
Abstract
Background:
Urethral stricture (US) disease frequently recurs after direct visual internal urethrotomy (DVIU). This study investigated the prognostic value of serum creatinine, estimated glomerular filtration rate (eGFR), and the hemoglobin/creatinine (Hgb/Cre) ratio for predicting 12-month recurrence in short-segment bulbar US.
Methods:
A retrospective cohort of 237 patients undergoing DVIU for isolated bulbar US <2 cm between 2012 and 2024 was analyzed. Demographics, comorbidities, laboratory parameters, and uroflowmetry were recorded. Renal function markers (creatinine, eGFR) and Hgb/Cre ratio were evaluated using receiver operating characteristic (ROC) analysis, Kaplan–Meier survival curves, and multivariable logistic regression.
Results:
Recurrence occurred in 103 patients (43.5%) within 12 months (median: 6 months). Patients with recurrence had higher creatinine (1.10 vs 0.99 mg/dL, p < 0.001), lower eGFR (74.0 vs 88.0 mL/min/1.73 m2, p < 0.001), and lower Hgb/Cre ratios (12.13 vs 14.28, p = 0.002). Endoscopic surgery–related etiology was strongly associated with recurrence (70.8% vs 47.0%, p = 0.001), whereas age, hemoglobin, Qmax, and PVR showed no significant relationship. In multivariable models, elevated creatinine (OR 3.47, 95% CI 1.82–6.60), reduced Hgb/Cre ratio (OR 0.90, 95% CI 0.85–0.95), and lower eGFR (OR 0.975, 95% CI 0.964–0.987) independently predicted recurrence. Kaplan–Meier analysis demonstrated significantly higher recurrence in patients with creatinine ⩾ 1.02 mg/dL, eGFR ⩽ 80.5 mL/min/1.73 m2, and Hgb/Cre ratio ⩽ 13.26.
Conclusions:
Elevated serum creatinine, reduced eGFR, and a lower Hgb/Cre ratio are independent predictors of 12-month recurrence following DVIU for short-segment bulbar US. Demographic and uroflowmetric parameters showed limited predictive value, whereas iatrogenic etiology markedly increased recurrence risk. Incorporating renal function markers into risk stratification may guide patient selection and support timely consideration of urethroplasty or drug-coated balloon dilatation (Optilume) in high-risk individuals. Prospective multicenter studies are warranted.
Keywords
Introduction
Urethral stricture (US) disease is a common cause of lower urinary tract symptoms (LUTS) in men and is associated with significant morbidity and a substantial healthcare burden. Epidemiological studies report a prevalence of 229–627 per 100,000 men, with incidence increasing with age. 1 The anterior urethra accounts for the majority of cases (92.2%), with the bulbar urethra being the most common subsite (46.9%). 2 In the United States alone, the condition accounts for an estimated 5000 hospitalizations and 1.5 million outpatient visits annually. These figures highlight both the clinical and socioeconomic importance of the disease. Pathophysiologically, US develops following insult to the urethral mucosa, leading to inflammation, collagen deposition, and eventual scar formation in the corpus spongiosum. Repeated cycles of injury and healing drive progressive spongiofibrosis and urethral lumen narrowing. Etiologically, most cases are related to iatrogenic factors—such as endoscopic manipulation or catheterization—while trauma, infections, and inflammatory conditions like lichen sclerosus also contribute significantly. 3
Several treatment options exist, with varying degrees of success. Minimally invasive techniques such as dilation and direct visual internal urethrotomy (DVIU) are frequently preferred because they are simple and carry low morbidity. However, long-term outcomes remain unsatisfactory, with recurrence rates consistently high in most series.4,5 Current guidelines discourage DVIU/dilatation as sole therapy for long (>2 cm) US. In contrast, for primary, single, short (<2 cm) non-obliterative bulbar strictures it remains an acceptable—though weakly recommended—initial option; even then, 12-month stricture-free rates are only ~60%. 6 Urethroplasty—particularly graft augmentation techniques—provides durable results in more than 85%–90% of patients and is therefore considered the gold standard. 7 Despite this, minimally invasive approaches remain widely used, underscoring the need for better predictors of treatment outcomes.
Previous studies have identified several clinical and anatomical predictors of recurrence after DVIU, including stricture length, prior interventions, and comorbidities.8,9 Importantly, most recurrences occur within the first 12 months after treatment, making this period particularly relevant for prognosis and patient follow-up. Yet, the role of biochemical and hematological markers in anticipating recurrence is still poorly defined. 10
Given these limitations, there is a growing need to identify objective and easily accessible predictors of recurrence after DVIU. In this context, the present study aimed to evaluate the predictive potential of serum creatinine levels and the hemoglobin/creatinine (Hgb/Cre) ratio for 12-month recurrence following DVIU in patients with bulbar urethral strictures <2 cm. Unlike most previous research that has primarily emphasized clinical and anatomical predictors, our analysis focuses on routinely available biochemical markers, which may offer an inexpensive, objective, and easily implementable tool in daily practice. By integrating such parameters into risk stratification, this study seeks to enhance early identification of high-risk patients, optimize postoperative follow-up strategies, and ultimately improve clinical outcomes and resource allocation.
Methods
This retrospective cohort study included patients who underwent DVIU for bulbar US at the Department of Urology, Haydarpasa Numune Training and Research Hospital, University of Health Sciences, Istanbul, Turkey, between January 2012 and August 2024. After application of the exclusion criteria, a total of 237 patients with isolated bulbar US less than 2 cm in length, confirmed by primary retrograde urethrography, were included in the final analysis (Figure 1).
