
Abstract
Prostate cancer (PCa) remains a leading cause of cancer-related morbidity and mortality among men worldwide, with advanced stages often exhibiting resistance to standard therapies. Drug resistance in advanced prostate cancer is a multifactorial process influenced by genetic mutations, hereditary factors, epigenetic alterations, lifestyle choices, and dietary habits. Understanding this complex interplay is crucial for developing effective predictive and therapeutic strategies. In this context, a multiomics approach integrating genomics, transcriptomics, proteomics, metabolomics, and epigenomics offers a comprehensive framework to dissect the molecular mechanisms driving drug resistance.
Current challenges include tumor heterogeneity, limited access to longitudinal patient data, and insufficient representation of diverse populations in omics datasets. This study highlights the novel application of multiomics integration to stratify patient subgroups based on molecular signatures, enabling early prediction of therapy resistance. We also emphasize key biomarkers and signaling pathways associated with treatment failure, including alterations in androgen receptor signaling, PI3K-AKT-motor pathways, and metabolic rewiring. The integration of these datasets not only enhances diagnostic precision but also aids in identifying actionable therapeutic targets. It also opens up new avenues for developing targeted therapies by integrative profiling and quantifying a broad spectrum of biomolecular features across distinct subtypes of malignant cells.
Introduction
Cancer remains one of the most pressing global health challenges of the 21st century. Among men, prostate cancer (PCa) is a leading contributor to both morbidity and mortality. As of GLOBOCAN 2022 estimates, prostate cancer accounted for approximately 1.5 million new cases and 397,000 deaths worldwide, making it one of the most burdensome malignancies globally. 1 While the risk of developing prostate cancer increases with age, the underlying molecular events that drive its initiation often begin much earlier in life. Histologically, the disease typically originates from prostatic intraepithelial neoplasia (PIN). This precursor lesion can evolve into localized adenocarcinoma and eventually metastasize due to the accumulation of somatic mutations over time.2–4 Prostate cancer is characterized by extensive interpatient and intra-tumoral heterogeneity, involving a complex interplay of genomic alterations, epigenetic changes, transcriptomic shifts, and proteomic variations. 5
The disease’s progression to hormone-resistant prostate cancer (HRPC) or castration-resistant prostate cancer (CRPC)-an aggressive and treatment-refractory form-represents a significant clinical challenge. Initially responsive to androgen deprivation therapy (ADT), many patients eventually develop resistance, leading to metastatic CRPC (mCRPC), where current therapeutic options offer limited long-term survival benefits.6,7 Beyond prostate cancer, recent reviews have also highlighted the pivotal role of multiomics approaches, including genomics, transcriptomics, proteomics, and metabolomics, in understanding the Renal Cell Carcinoma heterogeneity, resistance mechanisms, and the potential to pre-emptively tailor treatments. 8 Most multiomics datasets in prostate cancer are derived from European-ancestry cohorts, which limits the generalizability of predictive biomarkers. Recent studies have shown ancestry-specific differences in genomic, epigenomic, and transcriptomic profiles, such as distinct drug metabolism signatures across White, Black, and Asian patients, 9 and race-specific alterations in African American versus European American prostate cancers. 10 Addressing all those issues, including demographic bias through inclusion of diverse populations and stratified validation, is essential to ensure clinical applicability. In this context, multiomics-the integrated analysis of multiple layers of biological information, such as genomics, transcriptomics, epigenomics, proteomics, and metabolomics-is emerging as a transformative approach to understanding the complexity of prostate cancer. For example, genomic sequencing may reveal androgen receptor (AR) gene amplifications or TP53 mutations, transcriptomics can highlight gene expression profiles associated with therapy resistance, and proteomics can identify dysregulated signaling pathways that underlie aggressive tumor behavior.11,12 In addition, inflammation-related biomarkers have shown promise in predicting therapy response and resistance. Integrating inflammatory markers with multiomics profiling could provide novel predictive insights into tumor progression and drug resistance. 13
The main objective of this study is to explore how multiomics strategies can be harnessed to predict and overcome drug resistance in advanced prostate cancer, particularly in the context of mCRPC. Therefore, it is rational to develop personalized therapeutic approaches, uncover novel biomarkers, and enhance predictive modeling for resistance mechanisms by integrating high-throughput data from various biological domains. This comprehensive systems biology perspective holds promise in addressing the limitations of monotherapy and guiding more effective treatment regimens for patients with advanced disease.
