
Abstract
Background:
Bacterial biofilms play a key role in antibiotic resistance, infection recurrence, and reduced pathogen detection in prostatic secretion. Bovhyaluronidase azoximer is a biofilm-disrupting agent. This trial aimed to evaluate its effects on biofilms and clinical outcomes in patients with chronic prostatitis and associated infertility.
Methods:
Patients with chronic bacterial prostatitis and infertility completed the NIH-CPSI, IPSS, and QoL questionnaires, underwent microbiological culture of prostatic secretion, ejaculate, or the third portion of urine, light and electron microscopy of ejaculate before and after treatment. Patients were randomized into two groups treated with antibiotics combined with bovhyaluronidase azoximer, and antibiotics alone.
Results:
The experimental group showed greater improvements on the NIH-CPSI scale (MD −3.04, 95%CI: −3.77 to −2.3, p < 0.001). Significant reduction in bacterial colony count and neutrophil levels were detected in the experimental group. Ejaculate clearance from neutrophils and bacteria was more frequent in experimental group (41% vs 7.2%, p = 0.01; 41.7% vs 12.1%, p = 0.043). Electron microscopy revealed disappearance of the intercellular matrix of bacterial microcolonies only in the experimental group. Recurrence rates were significantly lower at both 6 months and 12 months in the experimental group.
Conclusions:
The combined use of bovhyaluronidase azoximer with antibiotics significantly improved symptoms, reduced leukocyte and bacterial counts, and lowered recurrence rates in patients with chronic prostatitis. Post-treatment microscopy confirmed the disruption of biofilm structures, suggesting enhanced microbial clearance.
Introduction
For a long while, it was believed that chronic abacterial prostatitis is unrelated to bacterial infection. However, recent studies have challenged this view. Advances in modified urine culture protocols 1 and DNA sequencing techniques 2 have enabled the detection of microflora in cases where conventional urine cultures are negative and have identified anaerobic organisms that do not grow on standard microbiological media. Furthermore, the fact that a significant proportion of patients diagnosed with abacterial prostatitis respond to antibiotic therapy 3 suggests that the role of bacteria in this condition may have been underestimated. Collectively, these findings point to a more substantial role of bacteria in chronic prostatitis than previously recognized.
Bacteria are frequently detected in sperm samples—often even more so than in urine. While some researchers interpret these findings as contamination, 4 growing evidence suggests that bacteria can negatively impact sperm quality, particularly morphology and concentration. 5 Bacteria contribute to persistent infections by forming biofilms—structured communities that enhance resistance to antibiotics and help pathogens evade immune responses. 6 Alarmingly, chronic infection can also contribute to infertility in up to 60% of cases, 7 although the prevalence of this factor remains debated. 8
This is particularly relevant in chronic prostatitis, considering the heterogeneous nature and complex pathogenesis of the condition. As a result, a variety of treatment strategies have been proposed. Nevertheless, patients often face suboptimal therapeutic outcomes and frequent relapses, with symptomatic therapy remaining a common approach in clinical practice. 9
Targeting biofilms pharmacologically may help prevent both recurrence of chronic prostatitis and its detrimental effects on fertility. A clinical trial has indirectly demonstrated that bovhyaluronidase azoximer can disrupt bacterial biofilms in chronic prostatitis. 10 Moreover, in vitro studies have confirmed its efficacy in breaking down Candida albicans biofilms and mixed fungal-bacterial biofilms. 11 We hypothesize that bovhyaluronidase azoximer may enhance the effectiveness of antibiotic therapy and improve clinical outcomes in patients with chronic prostatitis. The aim of this clinical trial is to evaluate the impact of bovhyaluronidase azoximer on biofilms and treatment efficacy in patients with chronic prostatitis and associated infertility.
Materials and methods
After obtaining IRB approval (protocol №152, June 14, 2022), a randomized controlled open-label trial was conducted to recruit patients with clinical signs of chronic bacterial prostatitis (confirmed by complaints, history, physical examination, and laboratory tests) and complaints of infertility (failure to achieve pregnancy within 12 months). All patients completed the NIH-CPSI, IPSS, and QoL questionnaires independently, without physician involvement, in accordance with Good Clinical Practice (GCP) guidelines. A physical examination, including a digital rectal examination (DRE), was also performed.
Subsequently, patients underwent a cultural study of prostate secretion, ejaculate, or the third portion of urine, in accordance with the Meares and Stamey method. 12 The specimens were cultured on blood agar and MacConkey agar quantitatively using 10 µl calibrated loops, incubated aerobically at 37°C for at least 72 h. Significant growth was defined as ⩾ 105 CFU/mL. Additionally, real-time polymerase chain reaction (RT-PCR) of the ejaculate was performed to rule out a standard panel of sexually transmitted infections. The concentration, motility of spermatozoa, and the number of leukocytes in the ejaculate were determined using light-optical microscopy. The presence of biofilms in the ejaculate, as well as the anatomical and functional state of spermatozoa, were assessed using electron microscopy. During microscopy, the number of bacterial colonies and neutrophilic leukocytes was counted in the area occupied by 100 spermatozoa.
To eliminate the possibility of scrotal pathology as a contributing factor to impaired fertility, all patients underwent ultrasound examination of the scrotal organs. Exclusion criteria were: pathology of scrotal organs identified by ultrasound that could affect fertility (such as varicocele, testicular hypoplasia, cryptorchidism, etc.), presence of sexually transmitted infections, a history of radiotherapy or systemic chemotherapy, and aspermia.