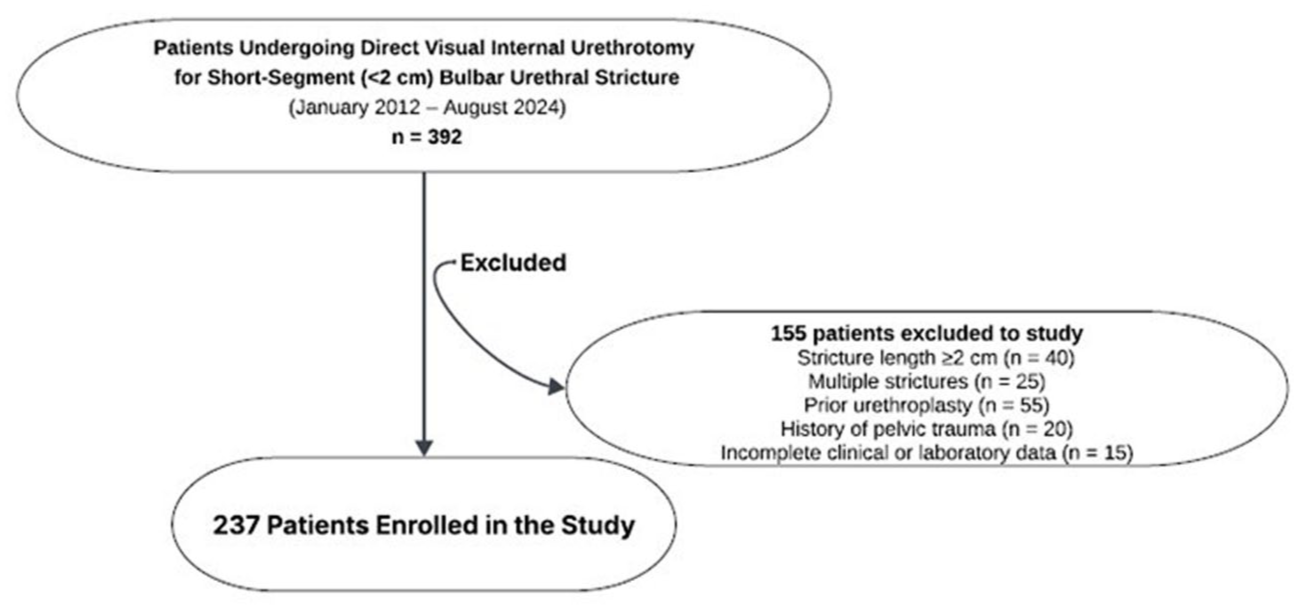
Flowchart of patient selection for recurrence analysis.
Demographic characteristics, comorbidities including hypertension (HT), diabetes mellitus (DM), coronary artery disease (CAD), and chronic kidney disease (CKD), as well as preoperative laboratory parameters such as serum hemoglobin and creatinine levels, preoperative Qmax and post-void residual (PVR) values were recorded, and the Hgb/Cre ratio was calculated. Estimated glomerular filtration rate (eGFR) was computed using the 2021 race-free CKD-EPI creatinine equation as described by Inker et al. 11
Under spinal or general anesthesia, the operation was initiated after identification of the stricture segment under endoscopic vision. A hydrophilic guidewire was then advanced across the narrowed lumen, followed by internal urethrotomy performed with a 21-Fr rigid internal urethrotome. A single cold-knife incision was made at the 12 o’clock position, and at the end of the procedure, a 16/18-Fr foley catheter was inserted and left in place for a median of 3 days. Catheter removal was followed by a standardized postoperative surveillance protocol. Uroflowmetry and symptom assessment were systematically performed at scheduled clinical evaluations at 3, 6, and 12 months. Uroflowmetry constituted the routine assessment at each visit, whereas retrograde urethrography was undertaken in cases demonstrating a decrease in Qmax or the onset of obstructive LUTS. In patients with persistent or equivocal findings, flexible cystoscopy was employed for definitive confirmation. Recurrence was defined as the re-emergence of obstructive urinary symptoms accompanied by reduced urinary flow and verified through radiological or endoscopic evaluation, or the requirement for repeat intervention. Follow-up completeness was evaluated at the scheduled 3-, 6-, and 12-month visits. Patients who missed one visit but returned later were not considered lost to follow-up. Loss to follow-up was defined as having no clinical or uroflowmetric data after the 3-month visit, and such cases were right-censored at their last recurrence-free assessment.
The study protocol was approved by the Haydarpasa Numune Training and Research Hospital Non-Interventional Clinical Research Ethics Committee on September 16, 2025 (Decision No: HNEAH-GOAEK/2025/123), and the study was conducted in accordance with the principles of the Declaration of Helsinki.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics, version 23 (IBM Corp., Armonk, NY, USA). Continuous variables were tested for normality with the Shapiro–Wilk test and presented as median and interquartile range (IQR). Comparisons between recurrence and non-recurrence groups were made using the Mann–Whitney U test for continuous variables and the chi-square test for categorical variables. Receiver operating characteristic (ROC) curve analysis was applied to determine the predictive accuracy of serum creatinine and the Hgb/Cre ratio, and optimal cut-off values were calculated using the Youden index. Recurrence-free survival was additionally evaluated using Kaplan–Meier survival analysis, and differences between groups were compared using the log-rank test. Multivariate logistic regression analysis was conducted to identify independent predictors of recurrence, and results were expressed as odds ratios (ORs) with 95% confidence intervals (CIs). A two-tailed p value of <0.05 was considered statistically significant.