Predisposition to prostate cancer: the influence of germline mutations, ethnicity, lifestyle, diet, and hormonal factors
Prostate cancer is one of the most prevalent malignancies affecting men globally, with a complex etiology influenced by both genetic and environmental factors. The predisposition to prostate cancer arises from a combination of genetic susceptibility, hereditary influences, lifestyle choices, dietary habits, and other environmental exposures.
Genetic and hereditary factors
Prostate cancer risk often arises from the interaction of multiple low-penetrance genetic variants (polygenic risk) along with some high-penetrance monogenic mutations.14,15 Males who have a first-degree relative (father or brother) with prostate cancer are at least twice as likely to develop the disease compared to those without a familial history. 16 If the relative was diagnosed at an early age (before 55 years), the relative risk increases to 3–5 times, indicating the importance of familial clustering and early-onset cases as red flags for heightened surveillance.
Germline mutations and DNA repair genes
Advancements in genetic research have identified specific germline mutations associated with a higher risk of developing aggressive or metastatic forms of PCa. Notable among these are mutations in DNA repair genes, such as BRCA1 and BRCA2. Although these two genes are primarily linked to breast and ovarian cancers, mutations in these genes significantly elevate the risk of prostate cancer, particularly aggressive variants. 17 Men with BRCA2 mutations may have a 2.5 to 8.6-fold increased risk, and these mutations are also associated with poor prognosis and reduced treatment response. Mutations in ATM (Ataxia-Telangiectasia Mutated) involved in DNA damage response, are found in a subset of PCa patients and are associated with higher-grade tumors. 18 In addition, CHEK2 and PALB2 genes also contribute to DNA repair and are increasingly recognized in hereditary cancer panels.19,20 Therefore, germline genetic testing for genes with mutations such as ATM, CHEK2, and BRCA1/2 is likely to be incorporated into standard diagnostic protocols for men with locally advanced or metastatic disease.
Ethnicity and race
Genetic predisposition also varies with ethnicity and geography. African-American men have a higher incidence and mortality rate from prostate cancer compared to Caucasian and Asian men.21,22 This disparity is likely due to genetic differences, environmental exposures, and socioeconomic factors. However, the risk increases in Asian men who migrate to Western countries, suggesting environmental and lifestyle modifications may unmask underlying genetic susceptibility. 23
Lifestyle and environmental factors
While genetics form the backbone of predisposition, lifestyle and environmental factors play a pivotal role in modulating prostate cancer risk. 24 Sedentary lifestyle is associated with a higher risk of PCa, particularly advanced and aggressive types. 25 Regular physical activity improves insulin sensitivity, reduces systemic inflammation, and modulates hormone levels, protecting against cancer development. In addition, obesity has been linked to more aggressive forms of prostate cancer and worse clinical outcomes. 26
Dietary and food habits
Traditional Western diets high in red meat, processed foods, and saturated fats and low in fruits and vegetables have been associated with higher incidence rates. 27 High consumption of red and processed meats, especially when cooked at high temperatures, produces heterocyclic amines and polycyclic aromatic hydrocarbons, known carcinogens. 28 High-fat diets may also increase androgen levels and oxidative stress, contributing to prostate carcinogenesis. Excessive dairy products and calcium intake have been controversially linked to increased PCa risk, possibly due to reduced circulating vitamin D levels. Conversely, diets rich in fruits, vegetables, whole grains, and omega-3 fatty acids appear protective. Lycopene, found abundantly in tomatoes, and isoflavones, present in soy products, are thought to possess anti-cancer properties. 29 The Mediterranean diet, characterized by olive oil, nuts, fish, and plant-based foods, has been linked to a lower risk of aggressive PCa. 30
Hormonal and endocrine factors
Prostate cancer is a hormonally-driven malignancy primarily regulated by androgens, particularly testosterone and dihydrotestosterone (DHT). Elevated levels of circulating androgens or increased androgen receptor sensitivity may predispose individuals to cancer development. 31 Additionally, endocrine-disrupting chemicals (EDCs) found in plastics, pesticides, and industrial pollutants can mimic or interfere with hormone signaling and have been implicated in hormonal imbalance and increased cancer risk.32–35
Overall, prostate cancer predisposition is a multifactorial interplay of hereditary, genetic, and environmental components. While genetic susceptibility, especially in the form of familial clustering and germline mutations, plays a pivotal role, modifiable risk factors such as diet, obesity, and lifestyle significantly influence disease development and progression. A deeper understanding of these factors enables personalized screening strategies, precision medicine, and family risk counseling. Integration of germline genetic testing, especially in high-risk groups, is critical in identifying predisposed individuals and optimizing therapeutic outcomes. Ongoing research into genetic profiling, polygenic risk scoring, and preventive interventions holds promise for reducing the global burden of prostate cancer.
