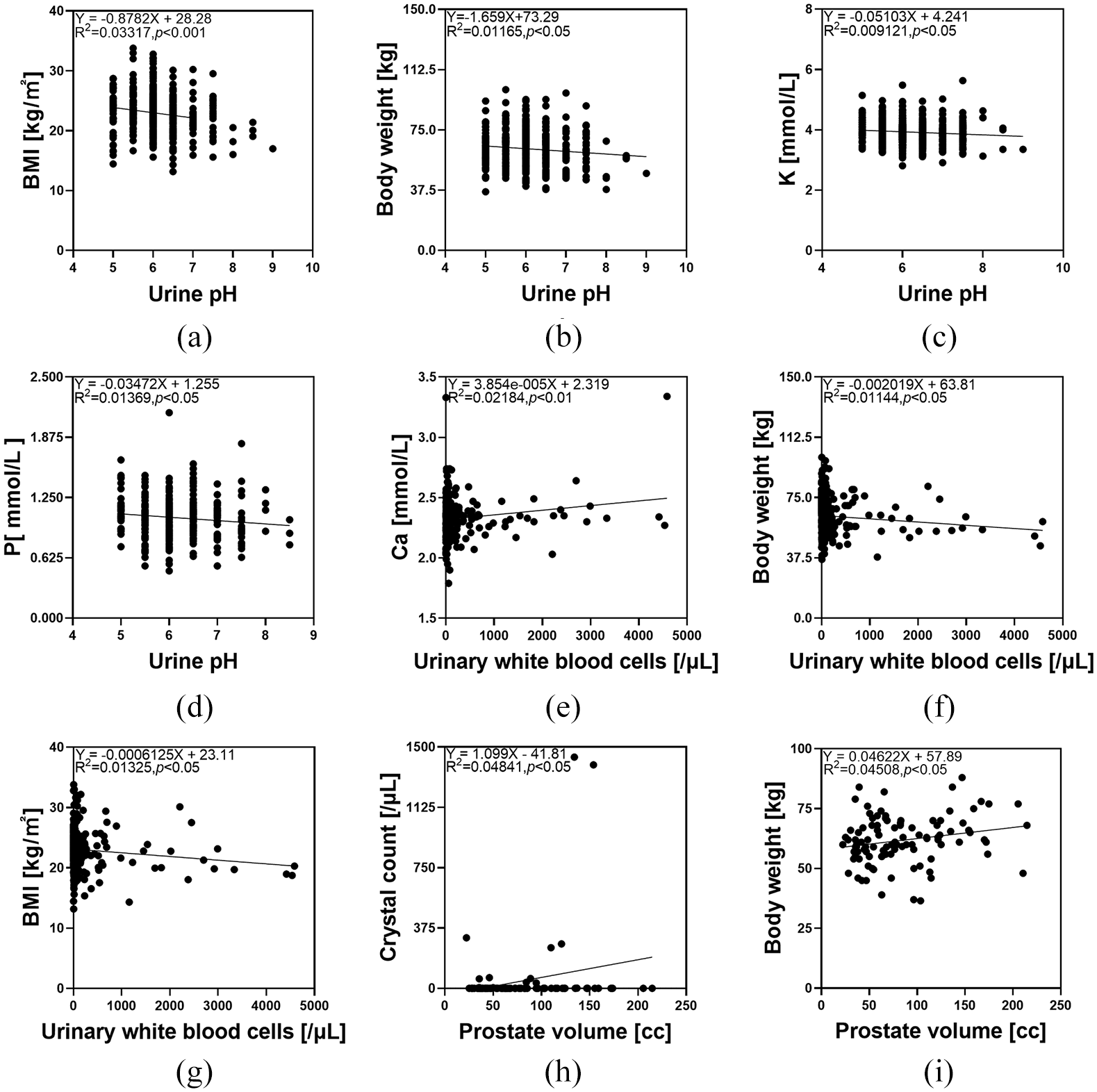
Correlation analysis of urine metabolism indices, prostate volume. a-g shows the correlation of urine metabolism indices. h-i shows the correlation of prostate volume. R2 represents the degree of correlation between the two variables. A p-value less than 0.05 is considered to indicate statistical significance.
