
Abstract
Trauma to a transplanted organ is rare, but clinicians increasingly confront this scenario with the rise in transplantations. Renal trauma requires multidisciplinary treatment, and guidelines are necessary for standardizing medical care. However, there are no diagnostic and treatment protocols for traumatic renal injury in transplanted kidneys. This review aims to consolidate current knowledge on the interdisciplinary approach to managing injuries of transplanted kidneys, with a focus on blunt trauma to the abdomen and pelvis. Transplanted kidneys, typically placed in the iliac fossa in a heterotopic, extraperitoneal position are more exposed to direct trauma, particularly in motor vehicle accidents. In the emergency setting, the initial imaging is often an Ultrasound scan. This bedside ultrasound helps identify free fluid in the abdomen, indicating possible bleeding and guiding the need for surgical intervention. However, Ultrasound scan is operator-dependent and has limited sensitivity for low-grade renal trauma. Hemodynamically stable patients, or those who stabilize with resuscitative efforts, should undergo contrast-enhanced CT or MRI for a more accurate assessment. Therapeutic strategies may include conservative management, radiological interventions such as angioembolization, or surgical exploration, depending on hemodynamic stability, the severity of injury, and the degree of graft dysfunction. Surgical intervention is reserved for patients who are hemodynamically unstable despite resuscitative efforts or who fail conservative treatment. Management of renal trauma in this population of patients requires a multidisciplinary approach involving transplant surgeons, nephrologists, interventional radiologists, and trauma specialists. Prospective and multicenter studies are lacking, and further research is warranted to compare outcomes of operative, non-operative, and interventional radiologic approaches in high-grade injuries (grades IV and V), and establish criteria for follow-up imaging in renal trauma.
Introduction
Renal trauma may involve damage to either the renal parenchyma or vascular structures, leading to hemorrhage, or may affect the collecting system, potentially causing urinary leakage. Renal trauma is observed in about 1%–5% of trauma cases, with the vast majority (80%–90%) resulting from blunt abdominal mechanisms. 1 Currently, clinical guidelines for the management of trauma involving transplanted kidneys remain limited. While various case reports have documented such injuries (Table 1), standardized protocols are lacking.2–12 Prompt evaluation by an urologist is crucial to coordinate appropriate multidisciplinary management, and nephrology consultation is important when acute kidney impairment is a concern. Serious complications, such as intraperitoneal rupture, may result in urinary peritonitis and compromise pelvic integrity, while bone fragments from associated fractures can damage surrounding soft tissues and trigger inflammatory reactions. 4 Early diagnostic assessment and specialized treatment are key to enhancing patient outcomes and minimizing complications. 12 This narrative review aims to consolidate current knowledge on the interdisciplinary approach to managing injuries of transplanted kidneys, with a focus on blunt trauma to the abdomen and pelvis.
Management of patients with traumatic injury to the transplanted kidney.
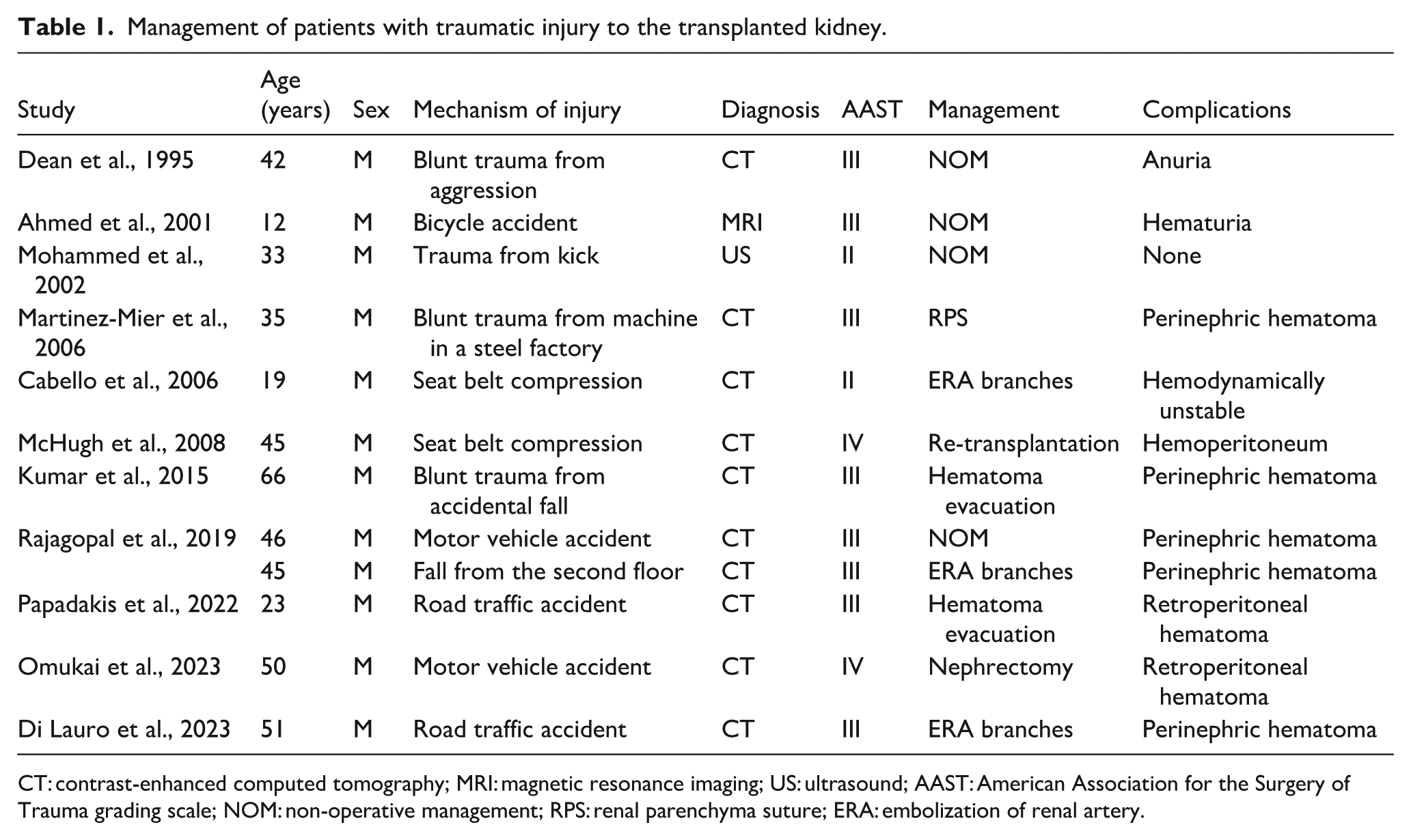
CT: contrast-enhanced computed tomography; MRI: magnetic resonance imaging; US: ultrasound; AAST: American Association for the Surgery of Trauma grading scale; NOM: non-operative management; RPS: renal parenchyma suture; ERA: embolization of renal artery.