Resistance as a therapeutic obstacle in prostate cancer: mechanisms and clinical implications
Resistance to conventional treatments remains a significant challenge in managing prostate cancer, particularly in its advanced stages. For localized or low-to-intermediate-risk prostate cancer, treatment options often include active surveillance, radical prostatectomy, external beam radiation therapy, or brachytherapy. 36 These interventions often offer high cure rates and favorable long-term outcomes. However, treatment becomes significantly more challenging in advanced or metastatic prostate cancer, particularly in the context of therapy resistance. As prostate cancer progresses to more aggressive forms such as mCRPC, it often exhibits resistance to multiple lines of conventional therapy. mCRPC represents a stage where the disease continues to advance despite androgen deprivation therapy (ADT), which is initially effective in reducing tumor burden by suppressing androgen levels. Resistance to ADT occurs as tumor cells adapt, leading to sustained AR signaling despite low circulating androgen levels. 37 This biological adaptability is a significant obstacle, as AR signaling remains a critical driver of prostate cancer cell survival and proliferation.
Resistance is not limited to hormonal therapy. Chemotherapy, particularly with docetaxel, a taxane-based agent, has been a mainstay treatment for mCRPC. However, while it provides some survival benefits, resistance inevitably develops. Studies indicate that nearly 90% of treatment failures in metastatic prostate cancer are due to chemotherapy resistance. 38 Multiple mechanisms contribute to this resistance, including drug efflux via ATP-binding cassette (ABC) transporters, alterations in microtubule dynamics, evasion of apoptosis, and enrichment of cancer stem-like cells. 39 As a result, treatment efficacy diminishes over time, leading to poor prognosis and limited therapeutic options. Despite the approval of newer agents such as abiraterone, enzalutamide, apalutamide, cabazitaxel, radium-223, and sipuleucel-T, the average extension in overall survival remains modest. The mean increase in overall longevity with these six FDA-approved therapies is only around 4.8 months. 40 These limited benefits are likely due to the rapid emergence of resistance mechanisms, including AR splice variants (e.g. AR-V7), which allow continued tumor progression even without androgens. Additionally, cross-resistance between hormonal agents like abiraterone and enzalutamide has been documented, further limiting sequential treatment strategies. 41
A further complication arises with the transition to CRPC, a form of the disease that arises in 10%–20% of men with prostate cancer metastasis within 5 years of follow-up. Patients with non-metastatic CRPC (nmCRPC) are also at high risk of disease progression. The underlying biology of CRPC is complex and driven by both AR-dependent and AR-independent pathways, including PI3K/AKT/mTOR signaling, epigenetic alterations, immune evasion, and metabolic reprograming. 42 Such multifaceted resistance mechanisms pose a significant challenge to the efficacy of existing treatments. Moreover, the tumor microenvironment plays a substantial role in promoting resistance. Cancer-associated fibroblasts, immune cells, and extracellular matrix components can influence drug penetration, support tumor cell survival, and modulate immune responses, thereby contributing to treatment failure. 43 Additionally, intra-tumoral heterogeneity and the presence of subclonal populations within the tumor further complicate treatment, as different clones may respond variably to therapy, allowing for the emergence of resistant populations. Addressing this challenge requires a deeper understanding of resistance mechanisms and the development of innovative, individualized treatment modalities.