Correlation analysis of prostate volume
Additionally, we used the coefficients from our generalized linear models to create regressions for postvoid residual volume, body weight, and crystal count as functions of the prostate volume. A correlation was found between prostate volume and postvoid residual volume (r = 0.452, P = 0.007), body weight (r = 0.212, P = 0.033), and crystal count (r = 0.22, P = 0.041) (Figure 2).
Discussion
The metabolic abnormalities were reported in the pathogenesis of BPH.11–13,15 Hormones, inflammation, metabolic syndrome, diabetes mellitus, proliferative arousal, lifestyle factors, obesity, stem cells, and telomerase pathways have been proposed to contribute to the pathogenesis of BPH.10,12,16–19 However, the pathogenesis of BPH in patients with bladder calculi has not been well studied. We retrospectively assessed demographic and clinical information of patients suffering from bladder calculi with and without BPH before treatment or surgery. Compared with patients with bladder calculi alone, the age distribution and systolic pressure of patients with BPH and bladder calculi were significantly higher, which had been widely mentioned in past studies.13,20 We also found that age was an independent risk factor for prostate hyperplasia in patients with bladder calculi. Furthermore, abnormalities in serum electrolyte and metabolite studies were more common in cases. In patients with BPH, we found higher AST/ALT, MCV, MR, and urinary red blood cells, as well as lower ALB/GLB, ChE, P, TG, PLT, NEUT, and WBC. In an observational study, high TG and high BMI were associated with the risk of BPH,13,17 but the difference in BMI was not significant in our study. Therefore, the results should be interpreted with caution due to the small number of included patients. Furthermore, although the revealed correlation did not imply causality, and the correlation of most parameters with BPH has not been reported. These findings suggested that metabolic abnormalities could contribute to BPH.
A previous study suggested that infection and inflammation affect the prostate, and inflammation may interact with androgen.10,14 Therefore, our findings of lower PLT, NEUT, WBC, and higher urinary red blood cells, MCV, and MR in patients with BPH quantitatively and more strongly support the role of infection and abnormal inflammation in BPH. However, the pathophysiological mechanism of the above abnormal inflammatory indicators has not been fully elucidated. It is well known that androgen is essential for the growth of the prostate, and the latest view is that low levels of testosterone (TT) is a risk factor for BPH.10,19,21,22 A cross-sectional study revealed that TG and gamma-glutamyl transferase (GGT) are related to TT, which is one of the main components of androgen. 23 In addition, ALB has also been shown to exist in combination with TT. 24 It has been found that TT has a positive correlation with ChE. 25 In two retrospective cohort studies, high TT was accompanied by high ALT and low AST.26,27 Therefore, the discovery of lower ALB/GLB, lower ChE, and higher AST/ALT in patients with BPH indicates lower TT, which more appropriately supports the role of metabolic abnormalities in the occurrence of BPH. Research has developed a tool, referred to as the fatty liver index, based on BMI, waist circumference, levels of TG, and GGT level. 23 Their study found a significant negative correlation between fatty liver index and TT. 23 Although they did not clearly point out the correlation between TG and TT, GGT, and TT, our research shows that there is a positive correlation between TG and TT, but the correlation between GGT and TT is not strong. In conclusion, our study considers that the abnormalities of these enzymes are also related to TT, thus affecting prostate hyperplasia. Further BPH studies are needed to confirm the exact etiologic mechanism. Causal relationship between elevated BMI and increased risk of BPH was reported. 17 Despite the potential factors of different crystal components in the urine microenvironment, we found that prostate volume is proportional to body weight, which clearly showed the relationship between obesity and BPH. 13 Moreover, we found a proportional relationship between prostate volume and crystal count, which was not found in previous studies. A keyword search was carried out in PubMed on urinary crystallization and BPH but found no relevant research exploring the correlation between the two. Above all, we suspected that the number of crystals might play a role in BPH.
Androgen was also related to the expression of Ca and electrolyte transporters. 28 As a non-metallic element, high serum P levels cause gonadotrophins to suppress TT. Conversely, low K has also been shown to inhibit the release of TT. 29 It has been found that TT level was negatively correlated with 24-h urine Na. As an essential element of human body, the sum of serum Na and 24-h urine Na was relatively stable, so TT level was positively correlated with serum Na. 30 Our study revealed that P was significantly higher in Group 2 than Group 1, which was consistent with the finding of previous study. 31 In addition, our study further indicated that P was an independent protective factor for BPH in patients with bladder calculi, indicating that the lack of P was closely related to BPH. Therefore, the correlation coefficient between urine pH, urine white blood cells, and serum K, serum P, and serum Ca also suggested that inflammation and urine microenvironment affect prostate hyperplasia through hormone regulation. However, the exact mechanism remained unclear.