Results
A total of 237 patients were included in the study, of whom 103 (43.5%) developed recurrence within 12 months, whereas 134 (56.5%) remained recurrence-free. The median time to recurrence was 6.0 months (IQR: 3.0–9.0 months), indicating that the majority of events occurred during the first year and predominantly in the early follow-up period.
Patients with and without recurrence did not differ in age (65.0 [57.0–71.5] vs 66.0 [56.3–72.0] years, p = 0.824) or hemoglobin (13.60 [12.10–15.00] vs 13.65 [12.33–14.50] g/dL, p = 0.921). Uroflowmetric measures were likewise comparable, including Qmax (9.0 [6.5–11.5] vs 9.5 [7.0–12.0] mL/s, p = 0.418) and PVR (75 [45–120] vs 70 [40–110] mL, p = 0.560). By contrast, recurrence was more frequent in endoscopic surgery–related strictures (70.8% vs 47.0%), whereas idiopathic (14.6% vs 31.3%) and catheterization-related etiologies (14.6% vs 21.7%) were less common (p = 0.001). Laboratory comparisons showed higher creatinine in the recurrence group (1.10 [0.90–1.55] vs 0.99 [0.80–1.19] mg/dL, p < 0.001) and a lower Hgb/Cre ratio (12.13 [8.18–15.88] vs 14.28 [10.70–17.20], p = 0.002). Additionally, eGFR was significantly lower among patients with recurrence (74.0 [50.0–92.0] vs 88.0 [69.75–99.00] mL/min/1.73 m2, p < 0.001). Comorbidities were generally similar, except for CKD, which was more prevalent among patients with recurrence (24.3% vs 13.4%, p = 0.048; Table 1).
Demographic, clinical, and laboratory profiles of patients with and without recurrence at 12 months.
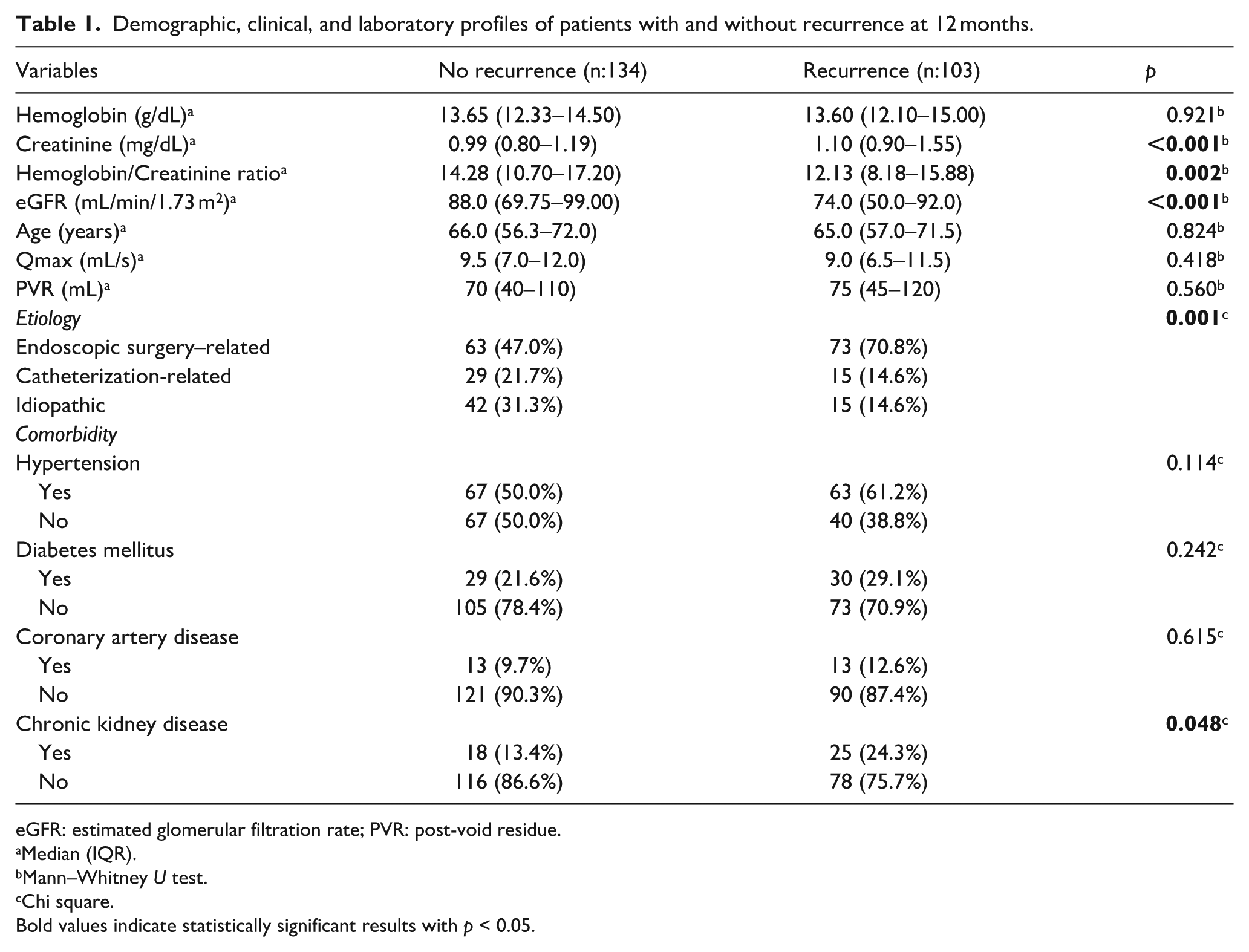
eGFR: estimated glomerular filtration rate; PVR: post-void residue.
