
Abstract
Background:
We created a classification system for encrusted ureteral stents (ES) (
Methods:
Retrospective review of patients with ES; clinico-demographics, additional lithiasis (AL), stent calcification characteristics, surgeries performed, complications and stone free rate were collected. Chi-square was used to compare the categorical variables and Kruskal-Wallis test for the comparison > 2 numerical groups; a p-value < .05 was considered significant.
Results:
We included 190 ES; 163 (85.8%) stents underwent one-time surgical removal. Most Grade I catheters were removed in a single surgery, without invasive/multimodal therapy; Grade II-III catheters required multimodal and invasive therapies. The presence of AL in kidney increased the number of surgical interventions performed in Grade I/II catheters (p < 0.05) and the likelihood of requiring multimodal (Grade I: 90%, Grade II: 83.3%, Grade III: 100%) or invasive surgery (Grade I: 38.1%, Grade II 58.3%, Grade III 90.9%) to achieve successful treatment.
Conclusions:
Incorporating both the calcified stent characteristics and the presence of AL, GARSA score can be used to determine the selection of the optimal surgical approach for patients with encrusted stents.
Keywords
Introduction
Ureteral catheters have been widely used since their introduction by Zimskind in 1967 in order to relieve obstruction in the urinary tract secondary to urolihiasis, malignant growth and after endourological procedures; however, as described by Zimskind in his publication, there are risk associated with its use, where 2 out of 13 patients presented incrustation of the silicone catheter. 1
The incidence of calcification in ureteral catheters is up to 10%, 2 patients with a history of urolithiasis have a higher risk of catheter calcification. 3 Although early catheter removal is recommended to prevent calcification, patients without proper follow-up are common, especially in recent years due to the COVID-19 pandemic. Several identifiable risk factors exist for encrusted ureteral stents (ES), including reduced diuresis, previous urinary tract stone formation, 4 bacterial biofilm, recurrent urinary tract infection, 5 catheters with larger surface/diameter 6 and prolonged indwelling time, either due to loss of follow-up, poor compliance, or inadequate communication between healthcare provider and patient. 7
ES can cause fever, renal colic, urinary tract infection, hematuria, hydronephrosis and lower urinary tract symptoms and, in some cases, can be asymptomatic.8,9 Removal of a ES is challenging for urologists, requiring complex surgeries (the employment of multiple surgical modalities or invasive surgical techniques) with potential complications, and increasing the healthcare costs. Surgical treatment of ES depends on the extent and location of calcification; to facilitate its approach, various ES classifications have been created to predict the complexity of the surgical treatment, success, and possible complications.
These classifications are based on different aspects some of which are: volume of calcification (Singh), 10 stone burden measurement in millimeters in each segment of the catheter (KUB classification) 11 and those based on the intensity and location of the calcification such as FECal 12 y V-GUES 13 ; they may be complex, difficult to memorize and apply in daily medical practice; moreover, these classifications do not include the presence or absence of concomitant additional lithiasis (AL), a crucial element, since more than 60% of ES are indicated by lithiasis pathology 14 and their presence impacts surgical decision-making.
A readily applicable and accessible classification system for ES is essential. This system should comprehensively address all potential clinical scenarios in a patient with ES, including the presence of AL (e.g.: pre-existing stones within the renal collecting system or ureter), and ideally possess the ability to predict treatment outcomes. For this reason, we created the new GARSA (
This study aims to demonstrate the GARSA classification’s usefulness to predict the surgical outcome of patients with ES with/without AL and help in surgical decision making.
Materials and methods
Study population
Previous approval by the hospital’s Ethics Committee (R-2023-1904-018), we conducted a retrospective review of the medical and radiographic records of patients over 18 years of age with a diagnosis of ES treated in two hospital units located in northeastern Mexico (UMAE 25 and HGZ 33 of the Instituto Mexicano del Seguro Social) between January 2014 and January 2024.
ES were defined as those that could not be removed cystoscopically on the first attempt (using rigid cistoscope and forceps) and required additional procedures for removal
Classification
GARSA score (Figure 1) was assigned according to radiographic findings (CT scanning) with interobserver agreement between two urologists.
