
Abstract
The purpose of this study is that the combination effects of Peyronie’s disease (PD) therapy with Phosphodiesterase type 5 inhibitors (PDE5i) plus acetylsalicylic acid on improve curvature progression and pain in the active phase of disease. We performed a retrospective cohort study of 161 patients affected by PD in active stage and erectile dysfunction treated with tadalafil 5 mg once daily were divided in two groups. Group A(GA): 93 men treated with only PDE5i (tadalafil 5 mg) for 1 year or more and Group B(GB): 68 men that received tadalafil 5 mg plus aspirin 100 mg with the same protocol of GA. The patients of both groups were assessed at baseline and follow-up (6 months) for erectile function, painful erections, penile plaque size, and penile curvature. Six months after the treatment the patients in both groups had a non-significantly reduction of penile plaques. However, in GB patients had a clinically significant reduction of the curvature after 6 months by treatments 20.21° ± 7.20 versus 28.13° ± 8.11 (GA), (p < 0.001). In the analysis of our secondary endpoint, we demonstrated a significantly lower intensity of pain during erection in GB (1.43 ± 1.12) compared GA (1.89 ± 1.25; p < 0.001). We observed that the regular use of this therapeutic combination significantly provided more benefit in patients with active stage PD in terms of penile deformity, pain, and discomfort during penetrative intercourses.
Keywords
Introduction
Peyronie’s disease (PD) is an acquired idiopathic fibrotic degeneration associated with the formation of fibrotic plaques in the tunica albuginea (TA), which causes pain and deformation of the penis during erection with a prevalence in men over 40 years ranging from 0.3% to 7%. 1 The etiology is unknown, although the triggering factor is generally recognized to be local injury (recurrent micro trauma or major trauma) to the corpora cavernosa during sexual intercourse. 2 The local trauma causes a hematoma and deposition of fibrin. The hematoma leads to the recruitment of inflammatory cells and pro-inflammatory cytokines, which inevitably results in the formation of chronic inflammatory tissue that evolves toward fibrosis.1,2 PD has two distinct stages. An acute inflammatory phase (active stage) where the inflammatory process causes the production of collagen, and the consequent remodeling of the tissue, resulting in fibrosis of the affected area with formation of one or more plaques that become stables in a time ranging from 12 to 16 months (second chronic stage).2,3 The management for PD during the active stage includes a conservative therapy such as oral drugs (vitamin E, colchicine, tamoxifen, nonsteroidal anti-inflammatory drugs, phosphodiesterase-5 inhibitors (PDE5i), carnitine, propolis, etc.), intra-plaque injections (such as corticosteroids, verapamil, pentoxifylline, clostridium histolyticum collagenase, interferon, etc), mechanical stretching with vacuum erection devices, and physical therapy (extra corporeal shockwave therapy and iontophoresis).3,4 Phosphodiesterase type 5 inhibitors (PDE5i) have long been used in the treatment of ED. 5 In PD, these agents are proposed to inhibit tissue remodeling after acute injuries by decreasing oxidative stress responsible for inflammation and fibrosis.6,7 Experimental trials on rats have suggested that continuous administration with PDE5i may reduce collagen deposition and increases apoptosis of fibroblast inhibiting plaques development in a rat model of PD 8 . However, the European and American Urological guidelines recommends use PDE5i to treat concomitant erectile dysfunction (ED) or if the deformity results in difficulty in penetrative intercourse in order to optimize penetration. 8 Acetylsalicylic acid and other nonsteroidal anti-inflammatory drugs (NSAIDs), as one of the most commonly used drugs, possesses a broad spectrum of numerous properties, such as antioxidant, anti-inflammatory, anti-apoptotic, and antifibrotic activities. 9 NSAIDs modulate different molecular pathways by acting on various cytokines, transcription factors, growth factors and their associated receptors, thus playing a protective role against cardiac fibrosis, atherosclerotic diseases and cancer progression. 10 Aspirin treatment has been reported to reduce inflammatory cells and improve collagen deposition in animal models. 11 It has also been observed to be capable of ameliorating progressive hepatic fibrosis, characterized by infiltration of inflammatory cells, fibrotic tissue deposition, and increased collagen content. 12 The hypothesis of this study is that there is a potential synergistic mechanisms of action of PDE5i and aspirin in PD and the combination effects of the two drugs improve curvature progression and pain duration in the active phase of PD.