Methods
Data sources and search strategy
On September 2025, a comprehensive search of medical literature databases was conducted using the following keywords: “renal trauma,” “kidney trauma,” “blunt renal trauma,” “renal transplantation,” “kidney” or “transplant,” and “management.” The databases consulted included Medline, Web of Science, PubMed, and Google Scholar (Figure 1). The aim was to identify relevant studies containing patient data and information suitable for inclusion in this review.
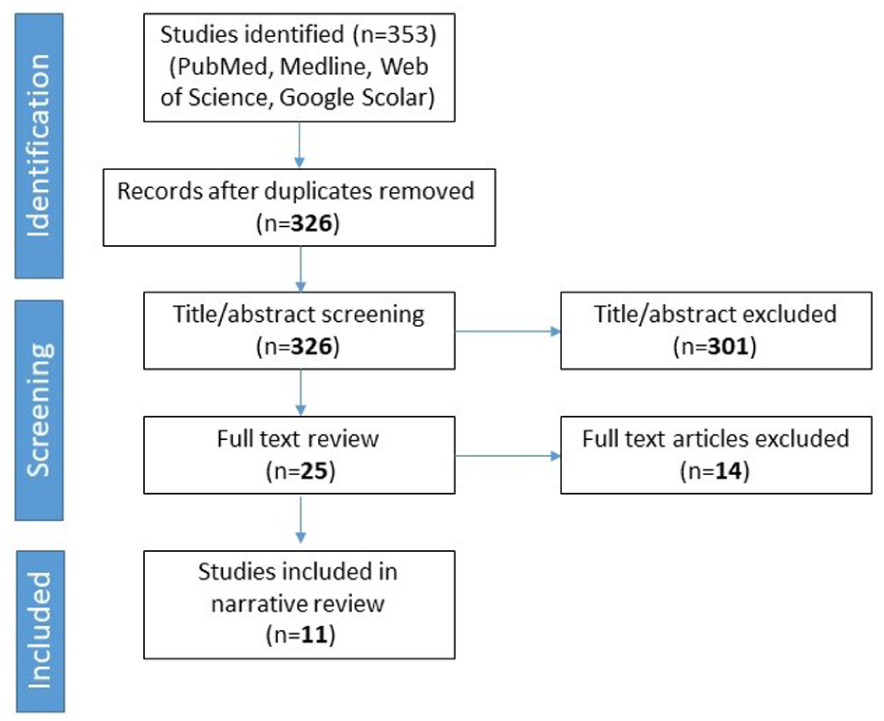
Study flow chart.
Study selection criteria
Eligible studies were limited to original research involving human subjects, encompassing both prospective and retrospective observational designs. Studies were excluded if they involved non-human subjects, focused on cancer, or reported iatrogenic injuries. The screening and selection process was overseen by the lead author (LD). One international research fellow (IRF) independently extracted a first dataset, which was subsequently reviewed by LD. Conversely, LD extracted a second dataset, which was then verified by IRF. Data extraction was carried out using a structured table that captured the following information: author, year of publication, patient count, age, sex, trauma mechanism, injury grading according to the American Association for the Surgery of Trauma (AAST) Organ Injury Scale, diagnostic modality for kidney injury, and therapeutic approach (Table 1).
Statistical analysis
Given the limited sample size and descriptive nature of available data, no formal meta-analysis was performed. Descriptive statistics were used to summarize case characteristics, including patient demographics, injury mechanism and severity, treatment strategy, and outcomes. The findings are presented qualitatively to inform clinical practice and guide future research directions.
