
Abstract
Ureteropelvic junction obstruction (UPJO) is a major cause of obstructive uropathy in pediatric patients. However, the optimal management remains controversial. We aimed to summarize the evidence comparing surgical versus conservative treatment. We searched MEDLINE/PubMed (2016 to 31 October 2024) and the Cochrane Central Register of Controlled Trials (CENTRAL) on 31 October 2024. The primary outcome was split renal function (SRF). Results were summarized in a structured table. Study quality was assessed using the ROBINS-I tool and the level of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) working group. Our search resulted in 2.251 reports. We included two non-randomized interventional studies with 136 patients. One study reported no statistically significant difference in SRF between the study groups after 1 year of follow up, while the second study reported higher SRF in surgical group 6 months postoperatively. The studies were judged to have a serious risk of bias, and the quality of evidence was rated as very low. The paucity of eligible data precluded the performance of a meta-analysis. Our findings could not support clinical recommendations. This study highlights the lack of high-quality evidence that will come from large, prospective, well-designed trials comparing surgical intervention to updated conservative treatment options.
Keywords
Introduction
Rationale
Ureteropelvic junction obstruction (UPJO) is among the primary causes of obstructive uropathy in children and a cause of chronic kidney disease (CKD) later in life. The widespread use of prenatal ultrasound has enabled early diagnosis, as hydronephrosis, especially in the absence of ureteral dilatation, raises a high index of suspicion for UPJO. Although clinicians encounter this clinical entity in everyday routine, there is still no consensus on its management. SFU grades 1 and 2 are typically managed conservatively due to their high-resolution rates. However, unilateral UPJO cases of grades 3 and 4 are either monitored with serial imaging or treated surgically.1,2 Current guidelines from the American Urological Association and the European Association of Urology have formulated recommendations on surgical indications. These include an SRF <40%, a functional decline >10%, worsening hydronephrosis and contralateral compromise. Children with SRF >40% are usually monitored through imaging.3,4 Nonetheless, significant controversy persists. Delaying surgery may expose patients to repeated, potentially invasive and costly testing, and might result in irreversible renal damage that current diagnostic tools fail to detect. Moreover, renal function deterioration may not manifest clinically until adulthood. 5 Weitz et al. attempted to answer this clinical question, but limited and low-quality evidence prevented reliable conclusions. 2 We attempted to conduct a new systematic review, to elicit recent evidence from studies published from 2016 onward.
Objective
To assess the effects of surgical compared to conservative treatment on renal outcomes in children with UPJO.
Methods
This review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) Statement. 6
Eligibility criteria
Types of studies
We included non-randomized interventional clinical studies, as the conduction of randomized controlled studies (RCTs), involving surgery raises serious ethical concerns. This issue modified our initial intention to include RCTs, although they are considered the gold standard for evaluating interventions and were included in the latest Cochrane systematic review (SR). 2 We initially applied the Cochrane Highly Sensitive Search Strategy to identify RCTs in MEDLINE and restricted our search to studies from 2016 onward, aiming to retrieve updated evidence post-Cochrane SR. However, we did not find any new RCTs, likely due to the ethical implications of randomly assigning patients to either surgical or conservative management. This led to a post hoc revision of our inclusion criteria to accept nonrandomized interventional clinical studies. We would also have included unpublished manuscripts with published results, but we found none. We included studies with a minimum duration of follow-up of 6 months. There was no language restriction.
Population
The population comprised infants of both sexes under 1 year of age with unilateral hydronephrosis classified as grade 3 or 4 according to the Society for Fetal Urology (SFU) criteria. A diagnosis of unilateral UPJO was established by either intravenous pyelography or functional isotopic renal scans, including mercaptoacetyltriglycine (MAG3) and diethylenetriamine pentaacetate (DTPA) scintigraphy. Exclusion criteria included: bilateral UPJO, structural anomalies, vesicoureteral reflux, and symptomatic patients.
Intervention
The intervention included all possible types of surgical correction of UPJO. The comparator consisted of conservative treatment, defined as a watchful-waiting approach of repeated imaging, with or without antibiotic prophylaxis.
Outcomes
The primary outcome was split renal function (SRF), assessed using DTPA renal scintigraphy. We aimed for studies with a minimum follow-up duration of 6 months, in order to assess the impact on renal function in a plausible time frame.
Search methods
Information sources
We searched the MEDLINE/PubMed database (2016 to 31 October 2024) and the Cochrane Central Register of Controlled Trials (CENTRAL) on 31 October 2024. Search on MEDLINE was limited from 2016 onward, according to the aforementioned eligibility criteria.
Search strategy
We adapted the search strategy used in the 2016 Cochrane review, applying the Cochrane Highly Sensitive Search Strategy filter to identify RCTs). 7 The search string and search syntax are available in Supplemental Appendix A.
Selection process
We imported records retrieved by the search on MEDLINE into SRaccelerator software and duplicates were removed after screening by one reviewer. Records from CENTRAL were screened manually. Two researchers independently screened all titles and abstracts of the records retrieved. Disagreements were resolved by consensus. Next, the reviewers independently screened full-text articles and again, any disagreement on inclusion was resolved by discussion and consensus.
