
Abstract
Objective:
To evaluate the therapeutic effect of acupuncture combined with cross-moxibustion in patients with severe overactive bladder (OAB).
Methods:
OAB patients from August 2018 to July 2023 were collected, and 101 severe OAB patients were selected based on the Overactive Bladder Symptom Scale (OABSS) score. The patients were divided into three groups according to their treatment methods, including 33 cases of behavioral therapy group, 32 cases were in the acupoint acupuncture group, and 36 cases were in the acupuncture combined with cross-moxibustion group. The treatment outcomes of the three groups were evaluated through the OABSS score, and the quality of life (QOL) was assessed.
Results:
Among the 101 patients with severe OAB, no statistical differences in age and gender were observed among the three groups of treatments. The treatment effects were evaluated using the OABSS score and it was found that behavioral treatment was basically ineffective. In contrast, both acupuncture and acupuncture combined with cross-moxibustion had significant differences via comparing at pre-post treatment periods, which the OABSS score decreased by 3.25 ± 1.83 and 7.83 ± 1.34 respectively, suggesting that acupuncture combined with cross-moxibustion is more effective than acupuncture group alone. The patient’s quality of life was further evaluated through QOL scores, and the results showed that while the acupuncture group was effective, acupuncture combined with cross-moxibustion improved more significantly.
Conclusion:
The combination of acupuncture and moxibustion is the most effective treatment for patients with severe overactive bladder.
Keywords
Introduction
Overactive Bladder (OAB) is a syndrome with frequent urination and urgency, with or without urge urinary incontinence, without urinary tract infection or other definite pathological changes. 1 These symptoms significantly impact patients’ social activities, work and overall quality of life.
The incidence of overactive bladder increases with age, and the incidence of female is higher than that of male. According to statistics, the overall incidence of OAB in the United States is approximately 16.6%, 2 while in China, it is about 6.0%. 3 In China, the incidence rate over 40 years old is as high as 11.3%, and the prevalence of OAB continues to rise with age. Women are significantly higher than men. However, because most studies are limited to patients with urinary incontinence, the incidence of overactive bladder may be underestimated. Moreover, with the arrival of aging in China, the prevalence rate and the number of patients will increase greatly.
The etiology of OAB remains unclear, but studies believe that its pathogenesis is related to many factors. Among them, detrusor instability, bladder hypersensitivity, abnormal function of urethra and pelvic floor muscles are considered as the main causes.4,5 In addition, abnormal mental behavior, hormone metabolism disorder and other factors may also affect the occurrence of overactive bladder. Diagnosis is primarily based on the patient’s medical history, physical examination and laboratory test. Among them, urodynamic examination, ultrasonic examination of bladder wall thickness and volume, and routine urine examination are helpful to make a clear diagnosis.
At present, the treatment strategies for OAB include behavioral therapy, pharmacotherapy and surgical interventions.4,6 Behavioral therapy mainly includes bladder training and pelvic floor muscle training, aiming at relieving symptoms by changing urination habits and improving pelvic floor muscle function. In drug therapy, M receptor antagonists, sedatives, antianxiety drugs, and calcium channel blockers are commonly used to relieve the symptoms of overactive bladder. For patients with severe symptoms and poor drug treatment effect, surgical treatment can be considered, such as detrusor transection and intestinal bladder enlargement. Among them, behavior training is not affected by the side effects and compliance of drugs, and it does not need any invasive treatment. These unique advantages make it one of the main treatment methods of OAB. However, in clinical work, many patients with severe symptoms experience limited success with behavioral therapy. However, the Traditional Chinese Medicine (TCM) culture in China is profound, pays attention to comprehensive conditioning, and has few side effects. It is worth investigating its efficacy in patients with OAB, especially those with severe cases. At present, studies have shown that acupuncture therapy has a certain effect on OAB, and its effect is equivalent to that of oral western medicine alone, and it is safer, 7 but the effect of severe OAB patients remains to be verified.
This study aims to investigate the effects of three different treatment modalities (including behavioral therapy, acupuncture therapy and acupuncture combined with cross moxibustion) on patients with severe OAB who are refractory to conventional treatment. By evaluating the effects of these three different treatments, we hope to find a more reasonable and effective treatment method for severe OAB patients and improve their quality of life.
