
Abstract
Introduction:
Circumcision is a simple procedure, but it is not free from complications. New methods have recently been developed, including the circular stapler CircumCYS®.
Material and methods:
This a retrospective analysis of our institutional series of 80 consecutive procedures. The stapler consists of a inner bell (in six different sizes), that it is designed to protect the gland, a pistol with a trigger, a circular scalpel and a stapler for the suture. The circumference of the penile shaft is measured at the level of the balano-preputial fold with the provided device. No antibiotic prophylaxis was necessary. A Dorsal Penile Nerve Block (DPNB) were performed by the urologist. Data were collected from medical records 14 days and 1 month after the surgery. Complication rate and Visual Analog Scale were investigated.
Results:
Eighty patients were treated between August 2023 and January 2024. The average operating time was 10 min (ds 6). Postoperatively we observed three scar edemas and two minor bleedings. The most common complication was the incarceration of the metal stitches within the scar (five cases). The average time for the stitches to fall out was 24.9 days (ds 3.9). Pain was consistently well-controlled (Visual Analog Scale 2/10 one hour post-surgery - ds 0.8).
Conclusion:
CircumCYS® is a reliable, safe and easy-to-use tool. The technique is very fast and this allows the execution of many circumcisions in a single session. The learning curve appears minimal.
Introduction
Phimosis is a pathological condition that involves the partial or total impossibility of uncovering the glans.
Circumcision is one of the most common urological procedure. Circumcision is often undertaken for religious and cultural practice but also for medical reasons. Most of these are due to inflammatory origin which, as they become chronic, lead to the evolution into stenosis and therefore into preputial scar.1,2
Specific benefits from male circumcision were identified for the prevention of urinary tract infections (UTIs), transmission of sexually transmitted infections (including human papillomavirus 3 ), human immunodeficiency virus (HIV) 4 penile cancer and reduction in the incidence of balanitis. 5 The three standard techniques for circumcision, recommended by the World Health Organization (WHO), are the dorsal slit, the forceps-guided method, and sleeve resection. 6 Although it is a simple procedure, circumcision is not free from complications, such as infections, wound dehiscence, bleeding, edema, excessive foreskin and unsatisfactory cosmetic results.7,8 Lastly, conventional circumcision is time-consuming, creating a problem of prolonged waiting lists, especially in high-volume centers for major surgery. The most widely used techniques in the world are still the manual ones, although new methods have recently been developed, including the circular stapler CircumCYS® that might allow to optimize surgery and healing times, as well as reduce post-operative complications and lower blood loss volume. 4 In this study, we aim to describe the technique and the results of our institutional series of CircumCYS® procedures.
Material and methods
This a retrospective analysis of our institutional series of 80 consecutive procedures performed with this device. The only circumcision excluded were those that needed to be performed for biopsy purposes. We used the chi-square test and Student’s t-test to try to identify some risk factors for the described complications. Statistical significance was defined as a p value of < 0.05. The study was conducted in accordance with the Declaration of Helsinki, and informed consent was obtained from all patients included in the study. The stapler consists of a inner bell, that it is designed to protect the gland, a pistol with a trigger, a circular scalpel, a stapler for the suture and a plastic gasket, which remains between the wound and the stitches. The glands bell comes in six different sizes (13, 17, 22, 25, 28, 34 mm).
Before entering the operating room, the circumference of the penile shaft is measured at the level of the balano-preputial fold with the appropriate device provided by the manufacturing company (Figure 1). None of our patients received any kind of antibiotic prophylaxis. A standard scrub of the genitalia with Betadine® was performed.
