
Abstract
Objective:
To research the best time to provide cardiopulmonary bypass (CPB) and the best way to do it when treating an extensive tumor thrombosis of the inferior vena cava vein (IVC).
Results:
The operating times in groups A and B were (376.7 ± 91.2) and (373.1 ± 80.7) minutes, respectively, with no statistically significant difference (t = 0.716, p > 0.05); intraoperative bleeding was (1916.7 ± 925.1) ml and (2600 ± 3756.3) ml, (t = −0.601, p < 0.05), and hospitalization was (32.3 ± 16.0) and (34.0 ± 8.0) days, with statistically significant differences (p < 0.05).
Conclusion:
The CPB approach has the advantages of less intraoperative blood loss, faster surgical procedures, and fewer hospitalizations.
Introduction
The difference between tumor thrombosis and hypercoagulable thrombosis is that tumor thrombosis develops when cancer cells separate from the central focus and penetrate the lumen, fusing with xenogeneic cells in the lumen to generate microscopic metastases. 1 Renal cancer with tumor thrombosis occurs 4%–10% of the time.2,3 The median survival of patients was 5 months. 4 The best course of treatment for patients is radical nephrectomy with the thrombectomy. The level of tumor thrombosis, according to world research, does not directly influence patient survival, but it can have an impact on the time frame of the operation, the quantity of intraoperative bleeding, and perioperative problems. 5 Preventing excessive intraoperative bleeding and safeguarding vital organs is one of the most important goals of surgery in the treatment of extended tumor thrombosis above the diaphragm, so the use of CPB during surgery is the best alternative. CPB, as a surgical technique in which an artificial device replaces a bodily function, is a crucial component of cardiovascular surgery.
The use of CPB as life support in emergency, difficult, and critical conditions that cannot be addressed by conventional methods makes surgery the safest and most successful treatment option.6–8 This article analyzes patients with renal cancer with tumor thrombosis of the inferior vena cava operated at the Clinic of Cardiovascular Surgery of Sechenov University; the materials are divided into two groups with and without intraoperative use of CPB technique, the relevant data are analyzed, and the optimal time frame for the use of CPB technique in renal cancer surgery with tumor thrombosis of the inferior vena cava is discussed.
Materials and methods
In renal cancer with IVC tumor thrombosis, massive intraoperative blood loss is a common complication. The severity of blood loss increases with the level of tumor thrombosis. CPB not only preserves the blood supply to vital organs other than the heart but also maintains a clear surgical field, supports the safe execution of cardiac surgery, and reduces intraoperative blood loss. Therefore, in renal cancer patients with high- level (level III-IV) IVC tumor thrombosis, we use extracorporeal circulation to minimize intraoperative blood loss.
Ten renal cancer patients with tumor thrombosis in the IVC had surgical therapy at the Clinic of Cardiovascular Surgery of Sechenov University between 2021 and 2023.
The study materials were divided into two groups. Group A: patients who underwent radical nephrectomy with thrombectomy under normothermic CPB; Group B: patients who underwent radical nephrectomy with thrombectomy without CPB.
The grouping criteria in this study were based on the phased evolution of surgical strategies at our institution, as follows:
Additional rationale for grouping consistency
- the temporal demarcation between groups (early exploratory phase vs later optimized phase) aligns with the natural evolution of clinical practice, reflecting a real-world research context.
- all patients were enrolled under uniform criteria specific to their respective phases, eliminating subjective selection bias.
- potential baseline disparities (e.g. thrombus stage, tumor location) were rigorously addressed via multivariable adjustment in our analysis, with results consistently supporting the clinical benefits of CPB (detailed in the Results section).