Methods
Subjects
From August 2018 to July 2023, a total of 101 patients with overactive bladder were collected. After auxiliary examination, pelvic floor dysfunction caused by currently known diseases, such as prostatic hyperplasia, cystitis and neurogenic bladder, was excluded. The oldest severe OAB patients are 93 years old and the youngest is 55 years old, with an average age of 75.68 years and a median age of 74 years old. There were 23 males and 78 females. According to different treatment methods, they were divided into three groups, 33 cases in behavioral therapy group; Acupoint acupuncture group: 32 cases; 36 cases in acupuncture combined with cross moxibustion group. See Figure 1 for details.
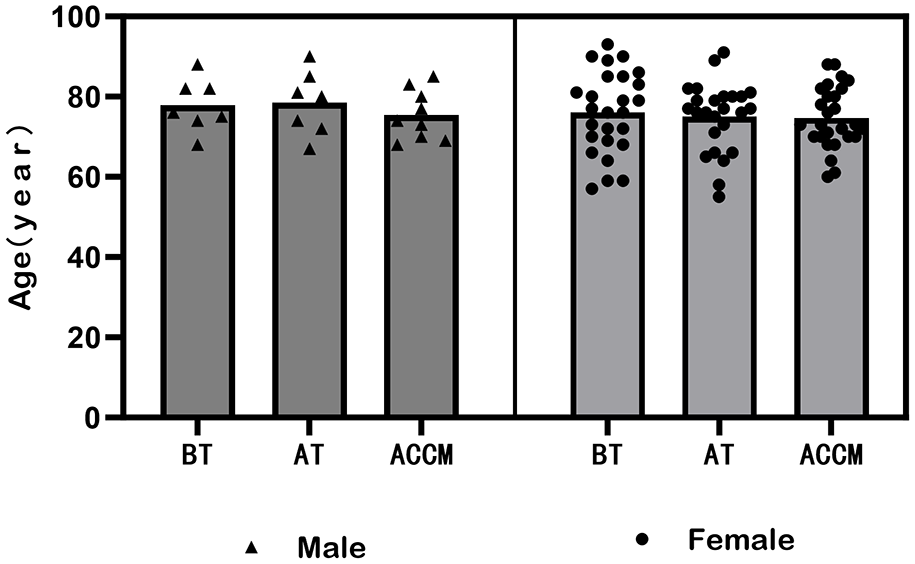
Age and gender related information of 101 patients with OAB.
Group rating scale
According to the overactive bladder scale (OABSS), OAB patients were graded into three types: mild, moderate and severe. Score < =5 is mild; The score of 6=<OABSS<=11 is moderate; OABSS score > =12 is severe. In this study, severe patients were selected, that is, OABSS score > =12. See Table 1 for the detailed scoring contents.
Bladder Hyperactivity Score (overactive bladder syndrome scale OABSS) .

Before and after treatment, the patients were graded according to their feelings about the quality of life, that is, QOL scale. As shown in Table 2, the score is divided into 7 grades from light to heavy. The lower the score, the higher the quality of life and the more significant the curative effect.
Influence of Urination Symptoms on Quality of Life (QOL) table.

Experimental method
A total of 101 patients with severe OAB were divided into three groups: behavioral therapy, acupuncture therapy and acupuncture combined with cross moxibustion. The specific treatment is as follows.
1) Behavioral therapy (BT): Mainly through bladder training, regular urination and pelvic floor muscle training. Bladder training: delay urination by subjective control, and gradually make the amount of urination greater than 300ml each time. Regular micturition: For patients with serious and uncontrollable urinary incontinence, micturition at a specified time can reduce the number of urinary incontinence and improve the quality of life. This method is not suitable for those with severe frequent urination. Pelvic floor muscle training: strengthen pelvic floor muscles and urethral sphincter through specific exercise methods. The treatment period is 15 days.
2) Acupuncture treatment (AT): By selecting relevant acupoints (including Qihai, Guanyuan, Intermediate, Qugu, Shuidao, Guilai, Yinlingquan, Sanyinjiao and Taixi), acupuncture treatment is carried out in a flat way, and the needle retention time is 30 min. The treatment period is 15 days.
