
Abstract
Objective:
To evaluate the impact of ejaculation-preserving (EP) prostate resection techniques on postoperative ejaculatory and urinary outcomes in men with benign prostatic obstruction (BPO), and to determine whether additional bladder-neck preservation provides further functional benefit compared with peri-verumontanum-only preservation.
Methods:
This meta-analysis was conducted in accordance with PRISMA 2020 guidelines. A systematic search of PubMed, Cochrane Library, and ScienceDirect up to June 2025 identified randomized controlled trials comparing EP and standard prostate resection. Studies were stratified by anatomical extent of preservation: peri-verumontanum only versus peri-verumontanum with bladder-neck preservation. Data were analyzed using a random-effects model in Review Manager v5.4, and study quality was assessed using the Cochrane Risk-of-Bias 2.0 tool.
Results:
Eight randomized controlled trials including 580 patients were analyzed. EP prostate resection improved antegrade ejaculation preservation compared with standard resection while maintaining comparable urinary and erectile outcomes. Subgroup analysis revealed no additional functional advantage from extending preservation beyond the peri-verumontanum.
Conclusion:
EP techniques are associated with improved preservation of antegrade ejaculation while maintaining comparable short term urinary outcomes. Peri-verumontanum preservation appears to provide comparable functional outcomes to approaches extending preservation up to bladder neck. However, these findings remain exploratory and require validation in future larger, methodologically robust studies.
Keywords
Introduction
Prostate resection remains as a mainstay treatment for lower urinary tract symptoms (LUTS) due to benign prostatic obstruction (BPO), particularly including cases of patients with refractory response to medical therapy. 1 While its efficacy in improving urinary symptoms has well been established, 2 its attention has increasingly shifted toward increasing postoperative quality of life, especially sexual function without compromising its efficacy. 3 Ejaculatory dysfunction, despite not being life-threatening, is among one of the most distressing complications following prostate surgery, compromising patients sexual satisfaction, psychological well-being, and overall patient reported outcomes. 4 As surgical success is increasingly judged by both symptom relief and sexual function preservation, concerns surrounding post operative ejaculation function have become more and more clinically relevant.
Retrograde ejaculation following prostate resection is primarily attributed from injury to anatomical structures critical for the physiological mechanism responsible of semen flow. Resection that involves the bladder neck, ejaculatory ducts or peri-verumontanum tissues may impair normal propulsion and compromise the structures necessary to maintain forward flow of semen during ejaculation. 5 Despite being as a harmless complication, retrograde ejaculation has been shown to negatively affect patient satisfaction and ultimately contributes to dissatisfaction with surgical outcomes. 6 While key anatomical structures involved in ejaculation are well established, it remains uncertain how differences in surgical preservation affect functional outcomes. This has led to growing efforts to refine optimal surgical techniques that minimize ejaculatory dysfunction without compromising treatment goals.
As concerns over postoperative sexual outcomes have grown, surgical approaches have been adapted in attempt to preserve ejaculatory function by minimizing injury to key anatomical structures. 7 These include preserving the peri-verumontanum structures, sparing the bladder neck, and avoiding injury to the ejaculatory ducts. While results suggest these modifications may improve rates of antegrade ejaculation, the extent of anatomical preservation varies considerably across techniques and standardized approaches of preservation remains undefined. Some approaches target only the peri-verumontanum region, while others preserve beyond this region up to bladder neck.8–15 This variation raises the question regarding the balance of how much preservation is truly necessary to balance ejaculatory function with resection efficacy.
This review aims to compare ejaculation-preserving prostate resection techniques against standard prostate resection approaches in terms of ejaculatory and urinary outcomes, with an additional subgroup analysis made based on the extent of anatomical preservation: peri-verumontanum only versus peri-verumontanum with bladder neck preservation to provide an overview of outcome patterns across techniques and to explore whether broader preservation trends align with differences in functional results.
Methods
Eligibility criteria
This review included randomized controlled trials involving sexually active adult male patients diagnosed with benign prostatic obstruction (BPO) presenting with lower urinary tract symptoms (LUTS) and also including patients failing medical therapy scheduled for prostate resection surgery. Eligible studies must compare ejaculation-preserving (EP) prostate resection techniques against standard resection methods, with reported outcomes including antegrade ejaculation preservation, urinary symptom scores (IPSS), peak urinary flow rate (Qmax), post-void residual urine (PVRU), erectile function (IIEF), or operative time. Only randomized controlled trials (RCTs), available in full text and written in English are included.
Studies were excluded if they involve participants included those with a diagnosis of prostate cancer, neurogenic bladder, detrusor underactivity, urethral strictures, bladder neck contracture, significant bladder stones, or previous prostatic or urethral surgery. Studies with non-sexually active individuals, patients with pre-existing ejaculatory dysfunction, or those receiving sexual function-altering medications were also excluded. Additional exclusions were applied to studies with incomplete data reporting, such as lack of baseline or follow-up data.
Information sources
Information was obtained from studies retrieved from PubMed, Cochrane Library, and ScienceDirect. Each database was last searched up to June 2025. Additional manual searching was performed using keywords being searched in search engines and manually screening through reference lists of relevant articles to identify any additional missed eligible studies that has not been identified.
Search strategy
A systematic search of scientific databases was screened, using the main keywords included based on the words “Ejaculatory Function,” “Prostate Resection” and “Ejaculation Preservation.” These were entered into the advanced search fields using the Boolean operator “AND” to combine major concepts, “OR” to include relevant synonyms. A comprehensive literature search was conducted in PubMed, Cochrane CENTRAL, and ScienceDirect up to June 2025. The search was restricted to English language publications. No study design filters were applied at the database search level. Only randomized controlled trials were selected during the screening process according to predefined inclusion criteria. The complete search strategies are provided in the Supplemental Material 1. The protocol for this review was registered in PROSPERO with the registration number CRD420251101523.