Patients meeting the eligibility criteria were then randomized 1:1 using an online service «Study randomizer» with permuted block randomization. They were assigned to either the control group, which received antibacterial therapy based on culture results (fluoroquinolones, tetracyclines, macrolides for 4–6 weeks), or the experimental group, which received the same antibacterial therapy in addition to Bovhyaluronidase azoximer (3000 IU i.m. for 12 weeks). No blinding was conducted.
After the 12-week treatment period, a follow-up visit was conducted, involving a comparable examination, assessment of patient compliance, evaluation of the efficacy of concomitant therapy, and collection of adverse event data. Further follow-up visits were scheduled at 3- and 6-month intervals. During these visits, a questionnaire was administered to detect disease recurrence, and any adverse events were recorded.
The primary endpoint was disease recurrence rate within 6 months after treatment. Secondary endpoints included subjective (NIH-CPSI total score and its domains, IPSS and QoL questionnaire scores changes) and objective (changes in microscopic examination results, incidence and grading of adverse events, and complication rates) outcomes at pre-defined follow-ups (at the end of 12-week treatment, after 3 and 6 months).
Statistical analysis was conducted using R version 4.5.1 (https://www.r-project.org/). Descriptive statistics were calculated using mean (standard deviation), median (inter-quartile range) and counts (percentage) as appropriate. In case of continuous endpoints, we used Mann–Whitney U test for inter-group comparison and Wilcox signed-rank test for intra-group comparison. In case of binary endpoints, we used Fisher exact test for inter-group comparison and exact McNemar test for intra-group comparison.
For the sake of normalization, the values for microscopic examination of bacterial colonies and neutrophils were log2-transformed so the difference represents a twofold change in the parameter. Zero values were replaced by 0.5 as a half of minimal detectable value. Additional sensitivity analysis was performed for addition of 0.5 to all values with no significant changes in the results.
For additional analysis of continuous endpoints, we filtered out outliers (by 1.5 IQR from Q1 and Q3) and tested for linearity of regression (by visual examination and Pearson’s correlation test), homoscedasticity of residuals (by Levene test), normality of residuals (by Shapiro-Wilk test), autocorrelation of residuals (by Durbin-Watson test), homogeneity of regression slopes (by type III ANOVA for group-baseline interaction). For continuous endpoints fitting these assumptions we performed univariable linear regression with change from baseline as the dependant variable and study group as the independent variable. Additional multivariable analysis with baseline level of the outcome as a covariate was performed.
For binary endpoints, we used logistic regression with study group as an independent variable and, additionally, the regression with baseline level of corresponding continuous variable (where applicable) as a covariate.
Inter-group differences were reported as mean difference or odds ratio as appropriate, with corresponding 95% confidence intervals.
To assess the robustness of the findings to missing data, a sensitivity analysis using extreme assumptions for patients with missing recurrence status was performed. Specifically, for the experimental group (antibiotics plus bovhyaluronidase azoximer), all patients with missing recurrence data were alternatively imputed as having experienced a recurrence (worst-case scenario) or as being recurrence-free (best-case scenario) at both 6 and 12 months. Fisher’s exact test was used to compare proportions of patients with at least one recurrence between treatment groups.
To address the issue of multiple testing, three key secondary endpoints of primary clinical interest were pre-specified: change in total NIH-CPSI score, change in electron microscopy-based bacterial colony counts (log2 scale), and change in electron microscopy-based neutrophil counts (log2 scale). For these key secondary endpoints, p-values from the ANCOVA models were additionally adjusted for multiplicity using the Holm method to control the family-wise error rate at an alpha level of 0.05. All other secondary analyses were considered exploratory, and their p values were interpreted descriptively without formal adjustment for multiple comparisons.
Statistical significance was determined at the 5% level using two-sided hypothesis tests.
Results
The study included 98 patients aged from 19.5 to 52.7 years (ME = 35.7, IQR: 31.6–39.6). (Figure 1) Descriptive statistics by visit are presented in Table 1. Two patients in the experimental group were lost to follow-up without explanation since 3-month visit. CONSORT flow chart is presented in the Figure 1. There was no statistically significant difference between the two groups in most of the screening results. However, upon assessing the indicators at the follow-up visit, which occurred 3 months later, several statistically significant differences were identified.
