
Abstract
Penile prosthesis implantation plays a crucial role in gender-affirming surgery (GAS) for transgender men, helping align physical traits with their gender identity. Phalloplasty, which involves creating a neophallus, often includes penile prosthesis implantation to restore erectile function and enable sexual intercourse.
This non-systematic review analyzed studies from PubMed and MEDLINE databases (2000–February 2025), focusing on original studies, excluding animal models and non-English studies. The review explores the types of penile prosthesis, surgical techniques, patient outcomes, and complications.
The three main types of penile prosthesis are the two-piece inflatable, semi-rigid (malleable), and three-piece inflatable. The three-piece inflatable prosthesis is most commonly used in transgender men due to its natural erectile and flaccid states. While inflatable devices offer superior functionality, they are more prone to complications such as mechanical failure, infection, and device migration. Malleable prosthesis, though easier to implant and less prone to failure, can cause discomfort and esthetic issues due to their semi-rigid state. Functional success rates for penile prosthesis implantation in transgender men range from 70% to 85%, with high patient satisfaction despite complications. Psychologically, implantation often reduces gender dysphoria, improving self-esteem and sexual function. However, unique challenges remain, such as scarring and the absence of erectile tissue in the neophallus.
Advancements in prosthetic design, surgical techniques, and tissue engineering aim to reduce complications and enhance both the physical and psychological well-being of transgender men.
Introduction
Gender-affirming surgery (GAS) is a critical aspect of medical care for transgender individuals, providing them with the opportunity to align their physical bodies with their gender identity. For transgender men (individuals assigned female at birth but who identify as male), one of the most complex and life-changing procedures available is phalloplasty, which may involve the implantation of a penile prosthesis. A penile prosthesis is a medical device implanted into the penis to enable erectile function and thereby facilitate penetrative sexual intercourse.
In 1936, Russian physician, Nikolaj A. Bogaraz created the first autologous penile implant using a patient’s own rib cartilage. 1 In 1973, nearly 40 years later, the first inflatable prosthesis and the Small-Carrion malleable penile prosthesis were introduced. Currently, penile implants are considered the gold standard treatment for several conditions in males, such as medically refractory erectile dysfunction (ED) and severe penile trauma.
There are three primary types of penile prostheses: the two-piece inflatable device, the semi-rigid (malleable) device, and the three-piece inflatable device. 2 Each prosthesis requires a distinct surgical approach and implantation technique. The three-piece prosthesis is widely regarded by many urologists as superior to the two-piece prosthesis and is used in more than 80% of penile implant procedures. 2 Furthermore, the most commonly implanted prosthetic device in transgender men is the three-piece inflatable penile prosthesis (IPP). 3
Given the intricate nature of phalloplasty, the inclusion of a penile prosthesis is often accompanied by numerous technical challenges and potential complications. This narrative review aims to provide an overview of the types of penile prostheses available, the surgical techniques employed, the outcomes, and the associated complications in transgender men. Additionally, it explores patient satisfaction, quality of life, and future directions in this field.
Methodology
In this non-systematic review, a comprehensive search was conducted in the PubMed and MEDLINE databases from 2000 to February 2025 using the following search terms: “penile prosthesis” AND “transgender male,” OR “implantation,” OR “surgical techniques of penile prosthesis,” OR “types of penile prosthesis,” OR “innovations in penile prosthesis,” OR “penile prostheses” AND “future,” OR “penile prostheses” AND “quality of life.”
The screening process was performed independently by one author and subsequently verified by eight co-authors. Any disagreements were resolved by the final author. Only original studies were included. Studies involving animal models or published in languages other than English were excluded. Studies not specifically pertaining to transgender individuals were also excluded.
Results
Penile prosthesis implantation in transgender men demonstrates varied outcomes, with functional success rates ranging from 70% to 85%. The most commonly used device is the three-piece inflatable prosthesis (IPP), preferred for its ability to provide a more natural erection and flaccid state.