Selection process
Electronic search and reporting processes were based on PRISMA guidelines. 16 After all database searches were completed, study duplicates were removed using the Rayyan AI tool. Titles and abstracts of the remaining after deduplication were screened by both reviewers independently. Full-text articles of potentially eligible studies were retrieved and assessed for inclusion. All selection decisions were also reviewed and confirmed by both reviewers. Any uncertainties regarding eligibility during the research were resolved through consensus discussion between reviewers.
Data collection process and data items
Once all included studies were identified and retrieved, data extraction from the studies was performed by a single reviewer (SG). Extracted data were cross-checked and verified by the senior reviewer (SMW), and any discrepancies were resolved through discussion to reach consensus. The following variables were extracted: first author’s name, year of publication, associated country, sample sizes, patient baseline characteristics, surgical technique used and measure of outcomes. No additional data were sought from study investigators.
Quality assessment of the studies
Risk of bias of all the included studies were assessed using Cochrane Risk-of-bias tool for randomized trials (RoB 2), which has been structured into a 5 set of domains evaluating the bias arising from randomization process, deviations from intended intervention, missing outcome data, measurement of the outcome and selection of reported result. 17
Synthesis methods and effect measures
Studies included in this review were subgrouped based on the extent of anatomical preservation. The primary outcome in this review was the number of patients with preserved antegrade ejaculation post-surgery. Ejaculatory outcomes from the studies were harmonized by defining the primary endpoint as preservation of antegrade ejaculation. In studies reporting retrograde ejaculation rates as the outcome, preserved antegrade ejaculation was calculated as the complement of retrograde ejaculation (i.e. total sample minus retrograde cases), provided outcomes were reported as mutually exclusive binary events. When questionnaire-based assessments were used, reported rates of preserved ejaculation were extracted directly. Secondary outcomes included postoperative IPSS, Qmax, PVRU, erectile function scores (IIEF), and operative time (minutes).
Statistical analyses were conducted using RevMan 5.4.1 software. Dichotomous outcome (presence of antegrade ejaculation) was analyzed using risk ratios (RR) with 95% CI. Continuous outcomes (IPSS, Qmax, PVRU, and operative time) were analyzed using mean differences (MD) with 95% CI. Erectile function outcomes were assessed using different validated questionnaires across studies (e.g. IIEF-5, IIEF-15). Because these instruments use different scoring ranges, pooled analysis was conducted using standardized mean differences (SMDs) to allow comparison across scales while preserving relative effect size. For studies reporting results using medians and interquartile ranges, the values were converted to mean and standard deviations by calculation using established statistical methods. 18 The following studies required conversion: Elshazly et al. 9 and Eliwa et al. 13 When outcomes were presented in graphical form (bar charts with standard deviations). the values were extracted using WebPlotDigitizer. 19 This approach was applied to the study by Abolazm et al. 8 Outcomes were considered statistically significant if the p-value was <0.05.
Given the clinical heterogeneity across studies in terms of surgical technique performed by different surgeons and settings, patient population, and follow-up period, a random-effects model was applied to account for both within-study and between-study variability, yielding a more conservative pooled estimate.
Classification subgroups of EP surgery approaches
For the purpose of subgroup analysis in this review, all included ejaculation-preserving techniques were classified based on the anatomical extent of preserved structures during prostate resection into two distinct group:
Peri-verumontanum sparing was defined as procedures that preserved tissue around the verumontanum, covering both limited and more extensive preservation in this area.
Peri-verumontanum sparing with bladder neck preservation subgroup included studies with preservation techniques that extend preservation from the peri-verumontanum up to the bladder neck region, regardless of whether supramontanal area was spared during the resection.
Surgical techniques in the studies included were independently reviewed and classified based on the anatomical regions described as being preserved.
Results
Literature search
A total of 956 articles were identified in the PubMed, ScienceDirect, and Cochrane Library databases. No additional records were identified through other sources. After removing 48 duplicate articles, 879 articles were excluded based on their titles or abstracts, remaining 29 articles from which 3 were not retrievable. The remaining 26 articles underwent full-text scrutiny. Among these, 18 articles were eliminated due to reasons such as review (n = 1), editorial comment (n = 4), no comparison (n = 4), insufficient outcome (n = 2), different study models (n = 6) and not written in English (n = 1). Ultimately, 8 articles encompassing a total of 580 participants, were selected for this meta-analysis.8–15 Figure 1 shows the PRISMA flowchart for this review. Figure 2 display the risk of bias assessments results of the studies included.