3) Acupuncture combined with cross moxibustion (ACCM): the above two methods of acupuncture combined with cross moxibustion are used for treatment, and the total treatment cycle is 15 days. Cross moxibustion was performed on the first day, the eighth day and the fifteenth day respectively, and acupuncture was used for the rest of the time. The specific cross moxibustion method is as follows: the patient lies in the supine position, and the moxibustion range includes Zhongwan, Jianli, Xiawan, Shenque, Tian Shu, Qihai, Guanyuan, Intermediate, Qugu, Shuidao, Huilai, etc. Paving gauze and evenly spreading Chinese herbal medicine powder (Radix Aconiti, Radix Aconiti Kusnezoffii, Herba Ephedrae, Herba Asari, Notopterygii Rhizoma, Radix Angelicae Dahuricae, Cortex Cinnamomi, and Rhizoma Zingiberis) on the gauze. Then spread Jiang Mo (1.5 cm thick and 5 inches wide), after shaping, put moxa sticks on it, ignite and burn three moxa sticks, so that they are evenly heated and slowly infiltrated for 1.5 h.
OABSS and QOL scores were scored before and after treatment.
Statistical analyses
The experimental results were analyzed by SPSS22.0 software, and the data was expressed as “mean standard deviation” (
Results
In this study, severe patients with OAB were divided into the BT group, the AT group and the ACCM group. The average age of patients in the three groups was similar, ranging from 74 to 76 years old. Statistical analysis indicated that there was no significant difference in the age of patients among the three groups (Figure 2(a)). Although the three groups had f fewer male patients and more female patients, there was no significant difference in the ratio of male to female among the three groups (Figure 2(b)).
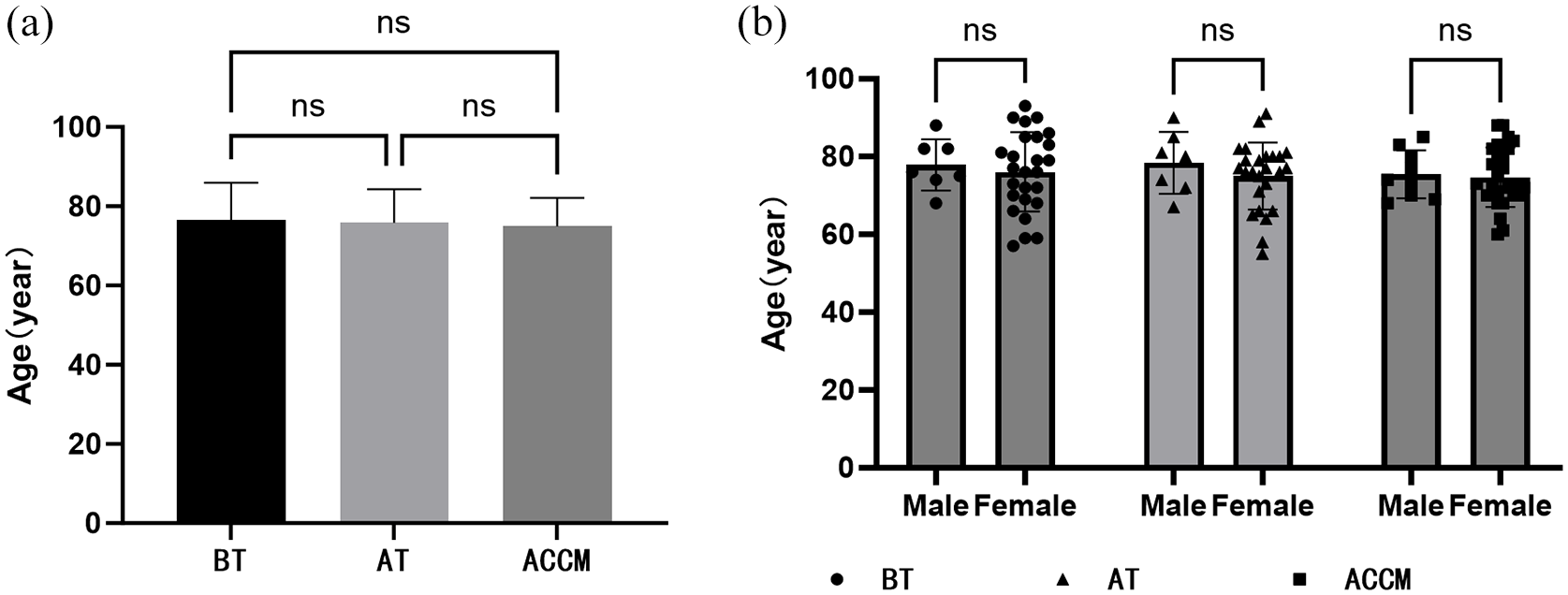
Statistical results of age and sex of OAB patients with three treatment methods: (a) age statistics of three different treatment groups and (b) statistical results of sex and age in three different treatment groups.
