
Abstract
Background:
We describe a modified technique for laparoscopic radical cystectomy (LRC) utilizing a mini-laparotomy incision for conduit formation and compare outcomes with the conventional technique.
Materials and methods:
This retrospective single-centre study included patients with bladder cancer undergoing LRC at a tertiary care centre between September 2019 and December 2024. Patients were divided into conventional LRC (CLRC) and modified LRC (MLRC) groups. Statistical analysis was performed using chi-square and Student’s t-test (p < 0.05 considered significant).
Results:
A total of 228 patients were included (CLRC: 58; MLRC: 170). Operative time was significantly longer in MLRC (253 vs 246 min, p = 0.0018). However, mean blood loss (370 vs 543 ml, p < 0.001), incision size (8.5 vs 14.5 cm, p < 0.001), time to oral intake (3.5 vs 3.8 days, p < 0.001), and hospital stay (10.8 vs 11.6 days, p < 0.001) were significantly reduced. Two early postoperative deaths (Clavien–Dindo Grade V) occurred in CLRC. At 2-year follow-up, recurrence (7.1% vs 10.3%) and mortality (1.2% vs 5.2%) were comparable between groups.
Conclusion:
The modified technique is feasible and reproducible. Despite longer operative time, it significantly reduces postoperative morbidity with comparable short-term oncological outcomes.
Introduction
Bladder cancer is one of the most common malignancies involving the urinary tract.1,2 Patients with bladder cancer are diagnosed late in life with median age being 65 years and usually suffer from multiple co morbidities which add to the morbidity. Radical Cystectomy (RC) along with bilateral pelvic lymph node dissection (PLND) is the gold standard curative treatment for Muscle Invasive Bladder Cancer (MIBC) and very high grade non-MIBC. The surgery is combined with neo-adjuvant and adjuvant chemotherapy for advanced malignancies. 1 After surgery, the 10-year recurrence-free survival rate is reported to be 50%–59% with overall survival rate being 45%.3,4 Recent EAU 5 and AUA 6 guidelines continue to recommend radical cystectomy as the standard of care for muscle-invasive bladder cancer. Radical cystectomy can be done as open approach or by minimal invasive approaches – laparoscopic RC (LRC) or robot-assisted RC (RARC). 1
Open RC might be associated with high surgical morbidity and mortality rate (30%, 1.5%), which might delay the recovery period and prolong the hospital stay. 7 These will consequently delay the adjuvant treatment in these patients. To reduce the morbidity associated with the open approach, minimal invasive techniques were introduced like Laparoscopic and robotic RC. LRC was introduced by de Badajoz et al. 8 After its introduction, it was adopted at many centres all over the globe. The advantages of LRC are reduced blood loss, less analgesic requirement and early discharge from hospital and return to work and normal activities. 1 However, it has a long learning curve. The conventional LRC is done with five ports with ileal conduit and/or orthotopic urinary diversion (Studer technique). The creation of ileal conduit requires a laparotomy incision, thereby increasing post-operative morbidity. With the introduction of Robotic Surgical system, the RARC procedure has gained a wide popularity because of its ease to the surgeon and lesser complications, though with longer operative time and more costs.1,9 Although robot-assisted radical cystectomy has gained widespread popularity, its adoption remains limited in resource-constrained settings due to high costs and infrastructure requirements. Consequently, there is a need for cost-effective minimally invasive alternatives that can deliver comparable perioperative and oncological outcomes. Due to the cost limitation of RARC, the LRC technique might be considered in Indian centres, especially where there is no robotic surgical system installed. Here we present LRC by a modified technique with a mini-laparotomy incision for conduit formation and compare with the conventional LRC done at the same institute.
Materials and methods
This is a retrospective study of all patients with MIBC and very high-risk non-MIBC who were managed at a tertiary care centre in central India over a period of 64 months from September 2019 to December 2024. The follow-up duration was 2 years (telephonic and physical). The records were retrieved from the medical record department of the institution.
The inclusion criteria were all patients with biopsy confirmed MIBC after Trans-urethral resection of bladder tumour (TURBT); Early cystectomy was performed in very high risk non-MIBC patients who had BCG failure and those patients with non-MIBC (HG pT1 stage) who were willing for LRC; patients undergoing palliative LRC to manage refractory haematuria, obstructive uropathy and bladder perforation.