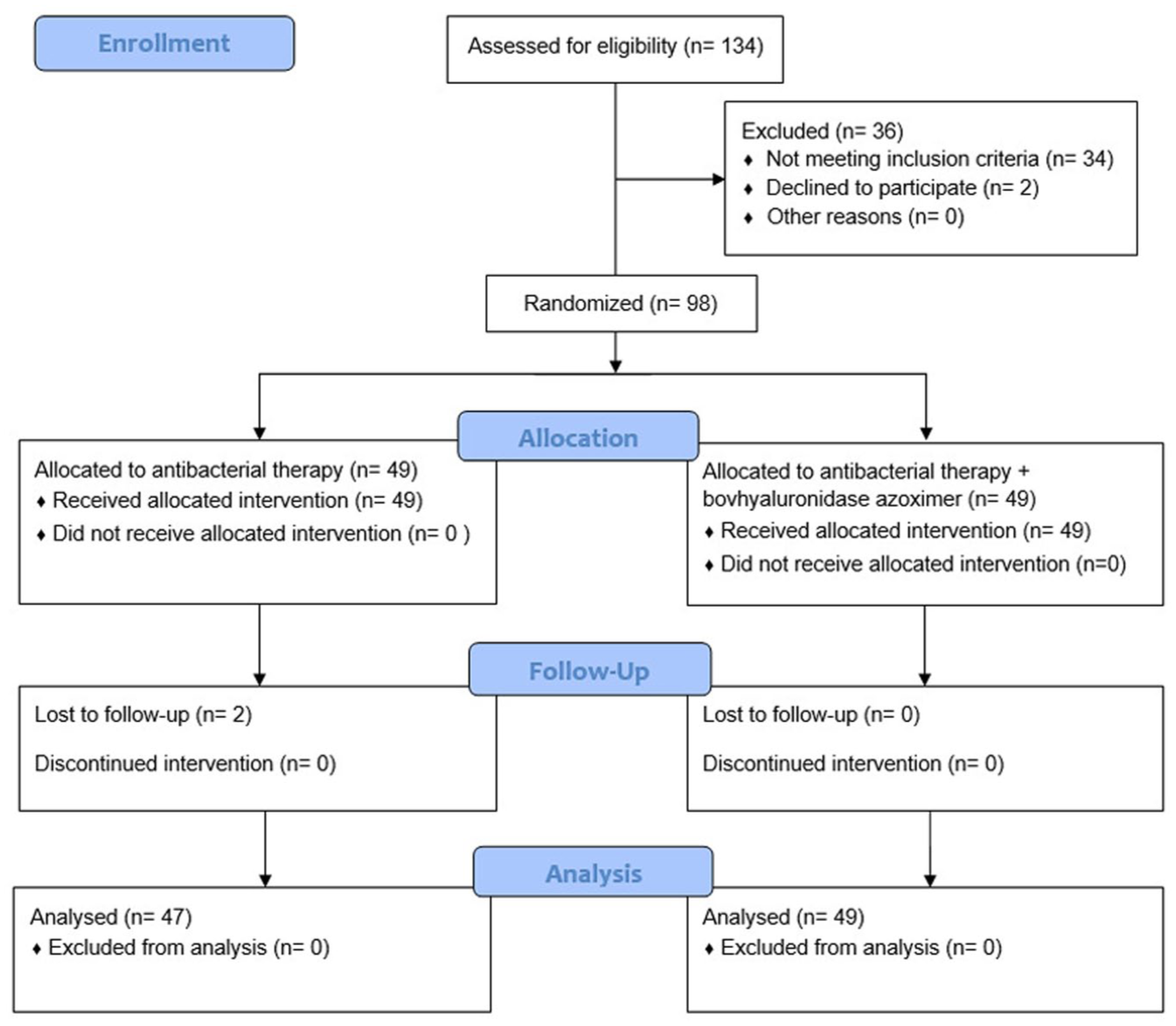
CONSORT flow chart.
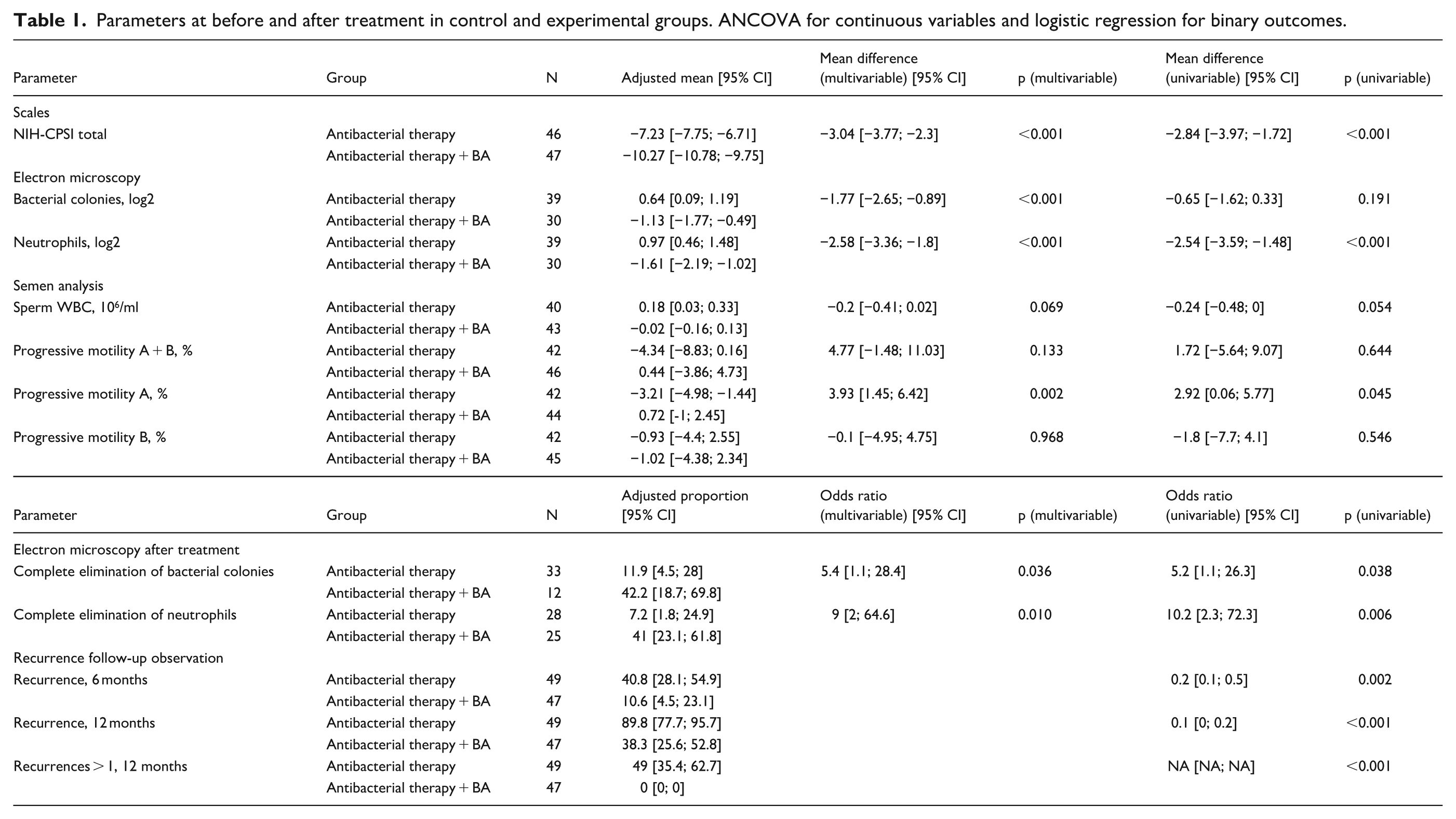
Parameters at before and after treatment in control and experimental groups. ANCOVA for continuous variables and logistic regression for binary outcomes.