Subjects and methods
Study design and selection criteria
We performed a retrospective cohort study of patients with PD seen between January 2015 and May 2024 at two referral andrology centers. The study was conducted according to the Declaration of Helsinki on ethical principles for medical research involving human subjects. The inclusion criteria were patients aged ⩾18 years with PD in the active stage lasting for ⩽12 months, presence of only one penile plaque ⩽ 20 mm in largest diameter, penile deviation of ⩽60°, associated ED. The exclusion criteria were: presence of two or more penile plaques, prior penile surgery, prior injection intraplaque therapy or mechanical treatments, low testosterone total serum levels (normal reference range: 300–1000 ng/dL), patients in PD stable stage lasting for >12 months. An accurate sociodemographic data, medical history and physical examination were obtained during the first visit. The following data were recorded from each patient: age, BMI (Body Mass Index), previous treatments, medications, comorbidities (diabetes, hypertension, cardiovascular disease, connective tissue disorder), penile trauma history, penile plaque position, number and size of plaques, disease duration, type and degree of penile curvature, ED (categorized as either normal or impaired based on subjective patient report) and pain during erection. Size, number and location of penile plaques was assessed (in mm) with an ultrasonography study (with a 6.5–15 MHz linear transducer). The degree of the penile curvature angle was measured with a goniometer after intracavernous vasoactive injection (alprostadil 10–20 mcg) before and after the treatment. ED was evaluated using the simplified International Index of Erectile Function (IIEF-5). Severity of ED was classified as severe (IIEF-5 ⩽10), moderate (IIEF-5 between 11 and 16), or mild (IIEF-5 between 17 and 21). The subjective pain during an erection was evaluated by means of the visual analog scale (VAS); with 0 as no pain and 10 as maximum pain. The adherence to daily medication was assessed during follow-up visits at 3 and 6 months after the start of the treatment. The results were evaluated at baseline and 6 months after the treatment.
Treatment protocols
Patients were retrospectively divided into a control group or an experimental group, namely those who had received daily PDE5i (tadalafil 5 mg) as part of their treatment [Group A (GA)] for 1 year or more and those who were already taking aspirin 100 mg once daily for 1 year or more as a preventive and/or curative measure for cardiovascular disease plus tadalafil 5 mg [Group B (GB)], respectively. The primary outcome was the change in penile curvature between visits in patients receiving daily PDE5i treatment compared to patients receiving daily aspirin plus tadalafil 5 mg daily. As a secondary endpoint we compared the pain development between Group A and B. During the clinical visits, patients were specifically queried regarding their adherence to daily medication. Those patients who demonstrated consistent medication intake and continued to remain in the active phase of the disease were considered as study participants. None of the patients had undergone treatment explicitly targeted PD such as Extracorporeal Shockwave Therapy, vacuum therapy, or traction therapy. Patients who had previously been treated with on-demand PDE5i were not excluded. In instances where patients initially initiated treatment with either PDE5i (Group A) or those who were treated with aspirin 100 mg plus tadalafil 5 mg (Group B) but were later redirected toward alternative treatment, we continued to monitor their penile curvature measurements until the initiation of the new treatment, which could include surgical intervention or collagenase clostridium histolyticum injections.
Statistical analysis
The data were analyzed in a common database. Continuous variables were described as medians and interquartile ranges and nominal variables as numbers and percentages. Comparisons between groups were performed using the Chi-square test or Fisher’s exact test for discrete variables and Mann–Whitney U test for continuous variables. All statistical analyses were conducted using SPSS version 24 (IBM Corp., Armonk, NY).
Results
A total of 161 medical records of patients affected by PD and ED, treated daily with PDE5i were included retrospectively in the study. Among them, GA was composed of 93 patients treated with only tadalafil 5 mg once daily and GB consisted of 68 patients that received tadalafil 5 mg plus aspirin 100 mg with the same protocol of GA. Patient’s characteristics at inclusion are shown in Table 1. Not statistically significant differences emerged between the two groups at baseline. The median follow-up was 8.7 months. Six months after the treatment the patients in both groups had a non-significantly reduction of plaque size (p = 0.212). However, in GB patients had a clinically significant reduction of the curvature from a mean ± SD of 32.81 ± 8.27° at baseline to a mean ± SD of 20.21 ± 7.20° after 6 months (p < 0.001) by treatments. In GA patients had a not significant decrease curvature degree from a mean ± SD of 33.51 ± 8.63° at baseline (p = 698) to a mean ± SD of 28.13 ± 8.11° after 6 months (p < 0.001). After treatment (p = 0.001) particularly in the GA, significant differences were observed in terms of IIEF-5 score a mean ± SD of 11.32 ± 5.33° at baseline to a mean ± SD of 17.63 ± 2.55° after 6 months. In the analysis of our secondary endpoint, we demonstrated a significantly lower intensity of pain during erection in GB compared GA (p < 0.001). GA had a mean ± SD intensity of pain of 1.89 ± 1.25 (range 1–4) while GB had a mean ± SD of 1.43 ± 1.12 (range 1–2), (Table 2).