All patients were admitted and after routine blood and radiological investigations, underwent TURBT. The management then proceeded as per the histopathology report. Initially, LRC and bilateral PLND was done as per standard five port technique, with ileal conduit and/or orthotopic urinary diversion (Studer technique) – labelled as CLRC for ease of comparison. Extracorporeal anastomosis was done with a large lower midline laparotomy incision initially from 2019 to 2020. But, from 2021 onwards, the LRC was done by a modified technique, referred to MLRC for ease of comparison. In MLRC, the size of laparotomy incision was reduced to 6–8 cm midline incision (mini laparotomy incision) and the small bowel was scored laparoscopically and specimens with ureters were held with graspers separately, easing the delivery of specimens through small wound. In all female patients, the specimen was delivered through vaginal vault prior to its closure.
Surgical Procedure of MLRC: Patient was kept in lithotomy position and pneumoperitoneum was created with Veress needle through supraumbilical incision. The port placement is shown in Figure 1. The position was then changed to steep Trendelenburg. Right ureter was first identified and dissected up to right VUJ preserving the periureteral adventitia. Lateral vesical space was created incising the peritoneum lateral to medial umbilical ligament up to levator fascia. Spermatic cord was then clipped and divided. Posterior peritoneum was incised and plane between peritoneum and bladder extended upto base of prostate by incising Denonvillers fascia. Lateral vesical pedicles were controlled with bipolar vessel sealing device, connecting posterior and lateral vesical space. Similar steps were repeated on left side, thereby completing the bladder drop. DVC was controlled with Vicryl 2-0 suture and prostatic urethral junction was dismembered, foleys was clipped and divided. Prostatic apex was separated from rectum by retrograde dissection, specimen was placed in left para colic gutter.
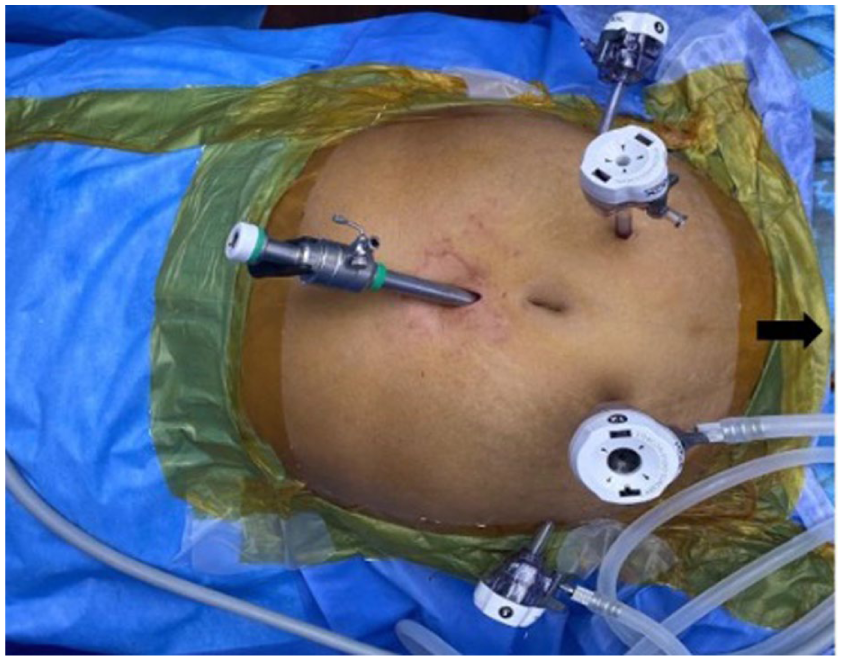
Port positioning in MLRC (black arrow represents foot end).
After completing bilateral extended PLND, the left ureter was tunnelled through sigmoid mesentery and both the ureters were grasped using forceps (Figure 2). Small bowel was marked 15 cm proximal to ICJ with two sutures and grasped with forceps (Figure 3). The marked small bowel and bilateral ureters were delivered through an 6–8 cm midline laparotomy incision. Bowel anastomosis was done by firing two 60 mm blue cartridge, mesentery was closed and proximal ileal conduit was closed with vicryl 3-0; bilateral uretero-enteric anastomosis done over 7 Fr IFT using brickers technique. Distal PDS loop 1-0 after placing 20 Fr abdominal drain. Figure 4 shows the post-operative image of the sutured midline incision.