In this study, the OABSS scores of severe OAB patients in the three groups were evaluated before and after treatment. The results showed that in the BT group, there was no significant difference with the score decreasing from 13.21 to 12.67 (Figure 3(a) and (b)). However, the AT group and ACCM group have significant effects. In AT group, the score changed from 12.72 to 9.72, and in the ACCM group, it changed from 12.92 to 5.08, with the decrease rates of 3.25 ± 1.83 and 7.83 ± 1.34 respectively (Figure 3(c)–(f)). The results of pairwise comparison among the three groups show that there were significant differences between groups other than the BT group, the AT group and the ACCM group, suggesting that acupuncture treatment and ACCM were better than BT treatment, and ACCM had the best effect (Figure 5(a)).
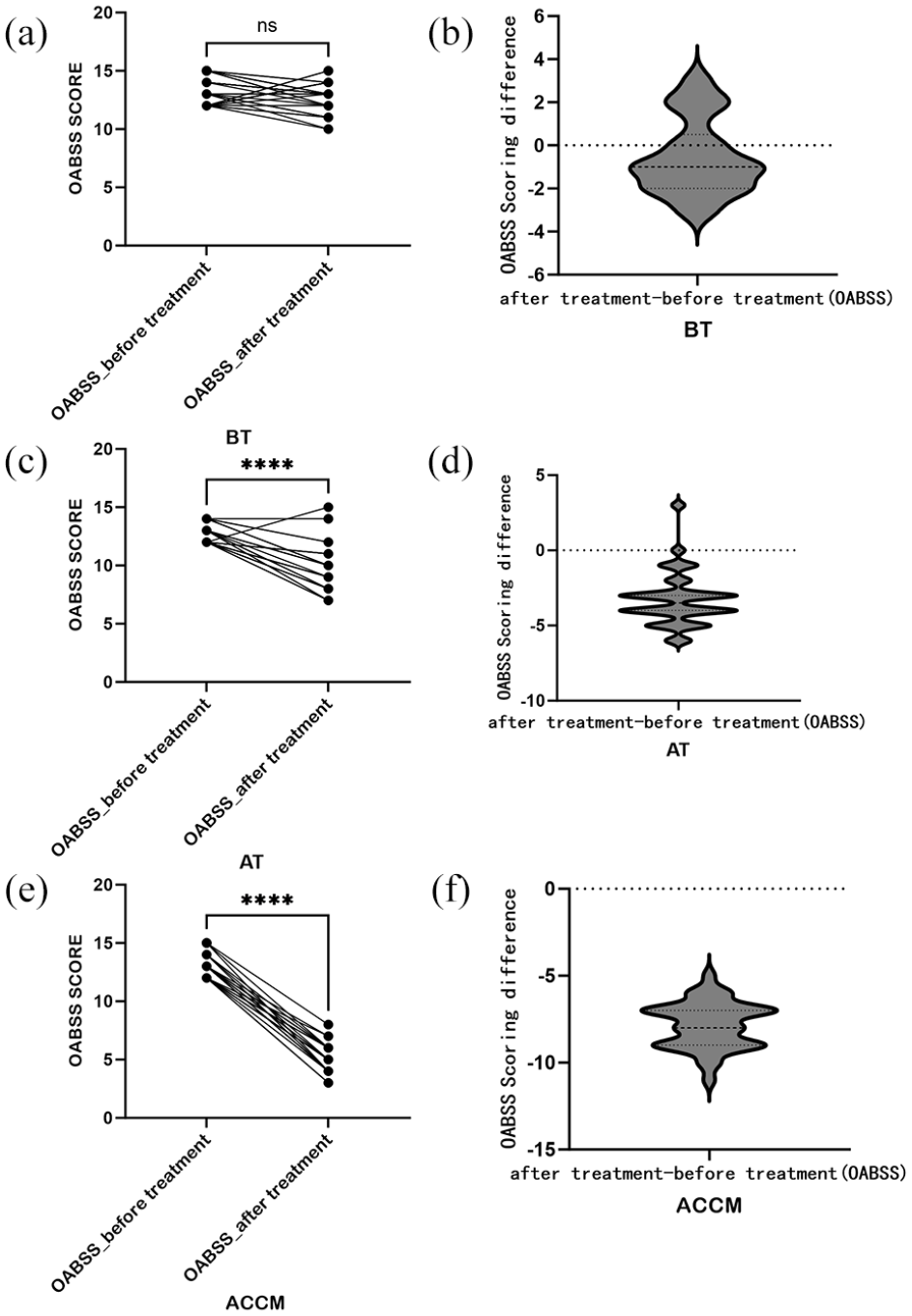
According to OABSS score, the curative effect of the three groups of treatment methods was evaluated: (a and b) OABSS evaluation results of BT group, (c and d) OABSS evaluation results of AT group, and (e and f) OABSS evaluation results of ACCM group.