The most common species were Corynebacterium spp. (found in 36.6% of patients), Eubacterium spp. (31.5%), Enterobacteriaceae spp./Enterococcus spp. (27%), Staphylococcus spp. (25.5%). More rarely were identified Bacteroides spp./Porphyromonas spp./Prevotella spp. (20.5%), Streptococcus spp. (17.5%), Anaerococcus spp. (16%), Peptostreptococcus spp./Parvimonas spp. (13.5%).
The NIH-CPSI scale showed a significant reduction (MD −3.04, 95%CI: −3.77 to −2.3, p < 0.001) in the experimental group compared to the control group (Figure 2). The measurement of MD among individual NIH-CPSI domains was not performed due to non-compliance with ANCOVA assumptions. In the total NIH-CPSI score, ANCOVA assumptions were met by summation, which resulted in a more even, non-discrete distribution.
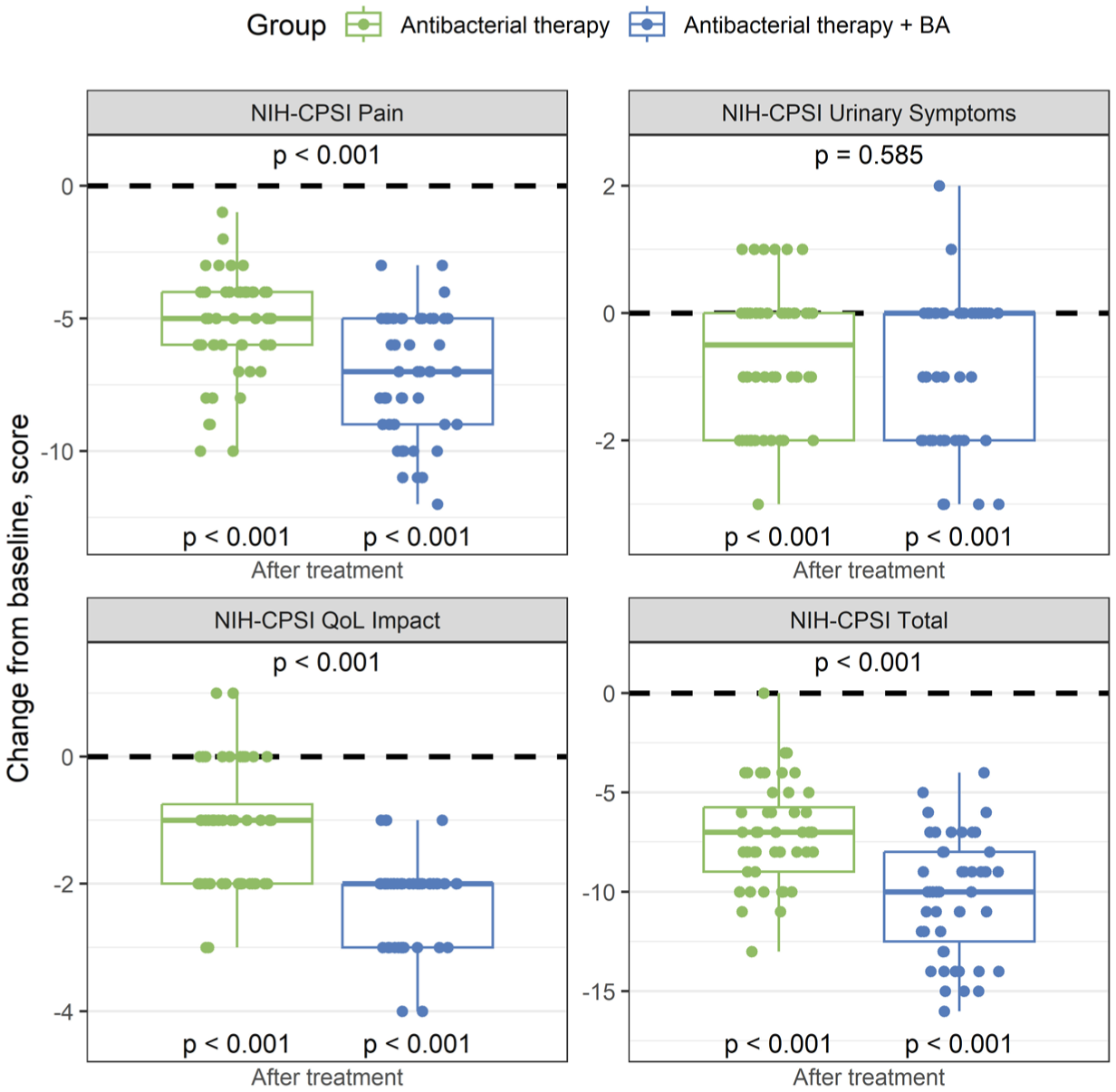
Change from baseline in NIH-CPSI domain scores.