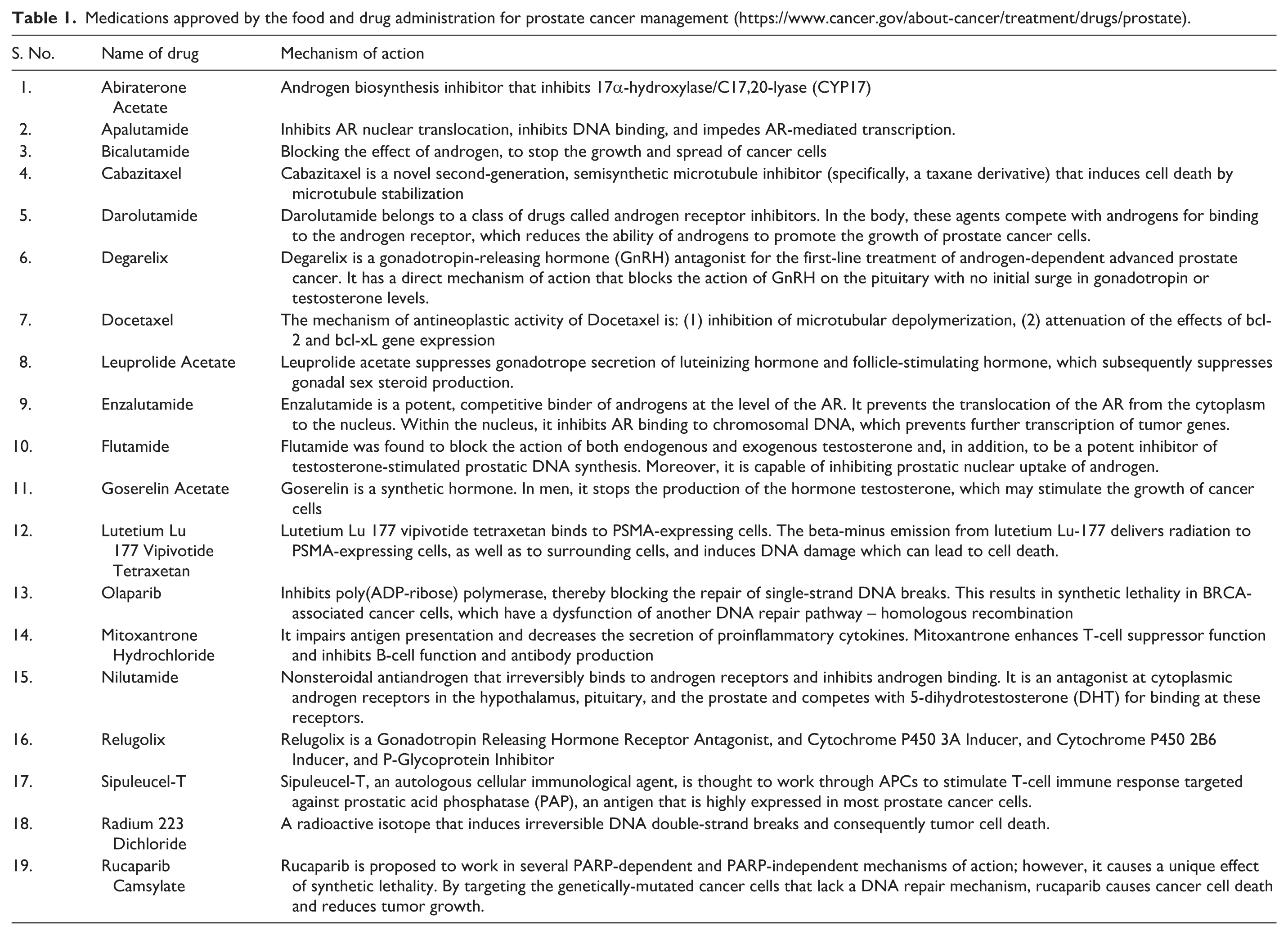
Even though there are several FDA-approved prostate cancer drugs are currently available (Table 1)44–47 around 15%–33 % of patients develop metastases within around 2 years, which increases the mortality rate, indicating the significance of understanding the multiomics approaches to combat drug resistance in advanced prostate cancer.
Medications approved by the food and drug administration for prostate cancer management (https://www.cancer.gov/about-cancer/treatment/drugs/prostate).
Novel therapeutic strategies to combat resistance in metastatic castration-resistant prostate cancer
The development of resistance in prostate cancer is multifactorial and complex, particularly in mCRPC-and continues to be a major clinical challenge. However, novel strategies like next-generation AR targeting, epigenetic modulation, immunotherapy, targeted gene repair inhibitors, and nanotechnology-based delivery systems AR degradation, epigenetic modulation, PSMA-targeted immunotherapies, synthetic lethality, and nanotechnology are reshaping the therapeutic landscape.