Patient’s characteristics.
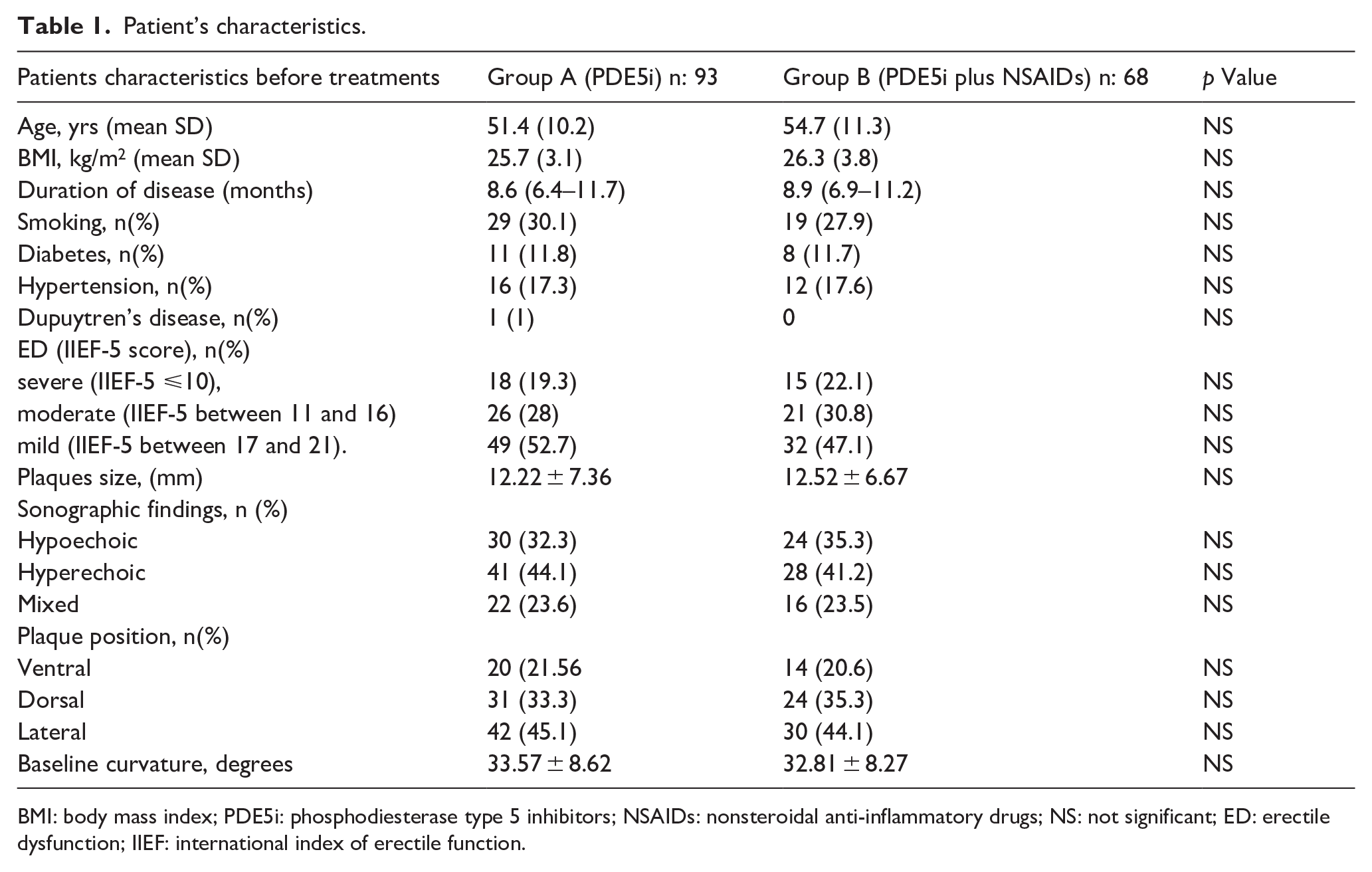
BMI: body mass index; PDE5i: phosphodiesterase type 5 inhibitors; NSAIDs: nonsteroidal anti-inflammatory drugs; NS: not significant; ED: erectile dysfunction; IIEF: international index of erectile function.