Group A: Radical nephrectomy with thrombectomy by CPB with normothermia
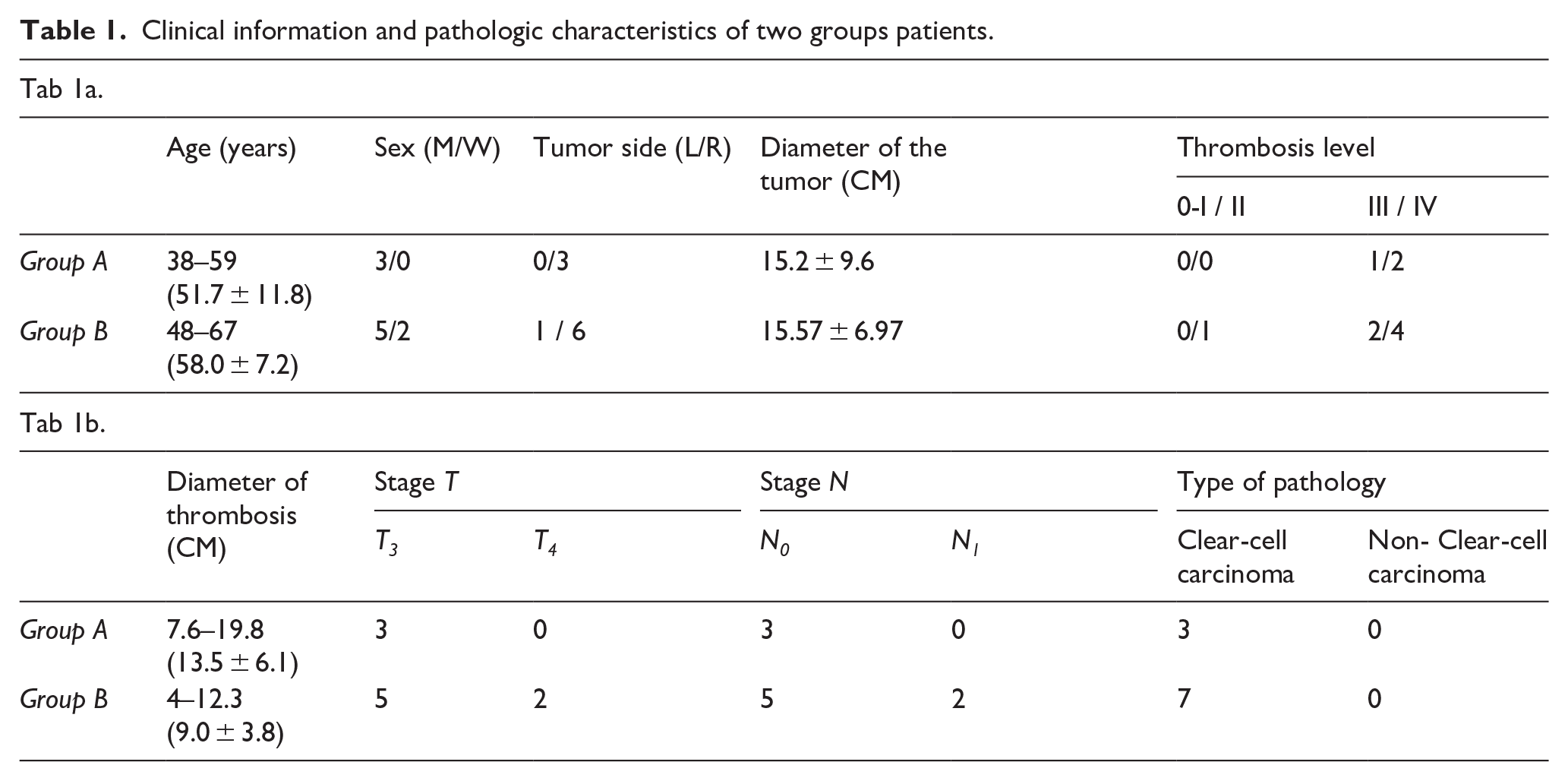
Three patients underwent radical nephrectomy and thrombectomy by CPB with normothermia (Table 1). All three are male (100%). The age of the patients ranged from 38 to 59 years (51.7 ± 11.8 years). Right renal cancer was present in three cases (100%). Tumor diameter ranged from 6 to 25 cm (15.2 ± 9.6 cm). Classification tumor thrombosis to Clinic Mayo: level III − 1 (33.3%) case and level IV − 2 cases (66.7%).
Clinical information and pathologic characteristics of two groups patients.