The percentage of sperm with progressive motility A showed a significant improvement in the experimental group (mean difference 3.93, 95%CI: 1.45 to 6.42, p = 0.002). No significant differences were found between the treatment groups in absolute sperm volume, sperm count, sperm concentration, normal morphology sperm count, alive sperm count, total motility, progressive motility B, sperm WBC count (p > 0.05).
Electron microscopy revealed a significant difference in the number of bacterial colonies (log2 difference −1.77, 95%CI: −2.65 to −0.89, p < 0.001) and neutrophils (log2 difference −2.58, 95%CI: −3.36 to −1.8, p < 0.001) in the ejaculate of the experimental group compared to the control group. Furthermore, the experimental group showed a significantly higher elimination rate of ejaculate neutrophils (41% vs 7.2%, p = 0.01), and bacterial colonies (41.7% vs 12.1%, p = 0.043) compared to the control. (Figure 3).
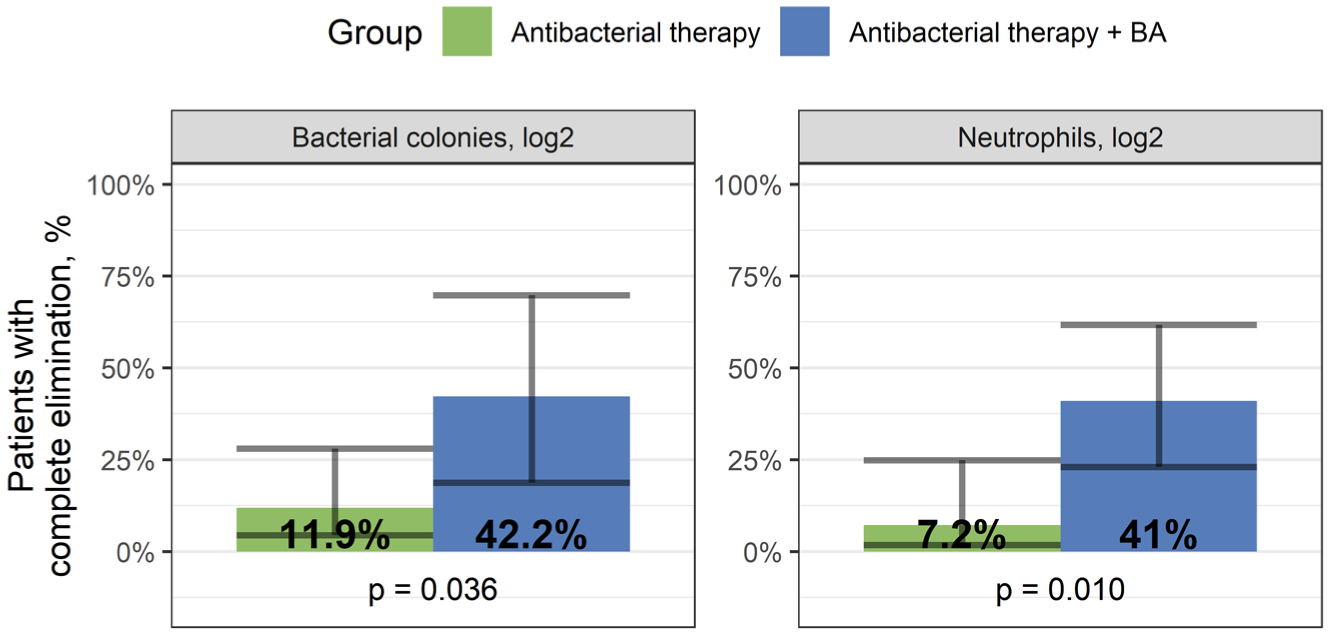
A – change from baseline in ejaculate neutrophil and bacterial colony count (log2 scale). B – complete elimination of neutrophils and bacterial colonies from the ejaculate.
Electron microscopy images of the ejaculate before and after treatment revealed a reduction in bacterial colonies in both groups. However, in the experimental group with bovhyaluronidase azoximer, the intercellular matrix was disrupted, and individual bacteria were observed with cell wall damage. In contrast, the microcolonies in the control group showed no signs of morphological changes (Figures 4 and 5).