Results
Incidence
Trauma to a transplanted organ is rare, but clinicians increasingly confront this scenario with the rise in transplantations. Renal injuries represent approximately 1%–5% of all trauma cases, with blunt abdominal trauma accounting for 80%–90% of these. Among patients experiencing blunt abdominal trauma, renal involvement occurs in 8%–10% of cases, while in penetrating trauma, the incidence is around 6%.1,12 About 10% of abdominopelvic traumas involve injury to the urological organs. Ureter injuries are rare (2%); of these, one-third are caused by blunt trauma, usually from traffic accidents with extreme deceleration as well as hyperextension and hyperlordosis, and usually affect the upper ureter. 13 Young males, particularly those involved in high-risk activities such as contact sports, road traffic accidents, assaults, or falls, are disproportionately affected, with an average age around 30 years. In the context of transplantation, kidneys are typically implanted in a heterotopic extraperitoneal location, most often in the iliac fossa. 13 This anatomical position makes them especially susceptible to injury from external forces such as seat belts during vehicular collisions. Trauma to a transplanted kidney occurs in pelvic contusions or blunt-object force trauma in the lower abdomen, with blunt renal injuries being associated with pelvic fractures in 60%–90% of cases, and with other intra-abdominal injuries in 44%–68% of cases. A kidney transplant injury is associated with an urether injury in 1% of cases.12,13
Mechanism of injury
The majority of blunt renal injuries to native kidneys are caused by road traffic collisions. In such scenarios, the transfer of kinetic energy leads to compression of the abdomen against restraints such as seat belts or steering wheels, resulting in trauma to abdominal organs. 14 Native kidneys are relatively protected due to the ribcage and surrounding musculature. In contrast, transplanted kidneys, typically placed in the iliac fossa in a heterotopic, extraperitoneal position are more exposed to direct trauma, particularly in motor vehicle accidents. Even in transplant patients, blunt renal trauma is more common than penetrating renal trauma. The causes of blunt renal trauma in order of frequency are: motor vehicle accidents, falls, sports injuries and pedestrian struck injuries. 12
Injury classification
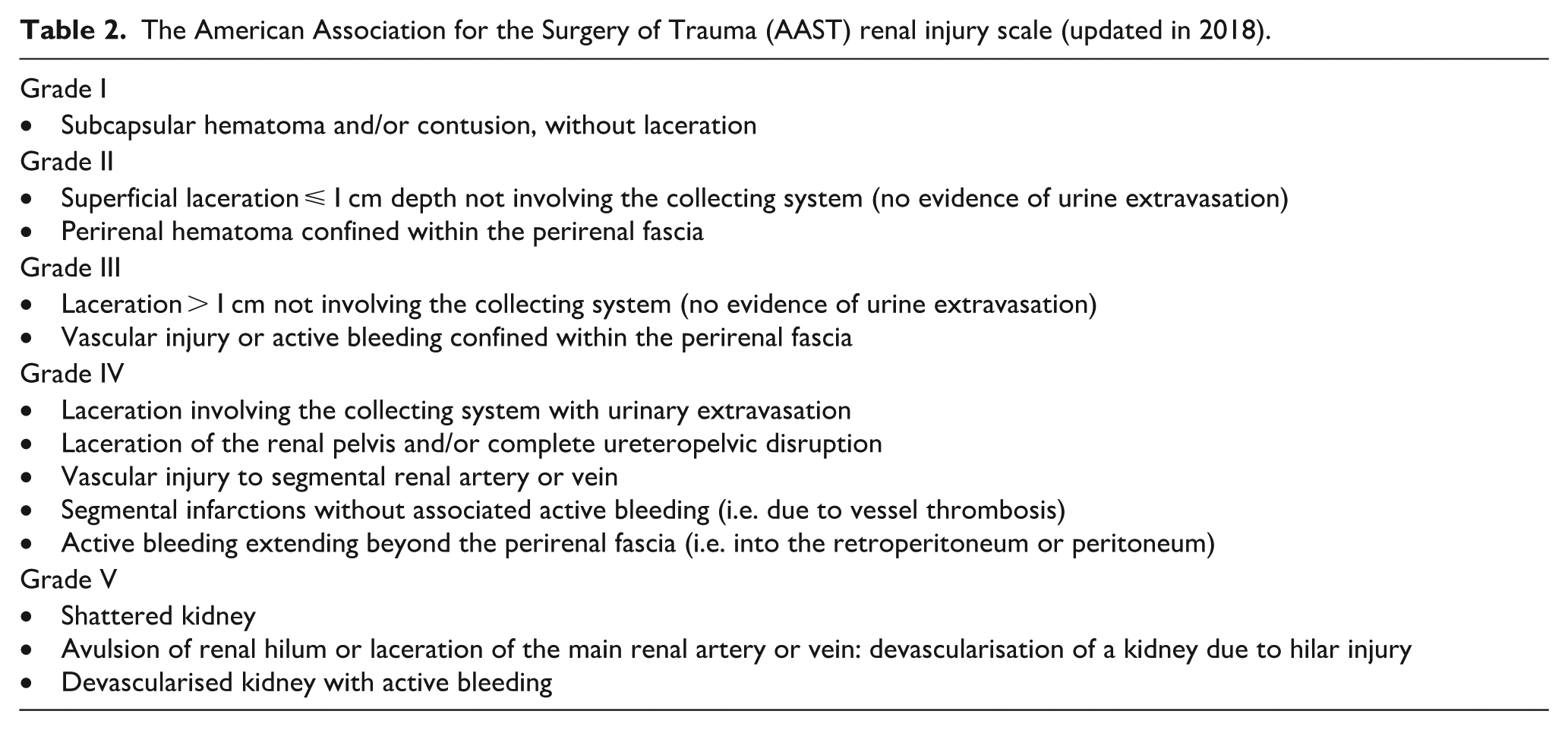
The American Association for the Surgery of Trauma (AAST) grading system remains the most widely accepted classification method for renal trauma. This scale is applied using findings from contrast-enhanced computed tomography (CT), which serves as the diagnostic gold standard for assessing renal injuries (Table 2). 15
The American Association for the Surgery of Trauma (AAST) renal injury scale (updated in 2018).