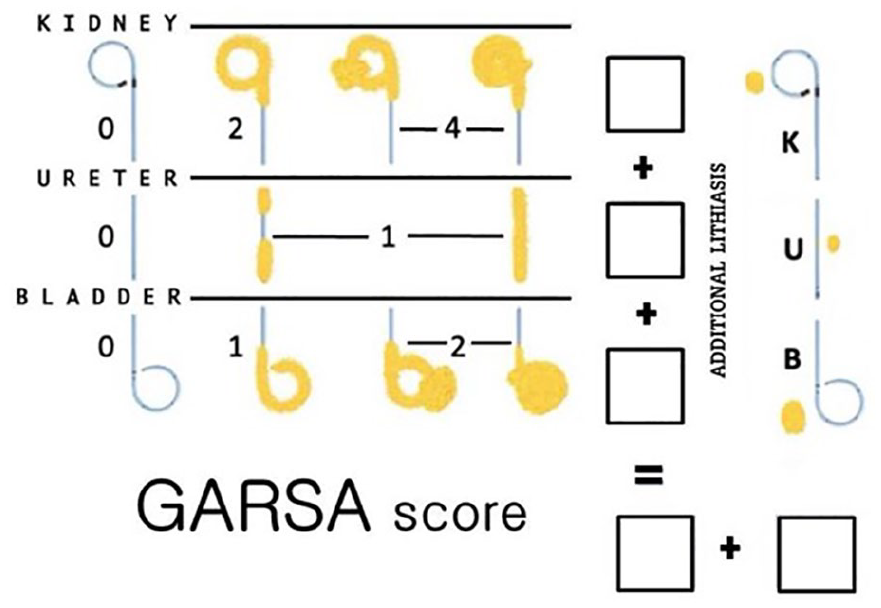
GARSA score classification is obtained adding the points of each segment: kidney (2 for circumferential, 4 for partial/complete bullous calcification) + ureter (one point) + bladder (one for circumferential, 2 for partial/complete bullous calcification). If there is additional lithiasis, the letter K (kidney), U (ureter) and B (bladder) are added. Grades: I (1–3 points), II (4–5 points), and III (6–7 points).
This system was designed after an extensive review of the literature, obtaining data of the number and type of surgeries performed for the resolution of the ES based on the characteristics and affected segment of the catheter. We designated the calcification as “bullous” to the stone burden encompassing the proximal or distal curl, and as “circumferential” to a tubular-appearing calcification encasing the catheter. As previously reported, renal calcification is associated with increased surgical complexity,8,11 therefore, the score is higher when the calcification is located at the renal section (2 points for circumferential calcification and 4 points if there is a bullous formation that partially or completely affects the proximal segment); for the remaining portion of the catheter, one point is awarded for ureteral calcification, and for the vesical segment, one point is assigned for circumferential calcification, and two points are assigned if a bullous formation is present that partially or completely affect the distal segment. The final score is obtained by adding the points given for the calcification present in the renal + ureteral + bladder segment (maximum value of 7), grouping them into three grades: I (1 to 3 points), II (4 to 5 points) and III (6–7 points) (the grades were assigned according to a previous pilot study); the letter K, U and B are added when there is AL independent to that of the ES (kidney, ureter and bladder respectively) (Figure 1). In this way, a ES can be Grade I + K + U if it belongs to Grade I and also has AL in the kidney and ureter (Figure 2); and Grade III + K if it belongs to Grade III and has AL in the kidney (Figure 3).
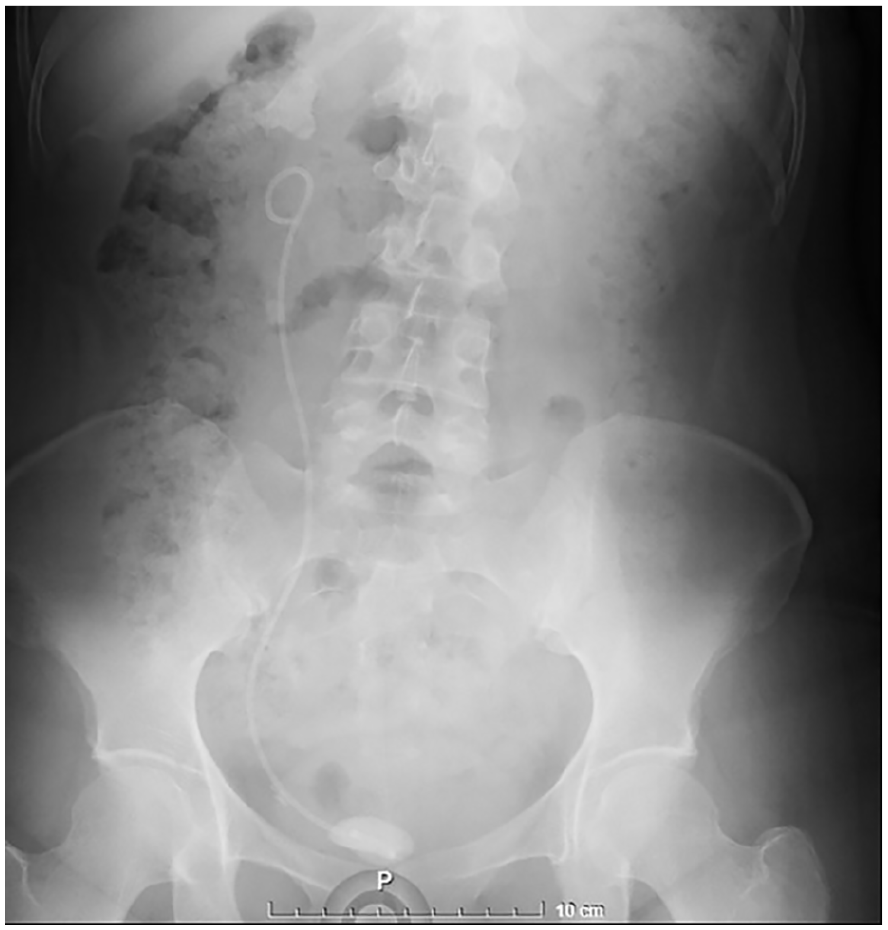
Radiographic findings of GARSA Grade I + K + U catheter: complete bullous formation in bladder segment (2 points), without renal or ureteral segment calcification; total score is 2 points = Grade I, plus concomitant kidney and ureter stones.