Next-Generation Androgen Receptor Targeting: Even in castration-resistant states, prostate cancer remains heavily dependent on AR signaling. Novel AR degraders, such as PROTACs (Proteolysis-Targeting Chimeras), represent a breakthrough approach. Unlike traditional inhibitors that block AR function, PROTACs induce degradation of the AR protein itself, eliminating its activity. 48 These molecules show promise in preclinical and early clinical trials, especially in tumors expressing AR splice variants resistant to current antiandrogens.
Epigenetic Therapy: Epigenetic dysregulation plays a central role in therapy resistance. EZH2, a histone methyltransferase, has emerged as a crucial mediator of AR-independent growth in resistant prostate cancer. Inhibitors of EZH2 can reprogram tumor cells to become more immunogenic and responsive to therapy. 49 Combining EZH2 inhibitors with checkpoint inhibitors is currently under clinical investigation as a synergistic strategy.
Immunotherapy and PSMA-Targeted Therapies: Prostate cancer has historically shown poor responses to immune checkpoint inhibitors due to its immunologically “cold” tumor microenvironment. However, targeting prostate-specific membrane antigen (PSMA) using novel platforms such as CAR-T cells, bispecific T-cell engagers (BiTEs), and PSMA-directed antibody-drug conjugates has shown promise in overcoming this resistance. For instance, in clinical trials, PSMA CAR-T cell therapy is being refined to improve infiltration, persistence, and reduced toxicity. 50
Synthetic Lethality and PARP Inhibitors: The discovery of DNA repair gene mutations (e.g. BRCA1/2, ATM) in prostate cancer has paved the way for synthetic lethality-based approaches using PARP inhibitors. These agents exploit defects in homologous recombination repair pathways, selectively killing cancer cells while sparing normal ones. Olaparib and rucaparib are now approved for mCRPC with BRCA mutations and are also being investigated in combination with other therapies to prevent or delay resistance. 51
Nanotechnology-Based Delivery: Nanoparticles deliver anticancer agents directly to tumor sites, bypassing drug efflux pumps and improving drug accumulation in resistant cancer cells. Lipid-based nanoparticles, dendrimers, and polymeric micelles are under active development for delivering chemotherapeutics and siRNA to silence resistance-associated genes like AR-V7 or BCL2. 52 This precision delivery can minimize systemic toxicity while overcoming multidrug resistance.
Multiomics approaches in personalized treatment strategies: unraveling drug resistance mechanisms in prostate cancer
Multiomics approaches, which integrate genomics, transcriptomics, proteomics, metabolomics, epigenomics, Cistromics, and Radiogenomics, have emerged as transformative tools in unraveling the complexity of drug resistance and guiding personalized treatment strategies. Each omics layer provides unique insights: genomics identifies mutations and copy number alterations (e.g. in AR, BRCA1/2); transcriptomics captures gene expression changes associated with therapy resistance; proteomics reveals post-translational modifications and signaling aberrations; metabolomics characterizes rewired metabolic pathways in resistant phenotypes; and epigenomics exposes DNA methylation and chromatin remodeling patterns that influence gene silencing or activation. When integrated, these datasets provide a systems-level understanding of resistance mechanisms, such as AR signaling adaptation, PI3K-AKT-mTOR activation, or metabolic plasticity.
Clinically, multiomics enables molecular stratification of patients, allowing for early identification of resistance-prone subtypes and guiding tailored therapeutic interventions. For instance, genomic profiling for DNA repair defects (e.g. BRCA2 mutations) informs the use of PARP inhibitors. Similarly, transcriptomic and proteomic markers can predict response to AR-targeted therapies or chemotherapy, while metabolomic profiles may uncover metabolic vulnerabilities for drug repurposing. Moreover, integrating multiomics with AI-driven analytics and liquid biopsy platforms facilitates non-invasive, real-time treatment response and resistance evolution monitoring.
While current multiomics studies have significantly supported our understanding of the mechanisms driving drug resistance in prostate cancer, the literature presents conflicting findings that merit careful interpretation. There are a number of technical limitations, such as variability in sample quality, data integration challenges, and standardized analytic pipelines, that constrain the reproducibility and comparability of results. Additionally, translational bottlenecks, including limited clinical validation and high costs of multiomics profiling, might hinder immediate clinical application. Therefore, a critical assessment of these issues is essential to guide future studies on clinically actionable insights. Integrating multiomics with functional validation and longitudinal patient data may help overcome these barriers and improve predictive accuracy for drug resistance.