In addition, we also scored QOL according to the patients’ quality of life. The results showed that it was consistent with OABSS score, and the BT group had the worst effect with little improvement (Figure 3(a) and (b)). Before and after treatment, the improvement in the AT group and the ACCM group was obvious, with the scores in the AT group changing from 4.96 to 3.5 and in the ACCM group changing from 5.08 to 0.67 respectively (Figure 4(c)–(f)). The decrease amounts in the AT group and the ACCM group were 1.47 and 4.12, respectively. Based on the results of pairwise comparison, it was suggested that the ACCM had the best improvement effect (Figure 5(b)).
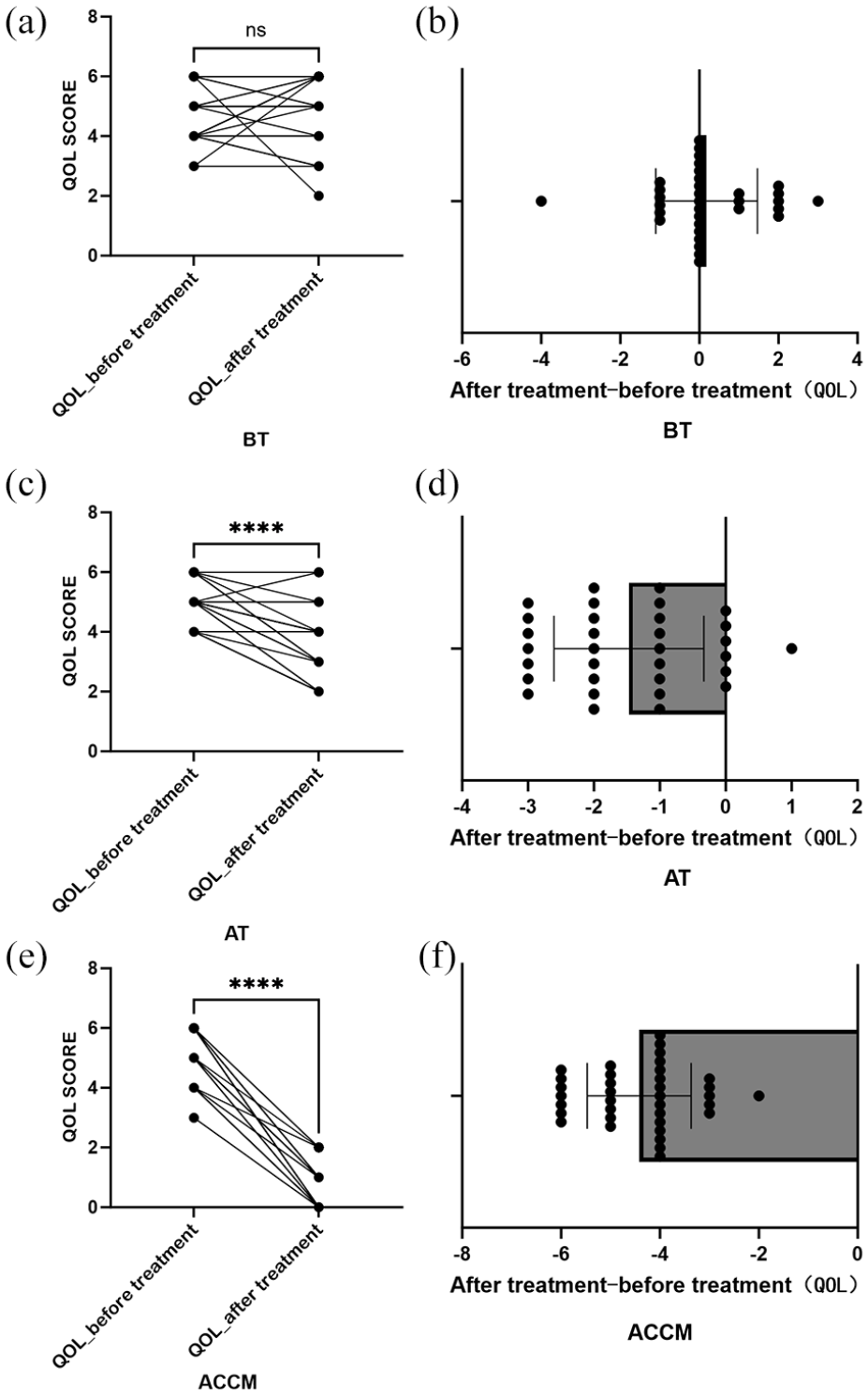
Evaluation results of three groups of treatment for severe OAB patients according to QOL score: (a and b) QOL evaluation results of BT group, (c and d) QOL evaluation results of AT group, and (e and f) QOL evaluation results of ACCM group.