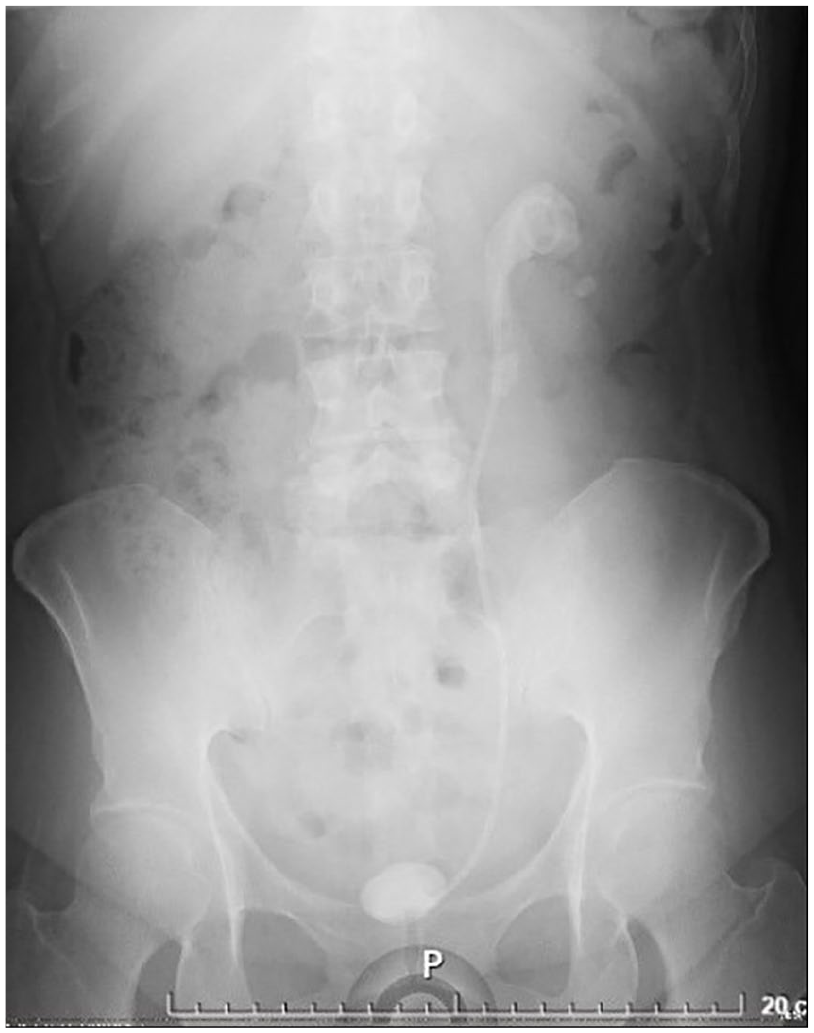
Radiographic findings of GARSA Grade III + K catheter: complete bullous formation in the bladder segment (2 points), ureteral segment calcification (1 point), complete bullous formation in renal segment (4 points); the total score is 7 points = Grade III, plus additional kidney lithiasis.
Prolonged time was defined as indwelling ES for ⩾ 5 months. Ancillary surgeries were those performed to resolve AL, either in the same event (different modality than the one used for catheter removal) or at a different surgical time. Invasive surgery was defined as requiring the performance of percutaneous nephrolithotomy (PCNL) or open surgery; multimodal surgery was considered if two or more different types of procedures were performed for ES removal in the same or different event (e.g. semirigid ureteroscopy/ flexible ureteroscopy, ureteroscopy/ PCNL, etc.). Stones ⩾ 4 mm were considered residual lithiasis.
Evaluations
The clinico-demographic variables of the patients, indication for catheter placement and the affected side were recorded. Each renal unit was analyzed independently. The primary objective was to analyze the type of surgery (cystolithotripsy/cystostomy, semirigid/flexible ureteroscopy, PCNL, pyelolithotomy, ureterolithotomy), ancillary surgeries to achieve stone-free status (of the AL), and complications secondary to the surgical procedure for ES removal; the secondary objective was to record the number of surgeries performed to remove the ES.
The choices regarding therapies used for the removal of each ES were made by the treating urologist, based on their experience and the availability of medical instruments. The complications recorded were only those secondary to the event related to the catheter removal and were categorized according to the Clavien-Dindo classification. 15
Statistical analysis
Quantitative values are shown as mean and standard deviation and qualitative variables are reported as frequency and percentage. For comparison of categorical variables, the chi-square test was used; for comparison of more than two groups, non-parametric Kruskal-Wallis test was used, a p-value of < 0.05 was considered significant.