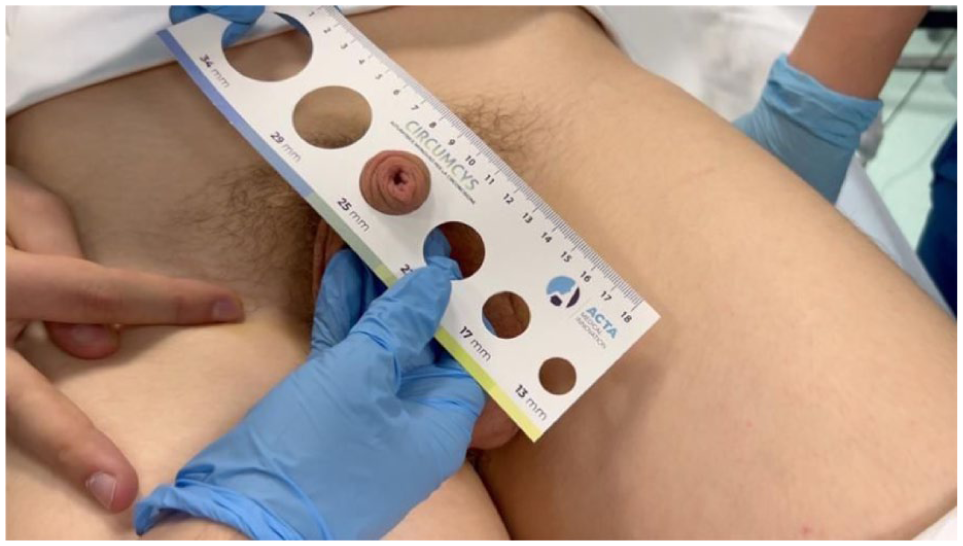
Measurement of the penile shaft at the level of the balano-preputial fold using the device provided by the manufacturing company.
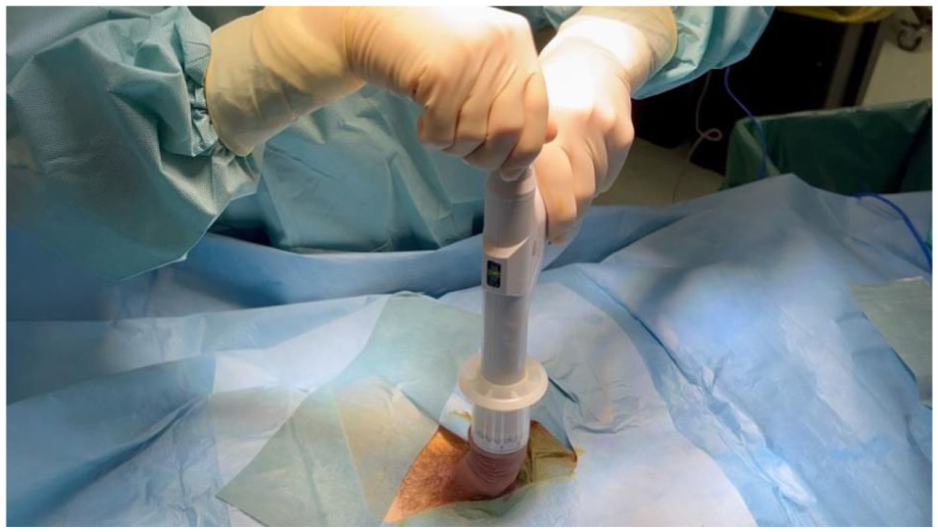
All surgeries were performed in the supine position and a Dorsal Penile Nerve Block (DPNB) were performed by the urologist. After positioning the inner bell over the glans (Figures 2 and 3; possibly after making a relieving incision in cases of severe phimosis), the pistol is positioned (Figure 4). Then, by operating the latch mechanism, which is rotated until the indicator is in the correct position (Figure 5), the pistol is engaged. At this point, the trigger can be pressed (Figure 6). After 60 s with the trigger engaged, the procedure is completed and the device is disengaged from the bell by rotating the latch mechanism (Figures 7 and 8). Frenulotomy was not routinely performed. A limited frenulotomy was carried out only when a short frenulum interfered with correct positioning of the bell. In all other cases, the frenulum was assessed at the end of the procedure and hemostasis was performed if necessary. The bell is then removed together with the prepuce, exposing the metallic staples, after which the dressing can be applied (Figures 9 and 10). At the end of the procedure, a compressive sterile dressing was applied using self-adherent gauze (Peha-haft®) in combination with topical gentamicin cream. The initial dressing was maintained until postoperative day 1, unless complications required earlier removal. Thereafter, patients were instructed to perform daily wound care for 7 days, consisting of local disinfection and application of topical gentamicin cream for the first 3 days (extended to 7 days in diabetic patients), followed by disinfection and light dressing only. Data were retrospectively collected from medical records 14 days and 1 month after the surgery. Patients consented to data collection. Complication rate and Visual Analog Scale (VAS) were investigated.