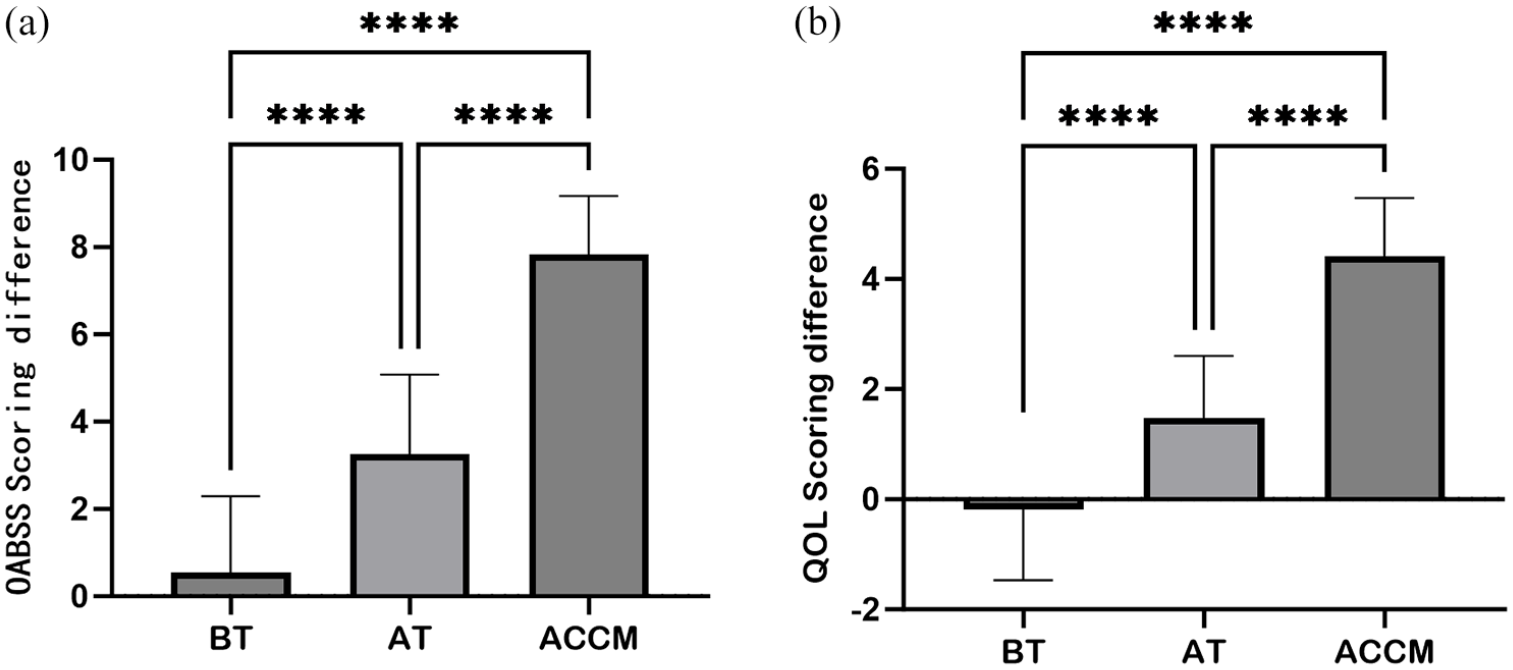
OABSS and QOL scores were used to analyze the results of the three groups. of BT, AT and ACCM: (a) OABSS score analysis results among the three groups, and (b) QOL score analysis results among the three groups.
Based on all the results, it was suggested that for severe OAB patients, the BT treatment was the worst. Although the AT had a certain effect, the ACCM treatment was the best.
Conclusion
There are various treatments for overactive bladder, each having its own advantages and limitations. In clinical practice, corresponding treatments should be selected. The comprehensive conditioning concept and individualized treatment in TCM are undoubtedly an optimized approach for treating OAB patients, especially those with severe OAB. The combined treatment of acupuncture points and cross moxibustion has a more precise effect. Although existing research lacks certain theoretical support, with the development and continuous exploration of TCM, the clinical design, sample size, and evaluation indices in the clinical trial of TCM for OAB will be further improved, thereby forming a more systematic and effective treatment plan and finally being applied in the clinic.
Discussion
Overactive Bladder (OAB) is a prevalent condition in urology that significantly impairs patients’ quality of life. The pathological mechanism underlying OAB, as understood in western medicine, encompass several theories, including the myogenic, 8 neurogenic, 9 epithelial, 10 and ion pathwaytheories. 11 In contrast, TCM attributes OAB primarily to stagnation of qi in the lower Jiao, 12 leading to abnormal gasification function of bladder, which is closely linked to lung, spleen, kidney, liver and other organs. Despite extensive research exploring the mechanism of OAB from various perspectives, such as anatomy, pathophysiology, immunohistochemistry, the exact pathogenesis 13 remains unresolved.