Results
During the study period, 138 patients with 190 encrusted stents were recorded. 34 patients had ES on repeated occasions and 18 had ES in both kidneys. The mean age was 46.20 ± 14.91 years, 74 women (53.6%) and 64 men (46.4%). The most frequent indication for double J catheter placement was the presence of urolithiasis in 82 of the ES (43.2%), and after an endourological procedure in 73 (38.4%); 96 renal units presented AL (Table 1). The median indwelling time was 7 months (IQR 25–75%: 4–11 months); in 137 ES (72.1%) the indwelling time was ⩾ 5 months. Calcification of the bladder segment was found in 148 ES (77.8%), in the renal segment was 117 (61.5%), and ureteral segment was 70 (36.8%); only one ES was fragmented.
Clinico-demographic characteristics.
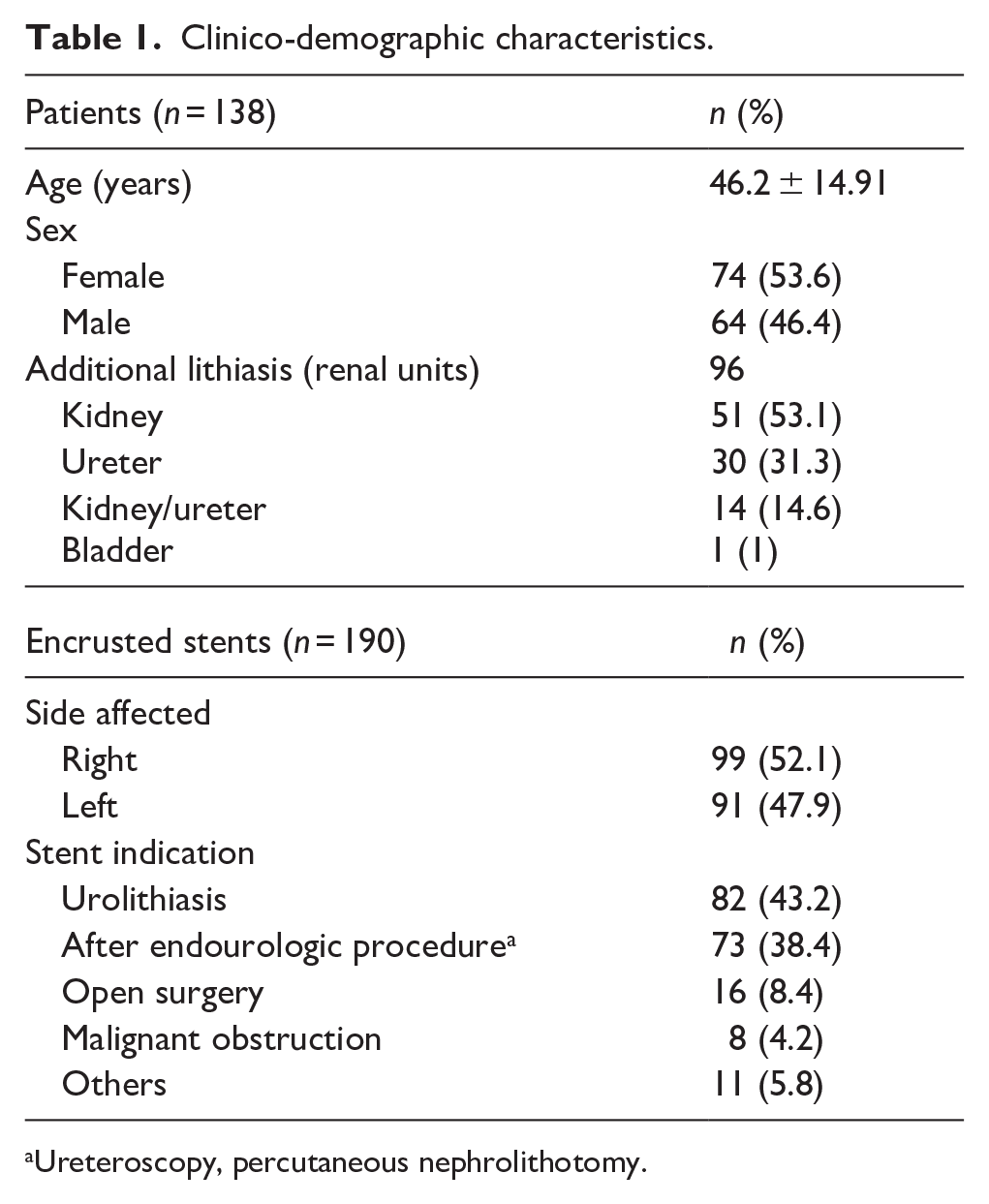
Ureteroscopy, percutaneous nephrolithotomy.
In 163 of the ES (85.8%), the catheter was removed in one single-event, 25 (13.2%) ES required two surgical events, and 2 (1%) ES required more than two surgical events; in 81 of the ES (42.6%), multimodal treatment was required. Table 2 shows the distribution of ES according to GARSA classification as well as the proportion of catheters that were removed in a single-event.
Distribution of the encrusted stent according to GARSA classification and proportion of stents removed in a single-event (n = 190).