One limitation of our study was that we did not evaluate hormones, biomarkers, and other potential factors, such as a prostate-specific antigen. 13 Similar to abnormal urine metabolism, these factors have been identified as factors leading to prostate disease, and they may also be involved in the pathogenesis of BPH. Our findings were limited because of the small scale of the study group and the control group, and missing clinical data was not added with statistical methods. Although this led to a significant reduction in the number of data that can be analyzed, it was conducive to avoided biased results due to statistical laws. Since chronic infection was also a confounding factor, we also evaluated the CFU in urine, but the types of colonies were always farraginous. Nevertheless, our study innovatively provided further clinical support into the pathogenesis of BPH.
Conclusions
In this retrospective study, age was an independent risk factor for prostate hyperplasia in patients with bladder calculi, while P was an independent protective factor. The pathogenesis of BPH secondary to bladder calculi is multifactorial, which was affected by abnormal metabolism and inflammation. Identifying the multiple factors of BPH secondary to bladder calculi can aid in the assessment and management of etiology, and reduce recurrence rates.
Footnotes
Acknowledgements
Not applicable.
Abbreviations and Acronyms
ADA = Adenosine deaminase, AG = Anion gap, ALB = Albumin, ALT = Alanine aminotransferase, ALP = Alkaline phosphatase, ApoA1 = Apolipoprotein A1, ApoB = Apolipoprotein B, AST = Aspartate aminotransferase, AST/ALT = Aspartate aminotransferase/Alanine aminotransferase, BASO = Basophil count, BMI = Body mass index, BPH = Benign prostatic hyperplasia, Ca = Calcium, CFU = Colony-forming unit, ChE = Cholinesterase, CK = Creatine kinase, CK-MB = Creatine kinase MB, CK-MB/CK = Creatine kinase MB/Creatine kinase, Cl = Chlorine, CO2 = Carbon dioxide, CR = Creatinine, Cys C = Cystatin C, DBIL = Direct bilirubin, EOSIN = Eosinophil count, FUCA = Fucosidase, GCA = Glycocholic acid, GGT = Gamma-glutamyl transferase, GLB = Globulin, GLU = Glucose, HB = Hemoglobin, HCY = Homocysteine, HDL-C = High density lipoprotein cholesterol, hsCRP = High sensitivity C-reactive protein, IBIL = Indirect bilirubin, K = Potassium, LDH = Lactate dehydrogenase, LDL-C = Low density lipoprotein cholesterol, LR = Lymphocyte ratio, LYMPH = Lymphocyte count, MCH = Mean erythrocyte hemoglobin content, MCHC = Mean erythrocyte hemoglobin concentration, MCV = Mean red cell volume, MONO = Monocyte count, MPV = Mean platelet volume, MR = Monocyte ratio, Na = Sodium, NEUT = Neutrophil count, NR = Neutrophil ratio, P = Phosphorus, PCV = Packed cell volume, PDW = Platelet distribution width, PLT = Blood platelet count, RBC = Red blood cell count, RDW = Red blood cell volume distribution width, TBA = Total bile acid, TBIL = Total bilirubin, TC = Total cholesterol, TG = Triglycerides, TP = Total protein, UA = Uric acid, UREA = Urea, UREA/CR = Urea/Creatinine, WBC = White blood cell count.
Authors’ contribution
Lu: Data collection, Manuscript writing
Gao: Data collection, Manuscript writing
Fei: Statistical analysis, Data collection
Liao: Statistical analysis, Data collection
Hou: Statistical analysis, Data collection
Lin: Manuscript editing
Rao: Manuscript editing
Yang: Study design
Sui: Study design
Authors’ information
Not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Shantou Medical Science and Technology Planning Project (Grant numbers [2022-81-22]).
Ethics approval and consent to participate
The study was approved by the ethics committee of Second Affiliated Hospital of Shantou University Medical College (Grant numbers [2022-74]). Informed consent was obtained from all subjects.
Consent for publication
Not applicable.
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.