Given the complex etiology of OAB, achieving optimal outcomes with single therapy is challenging; thus, a comprehensive treatment approach is anticipated to enhance efficacy. TCM emphasizes holistic conditioning, which may offer more effective treatment for OAB. TCM categorizes this condition under “stranguria” for treatment methods that warm yang and tonify the kidney to address the root cause. 14 For instance, Jinkui Shenqi Decoction 15 is one such remedy. Ruixin et al. 16 suggest that deficiencies in liver blood and qi can exacerbate OAB, recommending soothing the liver and alleviating depression to break the vicious circle. 17 Numerous well-known and proven TCM prescriptions, such as Wuling powder, Bupi Yishen Tonglin decoction, 18 are also utilized. Our research group selected commonly used TCM herbs from classical prescriptions including Radix Aconiti, Radix Aconiti Kusnezoffii, Herba Ephedrae, Herba Asari, Notopterygii Rhizoma, Radix Angelicae Dahuricae, Cortex Cinnamomi, and Zingiberis Rhizoma, 19 and employed a medicine powder for cross moxibustion. This method achieved the effect of external treatment for internal diseases through drug penetration. Additionally, we incorporated acupuncture points with established therapeutic effects, selecting points based on disease presentation and meridian pathways, employing a combination of local and distal points, and referencing numerous reputable medical records. 20 The acupuncture points chosen include Qihai, Guanyuan, Intermediate, Qugu, Shuidao, Huilai, Yinlingquan, Sanyinjiao, and Taixi. 21 Notably, tibial nerve stimulation in western medicine corresponds to the Sanyinjiao point in TCM. 22 By stimulating these acupoints, the functions of bladder detrusor and urethral sphincter can be restored to normal, thereby alleviating symptoms of frequent urination and urgency. 23 Moxibustion serves to warm, alleviate diarrhea, removing blood stasis, and regulate the 12 meridians and eight extraordinary meridians. Historical texts, such as Huangdi Neijing’s Lingshu Function 24 indicate that “acupuncture is not appropriate” and the introduction to Medicine25,26 also asserts that “if medicine alone is inadequate, moxibustion must be employed.” Cross moxibustion 27 derived from umbilical moxibustion, is an external treatment method that aligns with internal treatment principles. Previous studies have shown that medicated cake moxibustion effectively improves maximum single urination volume and average urination interval, demonstrating superior efficacy compared to tolterodine. 28 Research by Qiaoge and Yang 29 and others has also indicated that acupoint moxibustion can effectively regulate the bladder function in patients with neurogenic bladder OAB, suggesting that medicinal moxibustion may significantly enhance clinical symptoms in OAB patients.
Consequently, acupuncture and moxibustion appear to be effective in improving conditions for OAB patients, with minimal adverse reactions. Previous research conducted at our hospital demonstrated that the effectiveness of acupuncture at specific acupoints in treating mild to moderate OAB. 30 However, due to the inconsistencies in clinical design, sample size and evaluation metrics, the level of evidence supporting acupuncture and moxibustion in treating OAB remains limited hindering its international recognition regarding effectiveness, superiority and safety. 31 Moreover, there is currently a lack of comprehensive research focused on patients with severe OAB. Consequently, our research team has chosen to study this population, standardizing treatment protocols, including that incorporate TCM, the selection of acupoints, and the application of moxibustion techniques. We found that in patients with severe OAB, the application of ACCM significantly reduced the OABSS score, compared to acupuncture alone. At the same time, when evaluated alongside QOL score, our results further support the conclusion that combined therapies effectively enhance the quality of life for patients with severe OAB. At the same time, this approach offers several advantages, including ease of administration, minimal side effects, low technical complexity, and reduced resource requirements, making it suitable for widespread adoption and beneficial to the community.
In summary, various treatments exist for overactive bladder, each with its unique advantages and limitations; therefore, appropriate treatment options should be selected based on clinical circumstances. 31 The holistic and individualized treatment approach of TCM represents an optimized strategy for managing OAB, particularly in severe cases, and the combined treatment of acupuncture points and cross moxibustion has a more exact effect. Although current research may lack robust theoretical foundations, with the development and continuous exploration of TCM will enhance clinical trial design, sample size, and evaluation metrics, ultimately leading to the development of a more systematic and effective treatment protocol for clinical application.
Footnotes
Acknowledgements
Not applicable.
Author contributions
X. Guo designed the research; X. Guo, P. Hu, T. Han conducted the research; X. Guo and W. Gai provided essential reagents or provided essential materials; Y. Yu and X. Lu analyzed data or performed statistical analysis; X. Guo, wrote the manuscript; X. Lu revised the manuscript. Y. Yu had primary responsibility for the final content; and all authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by Shandong Medical and Health Science and Technology Development Plan Project (202204110044) and Qingdao Science and Technology Bureau Project (15-9-2-67-nsh).
Consent to participate statement
For studies using human participants, state whether written informed consent was obtained from participants to participate in the study. The study was approved by the ethics committee of Qingdao haici medical treatment group and performed in accordance with the principles of the Declaration of Helsinki.
Availability of data and materials
The data that support the findings of this study are not publicly available due to their containing information that could compromise the privacy of research participants, but are available from Xuechao Lu (Email:
Data statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.