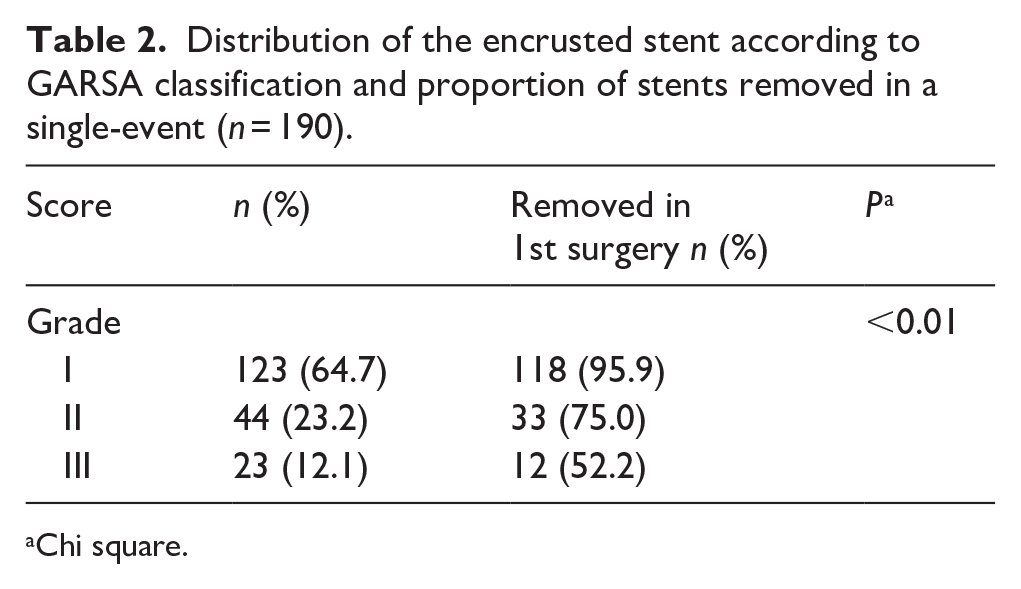
Chi square.
Considering only the surgical procedure for ES removal (Table 3), 47.8% of grade III catheters required more than one surgical event, 95.7% were managed multimodally, and in 73.9%, it was necessary to perform invasive surgery such as PCNL or pyelolithotomy/ureterolithotomy. Grade II catheters required repeat surgery in over 25% of cases, with 72.7% mandating multimodal interventions; additionally, one-third underwent invasive surgical procedures. In contrast, most grade I catheters could be removed during a single surgical procedure, without the need for multimodal or invasive techniques.
Comparison of surgical events, type of surgery and complications between GARSA classifications groups a (n, %).
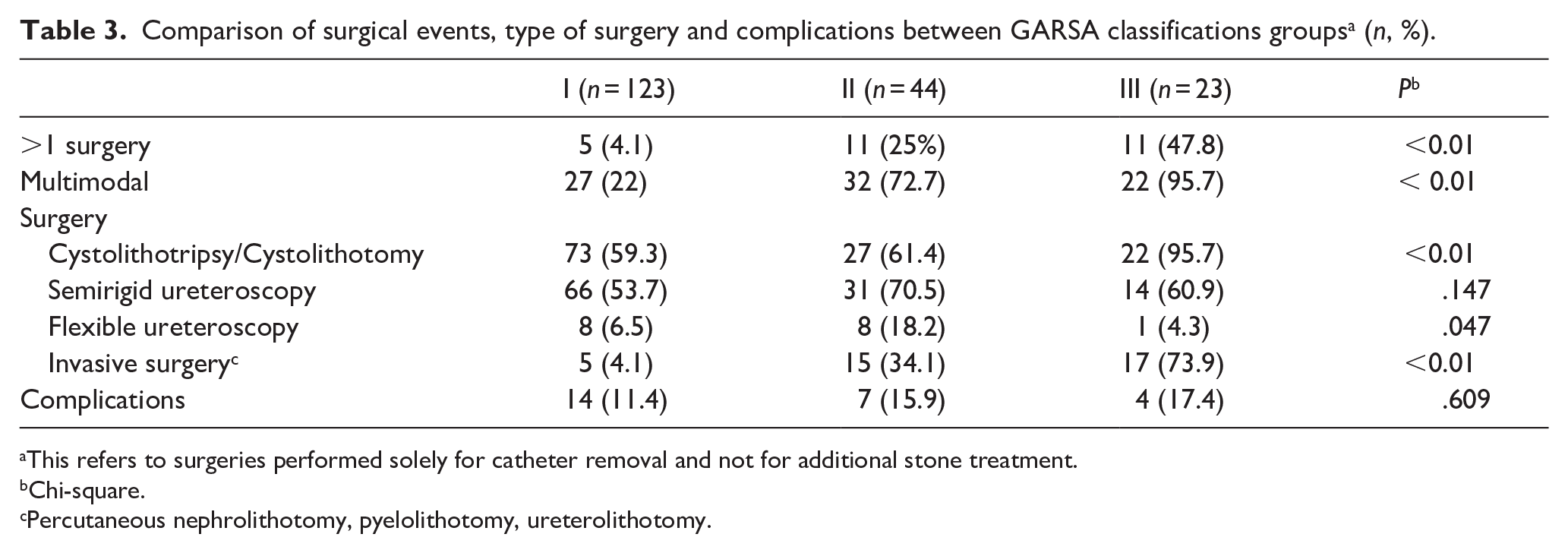
This refers to surgeries performed solely for catheter removal and not for additional stone treatment.