Comparison of clinical outcomes between two groups of patients before and after treatments.
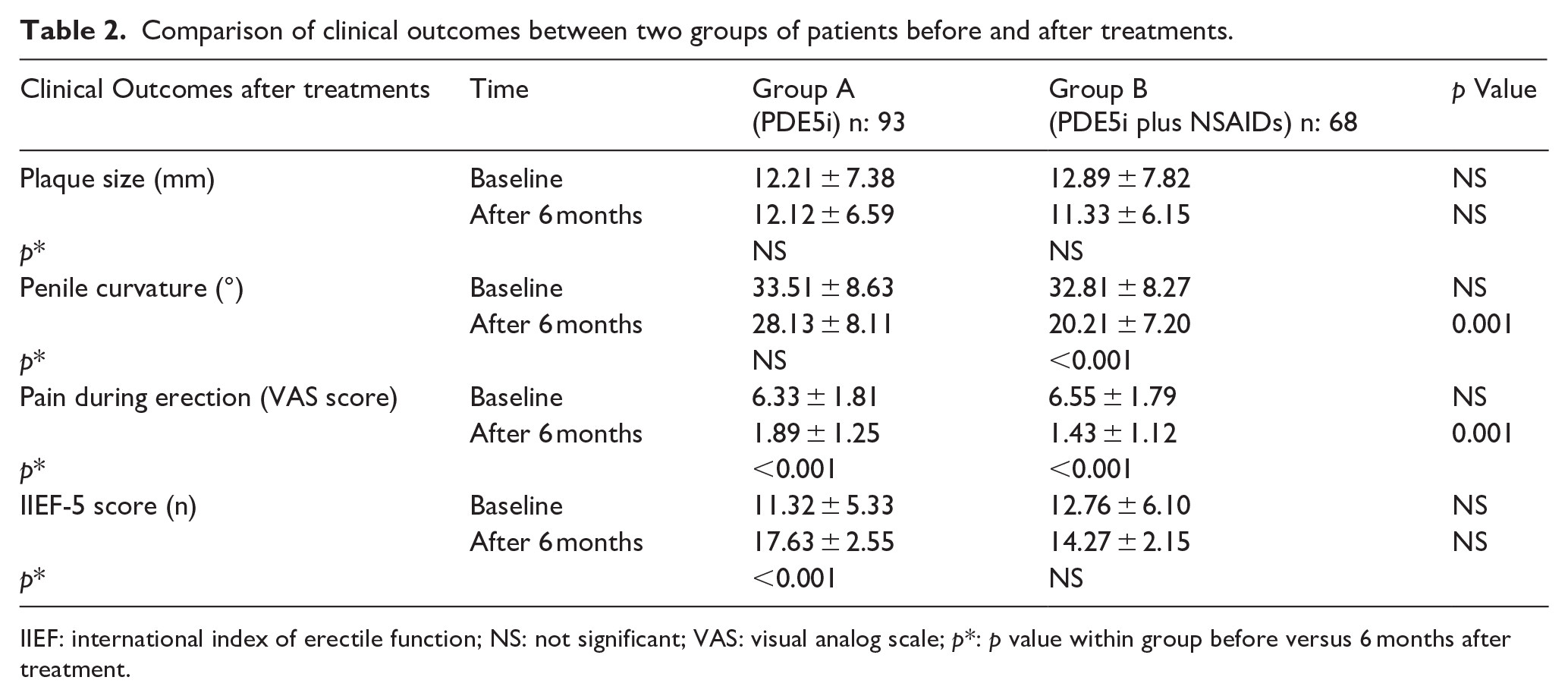
IIEF: international index of erectile function; NS: not significant; VAS: visual analog scale; p*: p value within group before versus 6 months after treatment.