General management
In the assessment of blunt abdominopelvic trauma, it is crucial to gather a detailed history of the incident, document symptoms in a targeted manner, and perform a thorough initial clinical evaluation. These steps are essential in guiding the prioritization of specialized interventions. Key indicators of potential injuries to the urinary tract include contusions, hematomas, skin abrasions, and swelling in the abdominal, pelvic, perineal, flank, or lumbar regions, as well as pain localized to these areas.13,16 Additional concerning signs include involuntary guarding, signs of an acute abdomen, visible hematuria, urethral bleeding, urinary urgency, and retention. Importantly, the absence of external findings does not rule out significant urological trauma. The insertion of a transurethral bladder catheter is frequently described in the literature as part of the initial management protocol in emergency settings, offering diagnostic and therapeutic benefits, particularly in patients with kidney transplants and suspected urotrauma. 14 In cases involving pelvic ring fractures, injuries to the urethra or bladder are relatively common, reported in up to 70% of cases, and must be actively ruled out. The lack of urethral bleeding or normal appearance of the perineal and anal regions should not be considered definitive evidence of an uninjured lower urinary tract. 17 The presence of gross hematuria or urethral bleeding following catheter insertion, especially when the anatomical status is not clearly defined, should raise suspicion for iatrogenic injury. In such scenarios, it is generally advisable to defer catheterization until primary imaging has excluded a lower urinary tract lesion. 18
Diagnosis
For suspected renal trauma, multiphasic contrast-enhanced CT imaging is the preferred diagnostic tool, as it allows thorough evaluation of the renal parenchyma, vasculature, and collecting system. The use of different contrast phases improves the ability to distinguish between active bleeding and urinary extravasation. 19 CT scans effectively replicate the injury patterns that would be observed during surgical exploration, offering detailed insight into both the extent and nature of the trauma. In the emergency setting, the initial imaging is often a Focused Assessment with Sonography for Trauma (FAST) exam. This bedside ultrasound helps identify free fluid in the abdomen, indicating possible internal bleeding and guiding the need for surgical intervention. 20 However, FAST is operator-dependent and has limited sensitivity for retroperitoneal bleeding and low-grade renal trauma. Hemodynamically stable patients, or those who stabilize with resuscitative efforts, should undergo contrast-enhanced CT for a more accurate assessment. Importantly, a negative scan does not fully exclude renal injury, and further workup should be guided by the patient’s evolving clinical status. 21 In cases of hemodynamic instability requiring immediate surgery, intraoperative intravenous urography may be used to evaluate the function of the contralateral kidney, which can influence intraoperative decision-making. MRI (Magnetic Resonance Imaging) represents a powerful, non-invasive imaging modality for assessing the structure and function of transplanted kidneys. 22 Its superior soft tissue contrast and capacity for functional imaging make it particularly useful for identifying post-transplant complications such as rejection, vascular abnormalities, or obstruction. MRI techniques, such as diffusion-weighted imaging (DWI) and blood oxygen level-dependent (BOLD) imaging, allow for the assessment of renal microstructure, perfusion, oxygenation, and potential parenchymal injury. MRI is effective in identifying perinephric fluid collections, which may suggest hematoma, lymphocele, or urinoma formation. 23
Advantages of MRI in Transplant Imaging:
Non-invasive nature: MRI does not involve ionizing radiation or intra-arterial contrast, minimizing patient risk.
Superior soft tissue resolution: It offers enhanced visualization of renal parenchyma and surrounding structures.
Functional insight: MRI can provide critical information on renal perfusion and oxygenation, complementing anatomical assessment.
Use of safe contrast agents: Gadolinium-based contrast agents, typically non-nephrotoxic, are generally considered safe even in patients with impaired kidney function.
However, MRI is relatively costly and may not always be the most accessible imaging choice. Furthermore, the diagnostic accuracy of certain MRI techniques can vary, and in some clinical scenarios, alternatives such as ultrasound or CT may be more appropriate depending on the specific diagnostic question. 22
Non-operative management (NOM)
There is general agreement among trauma and urology experts that hemodynamically stable patients benefit most from an initial non-operative approach. 15 The success of this strategy has been significantly enhanced by improvements in diagnostic imaging, which aid in accurate injury grading, and by the advent of effective angioembolization techniques. Early management typically includes Intensive Care Unit (ICU) admission for close monitoring, serial physical assessments, frequent hematocrit checks (every 6–8 h), transfusion support, and intervention for complications such as urinary leakage when necessary.11,14 This conservative approach helps preserve renal function and reduces the rate of unnecessary nephrectomies of transplanted kidneys. As patients stabilize, laboratory monitoring can be spaced out, and care can be transitioned from the ICU to the general ward or even outpatient follow-up. For high-grade injuries (AAST grades III) managed conservatively, a repeat contrast-enhanced CT is advised within 48–72 h, or sooner if clinically indicated, to detect delayed complications such as bleeding or urinoma formation. 21
The present systematic review of the available case literature identified 12 reported cases of traumatic allograft injury, of which seven were classified as AAST Grade III (Table 1), the predominant severity level in this series. The management strategies applied to these cases, along with the associated clinical outcomes, provide a unique opportunity to examine the role of NOM in this specific population and to identify factors associated with NOM failure and graft loss. Among the seven Grade III allograft injuries identified in this review, NOM was adopted in three cases (43%), represented by the series of Dean et al., 2 Ahmed et al., 3 and Rajagopal et al. 9 This proportion is notably lower than the NOM success rates reported for Grade III native kidney injuries in the general population, which range between 70% and 90% in contemporary series, 12 underscoring the higher complexity and lower tolerance for conservative management inherent to the transplant setting. The cases of Ahmed et al. 3 and Rajagopal et al. 9 document relatively self-limiting complications (hematuria and perinephric hematoma, respectively) consistent with successful NOM in hemodynamically stable patients with contained injuries. In contrast, the case reported by Dean et al. 2 stands out for the development of post-traumatic anuria, a clinical sign that suggests significant vascular compromise, ureteral disruption, or mass effect from subcapsular hematoma. This complication, managed without operative intervention, raises concern for either delayed graft dysfunction or undetected graft loss, and illustrates the inherent risks of NOM in the absence of close surveillance and clearly defined escalation criteria.