While inflatable prostheses offer superior functional outcomes, they are associated with higher complication rates compared to malleable prostheses, including mechanical failure, infection, and erosion. Early complications historically included higher infection rates (5%–10%), hematoma, and seroma formation, likely due to the complexity of phalloplasty and neourethral creation. 4 Mechanical failure, primarily in inflatable devices, occurred in 3%–19% of cases, often involving pump malfunction or fluid leakage. Lower rates of mechanical dysfunction have been reported with malleable prostheses, likely due to their simpler design.
Late complications such as prosthesis erosion and extrusion were more common in malleable devices, particularly due to the absence of natural erectile tissue in transgender men. 5 Additionally, device migration and urethral complications (e.g. strictures and fistulas) were reported. 6
Despite these complications, patient satisfaction remained high, with many transgender men reporting improved psychological well-being, reduced gender dysphoria, and enhanced self-esteem. Sexual function, including the ability to engage in penetrative intercourse, was rated as satisfactory; however, sensation and orgasmic function remained problematic for some individuals.7,8 The ability to stand and void postoperatively also contributed significantly to patient satisfaction.
Ongoing advancements in prosthetic design, tissue engineering, and surgical techniques may reduce complications and improve functional outcomes. These innovations include enhanced prosthetic durability, improved vascularization of the neophallus, and the potential development of bioengineered tissues to support neophallus function and reduce erosion risk. 1
Discussion
Surgical techniques
Phalloplasty involves the construction of a neophallus using various types of flaps, often derived from donor sites such as the radial forearm, the anterolateral thigh, or the latissimus dorsi. The choice of flap depends on several factors, including the surgeon’s expertise, the patient’s body habitus, and personal preferences. The goal is to create a neophallus that is esthetically satisfactory, sensate, and capable of enabling voiding while standing.
The surgery is typically performed in stages, with the initial stage focusing on neophallus creation. Later stages may include urethral lengthening, glansplasty, scrotoplasty, and the insertion of testicular implants. The final stage often involves penile prosthesis implantation, which represents the most technically demanding component due to the absence of native erectile tissue.
Penile prostheses: types and mechanisms
Penile prostheses are classified into two broad categories: malleable (non-inflatable) and inflatable prostheses.
Malleable (non-inflatable) prostheses
Malleable prostheses consist of bendable rods implanted into the neophallus. These rods can be manually positioned to simulate an erect or flaccid penis. Their simplicity is a major advantage, as they are less prone to mechanical failure and are easier to implant.
The malleable prosthesis is generally considered functionally inferior to the three-piece inflatable penile prosthesis. 9 In staged approaches, a malleable prosthesis may initially be implanted. 10 The development of a fibrous capsule around the malleable device can facilitate subsequent replacement with a three-piece inflatable prosthesis.
However, disadvantages include a constant semi-rigid state, which may lead to discomfort, esthetic concerns, and potential long-term damage to the neophallus. 11
Inflatable prostheses
Inflatable prostheses are more complex and typically consist of three components: two inflatable cylinders, a reservoir, and a pump. The cylinders are implanted into the neophallus, the reservoir is placed in the abdomen, and the pump is situated in the scrotum. 12 When activated, the pump transfers fluid from the reservoir to the cylinders, creating an erection.
This type of prosthesis provides a more natural erection and flaccid state, offering advantages in both function and esthetics. 13 However, the complexity of the device introduces a higher risk of mechanical failure and infection. 14
Two-piece inflatable penile prosthesis (IPP)
Currently, the most widely used two-piece IPP is the Ambicor inflatable prosthesis, which consists of a pump placed within a scrotal Dartos pouch and parylene-coated cylinders implanted in the corpora. 15 The device can be adjusted for proximal corporal and crural placement by adding rear tip extenders (RTEs), which range in length from 14 to 22 cm and in diameter from 12.5 to 15.5 mm.