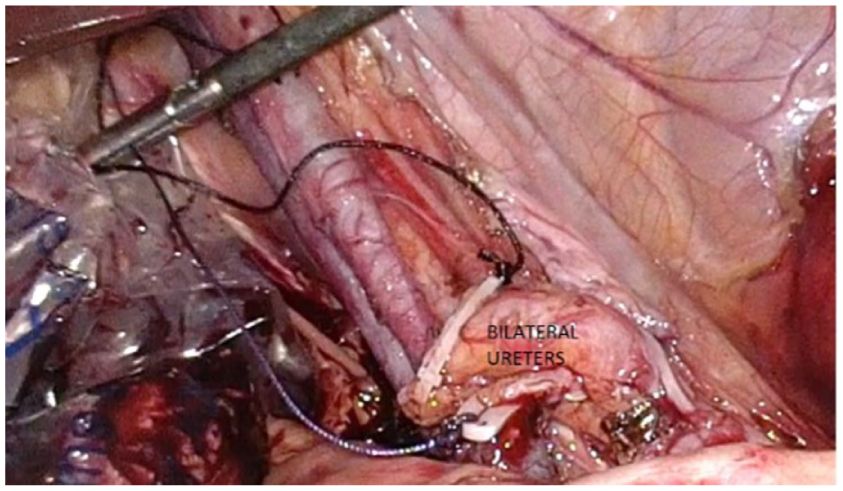
Bilateral ureters grasped with forceps.
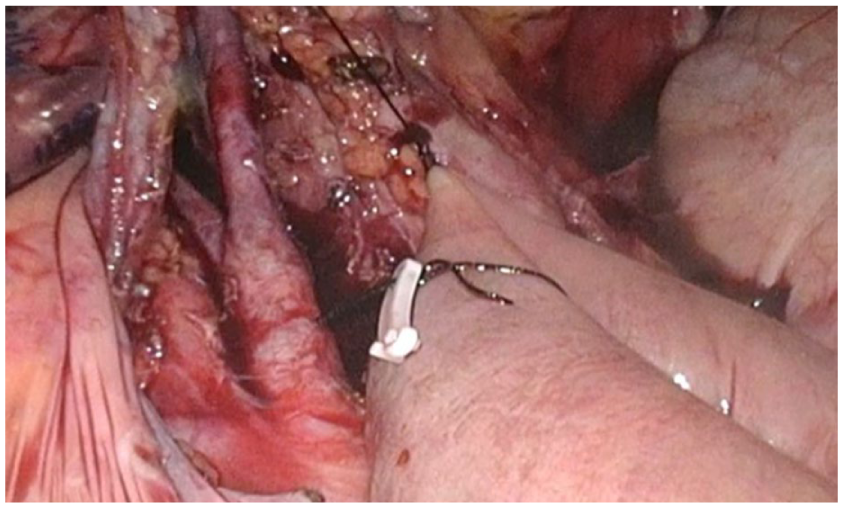
Bowel grasped prior to 19 cm laparotomy incision (proximal clipped suture, distal suture with knot).

Post-operative image of the sutured midline incision.
Post-operatively, DVT prophylaxis was given and the patients were kept nil by mouth till return of bowel motility; orals were usually started by third post-operative day. Early mobilization was preferred usually starting from post-operative day 1 onwards. Post-operatively, intravenous antibiotics were given till day two and then oral antibiotics were started.
Patients were planned for adjuvant therapy-based on histopathology report. After discharge, patients were followed up regularly, first at 7 days with histopathology report. Further follow up was planned as per the stage of the disease; usually at 3 months; then every 6 months for 2 years and then annually thereafter. Percentage of patients alive at 2 years was ascertained telephonically.
The data obtained from the MRD was entered into the excel sheet and analysed with respect to (i) demographic profile – age, gender, high-risk factors, co-morbidities, the type of TURBT histopathology undergoing LRC; (ii) intra-operative data – operative duration, blood loss, incision size, intra-operative complications; (iii) post-operative data – complications based on Clavin-Dindo grading, hospital stay and (iv) follow-up – the histopathology, the adjuvant therapy, recurrence at 1 and 2 years and survival at 2 years.