Median (IQR).
Mann–Whitney U test.
Chi square.
Bold values indicate statistically significant results with p < 0.05.
ROC analysis was performed to evaluate the predictive ability of serum creatinine, eGFR, and the Hgb/Cre ratio for 12-month recurrence. Serum creatinine demonstrated an AUC of 0.648 (95% CI: 0.577–0.718) with an optimal cut-off value of ⩾1.02 mg/dL, yielding a sensitivity of 55.3% and specificity of 65.6%. eGFR showed a comparable discriminatory performance, with an AUC of 0.643 (95% CI: 0.572–0.714) and an optimal cut-off value of ⩽80.5 mL/min/1.73 m2, corresponding to a sensitivity of 59.2% and specificity of 58.9%. The Hgb/Cre ratio showed a slightly lower discriminatory performance, with an AUC of 0.617 (95% CI: 0.545–0.689) and an optimal cut-off value of ⩽13.26, corresponding to a sensitivity of 58.3% and specificity of 59%. Although all three parameters exhibited modest predictive performance, serum creatinine remained the strongest individual predictor, followed closely by eGFR, while the Hgb/Cre ratio demonstrated the lowest discriminatory ability (Table 2, Figure 2).
ROC analysis of creatinine and hemoglobin/creatinine ratio for predicting 12 months recurrence.

AUC: area under curve, eGFR: estimated glomerular filtration rate.
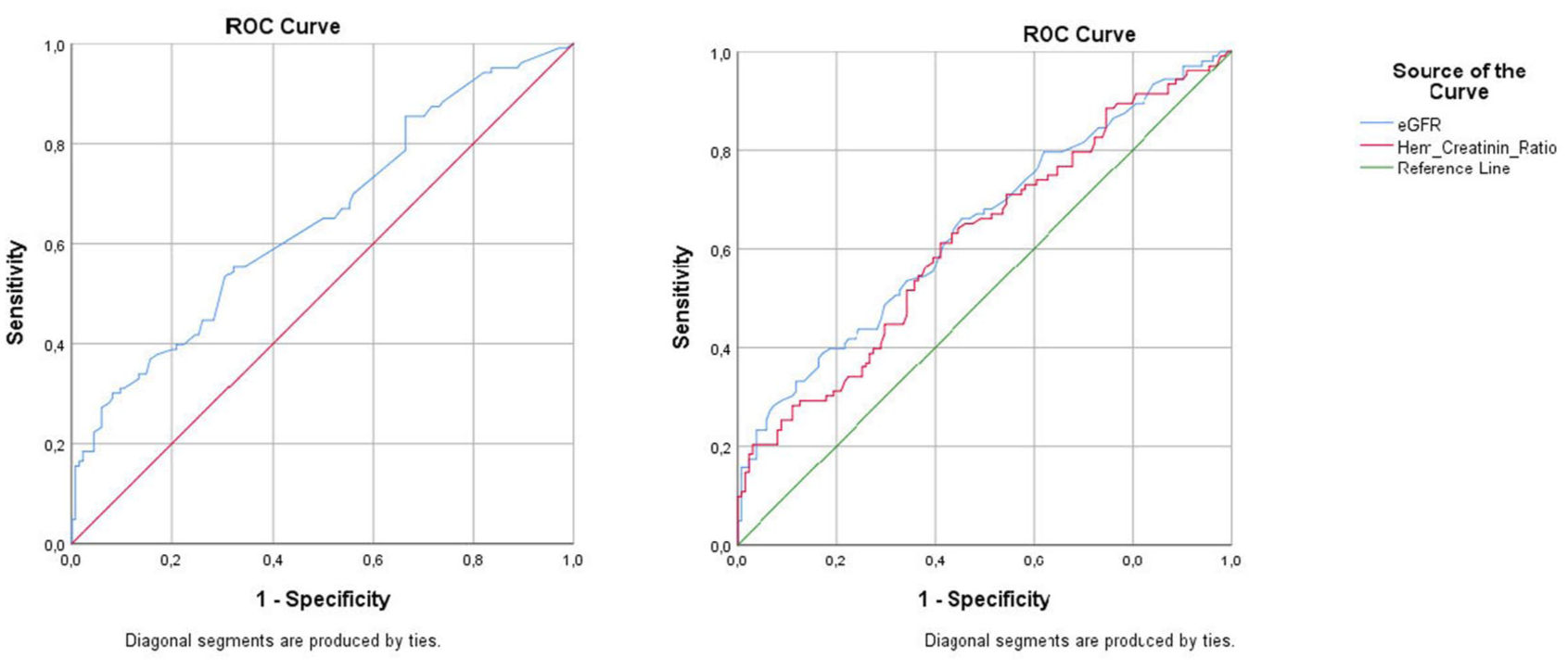
ROC curves of serum creatinine (a), hemoglobin/creatinine ratio and eGFR (b) for predicting 12 months recurrence after DVIU.