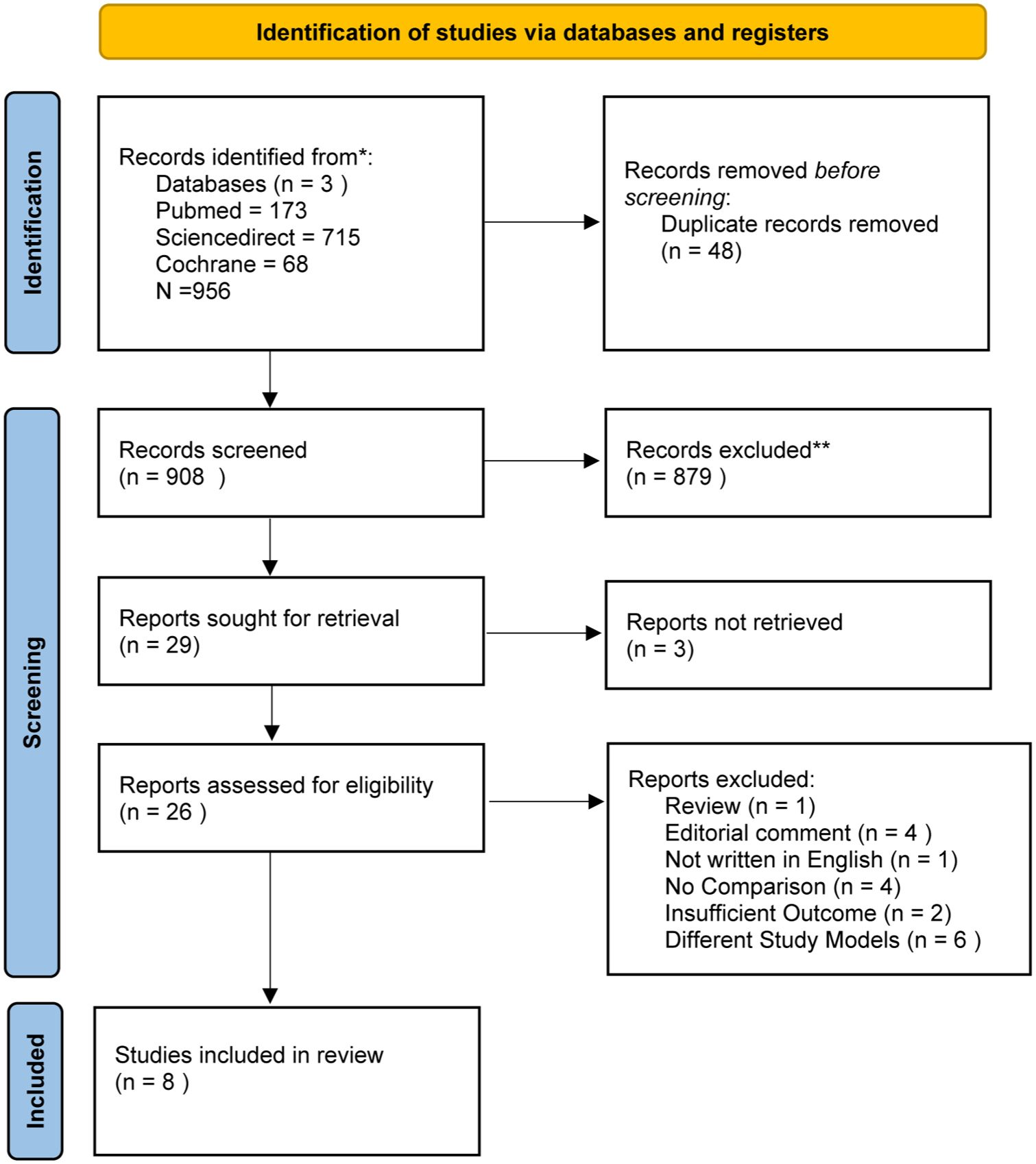
PRISMA flowchart.
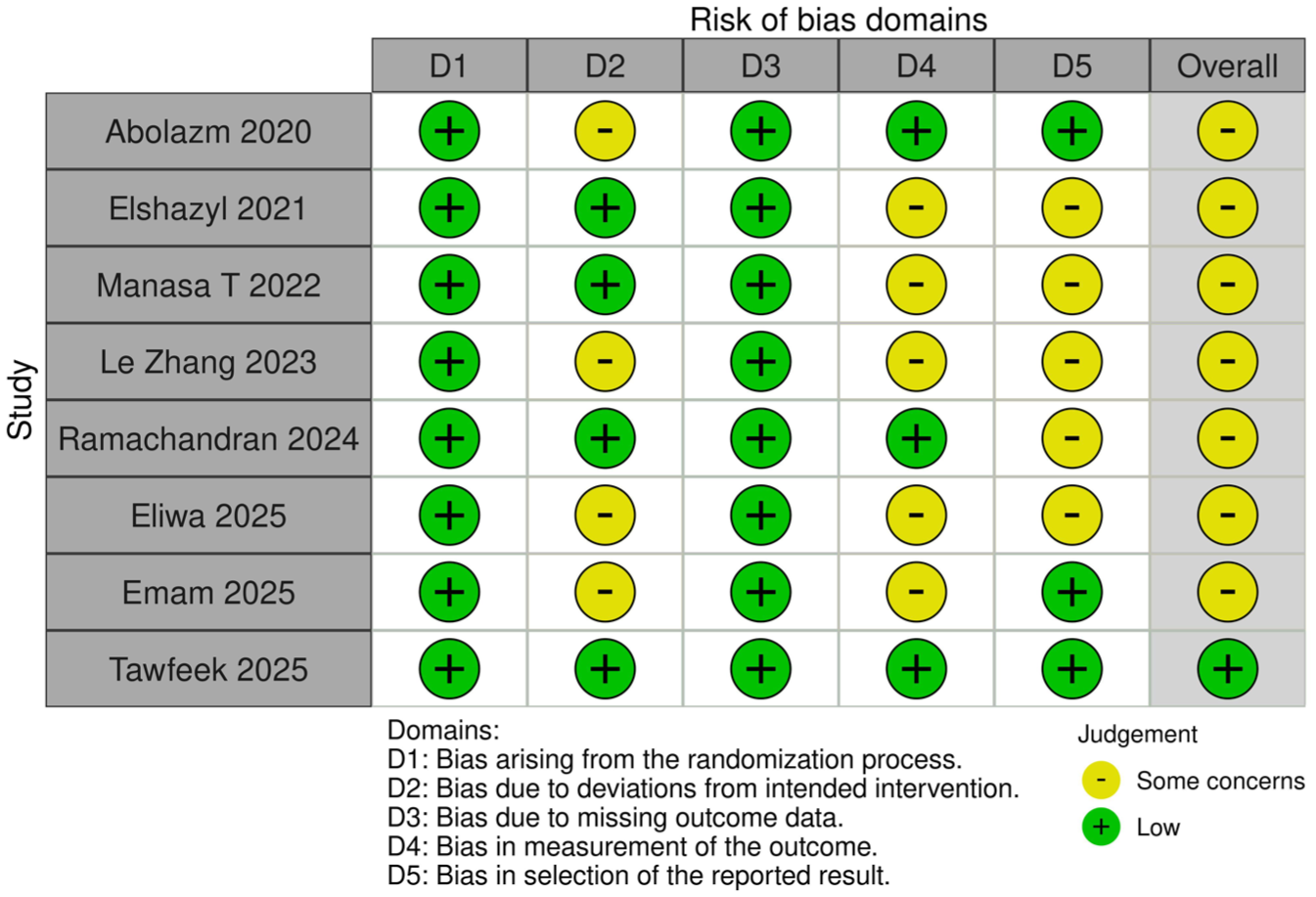
Risk of bias using Cochrane risk of bias tool for randomized trials (RoB 2).