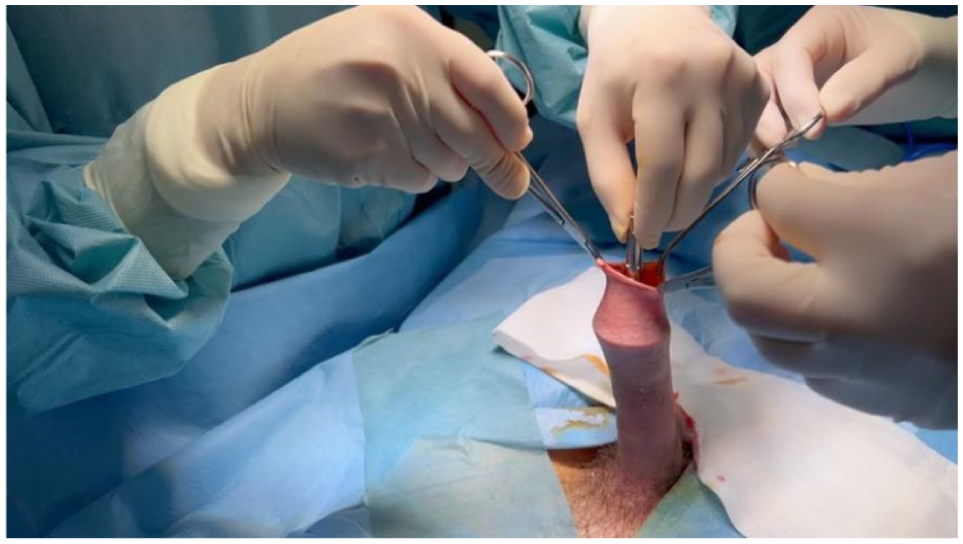
Positioning the inner bell over the glans.
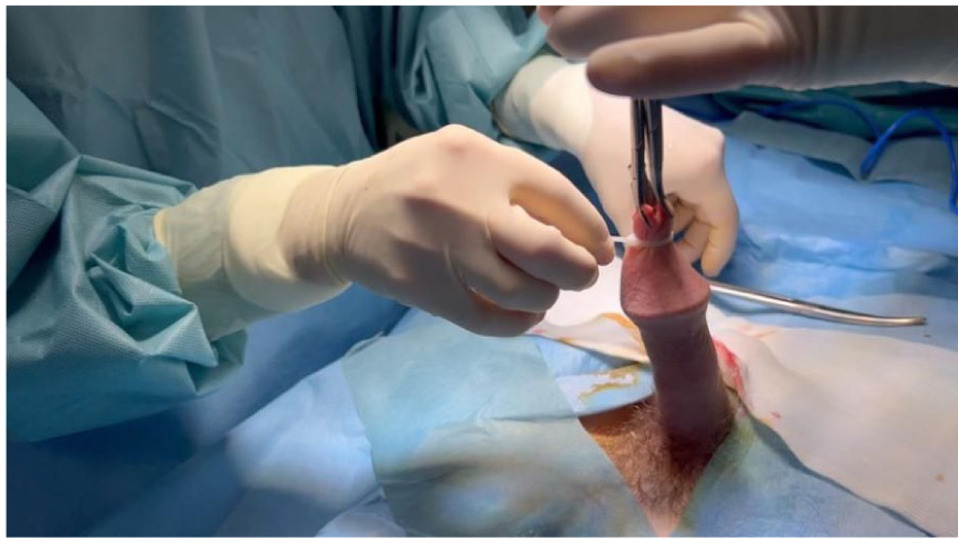
Positioning the inner bell over the glans and securing it with a plastic strap.