Data collection process
Data were collected by one reviewer using a data extraction form developed by the review team. Extracted data were checked by a second reviewer and any conflict was resolved through discussion.
Data items
Collected data included study characteristics, population characteristics, definition of intervention and comparator, and continuous outcome data, including number of participants on whom the outcome was measured in the intervention and comparator group, mean value and standard deviation of the outcome measurements. We extracted measurements of outcomes assessed at all possible time points, with a minimum follow-up of 6 months.
Study risk of bias assessment
We assessed the risk of bias using the Cochrane ROBINS-I tool. 8 The risk of bias was examined on an outcome basis, specifically for the SRF. A single reviewer assessed the risk of bias for each study. The overall risk was based on the most severe domain rating. All overall assessments along with decisions on the signaling questions were illustrated using appropriate graphs.
Synthesis methods
For continuous data, as our primary outcome, we used mean difference with 95% CI as measure of treatment effect. We planned to conduct a meta-analysis, using an intention-to-treat approach if all data were available and planned to contact with authors to retrieve any missing results. However, a meta-analysis was not feasible, as included studies were only two. Additionally, time points of main outcome assessments varied across the studies and the risk of bias of the studies was judged as serious. We also planned to conduct a sensitivity analysis including studies with low risk of bias. Since a statistical synthesis of meta-analysis was judged as inappropriate, we applied Grading of Recommendations Assessment, Development and Evaluation (GRADE) and presented the results visually by using a summary table.
Certainty assessment
We used the GRADE approach for rating the quality of evidence of included results. 9 We incorporated the overall ROBINS-I judgment to our GRADE assessment and used the other defined GRADE criteria.
Results
Study selection
Flow of studies
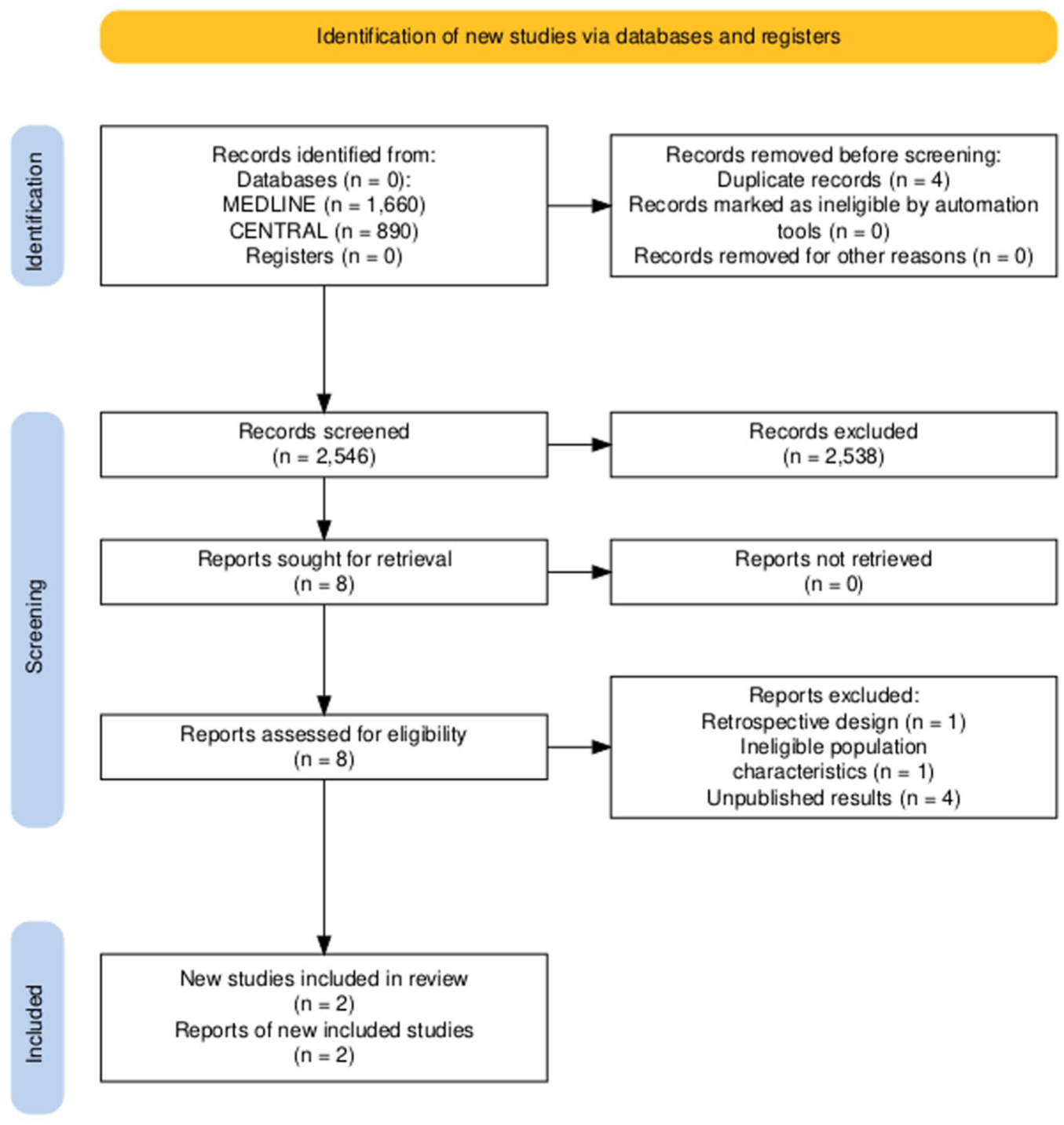
Our research on two databases revealed 2550 results. Duplicates were removed—one using an automated tool (SR Accelerator Deduplicator) followed by a manual review—and three additional duplicates were identified and removed by a reviewer during screening. After removal of duplicates, we screened 2546 records at title and abstract level and excluded 2538 records as irrelevant. The remaining eight records were sought for retrieval, and we finally screened eight records at full-text level for eligibility. Figure 1 shows the flow diagram indicating the process of study selection.