Study characteristics
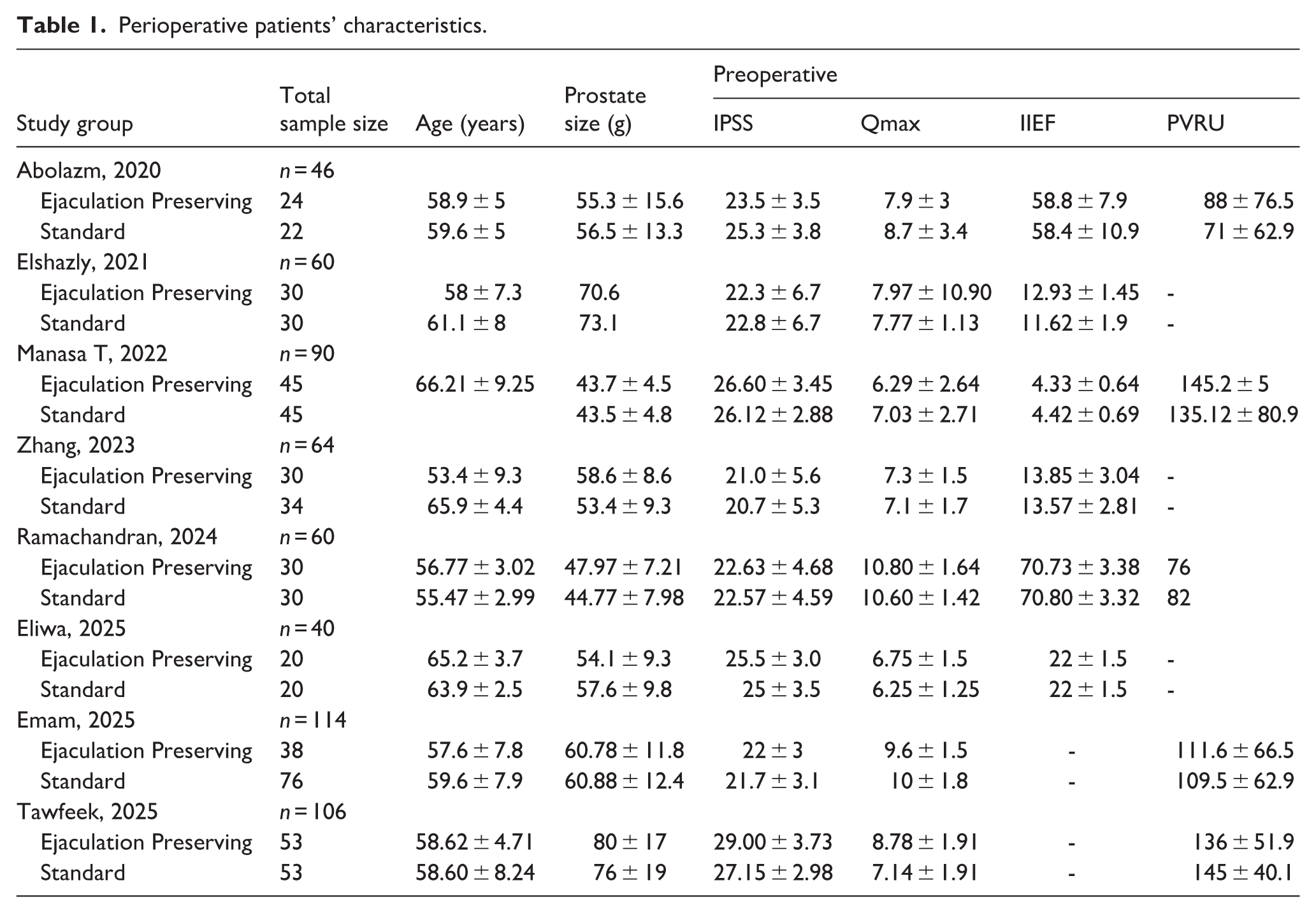
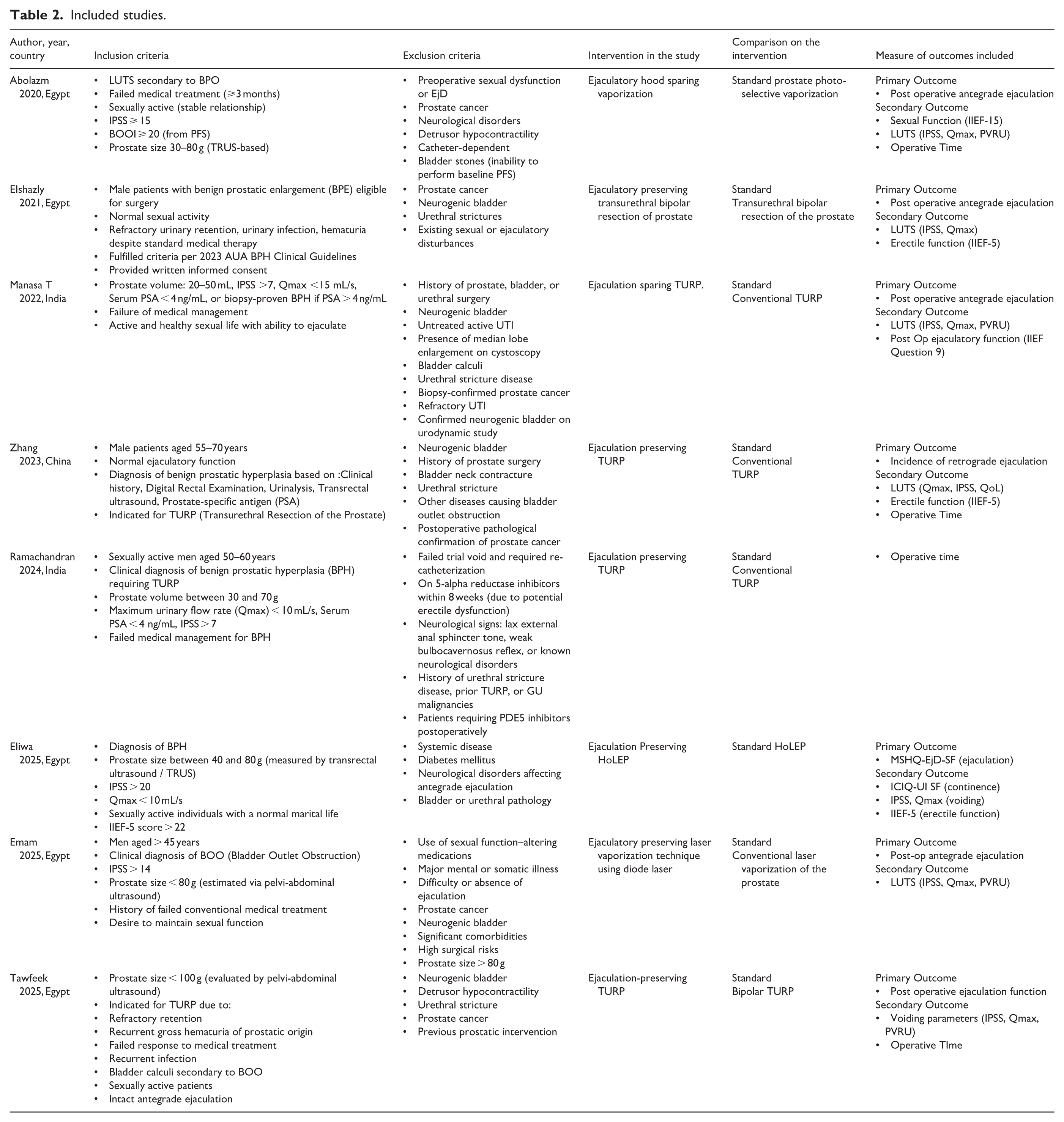
Across the included trials included in this review, baseline patient demographics were comparable between the groups. Patients mean age ranged from 53 to 66 years old. Table 1 outline the perioperative patient characteristics, and Table 2 displays the included studies.
Perioperative patients’ characteristics.
Included studies.
Number of patients with preserved antegrade ejaculation
Figure 3(a) shows Ejaculation-preserving techniques significantly improved the rate of