Three multivariable logistic regression models were developed to examine renal function–related predictors of 12-month recurrence, adjusting for age and stricture etiology. In Model A, higher serum creatinine was independently associated with recurrence (OR 3.47, 95% CI 1.82–6.60; p < 0.001), and endoscopic surgery–related strictures similarly conferred a markedly increased risk compared with other etiologies (OR 3.49, 95% CI 1.87–6.51; p < 0.001). Age did not demonstrate a significant association (p = 0.507). In Model B, a lower Hgb/Cre ratio also independently predicted recurrence (OR 0.90 per unit, 95% CI 0.85–0.95; p = 0.001), with endoscopic surgery–related etiology again exerting a strong effect (OR 3.42, 95% CI 1.86–6.29; p < 0.001); age remained non-significant (p = 0.197). Model C evaluated eGFR as a continuous renal function parameter and demonstrated that lower eGFR independently increased recurrence risk (OR 0.975 per mL/min/1.73 m2, 95% CI 0.964–0.987; p < 0.001). Endoscopic surgery–related strictures maintained a consistent and robust association across models (OR 3.38, 95% CI 1.82–6.25; p < 0.001), whereas age again did not reach statistical significance (p = 0.077). All models exhibited acceptable calibration (Hosmer–Lemeshow p > 0.05) and comparable overall classification accuracy (approximately 66%). Discriminative performance was modest but stable across renal markers. The creatinine-based model demonstrated the highest AUC (0.719, 95% CI 0.654–0.785), followed closely by the eGFR-based model (0.713, 95% CI 0.648–0.779) and the Hgb/Cre-based model (0.698, 95% CI 0.630–0.766; Table 3, Figure 3).
ROC curves of multivariable logistic regression models (Model A: creatinine-based; Model B: Hgb/Cre-based) for predicting 12-month recurrence after DVIU.
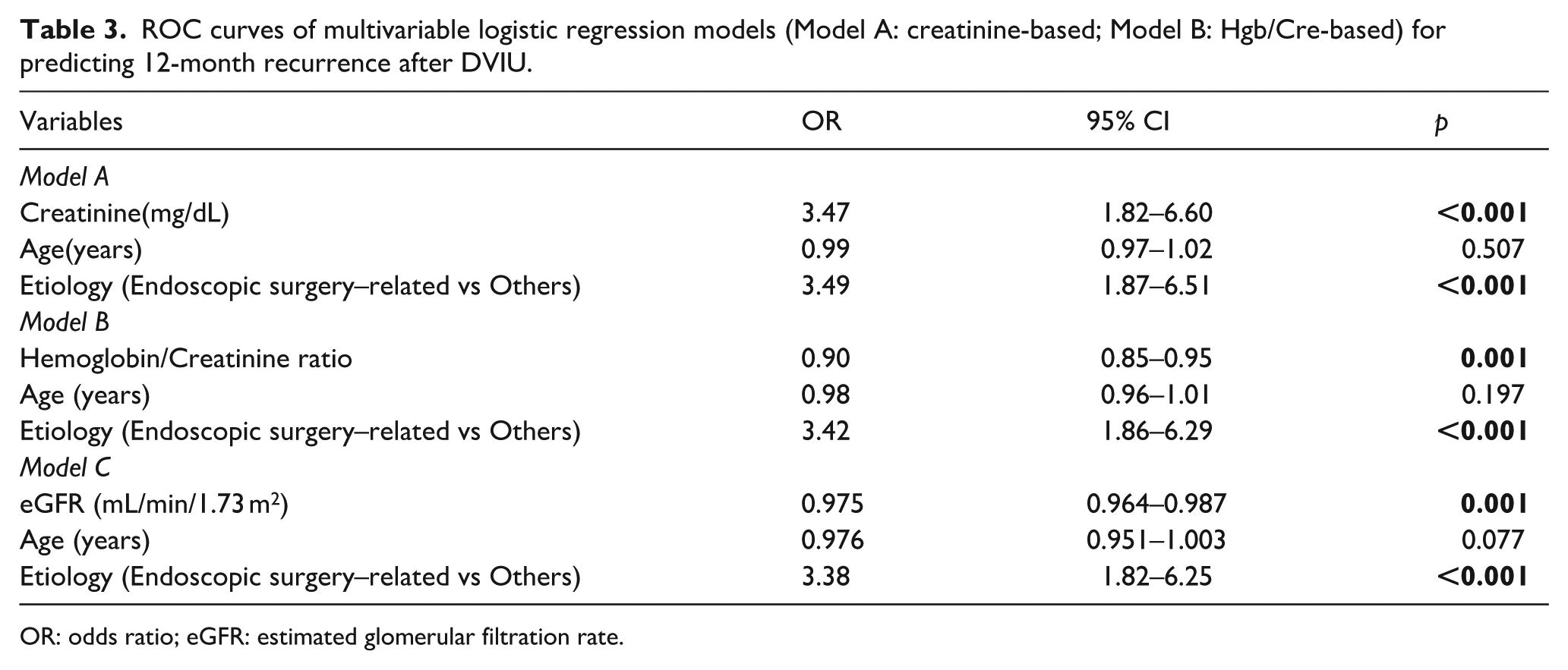
OR: odds ratio; eGFR: estimated glomerular filtration rate.