Study characteristics
A.K. Tabari 2019 11 : This was a single-center prospective interventional study that was conducted at a tertiary care pediatric surgery clinic of Iran. Due to ethical implications, randomization was not feasible. The study enrolled patients diagnosed with UPJO who were less than 1 year old, asymptomatic, had hydronephrosis of SFU grades 3 or 4, and whose affected kidney had a split function above 40%. Exclusion criteria consisted of bilateral disease, SRF < 40%, clinical symptoms related to UPJO, vesicoureteral reflux, and structural anomalies. Surgical intervention was a standard open pyeloplasty and conservative management was defined as a follow-up protocol along with prophylactic antibiotic administration. Outcomes, including cortical thickness, polar length, anteroposterior renal pelvis diameter (APD), SFU, SRF, and number of patients with renal scan T1/2< 10min, were assessed by ultrasonography and DTPA renal scintigraphy at defined time-points. Follow-up sonography was conducted at 6 and 12 months postoperatively for the surgery group and follow-up scintigraphy at 3 and 12 months. For the non-surgery group, follow-up imaging tests were performed at 6 and 12 months after the start of management. The duration of patients’ enrolling time was 12 months. Indications for delayed pyeloplasty in the conservative-treatment group were a deterioration of SRF > 10% and the development of clinical symptoms. Authors declared that they did not receive funding and did not have any conflict of interest.
Q.Deng 2021 12 : This was a single-center prospective interventional study that was conducted in a department of pediatric urology surgery in China. Randomization was not applied, as decisions on the nature of intervention were made after discussion with patients’ parents. The study population consisted of asymptomatic patients under 2 months old, diagnosed with UPJO by intravenous pyelography (separation of the renal pelvis ⩾3 cm) and a hydronephrosis SFU grade 4. Symptomatic patients, patients with bilateral hydronephrosis and structural anomalies were excluded. Patients in the surgical group received a standard open pyeloplasty, while patients in the non-surgical group were scheduled to a follow-up period. Imaging tests including renal ultrasound and DTPA renal scintigraphy were used to assess defined outcomes: length and width of the kidney, APD, SFU, cortical thickness, and SRF, at 3 and 6 months after implementation of an intervention. Secondary pyeloplasty was performed in case of a deterioration of renal function above 10% and symptomatic clinical presentation. Authors declared no conflicts of interest and reported as funding source the Anhui Provincial Health Commission.
Risk of bias in studies
We used the Cochrane ROBINS-I assessment tool for non-randomized studies of the effects of interventions to assess the risk of bias in included studies. Figure 2 illustrates the risk-of-bias traffic light plot and Figure 3 shows the risk-of-bias assessment summary plot.