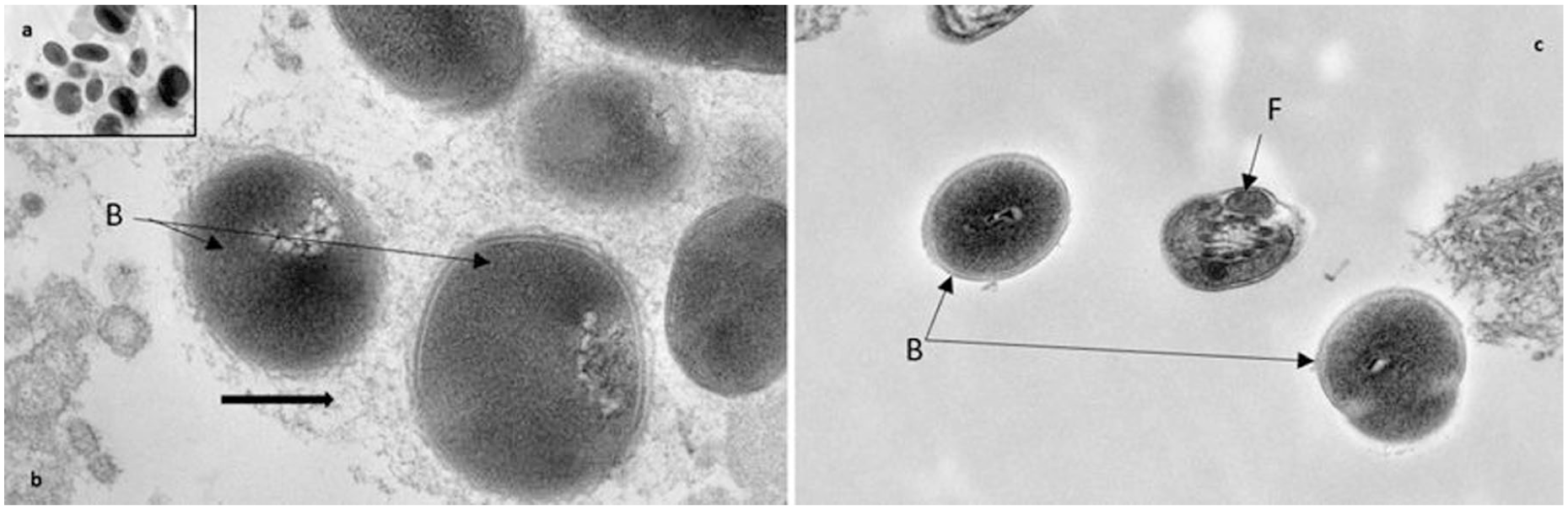
(a–c) Ultrathin sections of patient C. ejaculate before therapy with Bovhyaluronidase azoximer ((a and b) fragment) and after therapy (c). Gram-negative bacterial cells are located in a delicate fibrous matrix (arrows). After therapy, three single bacterial cells with a smooth cell wall were observed in the ejaculate. No matrix was detected. B - bacterial cells, F - cross-section of the spermatozoon flagellum.
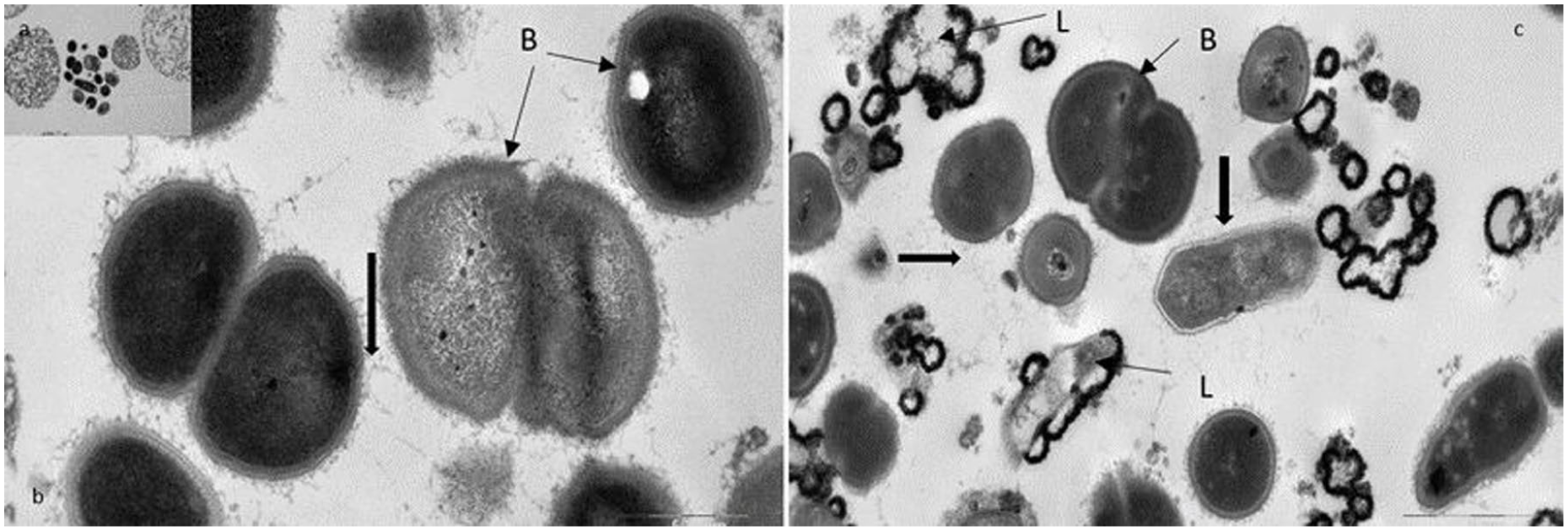
(a–c) Ultrathin sections of patient K ejaculate before therapy without Bovhyaluronidase azoximer ((a and b) - fragments) and after therapy (c) (control group). Bacterial cells (b) are located in a delicate fibrous matrix (arrows). Lysis of individual bacteria was detected (L). A delicate fibrous matrix is revealed between the bacterial cells.
For the three key secondary endpoints (NIH-CPSI total, electron microscopy bacterial colonies log2, and electron microscopy neutrophils log2), the multivariable p-values from the ANCOVA models were all 0.001. After Holm adjustment for multiple comparisons, the corresponding adjusted p-values were approximately 0.003 for each endpoint, remaining well below the prespecified significance level of 0.05.
Regarding disease recurrence, the dynamic follow-up data revealed that the experimental group showed significantly fewer recurrences at both 6 months (10.6% vs 40.8%, p = 0.002) and 12 months (38.3% vs 89.8%, p < 0.001) compared to the control. Three patients in the experimental group had missing recurrence data at both six and 12 months and were excluded from the complete-case analysis. In a sensitivity analysis assuming that all three experienced a recurrence (worst-case scenario), recurrence rates were 40.8% (20/49) versus 16.0% (8/50) at 6 months (p = 0.008) and 89.8% (44/49) versus 42.0% (21/50) at 12 months (p < 0.0001). Assuming instead that all three patients were recurrence-free (best-case scenario) yielded recurrence rates of 40.8% (20/49) versus 10.0% (5/50) at 6 months (p = 0.0005) and 89.8% (44/49) versus 36.0% (18/50) at 12 months (p < 0.0001). Additionally, there were no instances of multiple relapses within a 12-month period in the experimental group (0% vs 49%, p < 0.001; Figure 6).