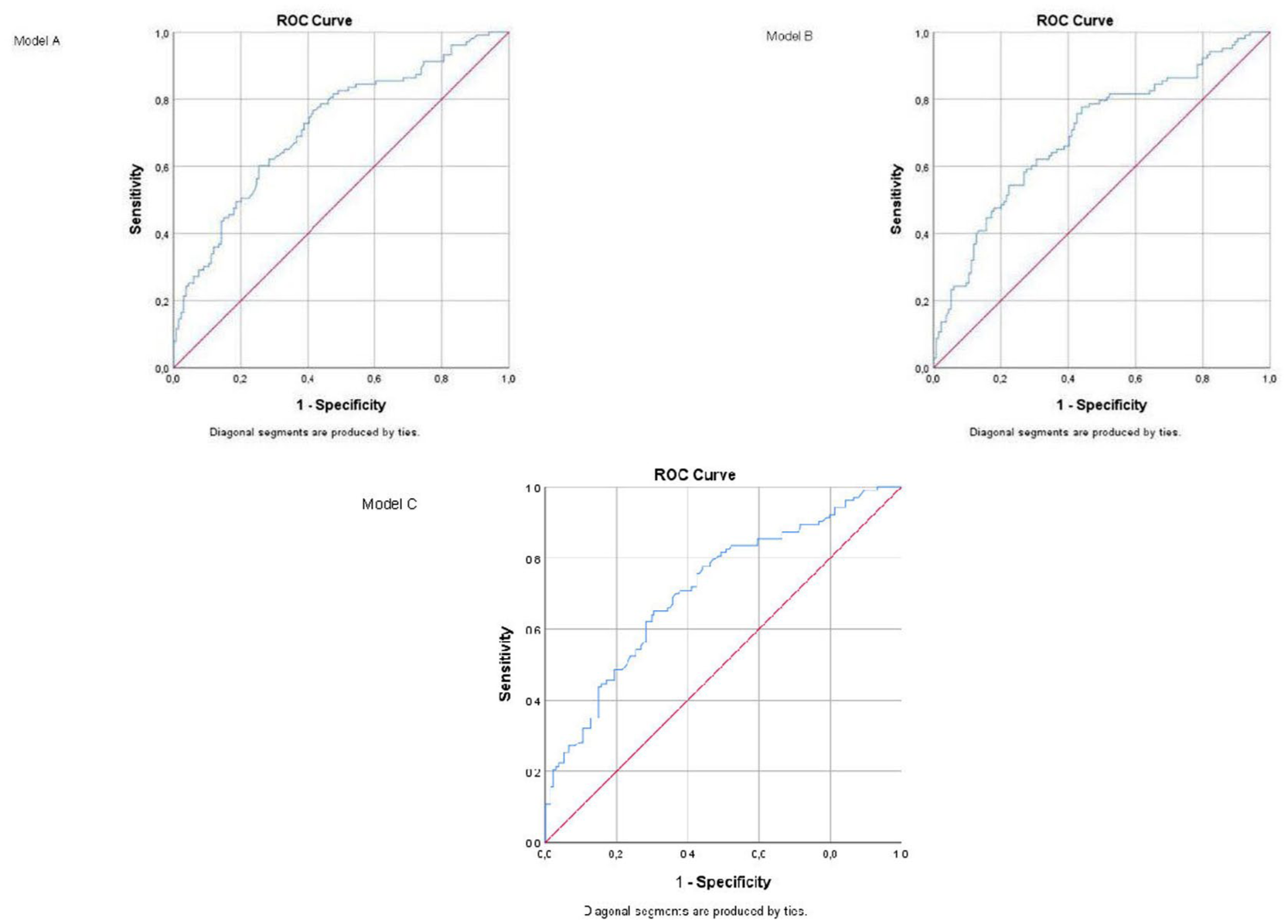
ROC curve of the multivariable logistic regression models for predicting 12-months recurrence after DVIU.
Kaplan–Meier analyses demonstrated significant differences in 12-month recurrence across biomarker-defined subgroups. Stratification by eGFR showed a clear separation of curves, with patients in the low eGFR group (⩽80.5 mL/min/1.73 m2) experiencing markedly higher recurrence rates throughout follow-up (log-rank χ2 = 6.647, p = 0.010; Breslow p = 0.022; Tarone–Ware p = 0.014). A similar but more pronounced pattern was observed for serum creatinine, where patients with elevated levels (⩾1.02 mg/dL) exhibited substantially higher 12-month recurrence (log-rank χ2 = 9.319, p = 0.002; Breslow p = 0.006; Tarone–Ware p = 0.004). Differences based on the Hgb/Cre ratio (⩽13.26 vs >13.26) were comparatively modest yet remained statistically significant (log-rank χ2 = 4.887, p = 0.027; Tarone–Ware p = 0.048). Overall, biomarkers reflecting impaired renal function demonstrated the greatest separation in recurrence probability, with creatinine and eGFR showing the strongest discriminatory capacity among the evaluated indicators (Figure 4).