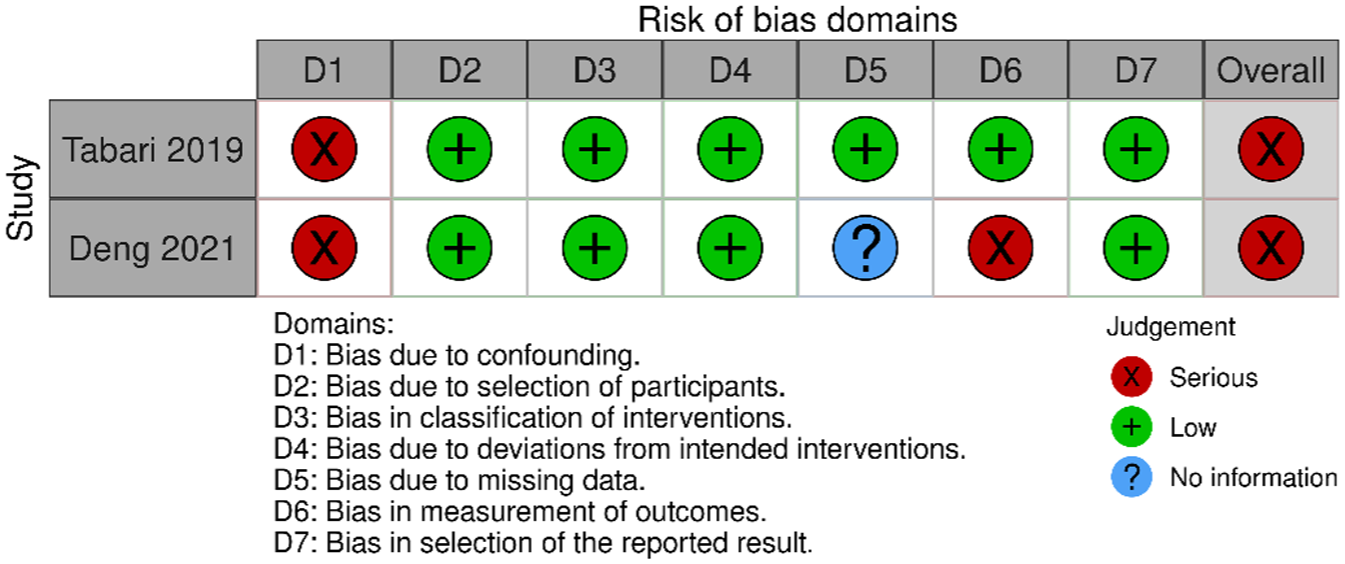
Risk-of-bias assessment traffic light plot. 13
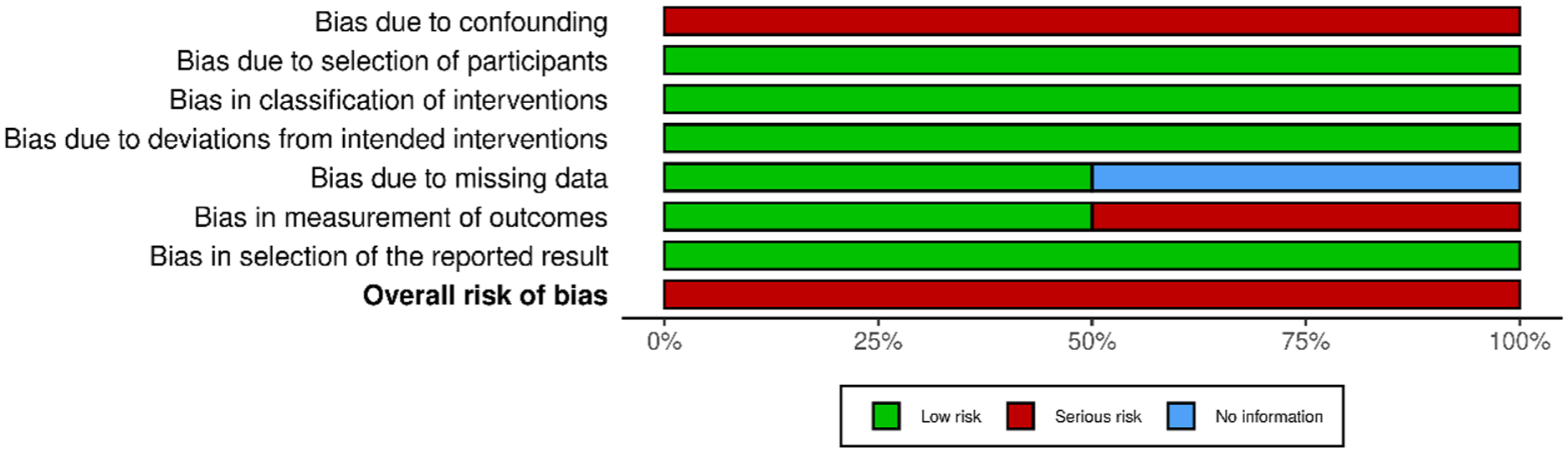
Risk-of-bias assessment summary plot. 12
Bias due to confounding
Both studies appear to have failed in controlling for the important confounding domains, as authors did not use an appropriate analysis method or adjust the study design to achieve control over them. In the study of Tabari et al., there was adequate identification of important confounding domains and measurement of the corresponding confounding variables such as age, gender, APD, SFU, and baseline SRF. Nonetheless, the analysis used, which was a simple Chi square test and not a regression model that would enable adjustment, failed to minimize the risk of bias due to confounding. Similarly, in the study of Deng et al., the authors reported on the baseline confounding variables among the study groups as well as a statistical comparison that does not reveal any statistically significant difference between them. However, the statistical test used to compare them were chi-square and t-tests and not a multivariate analysis as expected. Consequently, the aforementioned omissions introduce serious bias due to confounding. Additionally, in both studies, there were switches between study groups due to secondary surgical interventions, which necessitate the assessment of time-varying confounding. However, neither of the studies report an appropriate analysis method to control for time-varying confounding. Other confounding domains that are not addressed are the socioeconomic status of families and the medical specialty that referred patients to surgery practitioners.
Bias in selection of participants into the study
Both studies were rated low for bias in selection of participants, as they are prospectively recruited studies. Furthermore, participant selection was unrelated to both the intervention and the outcome, and the initiation of the intervention and follow-up occurred simultaneously for all participants.