Discussion
Most PD patients are unable to penetrate due painful erections and/or due to the angle of the curvature. Severe or moderate stage of ED is present in 20%–50% of PD patients and occurs for a variety of reasons including penile curvature and cavernosal fibrosis, which compromise penile vascularity. 8 In our study group (GA) ED was reported as severe stage in 20.5%, and moderate stage in 33.8% of patients, while in the group (GB), these percentages were 22.1% and 30.8%, respectively. Acute stage PD is a challenging entity with respect to management. The treatment strategy has shifted from traditional single therapy to new combination modalities. 4 The use of PDE5i was investigated in several studies in the field of DE. 13 Phosphodiesterase type 5 inhibitors were first used to treat PD in 2003, assuming that they promote a reduction in collagen deposition by inhibiting TGF-β1.14,15 Only two previous clinical trials have investigated the use of PDE5i in PD. The first one was a retrospective trial conducted in 2011 to examine whether PDE5i administration could promote healing of isolated septal scars in the absence of evidence of penile deformity. The results were encouraging, as the tadalafil group reported a higher IIEF-5 score, and resolution of the septal scar was observed in 24 patients (69%) compared to 3 patients (10%) in the control group. 15 Additionally, in a head-to-head comparison with vitamin E, sildenafil for 12 weeks showed better results in IIEF-5 scores and pain reduction compared to the vitamin E group. 16 Spirito et al. in a recent retrospective study examined the effects of daily tadalafil administration. Tadalafil 5 mgin patients with pain and erectile dysfunction in the PD phase. This study shows that acute administration of tadalafil does not reduce curvature and does not improve symptoms related to PD. 17 Finally, another recent study showed that adding sildenafil 50 mg daily to the pentoxifylline-colchicine combination was more effective in curvature than the pentoxifylline-colchicine combination alone was more effective in weight loss, pain, and erectile function. 18 These results, together with the lack of significant side effects of PDE5i, have led to the widespread use of PDE5i in the treatment of PD. Oxidative stress plays a very large role not only in the onset, but especially in the progression of PD, resulting in local tissue damage and the formation of fibrotic plaque and its possible calcification. 2 Multimodal or combined treatment is a therapeutic practice which has already been used in other fields of medicine, such as oncology and the treatment of infections (antibiotic combination therapy).2,3 In PD, this is particularly advantageous, since many antioxidants also have antinflammatory and antifibrotic properties that differ slightly, and therefore combining them makes it possible to reduce the dose of each antioxidant and to tackle PD and its various biochemical mechanisms, interfering in different ways with the many “chemical messengers” involved.1,2 Aspirin, known for its century-long history and diverse therapeutic applications, is widely used for conditions such as arthritis, pain relief, fever, and menstrual discomfort, as well as for cardiovascular health. Its role as a prophylactic agent against heart disease, thrombosis, and even cancer is under ongoing investigation. 19 Given its prevalence among various age groups as a self-administered medication, the potential effects of aspirin on erectile function represent an intriguing area of research. The mechanism of action of aspirin involves both enhancement and inhibition of pathways that could affect erectile function. 20 On one hand, aspirin enhances the activity of endothelial nitric oxide (NO) synthase, which increases the production of NO. NO is crucial for smooth muscle relaxation and improved vascular blood flow, which are essential for achieving and maintaining an erection. On the other hand, aspirin inhibits the cyclooxygenase pathway, which decreases the synthesis of vasodilatory prostaglandins such as prostaglandin I2 and prostaglandin E2. 21 This inhibition may potentially hinder normal erectile function due to reduced vasodilation. Clinical studies investigating the relationship between aspirin use and ED have produced mixed results, leading to an inconclusive understanding of this association. While some studies suggest that aspirin may contribute positively to erectile function through its effects on endothelial function and blood flow, others raise concerns about its potential adverse impacts due to decreased levels of key vasodilatory agents.22,23 In summary, while aspirin has demonstrated beneficial effects on vascular health, its influence on erectile function remains complex and unresolved, warranting further research to clarify its role and potential implications for men experiencing erectile dysfunction. However, aspirin is known to show various properties, such as antioxidant, anti-inflammatory, anti-apoptotic and antifibrotic activities. 24 Recent studies suggest that aspirin modulates different molecular pathways by acting on various cytokines, transcription factors, growth factors and their associated receptors, thus playing a protective role against cardiac fibrosis and nonalcoholic fatty liver disease, characterized by infiltration of inflammatory cells, fibrotic tissue deposition and increased collagen content. 25 The normal histological structure of the TA surrounding the penile corpora cavernosa consists of an inner circular and an outer longitudinally arranged elastin and collagen network. In the pathophysiology of PD, repetitive micro-traumas to the TA cause a proliferation of pro-fibrotic factors such as TGF-β1 and platelet-derived growth factor and a reduction in anti-fibrotic factors. TGF-β1 plays a role in soft tissue fibrosis and ED.26,27 Our results in this study are based on a thorough assessment of patients with PD in the acute phase exclusively without excluding patients with comorbidities such as cardiovascular disease. This reinforces the generalizability of our findings. Furthermore, this is the first study in the literature comparing the efficacy of a combined treatment with PDE5i plus aspirin in patients with PD in the acute stage and median follow-up of 8.7 months (Figure 1). However, our study has several limitations. It was a non-randomized and retrospective study, with grouping based on clinician choices, potentially introducing selection bias. Another limitation of our study include the relatively small treatment group. This may have limited the statistical power to detect a treatment effect regarding curvature development compared to PDE5i treatment alone.