Chi-square.
Percutaneous nephrolithotomy, pyelolithotomy, ureterolithotomy.
In 9 patients, the ES was cut to facilitate its removal; 25 surgical complications were recorded (13.2%), Clavien-Dindo II in 11 (44%), IIIB in 7 (28%), I in 6 (24%) and IIIA in 1 patient (4%) there was no difference in the presentation of surgical complications between different grades (Tables 3 and 4).
Surgical complications (n = 25).
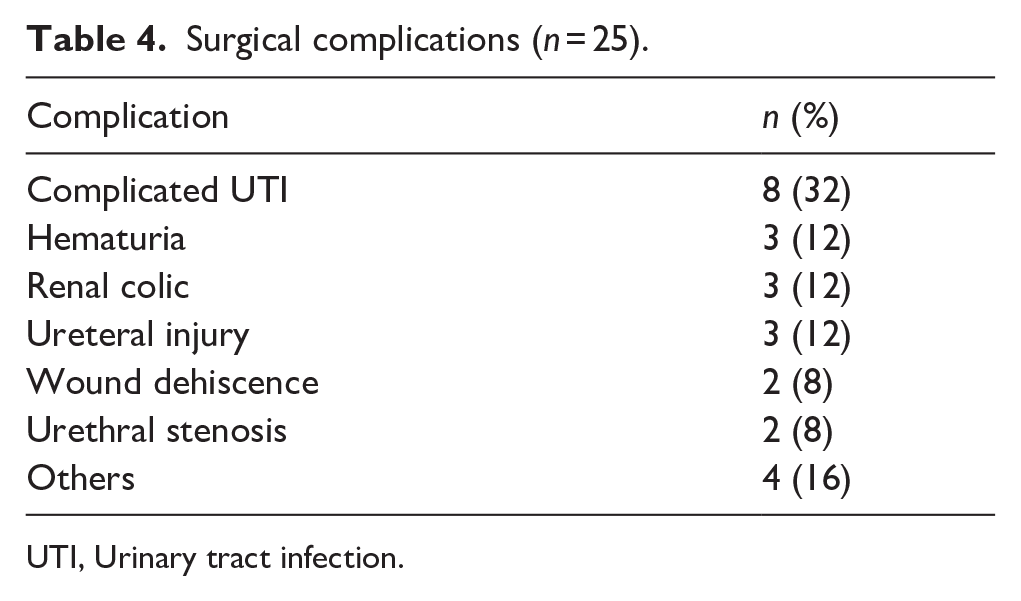
UTI, Urinary tract infection.
Out of 96 renal units with AL, 72 (75%) required ancillary surgeries to resolve the lithiasic burden (1.25 ± 0.5 surgeries). The patient diagnosed with bladder lithiasis experienced spontaneous resolution prior to the scheduled surgical intervention, consequently, this case was excluded from the subsequent analyses. Table 5 presents an analysis of the total number of surgical procedures performed to resolve both ES and additional lithiasis. The analysis is stratified by the different catheter grades, the presence or absence of AL, and its location. Across all three catheter grades, the presence of AL was associated with an increase in the number of surgeries required for problem resolution (P ⩽ .05).
Comparison of surgical events in patients with and without additional lithiasis (n = 95).