The retrieved data was entered in Excel sheet and arranged into tables to conclude the findings of the study. Analysis was done by SPSS™. Descriptive analyses were performed. All data were analysed for normality; those with a normal distribution were reported as mean with standard deviation, and those with a skewed distribution were reported as median with range. For comparison of the study variables, chi square or student t-test was used with significance set at a p-value of <0.05. Ninety-five percent confidence intervals (95% CI) were calculated for key continuous variables; categorical variables were presented as frequencies and percentages. No multivariate analysis was performed, which is acknowledged as a limitation of this study
Results
During the above-mentioned period, a total of 228 patients with bladder cancer underwent LRC; 58 patients underwent LRC by conventional technique (CLRC – done in the initial years 2019 and 2020) and 170 patients underwent LRC by the Modified technique – MLRC. The demographic profile is presented in Table 1. There were more males than females and smoking was the commonest risk factor in both the groups. All patients presented with painless haematuria. TURBT could be completed in 80% of patients. Amongst the 228 patients, 200 patients had MIBC, 18 patients had NMIBC (14 had BCG failure and 4 had high grade pT1 stage) and 10 patients underwent Palliative Cystectomy (5 had obstructive uropathy, 3 had refractory haematuria and 2 had bladder perforation). At CT evaluation, the median tumour size was 5.5 cm (range: 3.1–8.8 cm) and posterior wall was the commonest involved site seen in 48% of patients followed by lateral walls in 36% patients.
Demographic profile.
Table 2 compares the intra-operative events amongst the two groups. The duration of surgery was significantly increased in the MLRC group (p-value 0.0018) but the mean blood loss and the mean incision size was significantly decreased (p-value 0.0001 for both). The increased duration could be attributed to additional time taken to mark bowel and ureters, thereby reducing incision size.
Intra-operative events.
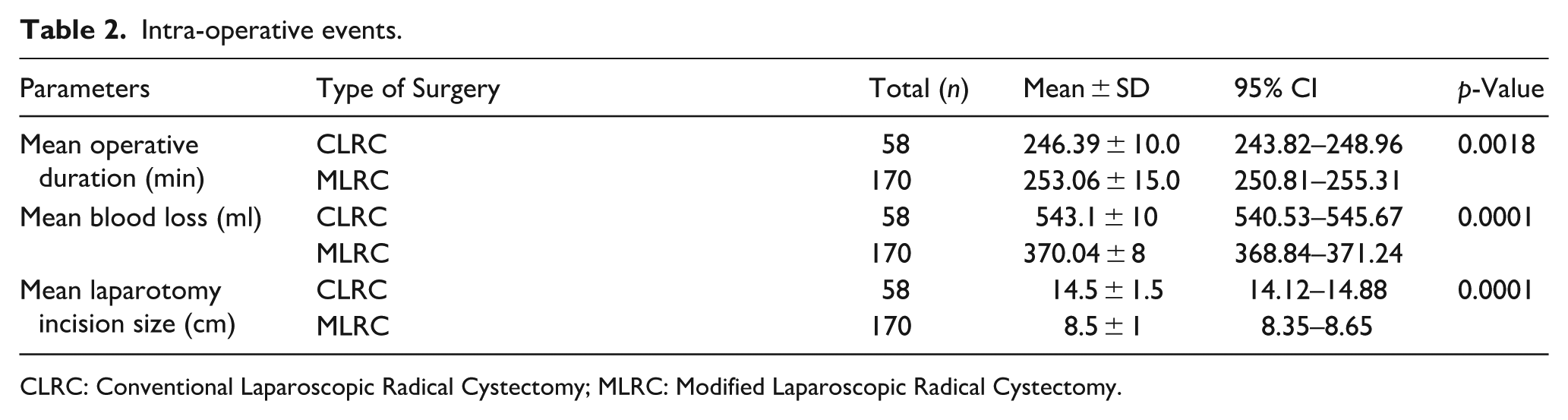
CLRC: Conventional Laparoscopic Radical Cystectomy; MLRC: Modified Laparoscopic Radical Cystectomy.