Several clinical and radiological factors emerged from the analysis of this case series as potential predictors of NOM failure and graft loss in allograft trauma:
Anuria and acute graft dysfunction: The development of anuria following allograft trauma, as observed in the case by Dean et al., 2 should be regarded as a critical warning sign and a likely indicator of NOM failure. In the transplanted kidney, ischemic injury from vascular pedicle compromise or extrinsic compression by hematoma can rapidly escalate to irreversible graft loss. Unlike native kidney trauma, where the contralateral kidney provides functional reserve, the transplant recipient has no such safety margin. Prompt cross-sectional imaging reassessment and low threshold for angiographic intervention are therefore mandatory in this context.
Perinephric and retroperitoneal hematoma: Perinephric hematoma was documented in three of the seven Grade III cases (Kumar et al. 8 ; Rajagopal et al. 9 ; Di Lauro et al. 12 ). While a stable, contained hematoma may be amenable to NOM with close monitoring, expansion, particularly in the presence of active contrast extravasation on CT, constitutes a standard indication for intervention. Of the three Grade III cases with perinephric hematoma, two ultimately required procedural management (hematoma evacuation and embolization, respectively), consistent with the broader literature on native kidney trauma, in which hematoma volume and CT evidence of active bleeding are well-established predictors of NOM failure.8,9
High-energy mechanisms: Motor vehicle accidents, workplace machinery trauma, and falls from height were the most frequent mechanisms associated with Grade III–IV injuries in this series.5,9–12 High-energy transfer mechanisms are associated with a greater likelihood of concurrent vascular injury, urinary extravasation, and multi-organ trauma, all of which individually increase the probability of NOM failure. This is consistent with data from the native kidney trauma literature and should inform the initial risk stratification of allograft trauma patients.
Angiographic embolization
Acute kidney dysfunction represents a relevant complication after trauma in kidney transplant patients, often impacting both clinical management and prognosis.12,24 Recent evidence suggests that trauma-related acute kidney injury (AKI) in transplant kidney occurs in approximately 30%–40% of patients admitted to ICU. The pathogenesis of post-traumatic AKI is typically multifactorial, with hypovolemic shock secondary to hemorrhage being a leading contributor due to compromised renal perfusion. Clinically, patients with suspected shock may present with tachycardia, hypotension, altered mental status ranging from drowsiness to unconsciousness, and signs of peripheral vasoconstriction such as pallor or mottled skin. Tachypnea is commonly observed and may reflect pain, metabolic acidosis, or a compensatory response to elevated lactate levels. Additionally, early signs such as oliguria or anuria and hypothermia can indicate the onset of shock-related renal impairment. Prompt evaluation of renal function in trauma patients is essential to identify potentially reversible contributors to AKI. 20 During the first 24 h, renal dysfunction may remain clinically silent or present only with subtle signs. In cases of reduced urine output, extrinsic causes such as urinary tract obstruction or bladder extravasation should be excluded. The presence of dark, concentrated urine in the absence of visible hematuria may point toward hypovolemia or suggest myoglobinuria associated with crush syndrome and severe rhabdomyolysis. Selective angiographic embolization has transformed the treatment of renal hemorrhage, boasting success rates of up to 88% in controlling bleeding and renal salvage rates as high as 90%. 25 Liguori et al. reported that renal angioembolization is an effective and minimally invasive treatment for grade III–IV blunt renal trauma, whereas outcomes are less favorable in grade V injuries, with higher failure rates. 26 This procedure, typically performed by an interventional radiologist, is contingent on immediate availability of specialized personnel and infrastructure. If not locally available, stable patients should be transferred to a facility where the service can be provided. Compared to surgery, embolization is associated with better renal preservation and lower morbidity, and is therefore preferred in eligible patients (Figure 2).27,28
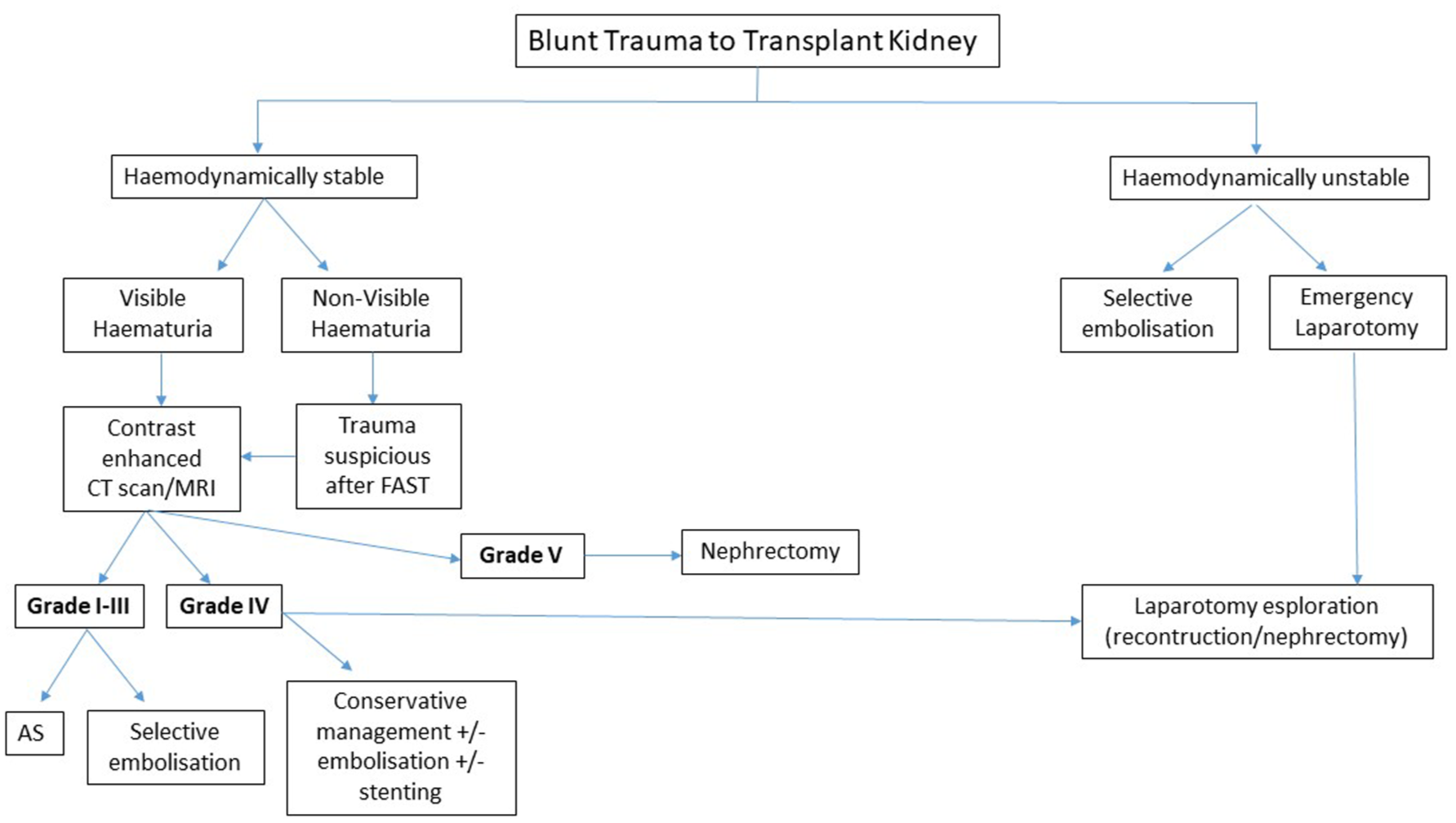
Management of blunt trauma injury to transplant kidney recipients.
Operative management