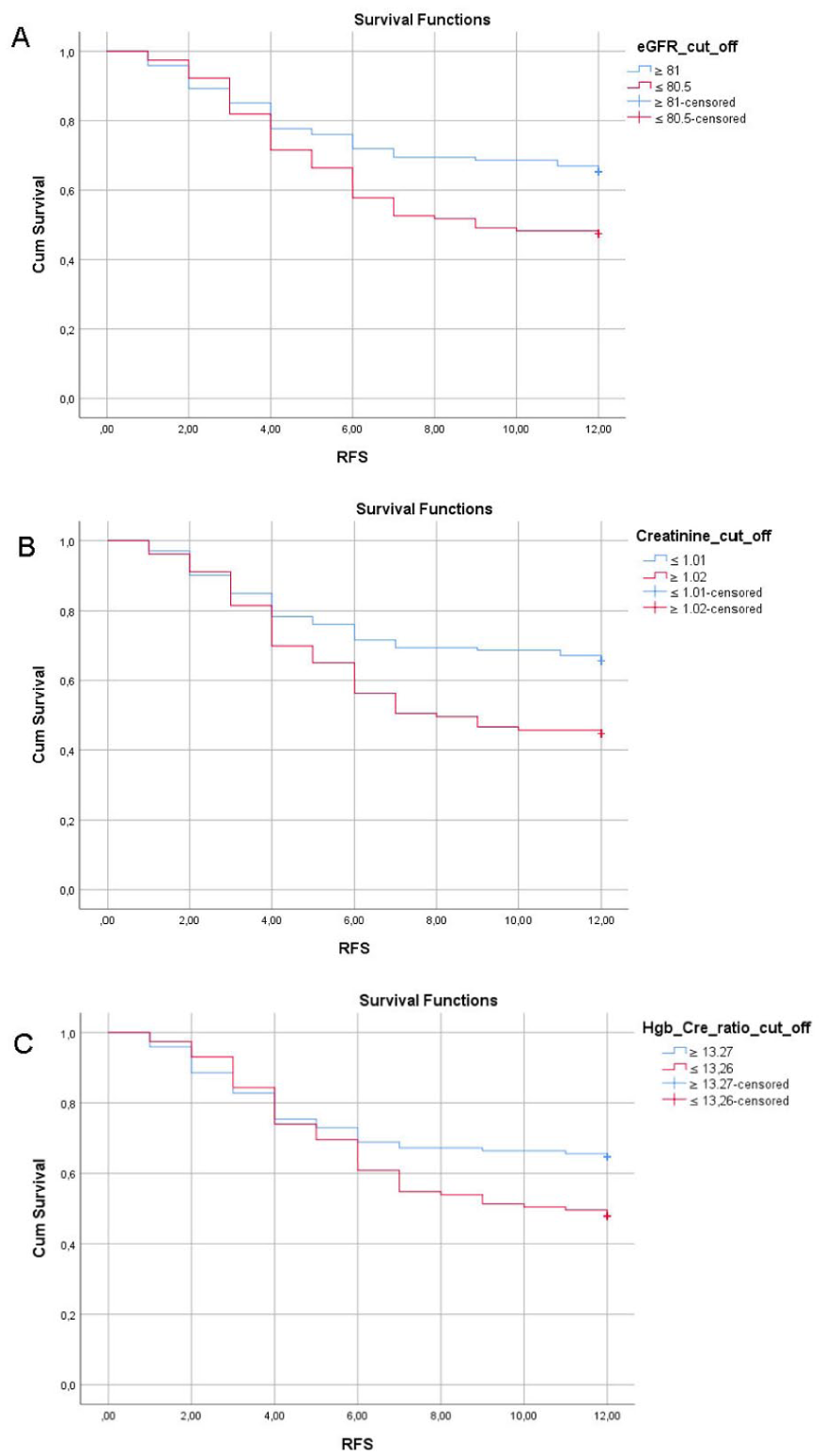
Kaplan–Meier analysis demonstrating 12-month recurrence according to eGFR (a), creatinine (b), and Hgb/Cre ratio cut-offs (c).
Discussion
US disease remains a challenging condition with high recurrence rates after minimally invasive procedures such as DVIU, highlighting the need for reliable and easily applicable predictors of treatment outcomes.
Impaired renal function has been consistently associated with delayed wound healing through multiple pathophysiological pathways. Patients with CKD exhibit disruptions in epithelialization and granulation tissue formation, accompanied by persistent inflammation, reduced angiogenesis, and impaired cellular proliferation, as demonstrated in both animal models and clinical observation. 12 Additionally, uremic toxins accumulating due to renal dysfunction contribute to endothelial dysfunction, systemic oxidative stress, and chronic low-grade inflammation—key factors that undermine effective tissue repair. 13 These mechanistic insights justify the observed association between elevated serum creatinine levels and, analogously, a lower Hgb/Cre ratio with higher rates of stricture recurrence following DVIU.
Recurrence after DVIU is strongly influenced by systemic comorbidities. Gul et al. reported that DM and HT were significantly associated with recurrence, 14 while Aydemir et al. demonstrated that repeated DVIU procedures and CAD increased the risk of treatment failure. 9 In our study, however, DM, HT, and CAD were not associated with recurrence, whereas the presence of CKD was found to be a significant factor, suggesting that renal dysfunction may have a decisive role in impaired healing and stricture recurrence.
In our cohort, neither preoperative Qmax nor PVR demonstrated a significant association with stricture recurrence. By contrast, Barbagli et al. reported that preoperative maximum flow (pQmax) was the only independent predictor of treatment failure after DVIU for untreated bulbar strictures, with pQmax > 8 mL/s associated with higher success rates and pQmax < 5 mL/s with higher recurrence risk. 15 These findings indicate that the prognostic value of uroflowmetry may vary depending on patient selection and clinical context.
In our study, neither age nor hemoglobin levels demonstrated a statistically significant association with recurrence after DVIU. By contrast, Harraz et al. identified advanced age as an independent predictor of treatment failure (OR 1.017; p = 0.03), whereas lower hemoglobin values showed borderline significance in univariate analysis (p = 0.05) but did not retain significance in multivariate analysis. 16 These observations suggest that the prognostic value of age and hemoglobin may vary across study populations and analytical approaches, and their role as reliable predictors of recurrence remains inconclusive.