Bias in classification of interventions
Both studies scored low for this domain, as intervention status was well defined and based solely on what was collected at the time of intervention.
Bias due to deviations from intended interventions
Both studies were rated low, as switches between interventions only occurred in the context of usual practice following an intervention. Moreover, the majority of deviations referred to changes that were consistent with the study protocol.
Bias due to missing data
Tabari (2019): As outlined in the table of follow-up characteristics, the number of participants for whom there was available outcome data coincides with the number of participants enrolled in the study. Consequently, this study scored low for bias due to missing data.
Deng (2021): There was no referral to possible missing data during follow-up, so we could not base a judgment about the risk of bias for this domain.
Bias in measurement of outcomes
Tabari (2019): This study was rated low for the domain of bias in measurement of outcomes. Outcome assessors, in this case nuclear medicine specialists, were blinded to the intervention received by study participants. Moreover, the outcome assessment method, the DTPA exam, was reported to have been conducted out at the same center, using the same protocol for both study groups.
Deng (2021): Although DTPA exams were performed at the same time points and probably at the same center, there is no information on the protocol used for measurements as well as the blinding status of outcome assessors. Thus, considering the potential subjective nature of outcome measure and the assessors’ awareness of participants’ intervention groups, we judged the risk of bias for this domain as serious.
Bias in selection of the reported result
Trial protocols were not retrievable for both studies. However, after comparing methods and results sections and taking under consideration the nature of the specific outcome domain, we concluded that there is no evidence of selective reporting of multiple analyzes and subgroups. Deng et al. selected and reported SRF for both groups at all planned time points. Similarly, Tabari et al. selected and reported SRF, as prespecified, for two groups at two time points. We found no unexplained discrepancies and we therefore rated both studies low for this domain of bias.
Based on the rating of each of the risk-of-bias domains, the overall risk of bias for both studies was judged as serious.
Results of individual studies
Two non-randomized studies compared the SRF between surgical and conservative treatment groups of pediatric patients with UPJO.
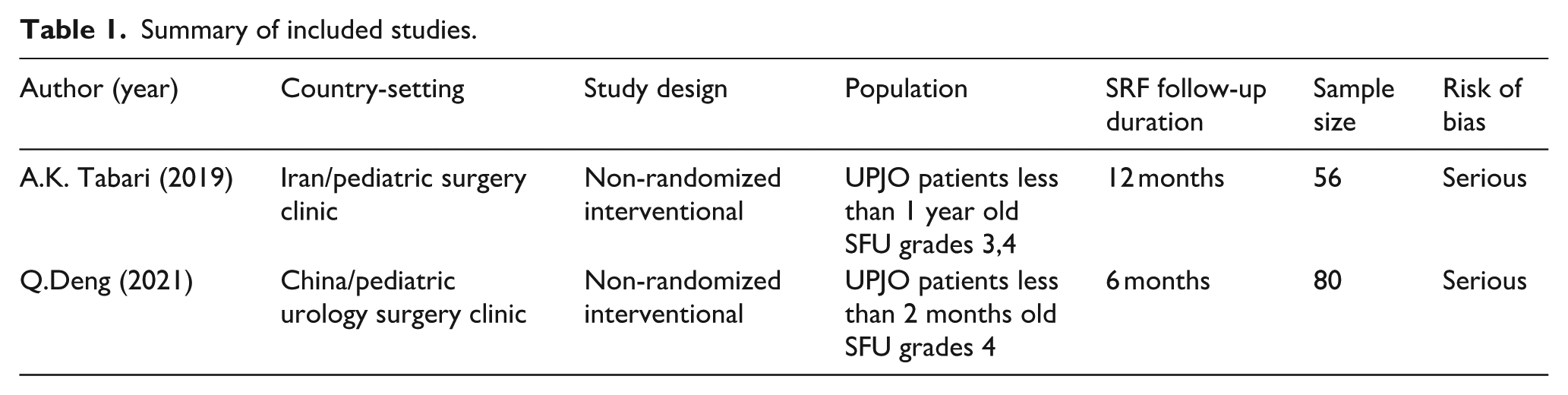
Table 1 presents the summary of included studies. The studies reported their results clearly and consistently, presenting effect estimates in a common format, using means and standard deviations for both baseline and post-intervention outcomes in the intervention and comparator groups. In addition, the studies shared key methodological features, including the same analysis method—allowing estimation of a common effect measure—as well as similar study designs, interventions, and population characteristics.
Summary of included studies.
However, the preliminary plan of a meta-analysis was not feasible due to significant limitations in the available data. Only two studies met the inclusion criteria, and both assessed the main outcome (split renal function) at different time points, preventing meaningful comparison. This inconsistency in outcome timing represented a major barrier to statistical synthesis. Furthermore, both studies were judged to have a serious risk of bias, which undermined the reliability of their findings and made quantitative pooling inappropriate. As a result, we opted for a structured, narrative synthesis of the available effect estimates.