Surgical intervention is reserved for patients who are hemodynamically unstable despite resuscitative efforts or who fail conservative treatment. Indications for surgery include ongoing hemorrhage requiring repeated transfusions, persistent or worsening urinary extravasation, and severe injuries such as renal pelvis or proximal ureteral avulsion. 28 The primary objective during surgery is hemorrhage control and, when feasible, renal preservation. Surgical intervention does not always necessitate total nephrectomy. In select cases, minor parenchymal or collecting system injuries can be repaired primarily, and partial nephrectomy may be appropriate when sufficient viable renal tissue remains. 29 Surgical intervention is associated with high complication rate, however failure to act may result in loss of graft. Renorrhaphy or partial nephrectomy entails wide exposure of the kidney, excision of nonviable tissue, ligation of bleeding vessels, watertight repair of any collecting system disruption using slowly absorbable sutures, and reconstruction of parenchymal defects, often utilizing the renal capsule. Polar lesions can be amputated while lacerations to the middle of the kidney require renorrhaphy. The collecting system should be closed in a water tight fashion with a slowly absorbable suture. Defects in the renal parenchyma may be closed primarily in many cases with renal capsule. 30 Successful preservation of functioning renal tissue is possible in most renal lacerations requiring exploration, although injury severity, renovascular trauma and associated injuries may compromise the function of the affected renal unit. The nephrectomy rate for immediate exploration of major renal lacerations varies considerably, depending on the type and severity of the trauma, but in clinically unstable patients with major renal injury it may reach 100%. 31 Penetrating mechanism, high-velocity weapons and overall injury severity of the patient are associated with a higher nephrectomy rate. Surgical repair of vascular injuries to the kidney requires specific surgical expertise and a degree of hemodynamic stability. Nephrectomy is still the most expeditious method of managing renal vascular injuries, and whereas renal artery repair is rarely possible and seldom successful, renal vein injuries carry a better prognosis. 32
Complications
Active hemorrhage is a critical complication of traumatic renal injury that plays a central role in determining the urgency and nature of acute management. Although more frequently associated with high-grade injuries (AAST grades IV and V), it can also occur in moderate injuries (grades II and III). Delayed bleeding, typically presenting 2–3 weeks post-injury, is often attributed to vascular abnormalities such as arteriovenous malformations or pseudoaneurysms complications that are more common in high-grade trauma and penetrating injuries.29,32 While active bleeding demands prompt intervention due to its hemodynamic implications, urinary extravasation is a more frequent finding, observed in approximately 7% of renal trauma cases. Encapsulated collections of urine, or urinomas, usually form in the subcapsular space and are often self-limiting. However, persistent or infected urinomas may necessitate percutaneous or surgical drainage. 33 Additional delayed sequelae include hydronephrosis, chronic pyelonephritis, and postrenal hypertension. In terms of management outcomes, non-operative treatment of high-grade trauma in transplant kidney is commonly followed by complications such as hematuria, fever, acute kidney injury, and urinoma formation. In contrast, operative management tends to be associated with risks including wound infection, perinephric abscess, and urinary tract infections. 34
The impact of immunosuppression on diagnosis, complications, and graft survival
Beyond the anatomical peculiarities of allograft positioning, the immunosuppressed status of the renal transplant recipient represents arguably the single most critical factor differentiating allograft trauma from native kidney trauma. Chronic immunosuppression, typically comprising a calcineurin inhibitor (tacrolimus or cyclosporine), an antiproliferative agent (mycophenolate mofetil or azathioprine), and low-dose corticosteroids, fundamentally alters the host response to injury at multiple levels, with direct consequences for diagnostic accuracy, post-traumatic and post-operative complication rates, and long-term graft survival. These implications deserve dedicated consideration in the clinical management of any renal transplant recipient presenting with abdominal or pelvic trauma. 35
(a) Implications for diagnosis: blunting of the inflammatory response