Group B: Radical nephrectomy with thrombectomy without CPB
Seven patients had radical nephrectomy and tumor thrombectomy without CPB (Table 1). Of these, five were male (71.4%) and two were female (28.6%). The age of the patients ranged from 48 to 67 years (58.0 ± 7.2 years). Right renal cancer was observed in six cases (85.7%) and left renal cancer in one case (14.3%). The diameter of the tumors was 15.57 ± 6.97 cm. Classification tumor thrombosis to Clinic Mayo: level II − 1 cases (14.3%), level III − 2 cases (28.6%), level IV − 4 cases (57.1%).
At the preoperative stage, all 10 patients received color Doppler ultrasound, CT/MRI to determine tumor size, extent of tumor thrombosis, and presence of invasion into the wall of the inferior vena cava; no significant distant metastases or absolute contraindications to surgery were found.
Surgical intervention
Group A: Radical nephrectomy with thrombectomy by CPB with normothermia
The surgical technique was based on a method conceived by Prof. Komarov et al.’s team. 9 Normothermic CPB was used during surgery for all patients. Operation time: 295–475 min (376.7 ± 91.2 min); intraoperative bleeding: 850–2500 ml (1916.7 ± 925.1 ml); CPR time: 24–56 min (37.0 ± 16.8 min); hospital stay: 16–48 days (32.3 ± 16.0 days; Table 2).
Perioperative period for both groups of patients.

During the oncological stage of the procedure, which was performed under CPB and heparinization, the kidney, adrenal gland, surrounding tissues, and tumor thrombus were removed as a single block after ligating and crossing the renal artery and its collateral vessels.
Following protamine injection, the kidney, adrenal gland, and surrounding tissues were excised as a single block in a dry field.
According to our experience: When performing thoracotomy, it is possible to cannulate the femoral artery in a typical location, as well as the femoral vein, and connect CPB by peripheral access. If a sternolaparotomy is performed, the aorta is cannulated in the typical location. The IVC is cannulated extrapericardially, considering the need for manipulation of the right heart. In the absence of descending thrombosis, the IVC may be cannulated below the renal vein mouth, and if present, the femoral vein may be cannulated. Pringle maneuver to prevent hepatic vein bleeding and hepatic stasis in all patients with a clamped suprahepatic IVC; in some cases, abdominal aortic cannulation is performed.
Group B: Radical nephrectomy with tumor thrombectomy without CPB application
The surgical procedure is also based on the method of Prof. Komarov et al. ’s team. 9 Operation time - 255–480 min (373.1 ± 80.7 min); intraoperative bleeding - 600–11.000 ml (2600 ± 3756.3 ml); hospital stay - 21–44 days (34.0 ± 8.0 days; Table 2).
Statistical methods
SPSS 27.0 statistical software was used to analyze quantitative data using t-test (normally distributed data) or Mann-Whitey U-test (non-normally distributed data) and stereotyped data using X2 test, with p < 0.05 considered as statistically significant difference.
Results
Comparison of perioperative parameters between the two groups is listed in Table 2. The operating time between Groups A and B did not differ statistically significantly (t = 0.716, p > 0.05). There were statistically significant differences in intraoperative bleeding (t = −0.601, p < 0.05) and hospital stay (t = −0.157, p < 0.05). Group A: One incidence of acute renal failure and one instance of pancreatic head bleeding following surgery were postoperative complications. Group B: the major postoperative complications were pancreatitis (one case), hematoma (one case), postoperative wound dehiscence (one case), acute urinary retention with drainage tube infection (one case), and lymphorrhea (one case).
Discussion
The following are the primary objectives of surgical treatment for renal cancer in patients with tumor thrombosis of the inferior vena cava, as reported in the international literature 10 :
1) maximal removal of renal tumor and tumor thrombosis.
2) excision of regional lymph nodes.
3) prevention of displacement of tumor thrombosis.
4) preservation of hemodynamics.
5) avoidance of organ ischemia.