preserved antegrade ejaculation compared to standard prostate resection (RR 3.13, 95% CI 2.43–4.02, p < 0.00001). Subgroup analysis showed similar benefit between techniques involving Peri-verumontanum sparing only (RR 3.57, 95% CI 2.20–5.79) and those with additional bladder neck preservation (RR 2.94, 95% CI 2.12–4.06), with no significant difference between subgroups (p = 0.51).
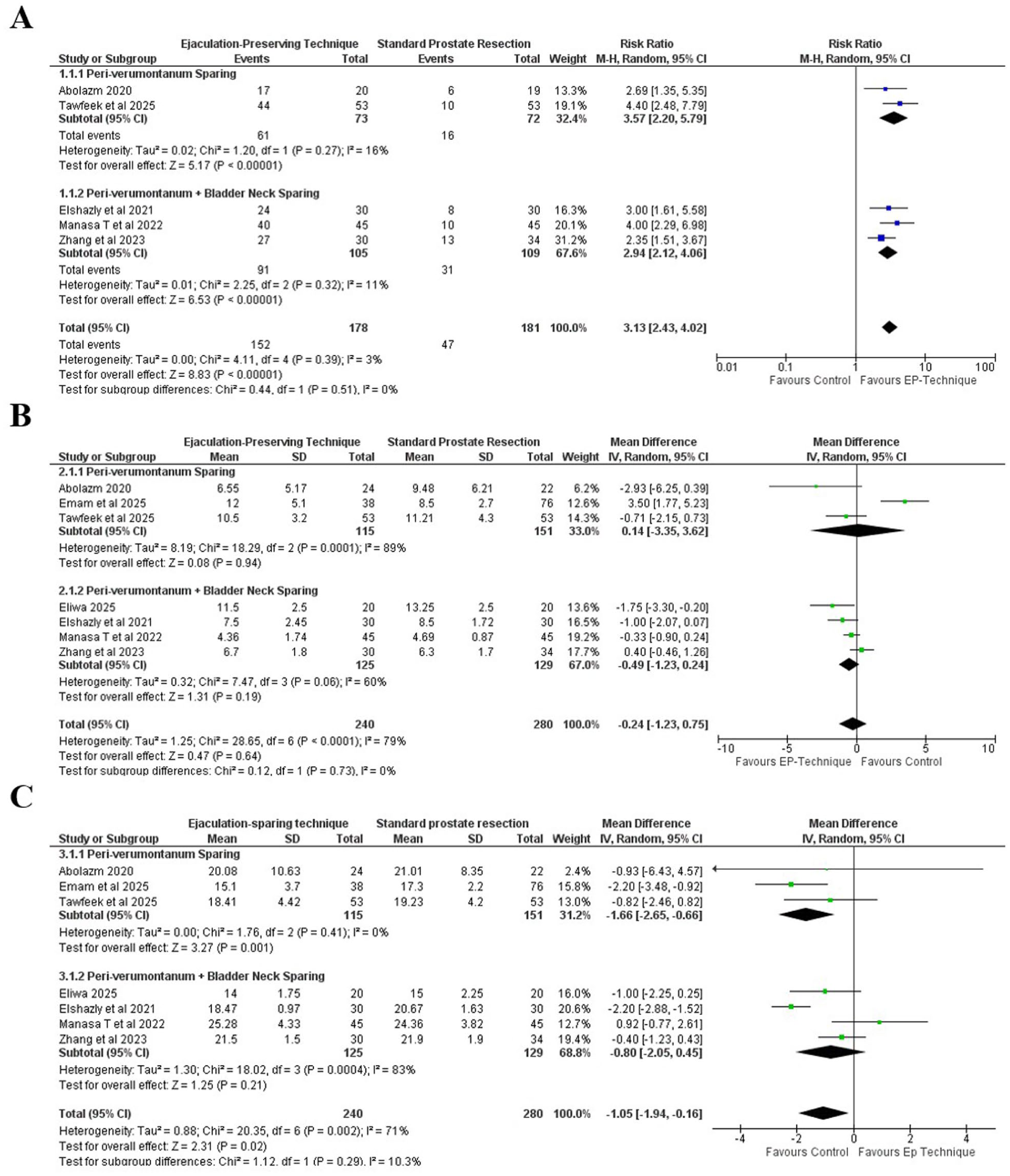
(a) Number of patients with preserved antegrade ejaculation, (b) postoperative IPSS (International Prostate Symptom Score), and (c) postoperative Qmax.