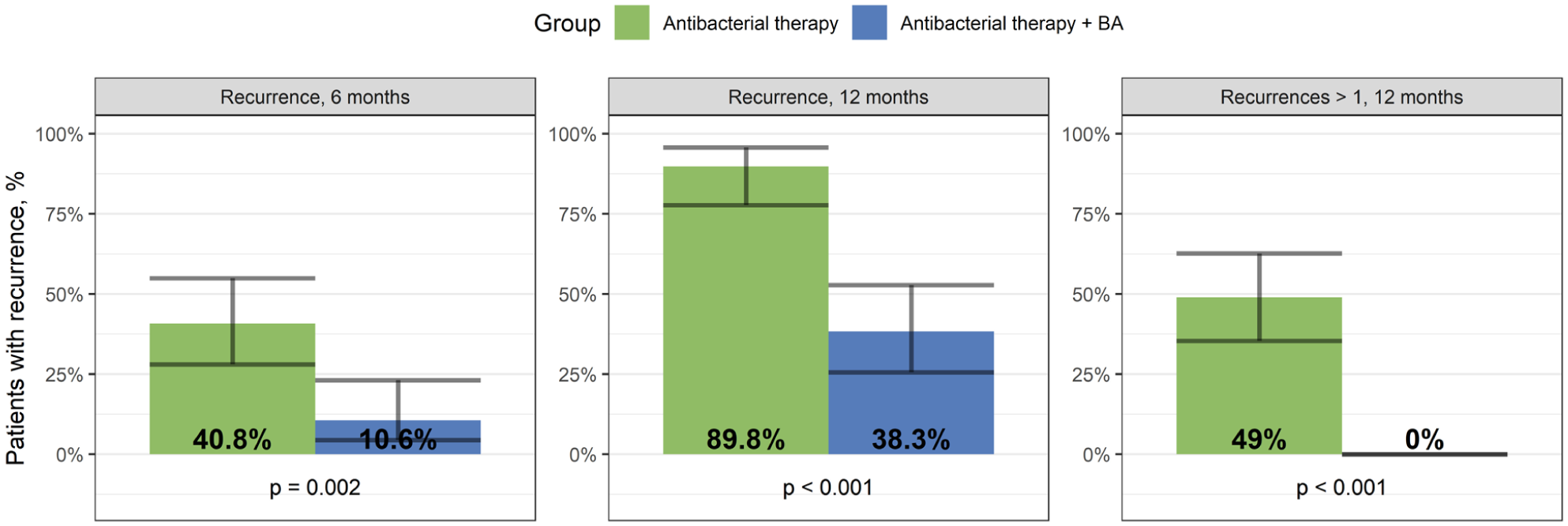
Frequency of disease recurrence at 6 and 12 months, number of cases of >1 recurrence per 12 months.
No serious adverse events occurred. Other adverse events were symptoms of mild intestinal dysbacteriosis due to antibacterial treatment (with no significant difference between the groups) and slight discomfort at the sight of Bovhyaluronidase azoximer i.m. injection. They required no specific actions.
Discussion
We conducted a randomized trial demonstrating anti-biofilm properties of Bovhyaluronidase azoximer. When added to a conventional antibacterial therapy we observed a statistically significant reduction of leukocytes, bacterial microcolonies, and intercellular matrix. These microbiological improvements translated into clinical benefits: NIH-CPSI questionnaire showed a modest reduction in symptom severity. However, it was not possible to conduct a statistically significant assessment of the differences between the groups for each domain due to the high heterogeneity of the data. Most importantly, the number of prostatitis recurrences during the 1-year follow-up was significantly lower.
NIH-CPSI questionnaire, being a subjective diagnostic tool, may be influenced by placebo effect due to open-label design of the study. A meta-analysis by Morozov et al. 13 showed that change up to −4.2 (95%CI −6.31, −2.09) points in NIH-CPSI total score may be related to placebo effect. However, this value implies comparison of questionnaire results before versus after therapy, and not comparison of changes between the groups. In our study absolute changes in each group surpass this value, with the change in experimental group of −10 points (Figure 2). Yet we should keep in mind, that this improvement is partially due to placebo effect, and the effect of the drugs itself is more modest.
Microscopy and bacterial culture of the prostatic secretion are standard tests for diagnosing prostatitis. However, semen culture has been shown to have higher sensitivity. 14 In chronic prostatitis, ejaculate analysis provides information about the prostate as well as reproductive organs such as seminal vesicles and epididymis. Additionally, for young man, providing an ejaculate sample is generally easier and less uncomfortable than undergoing prostate massage, which requires an urologist and may cause both physical and psychological discomfort or even pain. Therefore, due to its diagnostic value and ease of sample collection, our study implemented ejaculate analysis as the method of choice.