One of the most clinically insidious consequences of long-term immunosuppression is the attenuation of the systemic inflammatory response to injury and infection. Corticosteroids suppress the hypothalamic-pituitary axis and blunt the febrile response, while calcineurin inhibitors and antiproliferative agents impair leukocyte activation and cytokine signaling. As a result, classical clinical indicators of injury severity (fever, leukocytosis, peritoneal irritation, and localized pain) may be markedly diminished or entirely absent in the immunocompromised host, even in the setting of significant intra-abdominal pathology.35,36 In the context of allograft trauma, this diagnostic blunting carries specific risks. Perinephric hematoma or urinoma formation may progress silently without the localized inflammatory signs that would typically prompt early reassessment in immunocompetent patients. Similarly, the early stages of septic complications—wound infection, abscess, or infected hematoma, may not generate the expected clinical picture, leading to delayed recognition and treatment. 37 For these reasons, a low threshold for cross-sectional imaging and laboratory reassessment is mandatory in the transplant trauma patient, irrespective of the apparent clinical stability, and serial monitoring should be maintained beyond the timeframe routinely applied to non-immunocompromised individuals. Furthermore, the denervated nature of the allograft itself eliminates the afferent pain signals that would normally direct clinical attention to the injured organ. The absence of graft-site tenderness following trauma should therefore never be interpreted as reassuring, and the clinical assessment must rely primarily on objective imaging and functional parameters, in particular, graft Doppler ultrasonography and contrast-enhanced CT, rather than on symptomatology alone.35,37
(b) Implications for complications: infection, abscess, and sepsis
The immunosuppressed state substantially increases the risk of infective complications following both the traumatic injury itself and any subsequent surgical intervention. It has been estimated that approximately 70% of kidney transplant recipients experience at least one infectious episode within the first 3 years post-transplant, 38 and infection represents the second leading cause of death in recipients with functioning allografts, after cardiovascular disease. 37 In the transplant population, impaired innate and adaptive immunity reduces the capacity to contain bacterial contamination and mount an effective response to opportunistic pathogens, with the net state of immunosuppression representing the key determinant of individual infectious risk. 39 Post-traumatic perinephric hematoma and urinoma, both documented complications in the cases reviewed in the present series, represent fertile substrates for secondary infection in the immunocompromised host. Infected perinephric collections may progress rapidly to frank abscess formation or systemic sepsis, with potentially fatal consequences. The risk is further compounded by the frequent co-administration of high-dose corticosteroids as part of standard immunosuppressive regimens, which additionally impair wound healing and tissue repair following surgical drainage or exploration. A prospective observational study demonstrated that sepsis in renal allograft recipients is independently associated with a more than fifteen-fold increase in the risk of graft loss at 1 year compared to non-septic controls with similar clinical profiles. 40 These considerations have direct implications for management strategy. In the transplant trauma patient, the decision to proceed with operative intervention must weigh not only the hemodynamic and renal functional indications, but also the heightened infectious risk inherent to surgical exploration in an immunocompromised field. Antimicrobial prophylaxis and, where clinically indicated, empirical broad-spectrum antibiotic therapy should be implemented at an early stage in any transplant trauma patient undergoing invasive procedures. Microbiological surveillance of peri-graft collections is equally essential, given the susceptibility of these patients to resistant organisms and fungal pathogens that would be unlikely to cause significant disease in immunocompetent hosts.35,37
(c) Implications for graft survival: trauma-induced acute rejection
A largely underappreciated risk in the transplant trauma setting is the potential for trauma-induced acute allograft rejection. Although this relationship remains incompletely characterized in the literature, a plausible immunological mechanism has been proposed: major trauma and haemorrhagic shock trigger a systemic inflammatory response, including the release of damage-associated molecular patterns (DAMPs) and pro-inflammatory cytokines, which may act as a “danger signal” capable of activating alloreactive T-cell responses and disrupting the immunological tolerance that underpins stable graft function.41,42 Accumulating experimental and clinical evidence has established that DAMPs, released following ischemia-reperfusion injury and cellular stress, signal through innate pattern recognition receptors and directly promote the alloimmune response across all commonly transplanted solid organs. 41 Large-volume fluid resuscitation, blood product transfusion, and surgical stress, all common components of the management of major allograft trauma, may further perturb the immunological equilibrium of the recipient. Allogeneic blood transfusions in particular carry the theoretical risk of allosensitisation, with consequent elevation of panel-reactive antibody (PRA) levels and increased susceptibility to antibody-mediated rejection. 