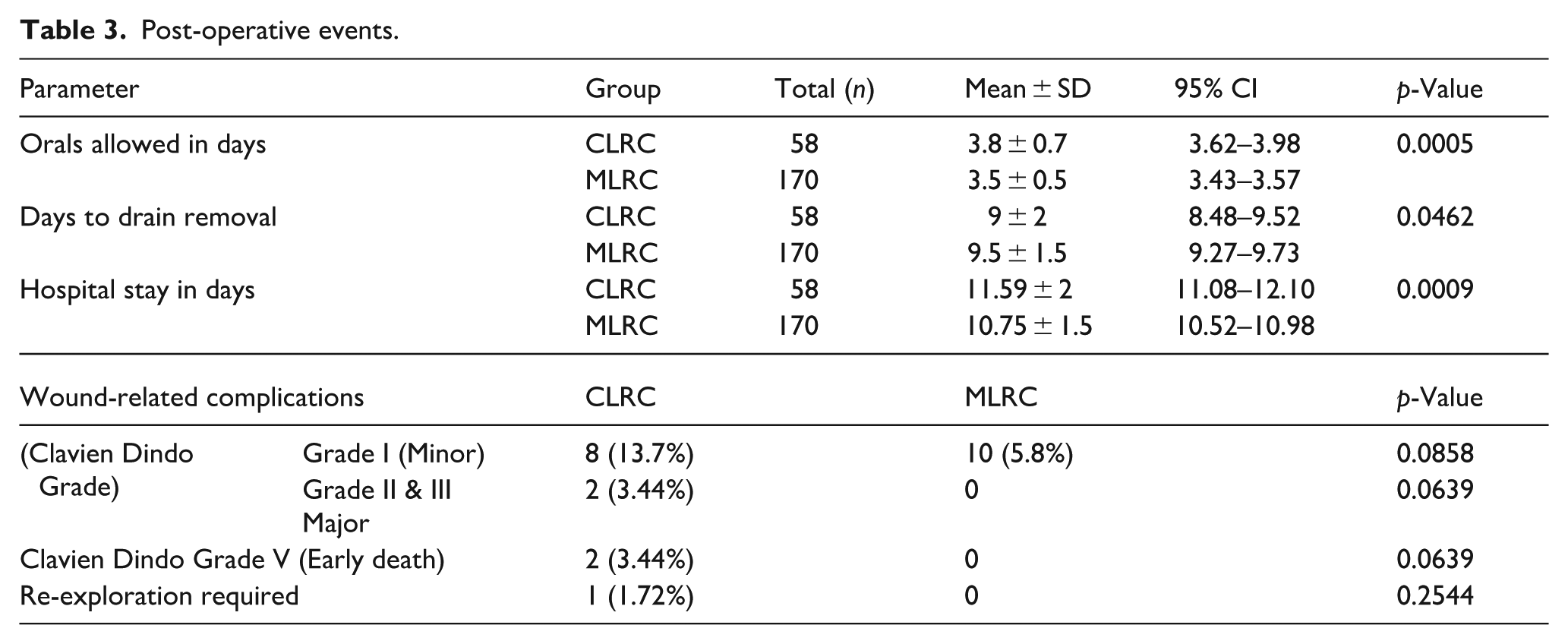
The comparison of post-operative events and complications amongst the two groups is depicted in Table 3. The time to oral intake (time from operation to orals allowed) and duration of hospital stay was significantly decreased in the MLRC group (p-value 0.0005 and 0.0009 respectively). There was marginal difference in days to drain removal as well (p-value being 0.0462). However, there was no statistically significant difference in wound-related complications. Two early postoperative deaths were observed in the CLRC group, classified as Clavien–Dindo Grade V complications
Post-operative events.