Postoperative IPSS (International Prostate Symptom Score) 3 months post-surgery
Figure 3(b) Postoperative IPSS did not differ significantly between ejaculation-preserving techniques and standard prostate resection (MD −0.24, 95% CI −1.23 to 0.75, p = 0.64). Subgroup analysis likewise showed no significant effect in either the peri-verumontanum sparing only group (MD 0.14, 95% CI −3.35 to 3.62) and those with additional bladder neck preservation (MD −0.49, 95% CI −1.23 to 0.24), with no significant subgroup difference (p = 0.73).
Postoperative Qmax 3 months post-surgery
Figure 3(c) EP techniques were associated with a modest reduction in postoperative Qmax compared with standard resection (MD −1.05 mL/s, 95% CI −1.94 to −0.16; p = 0.02; I2 = 71%). Subgroup analyses suggested a reduction in the peri-verumontanum-only group (MD −1.66, 95% CI −2.65 to −0.66), whereas no clear difference was observed in the peri-verumontanum + bladder neck group (MD −0.80, 95% CI −2.05 to 0.45). No significant between-subgroup difference was detected (p = 0.29).
Operative time
Figure 4(a) Ejaculation-sparing techniques were associated with a shorter operative time compared to standard prostate resection (mean difference −6.05 minutes; 95% CI −11.84 to −0.26; p = 0.04). However, substantial heterogeneity was observed (I2 = 78%), which may limit the robustness of this finding and could reflect variations in surgical methods and clinical settings.
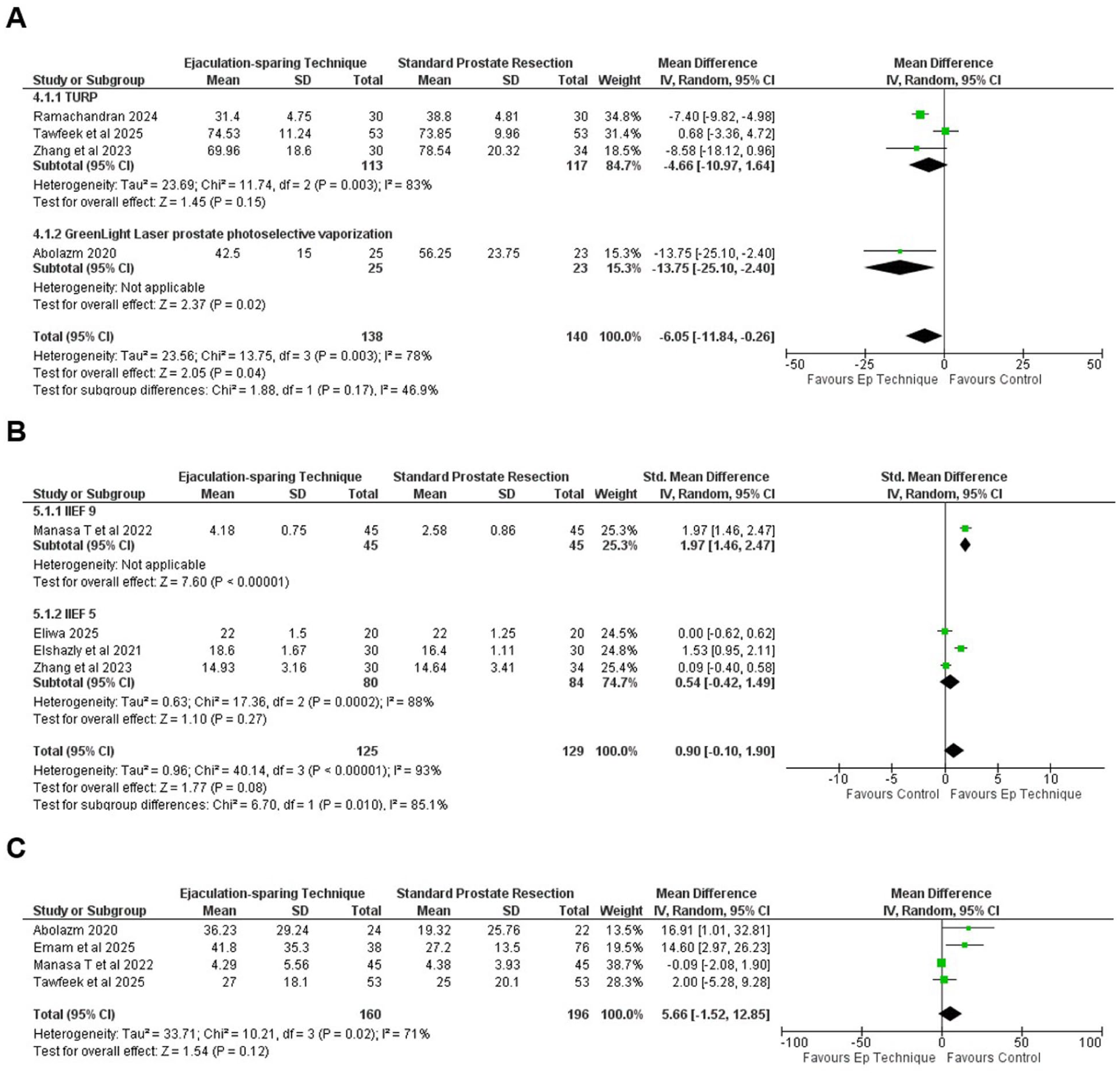
(a) Operative time, (b) postoperative erectile function (IIEF), and (c) postoperative PVRU.