Positioning of the pistol.
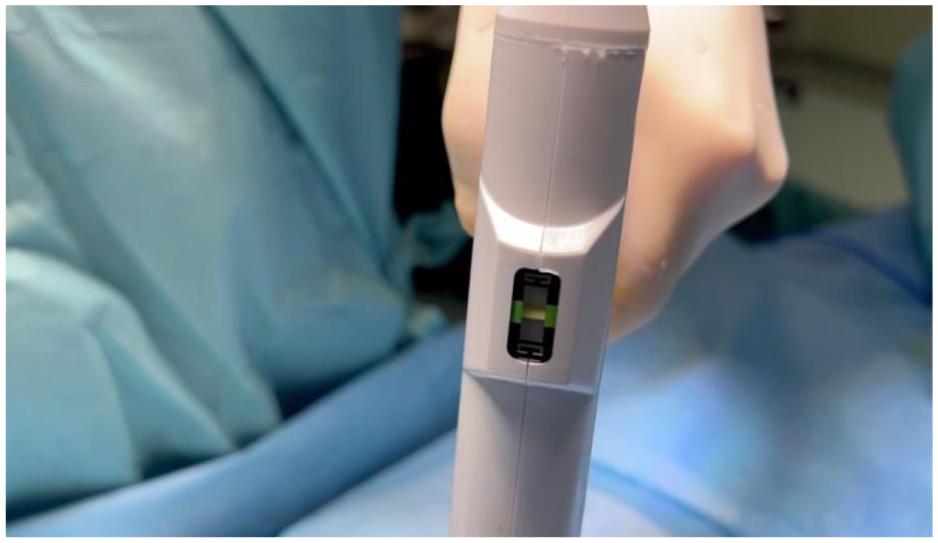
Rotating the latch mechanism until the indicator reaches the correct position.

The trigger can be pressed.
After 60 s with the trigger pressed, the procedure is concluded, and the pistol is released from the bell.

Rotating the latch mechanism in the opposite direction to release the pistol from the bell.

The bell is removed, along with the prepuce.
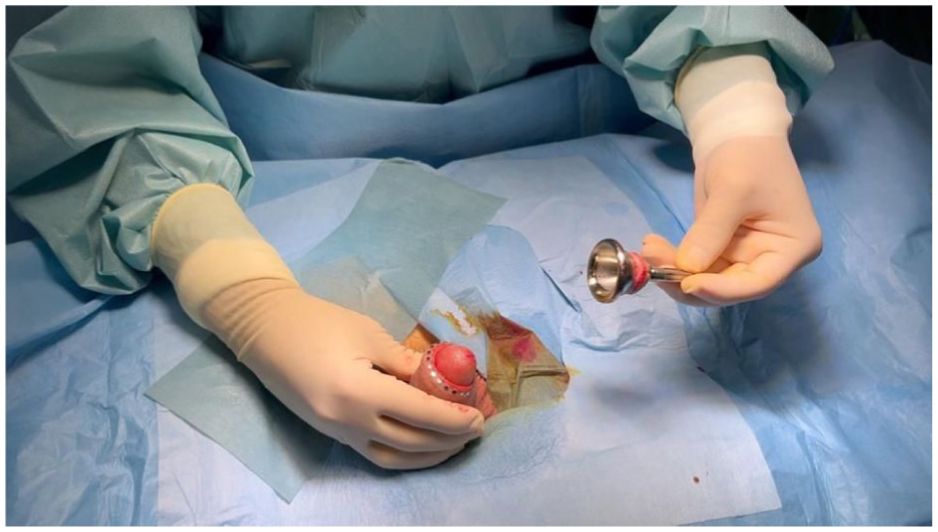
At the end, the wound with the metal staples in place is visible, and the medication can be applied.