The device is inflated by repeated manual compression of the pump, which transfers fluid into the cylinders, and deflated by activating the release valve. Two-piece IPP total complication rates ranged from 2.1% to 11.2%, mechanical failure rates from 0.7% to 6.1%, and infection rates from 0.7% to 4.8%, according to a 2018 literature analysis. 16
Three-piece inflatable prostheses
Three-piece prostheses account for over 80% of the penile implant market in the United States. 17 Early prototypes were introduced in the 1980s and included the same fundamental components as contemporary devices: a scrotal pump, two intracorporal inflatable cylinders, and an abdominal fluid reservoir.
Significant technological advancements during the 1980s and 1990s led to a reduction in complication rates from over 50% at initial introduction to approximately 13% after 4 years. 18
Three-piece penile prostheses may be implanted using either a trans-scrotal or infrapubic approach. 19 The penoscrotal technique offers advantages such as improved pump placement, enhanced corporal visualization, and a reduced risk of dorsal nerve injury. 19 In contrast, the infrapubic approach may allow for faster device placement and easier reservoir visualization. 19
Considerations for transgender men
The implantation of a penile prosthesis in transgender men presents unique challenges compared to cisgender men. The neophallus lacks the natural erectile tissue present in a natal penis, and the anatomy may vary depending on the type of phalloplasty performed. Additionally, the potential for scar tissue, the absence of a natural tunica albuginea, and the need for a neourethra complicate the surgical procedure. Outstanding challenges include achieving reliable anchorage of the PP, ensuring its long-term stability, and identifying the most effective approach to erosion prevention. 20
Outcomes and complications
Success rates and functional outcomes
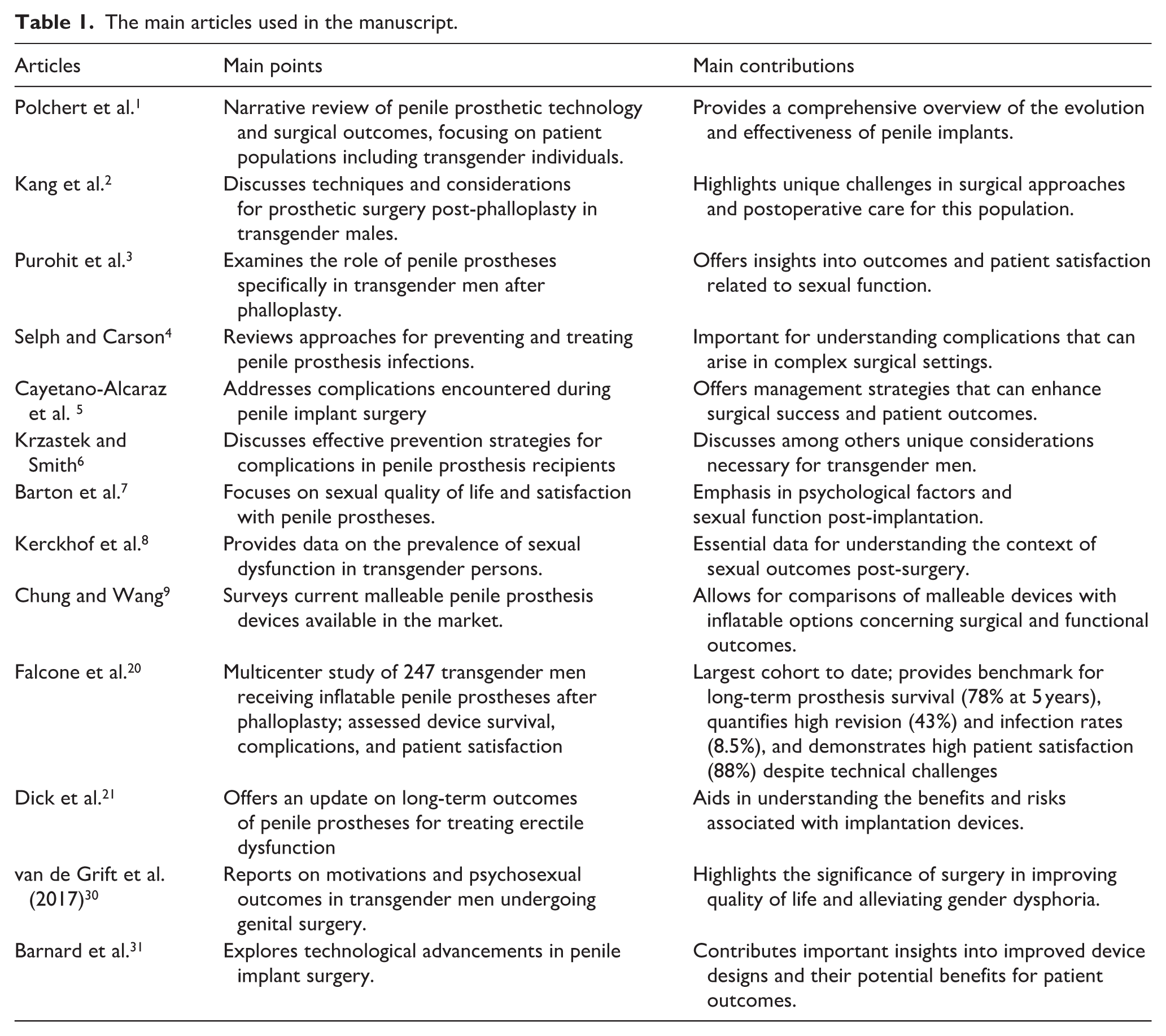