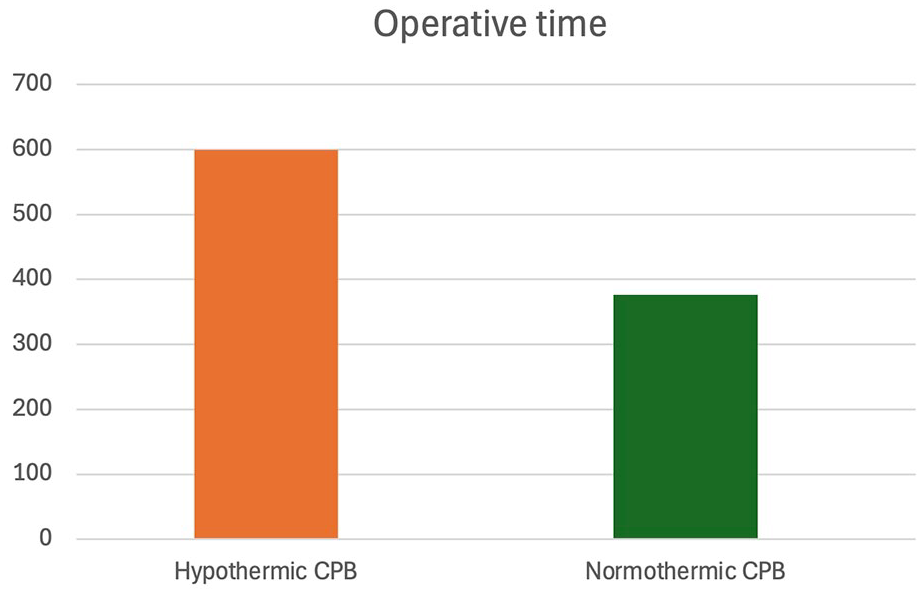
The complexity and risk of surgery are both dependent on the extent of tumor thrombosis. Large operative blood loss, severe perioperative complications, and high mortality are characteristics of open supradiaphragmatic tumor thrombectomy (levels III and IV).10,11 When a tumor thrombus invades or spreads to the right atrium or other major vessels, the primary goal is to stop intraoperative bleeding. CPB can give 4–5 L·min−1 of blood per minute during aortic or abdominal aortic cannulation, successfully ensuring circulatory stability and lowering the risk of bleeding.12,13 Hypothermic CPB is commonly used in renal cancer complicated by grade III-IV IVC tumor thrombosis. Based on our experience, normothermic CPB may reduce operative time in these procedures. Here, we compare studies in the world on the use of CPB in hypothermia based on the results 14 : The operative time for this type of surgery using hypothermic CPB, as reported in the literature, was 600 (285–995) minutes, whereas our operative time with normothermic CPB was 376.6 (295–475) minutes. (Figure 1) When CPB is used under normothermia, intraoperative operating time is shortened.
Comparison of results for CPB.
The following can be deduced from the analysis:
1) Thrombectomy with CPB should be undertaken for extended tumor thrombosis in the supradiaphragmatic region (levels III and IV).
2) When compared to hypothermia, normothermic CPB shortens the length of operation and lessens blood loss.
3) In levels III and IV, the distal end of the tumor thrombosis is located intrahepatically or supradiaphragmatically, and surgery without CPB needs adequate liver mobilization and blockade of hepatic blood flow; surgery with CPB does not require liver mobilization, which reduces the likelihood of postoperative liver failure.
4) Blocking the inferior vena cava’s proximal end avoids the displacement of tumor thrombosis and the development of TELA during the removal of tumor thrombus.
The results of the research suggested that using the CPB approach had advantages over not using it for the treatment of renal cancer with extensive tumor thrombosis of the inferior vena cava levels III and IV, including less bleeding, fewer problems, and a shorter hospital stay.
Conclusion
The CPB approach has the advantages of less intraoperative blood loss, faster surgical procedures, and fewer hospitalizations.
Footnotes
Author’s Contribution
1. Mingchen Shao: Conception and design, Drafting of the manuscript, Supervision.
2. Roman N Komarov: Conception and design, Drafting of the manuscript, Supervision.
3. Leonid M Rapoport: Conception and design, Drafting of the manuscript, Supervision.
4. Dmitry O Korolev: Drafting of the manuscript, Acquisition data.
5. Ilya Vasalatii: Drafting of the manuscript, Acquisition data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.