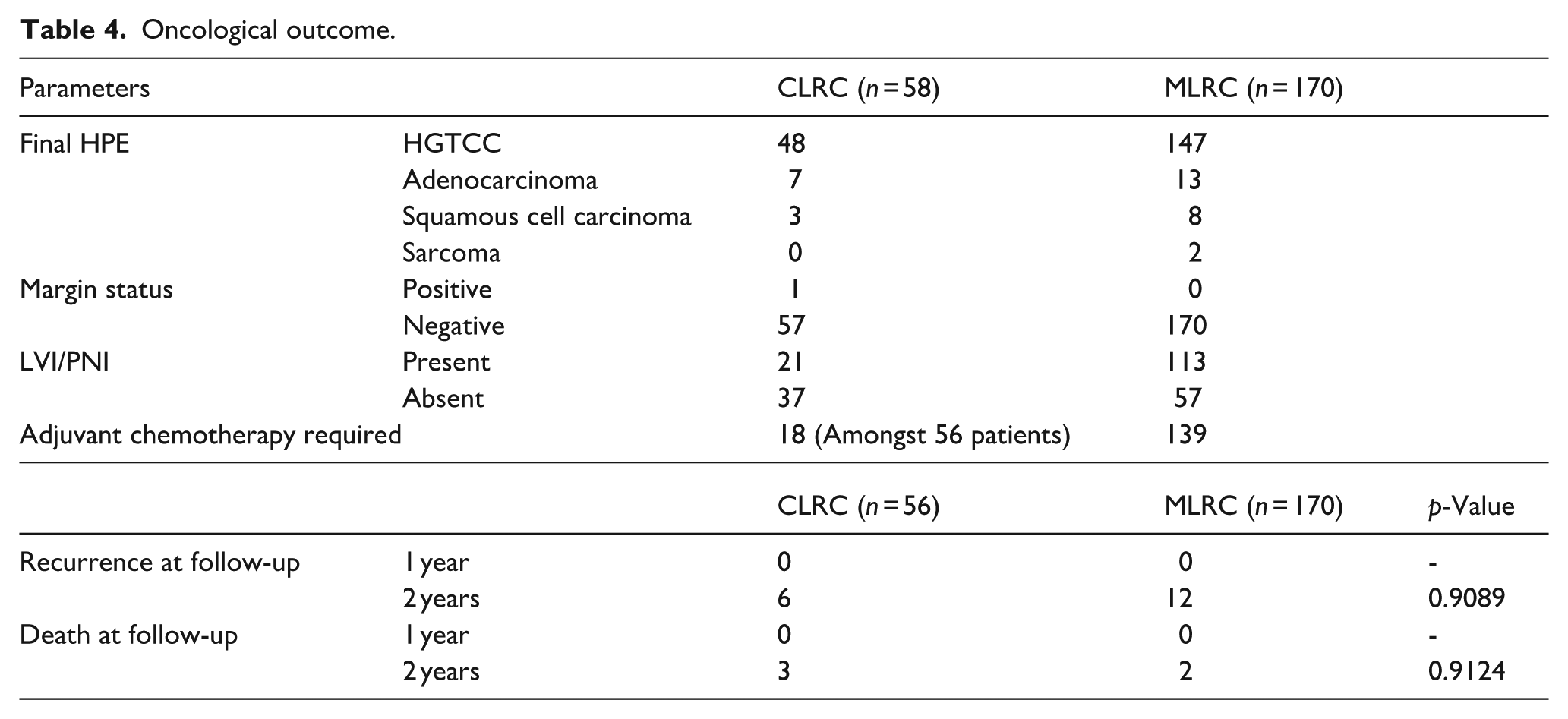
Oncological outcome is compared in Table 4. TCC was the commonest histopathology seen in 92.98% of the patients with the commonest stage being pT3-T4 disease diagnosed in about 65% of patients; 48 in CLRC group and 147 in MLRC group. There was only one patient with positive margins; in CLRC group. Mean number of nodes harvested per patient was 18 ± 4. Lympho-vascular and perineural invasion was seen in 21 patients in CLRC group and 113 patients in MLRC group. Adjuvant chemotherapy was given in 18 patients in CLRC group and 139 patients in MLRC group. There were no recurrence or death in first year in both groups. At the end of 2 years, six patients (10.3%) in the CLRC group and 12 patients (7.1%) in the MLRC group developed recurrence and three patients (5.12%) in the CLRC group and two patients (7.1%) in the MLRC group had died. However, the difference between the two was not statistically significant.
Oncological outcome.