Table 2 presents the results (calculated as the fraction of one kidney of the total renal function and given in percent) along with their effect estimates (mean differences, also expressed as percent), calculated by the review authors. SRF confidence intervals were calculated using the SD and the sample size. Tabari et al. (Tabari, Atqiaee and Mohajerzadeh, 2020) found a small difference of SRF in the surgical group compared to the conservative group at 1 year of follow-up (1.03% higher; 95% CI −2.6690% to 4.7290% higher; 56 participants, 1 study; very low certainty evidence). However, this difference does not appear to be statistically significant. Deng et al. 12 found a higher SRF in the conservative group at the time point of 3 months, reporting no statistical significance (−0.4% higher for the comparator group of conservative treatment; 95% CI −3.5589% to 2.7589%; 80 participants, 1 study; very low certainty evidence). Nonetheless, when examined at 6 months post-intervention, the two groups differed significantly, with the surgical-approach group exhibiting higher measurements of SRF. (3.94% higher for the intervention group of surgical treatment; 95% CI 0.9840% to 6.8960%; 80 participants, 1 study; very low certainty evidence).
Summary of findings: Surgical intervention compared to conservative management for unilateral UPJO.
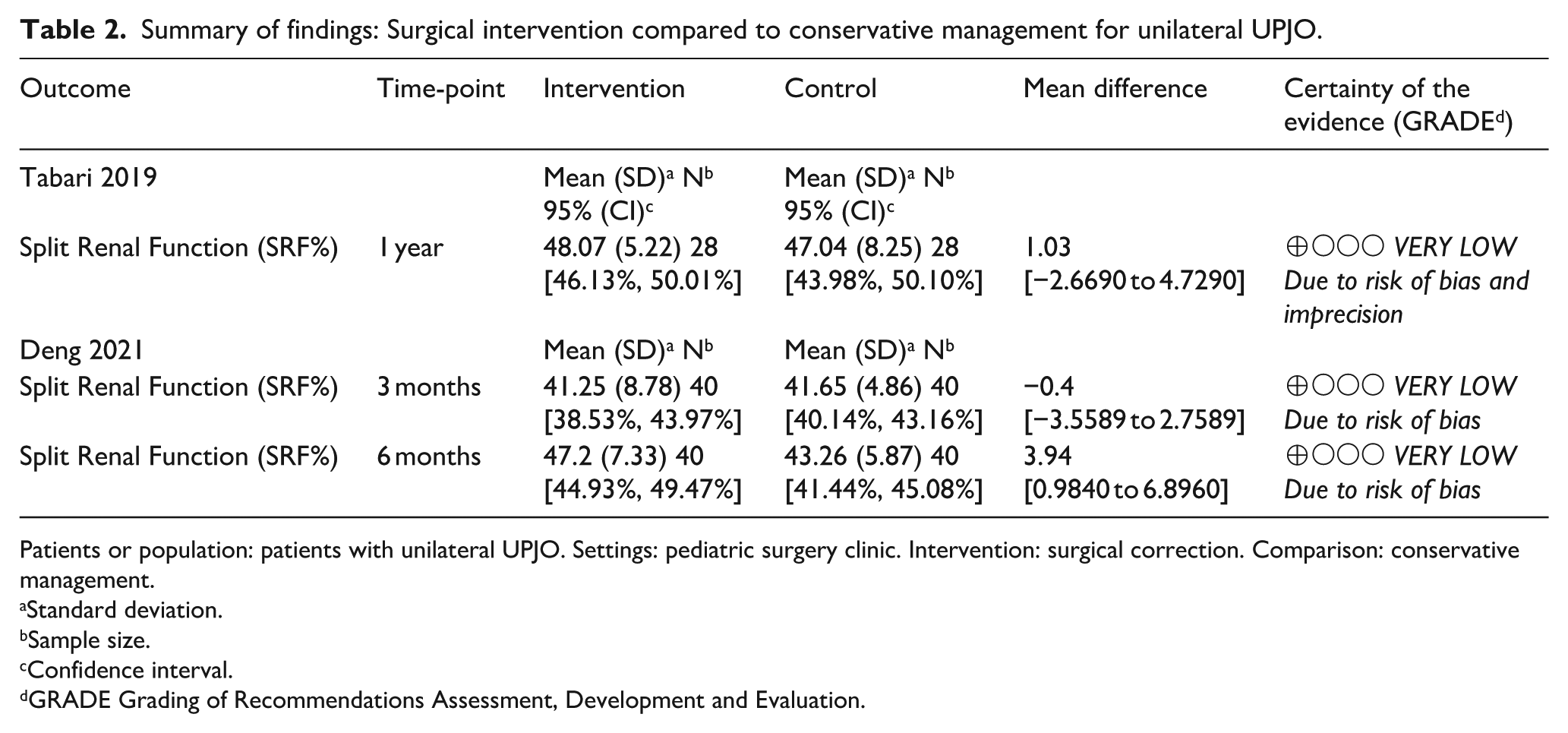
Patients or population: patients with unilateral UPJO. Settings: pediatric surgery clinic. Intervention: surgical correction. Comparison: conservative management.
Standard deviation.
Sample size.
Confidence interval.
GRADE Grading of Recommendations Assessment, Development and Evaluation.