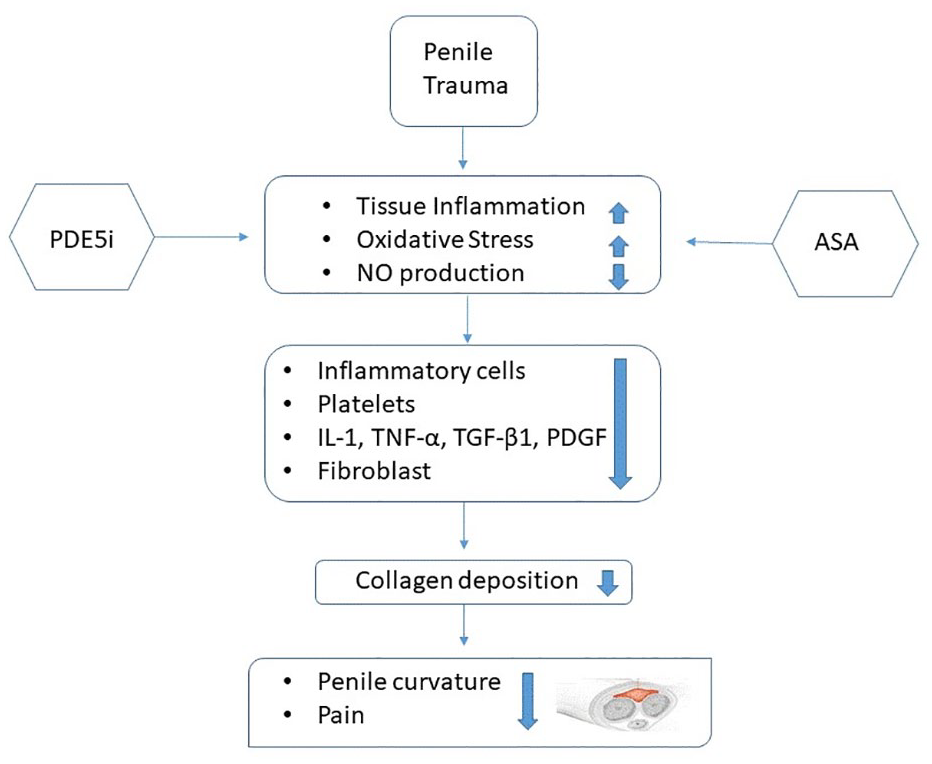
Phosphodiesterase type 5 inhibitors (PDE5i) plus acetylsalicylic acid (ASA) improve curvature progression and pain intensity during the active phase of peyronie’s disease reducing tissue inflammation, ameliorating oxidative stress trough NO-cGMP-PGK pathway activation.
Conclusions
The treatment strategy has shifted from traditional oral therapies to new combination modalities. In this study, we observed that the combination therapy tadalafil 5 mg plus aspirin daily could achieve benefits in patients affected by PD. The regular use of this therapeutic combination may provide greater benefits in patients with active stage PD in terms of penile deformity, pain, and discomfort during penetrative intercourses and erectile function. The relatively small sample size and the absence of long-term outcomes necessitate validation through future multicenter studies.
Footnotes
Acknowledgements
Nil
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was deemed not to be required given all data is available to the public and is anonymized.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.