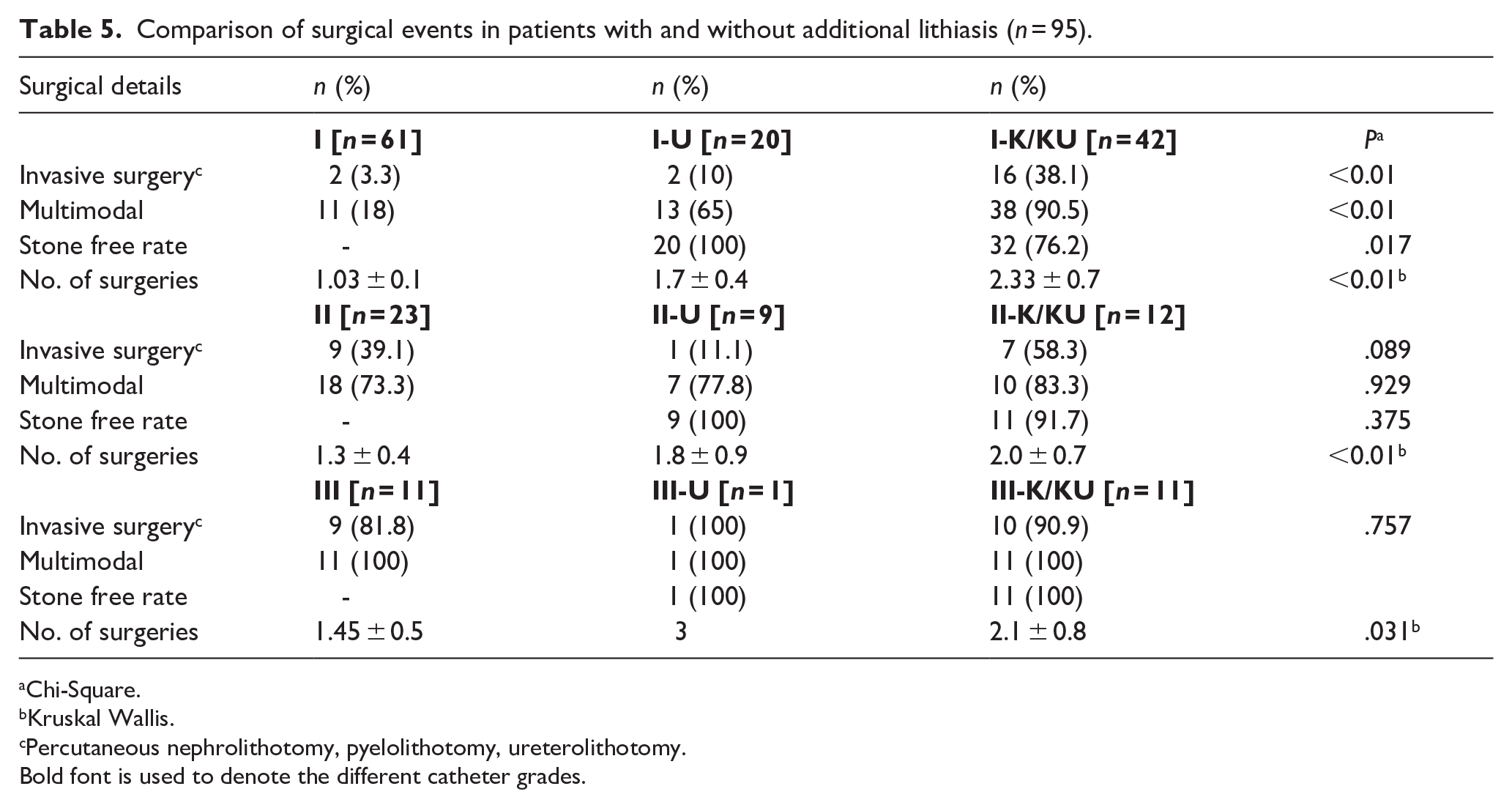
Chi-Square.
Kruskal Wallis.
Percutaneous nephrolithotomy, pyelolithotomy, ureterolithotomy.
Bold font is used to denote the different catheter grades.
In Grade I catheters, the presence of kidney or ureteral/kidney AL was associated with a lower likelihood of achieving stone-free status (compared to ureteral AL). No significant difference in the stone-free rate was observed across the other catheter grades (Table 5).
Discussion
ES represents a health problem for urological patients, with a potential risk of complications secondary to the presence of the ES or derived from its treatment. For the removal of ES, the use of multimodal endourological therapies or open surgery is essential in selected cases. Usually, the surgical management depends on the available material, the experience of the surgeon and the complexity of the ES,2,10,11,14,16,17 in some cases, more than one surgery may be necessary; accurate diagnosis, surgical planning and awareness of potential outcomes are of paramount importance for urologists.
GARSA score system offers a valuable tool for stratifying patients across various clinical settings to improve treatment outcomes. Patients with Grade I ES are excellent candidates for cystolithotripsy and/or semirigid ureteroscopy, with a high success rate and minimal need for more invasive or complex procedures; in contrast, half of those with Grade III ES will require more than one surgery, often necessitating a multimodal approach that includes an invasive procedure.
Despite the fact that up to 50% of patients with ES and pre-existing kidney stones may require ancillary surgeries, 18 few studies analyze the impact of AL on surgical planning and treatment success. If we consider the presence of AL, even for a patient with Grade I ES, the probability of requiring multimodal surgery increases to 90%, with a 40% chance of requiring invasive procedures; these findings indicate that treatment decisions for ES should be based on both the ES characteristics and the presence of AL, particularly in patients with concomitant kidney stones to minimize the number of surgical interventions required. Notably, none of the existing classification systems account for these crucial findings.
Calcification was observed in all segments of the catheter, with a higher prevalence in the bladder and renal sections, likely due to the role of urinary stasis in its formation. The location and severity of calcification significantly influence the choice and complexity of surgical procedures,12,17 this is mainly determined by the renal calcification; the GARSA classification reflects the importance of renal segment calcification by assigning a higher score to its presence. Compared to renal segment calcification, the bladder segment mostly requires less complex interventions for successful management, endoscopic lithotripsy serves as the mainstay approach, with open surgery reserved for giant lithiasis, therefore, GARSA classification assigns a lower score. Ureteral segment calcification, despite increasing surgical time, does not significantly impact the need for multiple interventions.8,11
Up to 75% of catheters with indwelling time > 12 weeks will develop calcifications, 19 the indwelling time directly correlates with the density of calcification in all its segments8,9 consequently escalating the complexity in management of ES. Despite the recommended practice of early ureteral catheter removal, our study found that 72.1% of the population had indwelling time ⩾ 5 months. This extended indwelling time can be explained by the characteristics of our patient population, which includes a high proportion of referrals from other public hospitals within the country and patients with lost follow-up, especially during the COVID-19 pandemic. The concerning rapid catheter calcification observed in nearly a third of analyzed patients warrants further investigation, including metabolic evaluation.