Both studies lacked reporting of SRF confidence intervals. After calculating them, we concluded that neither group, at any reported timepoint, crossed the clinically important threshold of 40%. This suggests that, even when a statistically significant difference was observed, it did not necessarily indicate clinical significance. The omission of SRF confidence intervals may have affected the ability to assess clinical relevance and represents a potential source of interpretive bias.
The overall level of certainty in the body of evidence regarding the SRF, was rated very low for both included studies, as illustrated in the summary of findings table (Table 2). The quality of evidence initially received a low rating, as defined for evidence deduced from observational studies and it was further downgraded to very low, for bias and imprecision. Serious risk of bias in both studies further downgraded the quality of evidence, as the risk-of-bias rating was attributed to a fundamental failure to adjust for confounding that weakens the confidence in the results. Additionally, in the case of Deng, bias in measurement of outcome due to lack of blinding, questioned the credibility of the results.
As far as Tabari is concerned, the level of certainty was also lowered for imprecision. This decision was taken on the basis of the wide confidence interval at 6 months, which included both possible harm and effect, and the small total sample size of 136, which did not meet the rule of thumb of 400 events.
Discussion interpretation
To the best of our knowledge, we present the first SR comparing surgical and non-surgical management of UPJO, 8 years after the respective Cochrane SR published in 2016. 2 This review included two studies which albeit their limitations, addressed the review question successfully. The studies shared similar study design, examined population with a common, well-defined pathology, used the same exclusion criteria and assigned subjects to similar interventions. However, their results could not be comparable, as authors examined populations of different mean age and, more importantly, assessed the main outcome at different time points.
Deng et al. (2021) reported a higher, but not statistically significant SRF in the conservative team at 3 months of follow-up, but this result was reversed after 6 months of follow-up. At this time point, Deng reported a statistically significant higher SRF in the surgical group. This change, although statistically significant, may not represent a clinically important difference. A critical change in SRF is considered a change above 10%. In this case, a mean difference of 3.94 (0.9840–6.8960), without longer follow-up, could be attributed to measurement variability. Indeed, Tabari et al. (2020), did not confirm this result at 1 year of follow-up. This inconsistency raises questions about transient or symptomatic changes in SRF. It also highlights the importance of long-term follow-up of pediatric patients which are in a state of ongoing development. Patients’ age is crucial for evaluation of SRF, as it physiologically changes over time, even in patients with renal pathology, until the age of two. Ideally, interventions performed only after the age of two, could provide the potentiality of an objective comparison.
The results of the previous systematic review of Cochrane that addressed the same question were similar. 2 In both studies included in the aforementioned review, SRF did not differ significantly between the surgical and conservative treatment groups. Despite included studies being RCTs, authors judged the quality of evidence as very low. Weitz et al., 14 in another systematic review examining the effects of non-surgical management of unilateral UPJO, noted that 21% of patients had a risk of renal function deterioration. However, this was highly noted even in patients submitted to secondary surgical intervention. This finding questioned the potentially protective role of surgery on renal function. Moreover, data contributing to this evidence mainly consisted of qualitative statements deduced from descriptive studies, thus degrading the trustworthiness of the evidence. Although the ideal timing and indications of surgery still remain unclarified, there is abundant research on surgery techniques. Laparoscopic and robotic approaches have gained ground due to their less invasive character, but endopyelotomy remains an option, especially the low-pressure approaches.15,16
Limitations of evidence
This review is limited by the small number of eligible studies and the small number of participants, despite them being adequately representative of the population of interest.
The value of evidence is critically downgraded by the risk of bias in the studies. The overall risk of bias for both studies was assessed as serious. Inadequate control for confounding domains in both studies interfered with the treatment effect and biased the results. For example, age at the time of intervention and SFU grade critically affect renal function irrespective of the treatment choice. Similarly, time-varying confounders may have led to switches between study groups and could have affected the outcome values, interfering with the direct causal association between treatment and outcome. As far as blinding is concerned, it was applied to outcome assessors in Tabari et al. (2020). In contrast, Deng et al. 12 made no reference to the blinding of investigators, even though it would be possible to apply blinding of nuclear medicine specialists. Lack of blinding could introduce measurement bias, as unblinded assessors may have had expectations of improvement in the surgery group and may have overestimated the SRF measurements. Moreover, Deng et al. 12 , in spite of defining the initial number of study sample, does not clearly state whether it coincides with the number of patients that was eventually analyzed or whether there were losses to follow-up. Consequently, lack of adequate reporting, could be attributed to selective reporting.
As far as adherence to intention-to-treat analysis is concerned, there is a lack of referral and clarification of the way patients with secondary surgical intervention were analyzed.
According to the GRADE approach, the studies were also evaluated for imprecision. Comparison of SRF at 1 year of follow-up produced a wide confidence interval for the treatment effect, which does not support a justifiable clinical decision.
Taking all the aforementioned deficiencies into consideration, the quality of evidence was rated very low, further limiting the validity of our results.