43 This risk is especially relevant in recipients who have already been sensitized by prior transplants, pregnancies, or transfusions. From a pharmacokinetic perspective, it is also important to recognize that major trauma and critical illness may significantly alter the absorption, distribution, and metabolism of immunosuppressive agents. Hemodynamic instability markedly impairs intestinal motility and reduces P-glycoprotein expression in the gut wall, leading to unpredictable fluctuations in tacrolimus bioavailability, with surges in whole-blood trough concentrations of up to 100% upon hemodynamic recovery, while abrupt troughs occur during periods of circulatory compromise. 44 More broadly, the pharmacokinetic derangements characteristic of critical illness, including altered protein binding, increased volume of distribution, impaired hepatic metabolism, and fluctuating renal clearance, affect all major immunosuppressive drug classes. 45 These changes may generate periods of relative under-immunosuppression that precipitate acute rejection episodes, while nephrotoxic calcineurin inhibitors may simultaneously exacerbate ischemic allograft injury, creating a compounding therapeutic dilemma. In light of these considerations, all transplant recipients sustaining significant allograft trauma should undergo close nephrological monitoring in the post-acute phase, including regular measurement of serum creatinine, tacrolimus/cyclosporine trough levels, and urinalysis. A clinically significant rise in creatinine, whether attributable to direct traumatic injury, ischemia-reperfusion, or immune-mediated injury, should prompt early allograft biopsy to guide appropriate management, tissue biopsy being the established gold standard for diagnosing acute rejection in the transplant recipient.46,47
Conclusions and future directions
Several important limitations must be acknowledged. The rarity of transplanted kidney trauma has precluded the development of prospective studies or randomized controlled trials, and the available evidence is restricted to case reports and small series with significant heterogeneity in reporting standards, follow-up duration, and outcome definitions. The absence of long-term functional outcomes—including graft survival, serum creatinine trajectories, and return to dialysis rates—in most reports makes it impossible to assess the true success rate of NOM beyond the immediate perioperative period. Renal trauma requires multidisciplinary treatment, and guidelines are necessary for standardizing medical care. However, there are no diagnostic and treatment protocols for traumatic renal injury in transplanted kidneys. With the growing number of renal transplant procedures, there is an increasing likelihood of encountering trauma involving renal allografts. Although the American Association for the Surgery of Trauma grading system is widely applied to native kidney injuries, it has not been specifically validated in transplant recipients. Management of renal trauma in this population requires a multidisciplinary approach involving transplant surgeons, nephrologists, interventional radiologists, and trauma specialists. Close monitoring of both the patient and the graft is essential, with serial assessments, preferably including FAST, conducted in specialized transplant units when feasible. Therapeutic strategies may include conservative management, radiological interventions such as angioembolization, or surgical exploration, depending on hemodynamic stability, the severity of injury, and the degree of graft dysfunction (Table 3). There is a pressing need for future studies aimed at establishing validated protocols and trauma grading systems tailored to renal transplant recipients, as current frameworks do not account for the unique anatomical and functional characteristics of the allograft. The evolution of renal trauma management toward a nephron-sparing paradigm reflects broader interdisciplinary collaboration and technological advancements. However, significant gaps in evidence remain. Prospective and multicenter studies are lacking, and further research is warranted to refine the AAST classification, clarify imaging indications in pediatric populations with hematuria following blunt trauma, compare outcomes of operative, non-operative, and interventional radiologic approaches in high-grade injuries (grades IV and V), and establish criteria for follow-up imaging in renal trauma.
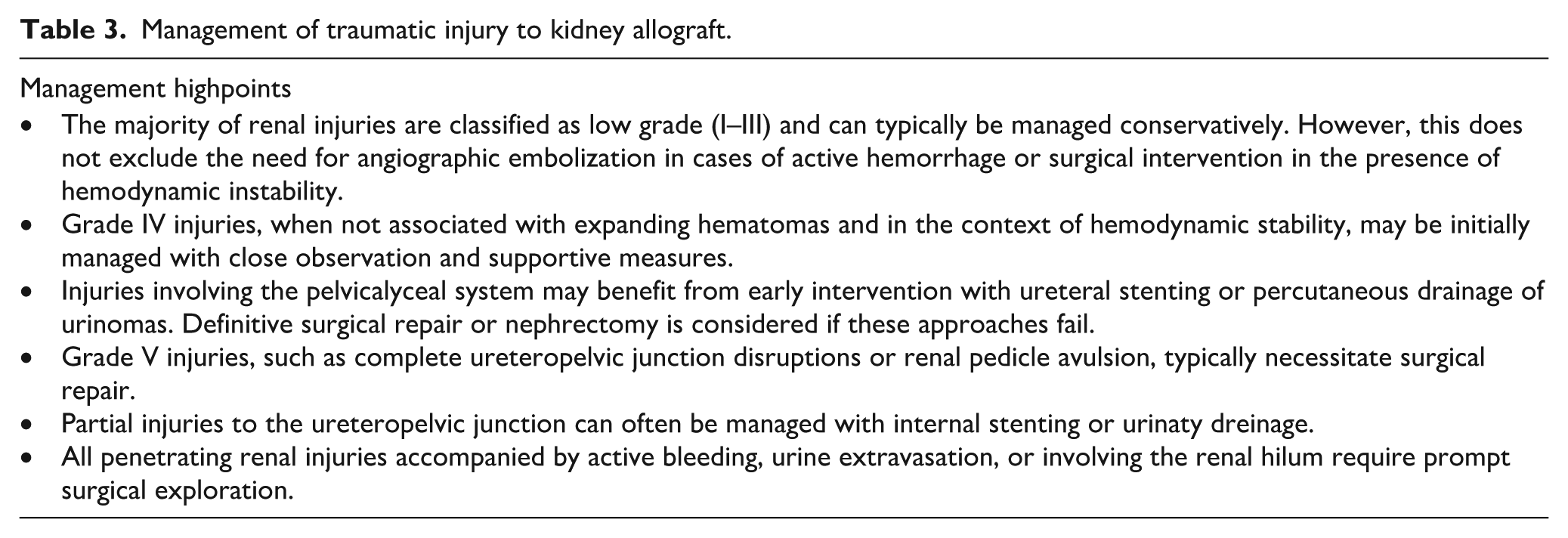
Management of traumatic injury to kidney allograft.
Footnotes
Ethical considerations
Ethical approval was deemed not to be required given all data is available to the public and is anonymized.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.*