Discussion
The standard management of patients with MIBC is Open Radical Cystectomy (ORC) and it offers the longest cancer-specific survival. 1 Even the 2016 EAU guidelines state that ORC should be offered to all patients as better rates are obtained with use of multidisciplinary therapy – radiotherapy and chemotherapy.1,3 However, with improvements in minimal access surgery, LRC gained wide popularity since the end of the 20th century 1 ; the peri-operative complications being less and recovery faster (in view of improved cosmesis, decreased postoperative pain and shorter recovery) along with good malignancy control and similar oncological outcomes when compared to ORC.1,10,11 Thus, it has emerged as an attractive technique to patients and surgeons alike. 10 However, careful patient selection and advanced laparoscopic skills are required for optimal outcomes in LRC. 12 Surgeon’s fatigue is yet another factor to be looked into. 13 Continued developments in the field of single-site surgery and robotics provide significant improvements over current techniques and outcomes like the four-tier hybrid classification in predicting recurrence and progression in patients with stage Ta NMIBC.12,14,15 With this study, we retrospectively compared patients with bladder malignancy undergoing conventional LRC (CLRC) and modified LRC (MLRC) at our institute.
As is well known, LRC with intestinal urinary reconstruction is a major and complex operative procedure with significant complications and mortality.2,16–19 The preparation of ileal conduit after LRC increases the chances of bowel-related complications like obstruction, leak and perforation. 2 Also, the large laparotomy incision increases the rate of wound-related complications. Hence, perioperative management plays an important role to reduce the hospital stay and in improving patient quality of care. 2 In this study, we modified the LRC and decreased the mean size of incision from 14.5 cm in CLRC to 8.5 cm in MLRC. Though the intra-operative time was significantly increased, the hospital stay, time to oral and days to drain removal were significantly reduced. The wound related complications, though less in MLRC group, were not statistically significant. The oncological outcome was also similar. The increased operative duration observed in the MLRC group may be attributed to the additional steps involved in bowel marking and ureteric handling. However, this is likely to improve with increasing surgical experience, reflecting a learning curve effect.
Recently, there has been considerable debate on LRC with main focus on the urinary diversion technique – as to whether an intracorporeal technique is more beneficial than an extracorporeal technique. The intracorporeal technique looks definitely aesthetically superior, in women, where a vaginal specimen extraction is obtained, resulting in a truly ‘incision-free’ cystectomy, the intra-operative time is increased significantly in males which has been found to be associated with a higher rate of bowel-related complications in initial series by Haber et al. 20 Although intracorporeal bowel surgery is becoming more popular, in our study, we shifted to mini-laparotomy incision and just scored the bowel intra-corporeally, thereby the intra-operative time did not increase much. Recent studies on robotic intracorporeal urinary diversion have demonstrated improved perioperative outcomes but at significantly higher cost and infrastructure requirements. In this context, the MLRC technique offers a cost-effective alternative, particularly relevant in resource-limited settings. 15
In our study, there were no major complications and two early postoperative deaths in CLRC, that too in elderly and co-morbid patients. The disease-free survival at the end of 2 years was 88.86% in CLRC group and 92.85% in MLRC group which is comparable with that reported in literature by Hemal et al. 21 – amongst 48 patients, 3-year cancer-specific survival rate of 73% and one postoperative death from sepsis. 21 Huang et al. 22 has reported the largest published study currently available in171 patients with a median follow-up of 3 years. 22 They reported the 5-year overall, cancer-specific and recurrence-free survival rates to be 74%, 81% and 73%, respectively, with a median follow-up of 37 months. 22 Haber and Gill 23 reported the intermediate-term oncological outcomes of 37 patients with a follow-up of 5 years. In their study, the 5-year overall and cancer-specific survival was 63% and 92%, respectively. 23
This study has some limitations – its retrospective design, small sample size, same operative team and short follow-up time. Larger multi-centre randomized controlled trials would be required to furnish better quality evidence to support this technique. However, it can be concluded that the MLRC technique can act as a bridge in the learning curve of urologists while transition from extra-corporeal to totally intracorporeal LRC. These findings should be interpreted with caution due to the retrospective design, single-centre setting, short follow-up duration and absence of multivariate analysis. The surgical time though is increased; but the post-operative morbidity is significantly reduced with similar oncological outcome. This can be used in institutions where the robotic surgical system is yet to be installed.
Conclusion
The modified technique is feasible and reproducible. Despite longer operative time, it significantly reduces postoperative morbidity with comparable short-term oncological outcomes.
Footnotes
Acknowledgements
None.
Author note
This manuscript has been read and approved by all the authors, the requirements for authorship have been met and each author believes that the manuscript represents honest work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.