Results
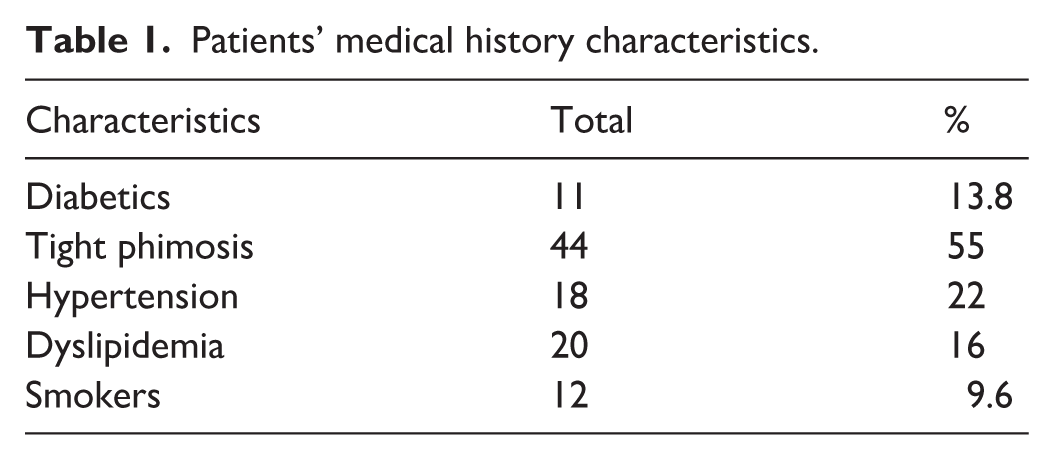
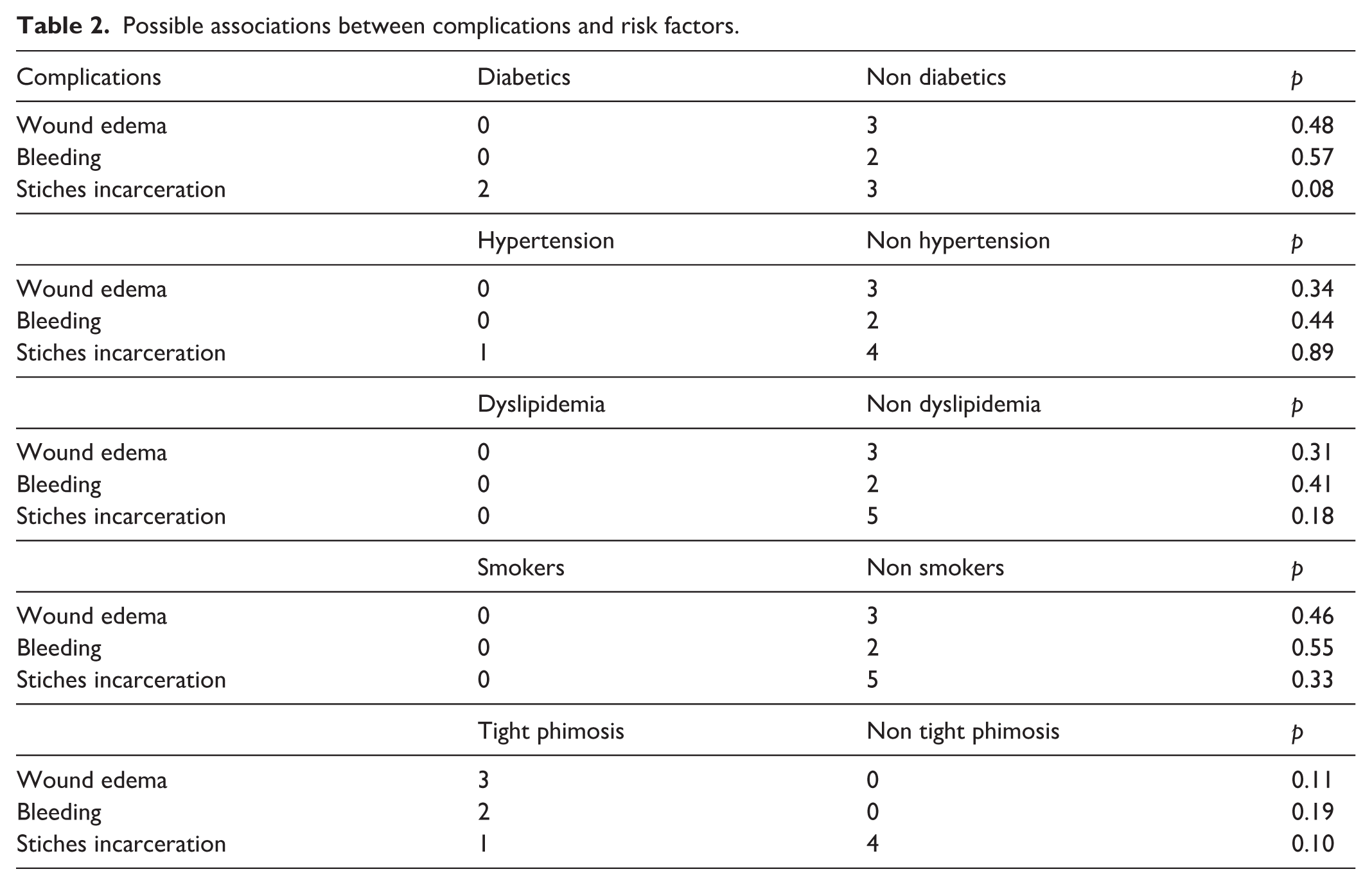
Eighty patients were treated between August 2023 and January 2024. The mean age was 46 years (ds 23). Forty-four out of 80 patients had a tight phimosis (Table 1 population characteristics). In these cases, the device can be used after performing a longitudinal cut on the foreskin with scissors. The average operating time was 10 min (ds 6). Postoperatively we observed three scar edemas and two minor bleedings. The most common complication we observed was the incarceration of the metal stitches within the scar (five cases) and the subsequent removal of stitches by the urologist during follow-up visits. None of the characteristics of our population seem to be predictive of these complications (Table 2). We did not observed any major complications. The average time for the stitches to fall out was 24.9 days (ds 3.9). Concerning pain assessment, we administered the VAS (Visual Analog Scale) to out patients. Pain was consistently well-controlled, with an average score of 2/10 1 hour post-surgery (ds 0.8) and 1/10 at 7 days post-surgery (ds 0.2).
Patients’ medical history characteristics.
Possible associations between complications and risk factors.
Discussion
Approximately 1.4 million male circumcisions are performed annually in US medical settings 9 and it remains one of the most commonly performed surgeries by Urologists. Standard manual surgical approaches are currently still the most common and recommended by the WHO. Nonetheless, conventional circumcision has several drawbacks 10 : it necessitates training and can have a high complication rate,11,12 particularly in some countries where it is often carried out by poorly trained and equipped health workers.13 –15 Lastly, we must remember