Postoperative erectile function (IIEF)
Figure 4(b) shows the pooled analysis of postoperative erectile function using IIEF-5 and IIEF-9 scores. Overall, ejaculation-preserving (EP) techniques showed a non-significant trend toward better outcomes (SMD = 0.90, 95% CI [–0.10, 1.90], p = 0.08).
Postoperative PVRU
Figure 4(c) compares postoperative post-void residual urine (PVRU) volumes between ejaculation-preserving and standard resection techniques. The EP group showed a non-significant trend toward higher PVRU (MD = 5.66 mL, 95% CI [–1.52, 12.85], p = 0.12), suggesting similar effectiveness in bladder emptying.
Sensitivity analysis
Leave-one-out analyses showed that the findings for antegrade ejaculation, IPSS, PVRU, and IIEF were robust, with no material change in direction or significance when individual studies were excluded. For the primary outcome, most studies reported 3-month postoperative data while one study reported 12-month follow-up. A sensitivity analysis excluding the 12-month study was performed to assess the impact of follow-up variability, and the pooled effect estimate remained directionally and statistically consistent. For Qmax, the pooled effect became attenuated and lost statistical significance after exclusion of one study, indicating sensitivity of this outcome to that trial. For operative time, exclusion of certain studies reduced the precision and rendered the result non-significant, although the direction of effect consistently favored ejaculation-preserving techniques.
Discussion
Ejaculation is considered as crucial component of sexual well-being in sexually active men, and the loss of antegrade ejaculation remains one of the major limitations of conventional prostate resection. A 20-year systematic review reported an overall of 46% incidence of retrograde ejaculation after TURP, underscoring its significant impact on postoperative ejaculation function. 20 As a result, sexually active men with LUTS due to BPO indicated for surgery may postpone surgery or opt for less invasive but potentially less effective alternatives.21–23 By refining anatomical targets during resection of the prostate, surgeons can reduce the incidence of retrograde ejaculation without compromising core therapeutic goals. 7
The result from this review shows that EP prostate resection techniques maintain antegrade ejaculation at significantly higher rates (RR 3.13) compared with conventional approaches, without compromising urinary symptom relief or bladder emptying and erectile function. Notably, stratification by anatomical preservation using subgroup analysis showed no significant difference in outcomes between techniques that spared both the peri-verumontanum and bladder neck, and those that targeted the peri-verumontanum alone (RR 2.94 vs 3.57; p = 0.51).
The bladder neck has been regarded as a key structure in preventing retrograde ejaculation. The bladder neck as a circular extension of the detrusor muscle under sympathetic adrenergic control, contracts involuntarily during ejaculation to prevent retrograde flow. The prostate merges with the bladder neck and, through its smooth muscle and fibromuscular stroma, that contributes to dynamic urinary outflow resistance. 24 Based on this concept, surgical approaches aimed to maintain ejaculatory function included preservation of bladder neck. However, despite this understanding, a study raising question about whether the bladder neck is truly indispensable prompting a deeper look into other anatomical contributors to ejaculation control. 25
In contrast to the understanding concept described in the preceding paragraph, Gil-Vernet et al., through the first dynamic endorectal ultrasound study of ejaculation, proposed a different perspective. Their real-time imaging revealed that antegrade ejaculation occurs through a coordinated sequence beginning with a caudal shift of the verumontanum, which briefly seals against the opposing urethral wall. This action, supported by the synchronized contractions of the bulbospongiosus muscle and external urethral sphincter, propelled seminal fluid distally without relying on complete closure of the bladder neck. 25 These findings highlight the verumontanum and adjacent structures collectively referred to as the ejaculatory high-pressure zone as crucial components in maintaining antegrade ejaculation, especially when designing surgical strategies that aim to preserve sexual outcomes.21,26
Our results suggest that ejaculation-preserving techniques are associated with higher rates of antegrade ejaculation compared with conventional prostate resection. These findings are in agreement with a previous meta-analysis that also reported superior preservation rates with ejaculation-preserving techniques compared to standard resection. 27 Our review expands on this earlier work by including more recent studies and applying anatomical subgroup classification, thereby offering a more granular perspective on how preservation extent may relate to functional outcomes. Subgroup findings are consistent with physiological observations suggesting that the peri-verumontanum region plays a central role in antegrade ejaculation. Results between the two subgroups shows a similar trend favoring EP prostate resection with no significant difference between them. While these findings strengthen the case for focused peri-verumontanum preservation, surgical decision-making must also account for additional potential trade-offs for the surgery techniques that extend preservation proximally beyond the verumontanum, such as those including supramontanal or bladder neck sparing. These approaches inevitably leave a greater portion of periurethral tissue intact, raising the concern that more extensive preservation could increase the likelihood of increased residual adenoma, with possible implications for symptom recurrence or retreatment. 28 Although our meta-analysis did not directly assess recurrence rates or retreatment outcomes, the possibility of incomplete adenoma resection warrants further investigation. Future studies should aim to better define the balance between functional preservation and complete adenoma clearance to guide optimal surgical planning.