The KUB classification is difficult to apply since it relies on measurements in radiographic studies and assigns equal values to the intensity of calcification irrespective of renal or bladder location, potentially introducing bias and compromising the discriminatory power of the classification. While FECal classification offers simplicity and time-saving efficiency, it does not discriminate between proximal and distal stone burden, which is a critical factor to stablish management. Due to its visual scale design, GARSA classification offers the advantage of being readily memorized and easily applied based on imaging findings (abdominal plain film or CT scanning), thereby obviating the need of complex radiographic measurements.
The incidence of complications after catheter removal ranges from 7 to 23%,11,14 In our study population, the complication rate was 13.2%, without significant differences between the different grade groups. Previous studies have observed an association between calcification complexity and the risk of post-surgical complications. 13 Due to the retrospective nature of this study, only complications requiring urgent hospital attention or inpatient admission were recorded, potentially excluding milder complications managed on outpatient basis, underestimating the true incidence of complications.
Nine patients underwent a previously described technique where the catheter is bisected to facilitate the instrumentation of the urinary tract. This maneuver allows an increased ureteral lumen, thereby enabling a safer semirigid ureteroscopy and subsequent access to the renal cavities, 18 this procedure mitigates the risk of ureteral injury caused by traction or manipulation, therefore, we recommend this procedure for catheters with extensive calcifications.
Biofilm’s role in ureteral catheter calcification warrants careful consideration as it promotes mineral deposition and thus calcification. 5 Recurrent urinary tract infections are a known risk factor for the development of catheter calcification. Further research is needed to assess antimicrobial prophylaxis or the use of alternative therapies for preventing this complication. 20
This study represents the largest published cohort of ES to date. GARSA classification demonstrates ease of use, has the ability to detect ES with characteristics that allow for single-procedure treatment while simultaneously predicting the need for more invasive options like PCNL or open surgery; moreover, this classification includes the presence of AL, which undoubtedly impacts the selection of the surgical procedure. However, it is crucial to acknowledge that treatment success rely on the availability of advanced medical equipment and the expertise of the surgical team.
We analyzed the surgical procedures necessary for both the removal of the ES and AL (occurring within the same or distinct event), this allows for the identification of the most appropriate treatment based on the specific characteristics of the ES and the presence of pre-existing lithiasis. Proper preoperative planning tailored to stone burden and localization, may enhance the probability of single-procedure ES removal and improve patient outcomes. 21
While surgical time and the catheter material remains a crucial variable, the retrospective design of the current study and the lack of data in medical records pose significant limitations regarding these and other variables; these limitations preclude robust analysis and introduce the potential for interpretation bias. Radiographic findings in AL patients may be biased due to the difficulty in distinguishing AL from catheter calcification. We acknowledge that the analyzed classifications are visual in nature, and inherently susceptible of interobserver variability.
Furthermore, the selection of surgical techniques across the study period demonstrates a complex interplay between the availability of endourologic equipment at the time of intervention, the discretion of the treating surgeon, and the specific comorbidities of each patient.
Prioritizing preventive strategies is paramount for optimal patient management. Therefore, the implementation of comprehensive follow-up programs, incorporating options such as telephone consultations, electronic monitoring or home patient visits, is potentially beneficial for individuals requiring indwelling ureteral catheter.
Conclusions
GARSA grading system offers straightforward application. By incorporating both the ES different grades and the presence of AL, this novel classification helps to predict whether the patient will require multiple surgeries, multimodal treatment and invasive surgical procedures; its utility lies in enabling the management of ES and AL during a single surgical procedure.
Summary
The novel GARSA classification system empowers clinicians to tailor treatment for patients with calcified ureteral catheters. This individualized approach minimizes the need for multiple surgical interventions and its associated complications.
Footnotes
Acknowledgements
We are grateful to the urology residents of both hospitals, specially to Dr. Hugo Peña, Dr. Sergio Ávila, Dr. Jesús Valencia and Dr. Gerardo Lily for their help in writing the manuscript.
Authors’ Contributions
María E Garza-Montúfar: conceptualization, investigation, software, resources, original draft, data curation, review & editing. Hid F Cordero-Franco: Methodology, formal analysis, validation, review & editing. Carlos M García-Pérez: Methodology, validation, visualization. Juan H Díaz-García: Methodology, supervision Brissia Lazalde: Review & editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study was approved by Local Research Ethics Committee No. 1904 (R-2023-1904-018). This study was performed in accordance with the principles of the Declaration of Helsinki. Given the retrospective nature of the study and the use of radiological records and historical archives, the committee exempted the requirement for informed consent.