The success of penile prosthesis implantation is generally measured by the device’s functionality, patient satisfaction, and complication rates. 21 For transgender men, the success of these devices is often tempered by the complex interplay between achieving desired sexual function and avoiding complications. The reported success rates for penile prosthesis implantation in transgender men vary, with studies indicating a functional success rate ranging from 70% to 85%. Functionally, inflatable prostheses are often preferred due to their ability to produce a more natural erection and flaccid state. However, they are associated with higher complication rates than malleable prostheses. Studies have shown that up to 40% of transgender men experience some form of complication following the implantation of an inflatable prosthesis, including device malfunction, infection, and erosion. 22 Recent evidence from a multicenter study of 247 transgender men undergoing phalloplasty with inflatable penile prosthesis insertion demonstrated that approximately 78% of implants remained in place at 5 years, with a high patient satisfaction rate of 88%, although only 77% reported regular sexual use of the device. The study also highlighted a notable overall revision rate of 43% and an infection rate of 8.5%, emphasizing the technical challenges and increased risk profile in this population. 20
Complications
Complications associated with penile prostheses in transgender men can be categorized into early (occurring within the first year post-implantation) and late complications.
Early complications
- Infection: Infection rates in penile prosthesis implantation are higher in transgender men than in cisgender men, possibly due to the extensive surgical procedures required to create the neophallus and the presence of a neourethra. Infection can necessitate the removal of the prosthesis, leading to significant morbidity. 4
- Hematoma and Seroma Formation: These are common early complications that may arise due to the extensive dissection required during surgery. Proper intraoperative hemostasis and postoperative management are crucial in minimizing these risks.