Design of included interventional studies that lack randomization consists an additional limitation, as, according to the evidence pyramid, it downgrades the trustworthiness of the evidence. Nonetheless, a randomized study that assigns patients to either a surgical or a non-surgical intervention, raises crucial ethical concerns, making the choice of this design understandable and the existence of relevant RCTs rather questionable. Surprisingly, studies included in the previous SR, were RCTs, which may reflect a concerning approach of the past. The problem of absence of recent RCTs that we encountered during our search reflects the evolvement of clinical approach to a more ethical and holistic one, that involves carers in the final decision. Moreover, a stratification by SRF that aligns with the current guidelines may help guide surgical decisions and future studies.
The non-surgical treatment arm consisted of repeated imaginary tests with or without antibiotic prophylaxis. However, as indicated by Weitz, 14 ultrasound findings of anteroposterior pelvis dilatation may fail to evaluate the severity of the condition, endangering renal function. On the other hand, repeated scintigraphic imaging tests that reliably evaluate drainage pattern and renal function, expose patients to substantial radiation. Currently, there are constantly emerging alternative methods of assessing renal injury, including biomarkers and sophisticated techniques such as urinary proteomic analyzes that could be used in the conservative-treatment group. These methods could represent a more sensitive means of monitoring, improve patients’ quality of life and alter their long-term prognosis.
Finally, patients of included studies were monitored for only a short follow-up period of up to 1 year. This lack of longitudinal data can determinately affect the applicability of results because of the uncertainty of the long-term impact on renal function, considering that renal development continues into early childhood.
Limitations of review processes
The literature search was extensive considering the formulated search strategy. Nonetheless, the post hoc modification of our eligibility criteria and inclusion of non-randomized clinical studies constitutes the main limitation of the review process. Initial application of RCT search filter and time restriction to studies published in 2016 onward, may have led to the omission of eligible non-randomized studies. However, the inclusion of non-randomized studies, when it comes to proceeding or not to a surgery, is ethically acceptable. Depriving a surgery from a patient that is at risk for chronic renal disease or subject another to an intervention that may be accompanied by complications, is ethically unacceptable. The search was limited to two databases, MEDLINE and CENTRAL, which, however, according to Cochrane guidelines, 17 are the two most important databases for addressing intervention-related review questions. Consequently, we are confident that the comprehensiveness of our review was not affected determinately. The Embase database, which is also recommended, was not searched, as access was not available to review authors. Two review authors screened independently the search results, while one review author conducted the data extraction. Nonetheless, given the small number of included studies, we believe the risk of error introduced by single-reviewer extraction was minimal. Due to time restrictions, we did not contact authors to retrieve study protocols and clarify ambiguities. Risk of bias and certainty of the evidence was rated by one review author, and, due to inadequate and imprecise data, we did not proceed to planned statistical synthesis.
Conclusions
The outcomes of this review, being inconclusive and of low quality, cannot guide clinical decisions. We found limited data which indicate that patients with UPJO seem to benefit from a surgical approach regarding their renal function, but this finding is not supported by the second included study, which shows that surgery does not alter significantly clinical course and renal function. Additionally, there are no longitudinal data to confirm this result over a longer follow-up period, beyond 1 year. More importantly, the limited reliability of the evidence precludes for drawing definite conclusions, let alone making clinical practice recommendations. The lack of trustworthy evidence on best treatment option for patients with grade 3 and 4 UPJO was also highlighted in the previous SR. 2 Our review confirms this deficiency 8 years later. Surprisingly, despite the review question addressing a common clinical problem, very few relevant clinical studies were conducted during this time interval. Meanwhile, new, noninvasive techniques of evaluating renal ongoing damage have emerged, such as urinary proteomic profiling.
Our understanding of UPJO pathophysiology and optimal treatment would benefit from large, prospective, well-designed clinical trials. These should include patients across different age groups, receive the most appropriate surgical interventions based on the latest evidence, and be compared with all currently available conservative treatment options. Additionally, we highly recommend incorporating aspects of undesirable treatment effects and follow-up patients for longer intervals to determine their prognosis. Moreover, a review of all existing studies, including retrospective studies could generate further clarification on the subject and provide guidance on design of future studies. Given the current state of knowledge, it is evident that a personalized approach, that evaluates the risks and benefits for each patient and involves carers in the final decision, remains a necessity. Current guidelines provided by pediatric urology associations are not based on strong evidence and are expected to be formulated by multicenter, well-designed studies. This review underscores the remaining controversy and highlights the need for further research on this clinical question.
Supplemental Material
sj-docx-1-urj-10.1177_03915603251384442 – Supplemental material for Comparison of surgical versus conservative treatment in ureteropelvic junction obstruction: A systematic review of non-randomized trials
Supplemental material, sj-docx-1-urj-10.1177_03915603251384442 for Comparison of surgical versus conservative treatment in ureteropelvic junction obstruction: A systematic review of non-randomized trials by Despoina Samourkasidou, Despoina Tramma, Nikolaos Gkiourtzis, Vaia Dokousli, Thomas Karagiannis and Michalis Aivaliotis in Urologia Journal
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
“Ethical approval was not required.”
Consent to participate
Not applicable.
Consent for publication
Not applicable.
ORCID iDs
Data availability
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.