Bacterial biofilms are composed of bacteria and the extracellular polymeric matrix they produce. The matrix consists of proteins, polysaccharides and nucleic acids. It not only acts as a mechanical barrier protecting bacteria from immune cells and antibiotics but allows for gene transfer and chemical communication between cells, as the bacteria within the biofilm are immobile and located in close proximity. 15 This environment allows for faster development of antibiotic resistance. Oxygen levels are significantly lower in the center of the biofilm compared to its surface, leading to slower bacterial metabolism. In addition, so called persister cells identified within biofilms are a subset of bacteria capable of surviving even at high antibiotic concentration. These combined factors contribute to the biofilm’s high level of antibiotic resistance. Different bacteria were shown to be up to 30 thousand time more resistant than their planktonic forms. 16
There is currently no standardized approach to deal with biofilms. One possible strategy is physiotherapy, which may be effective for superficial infections. However, when it comes to the prostate – a gland located deep within the pelvis - the choice of treatment modalities and their effectiveness is limited. 17 Another strategy involves the use of various biological or chemical agents aimed at slowing biofilm formation or disrupting established biofilm.16–21 Unfortunately, most of supporting data come from in vitro studies, so the actual clinical benefit of these substances remain uncertain. The results of our study suggest that bovhyaluronidase azoximer may have potential as an anti-biofilm agent. In light of the global rise in antibiotic resistance, the introduction of drugs that inhibit biofilm formation and reduce contributing factors is essential to preserve the efficacy of existing antibacterial therapies.
In recent years, there has been an increase in the use of complementary and alternative medicine (CAM) for the treatment of chronic diseases, including chronic prostatitis. 22 There is a number of studies reporting outcomes of treatment with Bovhyaluronidase azoximer. Kulchavenya et al. proposed an interesting strategy involving the administration of two suppositories during the diagnostic stage. 10 This approach enabled more accurate identification of pathogens in prostatic secretion, increasing the proportion of patients with identified pathogens from 69.2% to 82%. In 7/12 patients initially diagnosed with abacterial prostatitis, enzymatic provocation with bovhyaluronidase azoximer enabled bacterial identification, allowing for etiotropic treatment. Furthermore, the number of leukocytes increased by 50.2%. In a multicenter randomized study, Kotov et al. administered bovhyaluronidase azoximer following transurethral resection of the prostate. 23 Patients receiving 20 suppositories experienced lower rates of bacteriuria, leukocyturia and overall infectious complications. However, there were no statistically significant differences between the experimental and control groups in postoperative urinary parameters such as IPSS, QoL, Qmax, and post-void residual volume.
One significant limitation of current study is the absence of childbirth rate assessment. This outcome reflects the fertility of a couple and can be significantly influenced by female factors, thus limiting its interpretive value. Additionally, it remains unclear whether the study drug exerts a significant effect on spermogram parameters. Although a trend toward improvement was observed, these changes did not reach statistical significance. Experimental group favored only in improvement of the percentage of sperm with progressive motility A, so its influence on fertility is disputable. Therefore, further prospective randomized studies are warranted to clarify its impact in this area. Another limitation is an open-label design. Placebo effect might contribute to improvement of questionnaires results, however, we assessed multiple objective features by microscopy and cultural methods, so we believe subjective improvement reflects normalization of mictobiota and inflammation to a greater extent than expectation of symptoms relief from the new drug. Although it’s a common feature of many bacteria to form biofilms, the efficacy of biofilm-disrupting agents may differ depending on pathogen distribution, so in areas with other microbiota spectrum outcomes also might differ.
Conclusions
An important aspect of chronic prostatitis treatment is the disruption of bacterial biofilm, with the aim of reducing antibiotic resistance and recurrence rates. The addition of bovhyaluronidase azoximer to antibiotic therapy led to a statistically significant improvement in NIH-CPSI scores, a reduction in leukocytes and bacteria colonies as well as a lower recurrence rate compared to antibiotic treatment alone. Following bovhyaluronidase azoximer treatment, only individual bacterial cells were observed, whereas bacterial microcolonies persisted in its absence.
Supplemental Material
sj-docx-1-urj-10.1177_03915603261453123 – Supplemental material for A randomized controlled trial on the impact of bovhyaluronidase azoximer on ejaculate biofilms in patients with chronic prostatitis
Supplemental material, sj-docx-1-urj-10.1177_03915603261453123 for A randomized controlled trial on the impact of bovhyaluronidase azoximer on ejaculate biofilms in patients with chronic prostatitis by Morozov Andrey, Vovdenko Stanislav, Bragina Elizaveta, Boldyreva Margarita, Mhitaryan Ofelia, Zubkov Dmitry, Allenov Sergey, Korolev Dmitry, Evdokimov Mikhail, Rapoport Leonid, Gazimiev Magomed and Spivak Leonid in Urologia Journal
Footnotes
Abbreviations
NIH-CPSI - National Institutes of Health Chronic Prostatitis Symptom Index
IPSS - International Prostate Symptom Score
QoL - Quality of life
RT-PCR - Reverse transcription-polymerase chain reaction
GCP - Good clinical practice
DRE - Digital rectal examination
Ethical considerations
This study was approved by the Institutional Ethics Committee prior to data collection as it was collected from the database.
Consent to participate
Written informed consent was obtained from all patients prior to surgery and inclusion in the study.
Human ethics and consent to participate declarations
IRB approval – protocol №152, June 14, 2022. All the patients read and signed an informed consent form. The research followed principles from the Declaration of Helsinki.
Authors’ contributions
MA – data analysis, critical review, writing the manuscript
VS - data analysis, critical review, writing the manuscript
BE - microscopic imaging and interpretation
BM – data analysis, supervision
MO– data acquisition, database maintenance
ZD - statistical processing
AS– critical review, supervision
KD – critical review, supervision
EM – data acquisition, supervision
RL– critical review, supervision
GM – critical review, supervision
SL – study design, critical review, supervision.
All authors contributed equally to the manuscript and read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dmitry Zubkov reports a relationship with NPO Petrovax Pharm LLC that includes: employment as a statistician. He took part in development of the study design and statistical analysis, but was not involved in data collection or manuscript writing.
Other authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Data availability statement
All of the data are provided within the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.