- Mechanical Failure: Although more common in inflatable prostheses, mechanical failure can occur in any type of prosthesis. This can result from a malfunctioning pump, fluid leakage, or a failure of the inflatable cylinders. Evidence from Falcone et al. supports that mechanical and other device-related complications are frequent, contributing to an overall revision rate of 43% in transgender men. 20 The longevity of implants in phalloplasty is generally considered significantly shorter compared with that observed in patients treated for erectile dysfunction.23–29
Late complications
- Erosion and Extrusion:
Erosion refers to the prosthesis wearing through the neophallus or the scrotal skin, which can lead to extrusion. This complication is more common in malleable prostheses due to their constant pressure on the surrounding tissues. The thinness of the neophallus and the lack of natural tissue planes in transgender men increase the risk. 5
- Device Migration: Migration of the prosthesis within the neophallus can occur, especially in cases where the neophallus lacks sufficient structural support. This can lead to discomfort, dysfunction, and the need for surgical revision. 6
- Urethral Complications: The construction of a neourethra in phalloplasty can lead to urethral complications such as strictures, fistulas, and diverticula. These complications can complicate the insertion and function of a penile prosthesis, sometimes necessitating additional surgeries. 6
Patient satisfaction and quality of life
Patient satisfaction following penile prosthesis implantation is a multifaceted issue, influenced by both the functional outcomes of the prosthesis and the psychological impact of achieving a body congruent with one’s gender identity. Studies have shown that despite the high rates of complications, many transgender men report satisfaction even up to 88% with their prostheses, as the devices contribute significantly to their sense of masculinity and sexual function.20,30
Psychological impact
The psychological benefits of penile prosthesis implantation should not be underestimated. For many transgender men, the ability to engage in penetrative sexual intercourse is integral to their gender identity and psychological well-being. The prosthesis provides not only sexual function but also helps alleviate gender dysphoria, which can have a profound impact on overall mental health. 30
Sexual function
Sexual function, including the ability to achieve penetrative intercourse, is often reported as satisfactory by many transgender men with penile prostheses, particularly those with inflatable devices. 7 However, issues such as sensation and orgasmic function can remain problematic, as the neophallus lacks the same sensory innervation as a natal penis. 8 The ability to stand to void is another significant factor contributing to patient satisfaction, with many patients reporting a high degree of contentment when this function is successfully achieved postoperatively.
Future directions and innovations
As the field of transgender surgery continues to evolve, so too does the technology and surgical techniques associated with penile prosthesis implantation. Future directions in this area focus on reducing complication rates, improving device functionality, and enhancing patient satisfaction. 10
Advances in prosthetic design
Improvements in prosthetic design are ongoing, with a focus on developing devices that are more reliable and better suited to the unique anatomical challenges presented by transgender men. Innovations may include prostheses with adjustable rigidity, better resistance to erosion, and designs that are more anatomically congruent with the neophallus. 31
Tissue engineering and regenerative medicine
Tissue engineering and regenerative medicine offer exciting possibilities for the future of penile prosthesis implantation in transgender men. Research into the development of bioengineered tissues that could replicate the tunica albuginea or provide better structural support to the neophallus is ongoing. These advances could potentially reduce the risk of complications such as erosion and extrusion. 32
Enhanced surgical techniques
Refinements in surgical techniques are also critical to improving outcomes. Techniques that focus on better vascularization of the neophallus, more secure implantation of the prosthesis, and innovative methods for urethral construction are all areas of active research. These advancements could significantly improve both the functional outcomes and the longevity of penile prostheses in transgender men. 33
Patient-centered care and shared decision-making
As with all aspects of transgender healthcare, a patient-centered approach that involves shared decision-making is paramount. This involves not only discussing the risks and benefits of penile prosthesis implantation with patients but also considering their individual goals, expectations, and concerns. Enhanced preoperative counseling and postoperative support are essential components of this approach.
Conclusion
Penile prosthesis implantation in transgender men is a complex and evolving field that presents unique challenges compared to implantation in cisgender men. While the procedure can significantly enhance quality of life by enabling sexual function and reducing gender dysphoria, it remains associated with relatively high complication rates.
Ongoing advancements in prosthetic design, surgical techniques, and tissue engineering hold promise for improving outcomes. Ultimately, the success of penile prosthesis implantation in transgender men is measured not only by technical surgical outcomes but also by the extent to which it enables individuals to achieve bodily congruence, improved quality of life, and enhanced psychological well-being (Table 1).
The main articles used in the manuscript.
Footnotes
Author contributions
Conceived the study and design: Sotirios Kapsalos- Dedes, Themistoklis Bellos, Petros Drettas
Data collection and analysis: Stamatios Katsimperis, Aggelos Tzoras, Fotios Gasparos
Manuscript writing and statistical analysis: Sotirios Kapsalos- Dedes, Themistoklis Bellos, Nikolaos Kostakopoulos, Lazaros Tzelves, Panagiotis Stamatakos
Manuscript editing and review: Nikolaos Kostakopoulos, Nikolaos Ferakis, Petros Drettas
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.