Secondary functional outcomes further strengthen the safety profile of EP approaches. IPSS improvement and PVRU volumes were similar between groups, indicating comparable efficacy in symptom relief and bladder emptying. EP techniques were associated with a reduction in postoperative Qmax compared with standard resection (MD −1.05 mL/s). Although statistically significant, the magnitude of this difference is small and likely below the threshold of clinical relevance, as postoperative values in both groups remained within ranges consistent with symptomatic improvement. Furthermore, sensitivity analysis demonstrated that the statistical significance of the Qmax difference was lost following exclusion of one study, suggesting that this finding may be driven by a single influential trial. Therefore, the observed reduction in Qmax should be interpreted with caution. Erectile function outcomes assessed with IIEF were comparable overall. EP techniques reduced operative time by an average of 6.05 min (95% CI −11.84, −0.26) compared with conventional resection. Reinforcing that anatomical preservation can be achieved without compromising operative outcomes.
Surgeon experience was inconsistently reported across the included studies. Most trials described procedures as being performed by experienced surgeons; however, two studies (Emam et al. 14 and Tawfeek et al. 15 ) did not report surgeon experience, case volume, or learning curve status. Ejaculation-preserving techniques require precise identification of peri-verumontanum and adjacent anatomical landmarks, which may increase technical complexity and introduce a learning curve effect. Therefore, the potential impact of surgeon experience on operative time and reproducibility cannot be fully excluded, and generalizability to lower-volume or early-learning settings remains uncertain. In addition, variability in operative duration may be influenced by surgeon workload, ergonomic demands, and fatigue particularly in technically demanding minimally invasive platforms as highlighted in recent literature examining surgeon performance and fatigue in urologic surgery. 29
These findings align with emerging surgical recommendation. A recent expert consensus by Lebdai et al. established a standardized technique for ejaculation-preserving surgery. Their protocol, developed within the PARTURP randomized trial, prioritizes preservation of the peri-verumontanum and adjacent posterior urethra. 30 Although this standardized technique has yet to be validated in future larger comparative trials, our pooled results quantitatively support the functional importance of these preservation targets across different surgical modalities, reinforcing the physiological basis for their inclusion in preservation strategies.
Limitation of this study was firstly the limited number of studies within each anatomical subgroup, which may limit statistical power and generalizability. Secondly, variations of methodological and technical introduced heterogeneity across included trials, including differences in surgical platform, preservation extent, and operative technique. Because few trials were available per modality, we could not perform reliable modality-specific subgroup analyses; therefore, findings should be interpreted as reflecting the ejaculation-preserving concept across platforms. Long-term outcomes such as recurrence rates, need for retreatment, and durability of symptom relief were not consistently reported across studies. These parameters are critical when weighing functional preservation against oncological and obstructive completeness, and their absence limits the ability to fully assess the long-term clinical trade-offs of extended preservation strategies. Furthermore, Ejaculatory function was not uniformly defined across studies. Some trials reported antegrade ejaculation rates directly, whereas others reported retrograde ejaculation or questionnaire-based outcomes. Although we harmonized these definitions mathematically where appropriate, variation in assessment tools and reporting methods may introduce classification bias. Several studies exhibited concerns in specific risk-of-bias domains, pooled effect estimates were directionally consistent. Nonetheless, methodological limitations reduce overall certainty, and findings should be interpreted cautiously. Lastly, the assessment of ejaculatory outcomes was subjected to patient reporting, making pooled analysis vulnerable to reporting bias. In addition, this review did not directly compare peri-verumontanum sparing only and techniques that included bladder neck preservation as a head-to-head comparison, subgroup results should be interpreted as exploratory overview rather than definitive evidence of anatomical superiority. This meta-analysis is intended to serve as a stepping stone for future research with standardized definitions, consistent outcome reporting, and direct comparisons between preservation strategies.
By stratifying techniques according to their anatomical preservation targets, this meta-analysis provides an overview that clarifies the functional relevance of specific zones such as the peri-verumontanum and bladder neck. The evidence supports a more focused approach to anatomical preservation that can maintain antegrade ejaculation without compromising urinary outcomes, particularly in younger or sexually active patients for whom postoperative sexual quality of life is a priority.
Conclusion
Current evidence suggests that ejaculation-preserving prostate resection techniques improve preservation of antegrade ejaculation without clinically meaningful compromise in short-term urinary outcomes. Stratified analyses indicate that peri-verumontanum preservation alone may provide comparable functional outcomes to more extensive preservation strategies. However, these findings should be interpreted cautiously given methodological heterogeneity and variability in study quality. The absence of consistent long-term durability data further limits definitive conclusions. Larger, standardized trials with extended follow-up are needed to confirm reproducibility and long-term clinical trade-offs.
Supplemental Material
sj-docx-1-urj-10.1177_03915603261450670 – Supplemental material for Optimizing ejaculatory function after prostate resection: A stratified meta-analysis of anatomical preservation strategies
Supplemental material, sj-docx-1-urj-10.1177_03915603261450670 for Optimizing ejaculatory function after prostate resection: A stratified meta-analysis of anatomical preservation strategies by Syah Mirsya Warli and Satria Gohtama in Urologia Journal
Footnotes
Author contributions
Study concept and design: Syah Mirsya Warli, Satria Gohtama. Data acquisition: Satria Gohtama. Data analysis and interpretation: Syah Mirsya Warli, Satria Gohtama. Drafting of the manuscript: Syah Mirsya Warli, Satria Gohtama. Critical revision of the manuscript: Syah Mirsya Warli. Final approval of the version to be published: Syah Mirsya Warli, Satria Gohtama.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data supporting this study has been included within the article and/or supporting materials.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.