In our cohort, etiology emerged as a significant determinant of recurrence, with strictures secondary to prior endoscopic surgery exhibiting higher failure rates compared to idiopathic and catheter-related cases. This finding is consistent with Yuruk et al., who analyzed treatment-naïve patients undergoing DVIU and reported that strictures caused by transurethral interventions (iatrogenic) were associated with significantly higher recurrence rates than idiopathic strictures. 17 Similarly, Barbagli et al. demonstrated that non-idiopathic etiology predicted recurrence in univariate analysis but lost significance after adjusting functional parameters such as preoperative Qmax. 15 More recently, Hernández-Hernández et al. also reported that bulbar strictures related to previous transurethral procedures carried significantly higher failure rates after DVIU, further underscoring the adverse prognostic impact of iatrogenic etiology. 18 Taken together, these results suggest that while iatrogenic etiologies, particularly those related to prior transurethral manipulation, represent an important risk factor for recurrence, their impact may be modulated by accompanying clinical characteristics.
In our study, reduced eGFR and elevated creatinine were associated with higher recurrence rates after DVIU. This observation is consistent with evidence showing that impaired renal function negatively influences urethral wound healing. Pathak et al. reported that patients with renal dysfunction undergoing urethral surgery experienced delayed epithelial recovery and higher rates of wound-related complications, likely due to reduced vascularization and persistent inflammation. 19 These alterations in healing may predispose individuals to earlier stricture recurrence, supporting the relevance of renal reserve in postoperative outcomes.
In our study, a lower Hgb/Cre ratio was significantly associated with recurrence following DVIU. This finding aligns with emerging evidence from other medical disciplines, where the hemoglobin-to-creatinine ratio has been proposed as a combined marker of hematologic and renal reserve, reflecting systemic vulnerability. For instance, Demir et al. demonstrated that a reduced Hgb/Cre ratio was independently associated with long-term mortality in patients with acute coronary syndrome, 20 while Çamcı et al. reported that lower ratios predicted the development of contrast-induced nephropathy after percutaneous coronary interventions. 21 These studies support the notion that impaired renal function, when coupled with reduced hematologic reserve, predisposes individuals to adverse outcomes such as delayed tissue repair, increased inflammation, and poor clinical recovery.
While the Hgb/Cre ratio has gained attention in systemic conditions such as cardiovascular and renal diseases, its prognostic utility in urological practice remains notably underexplored. To our knowledge, this study represents one of the first attempts to assess the predictive relevance of Hgb/Cre in the context of US disease, highlighting its potential as a surrogate marker of systemic vulnerability that may influence local tissue healing and surgical outcomes. Future investigations may further enhance predictive modeling by incorporating broader multimarker approaches, including the Pan-Immune-Inflammation Value, the Systemic Immune-Inflammation Index, and the Systemic Inflammation Response Index, which have demonstrated prognostic relevance in various urological conditions. 22 Given that systemic vulnerability and impaired healing responses may influence the durability of endoscopic treatments, identifying patients with an elevated risk of recurrence becomes clinically relevant for optimizing treatment planning. For individuals exhibiting adverse biochemical profiles—such as elevated creatinine, reduced eGFR, or a lower Hgb/Cre ratio—early consideration of definitive urethroplasty may be appropriate, even before repeated endoscopic failures occur. For patients who are not suitable candidates for urethroplasty, minimally invasive alternatives such as drug-coated balloon dilatation (Optilume) may represent a reasonable option.
This study has several important limitations. The retrospective and single-center design may introduce unmeasured confounding and limits the generalizability of the findings. Additionally, the 12-month follow-up horizon, although consistent with previous DVIU studies, is relatively short and may underestimate late recurrences that often manifest beyond the first postoperative year. The absence of patient-reported outcome measures (PROMs) represents another limitation, as symptom burden may not always correspond to anatomical recurrence and PROM data would have allowed a more comprehensive, patient-centered assessment of treatment outcomes. The modest discriminative performance of the evaluated biomarkers (AUC ~0.70) further underscores the need for cautious interpretation and highlights the importance of developing more robust, integrative prediction models. Moreover, the clinical usefulness of the proposed cut-off values remains uncertain, as the study did not include decision-curve analysis or other net-benefit assessments that would clarify their impact on treatment decision-making. Despite these limitations, the present findings provide an important foundation for future prospective, multicenter studies aimed at validating the potential role of renal function parameters—particularly creatinine, eGFR, and the Hgb/Cre ratio—in risk stratification following DVIU.
Conclusion
Elevated serum creatinine, a reduced eGFR and lower Hgb/Cre ratio were independently associated with 12-month recurrence following DVIU for short-segment bulbar US, whereas demographic and uroflowmetric parameters demonstrated limited predictive utility. As simple and routinely accessible biomarkers, eGFR, creatinine and the Hgb/Cre ratio may assist in identifying patients at increased risk of failure after endoscopic treatment. In such individuals, early consideration of definitive urethroplasty—or, where urethroplasty is not feasible, minimally invasive alternatives such as drug-coated balloon dilatation (Optilume)—may help optimize long-term outcomes. These findings should be interpreted as hypothesis-generating and warrant validation in prospective, multicenter studies.
Footnotes
Author contributions
R.K.: Conceptualization (lead); writing – original draft (lead), Software (lead). K.K.: Writing—review and editing (equal). H.Ç.: formal analysis (lead). E.T.: Writing—review and editing (equal). M.İ.Ö.: Supervisor.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.