that standard MC always requires time. Our series of circumcisions performed with a circular stapler (CircumCYS®) demonstrates that this approach has several advantages, primarily its ease of use, with a learning curve essentially reduced to a few tips and tricks, low complication rates, and consistently minimal pain. 16 Lastly, the reduced operative time17,18 with this approach makes it suitable for high-volume centers. While the primary perceived limitation of using the stapler might initially seem to be the cost, the number of surgeries that can be performed in a single session—approximately 100% more compared to a manual approach—could make the purchase of these devices cost-effective.19,20 As previously mentioned, the most common complication we observed was the incarceration of stitches within the wound. Perhaps the solution to reducing this issue could be to remove the metal stitches manually at 2 weeks post-procedure in cases where the plastic gasket, which remains between the wound and the stitches, is no longer intact.
Conclusion
CircumCYS® is a reliable, safe and easy-to-use tool. The technique is very fast and this allows the execution of many circumcisions in a single session; we believe that this aspect might be very important in high-volume centers. The learning curve appears minimal, but in our experience care must be taken when choosing the size of the bell, during initial measurement phase: choosing the narrowest, when in doubt, could lead to a partial circumcision. We are planning to conduct a prospective trial in the future that will randomize patients to undergo either circular stapler procedures or standard techniques, with the aim of further evaluating their efficacy, safety, and clinical outcomes.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.