As precision oncology advances, multiomics enhances diagnostic accuracy and therapeutic targeting and redefines clinical decision-making in prostate cancer management (Figure 1), paving the way for highly personalized, adaptive, and effective care for drug-resistant PCa.
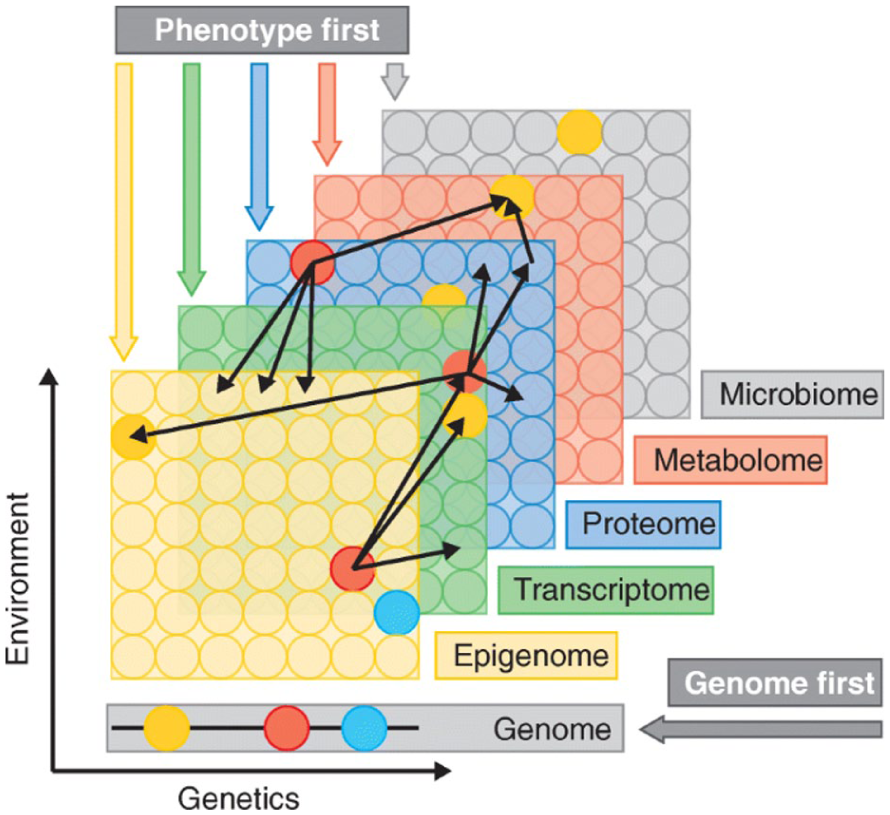
A multiomics model illustrating the interplay between genetics, environment, and phenotypic expression.
It depicts a conceptual multiomics model highlighting how genetic alterations interact with environmental exposures and epigenetic regulation to shape transcriptomic, proteomic, metabolomic, and epigenomic profiles, ultimately driving phenotypic expression and therapeutic response. The layered design illustrates the association of biological information from DNA to phenotype, while emphasizing feedback loops between environment and epigenome. This integrative framework underscores the necessity of combining multiple omics layers to capture the complexity of drug resistance in prostate cancer.
Genomics
Genomic profiling has become a cornerstone in deciphering and managing therapeutic resistance in PCa, particularly in advanced stages such as mCRPC. Resistance to the AR-targeted therapies and chemotherapy is frequently driven by genomic alterations that rewire cellular signaling and survival pathways. High-resolution next-generation sequencing (NGS) technologies now enable the identification of somatic and germline mutations, copy number alterations, and structural variants that influence treatment response and resistance.54,55 Clinically actionable genomic alterations have direct therapeutic implications. DNA damage repair (DDR) gene mutations—particularly in BRCA1/2 and ATM-predict response to PARP inhibitors, leading to the FDA approval of olaparib and rucaparib for mCRPC with homologous recombination repair (HRR) deficiencies.51,56 Similarly, AR gene amplifications, point mutations (e.g. T878A, L702H), and splice variants like AR-V7 correlate with resistance to AR pathway inhibitors and guide the selection of alternative therapies, such as taxane-based chemotherapy. 57
Emerging genomic frameworks are now integrated with AI-driven predictive models and liquid biopsy platforms (cfDNA and CTCs) for real-time monitoring of tumor evolution and resistance emergence. 58 These advances support a dynamic, precision-guided treatment paradigm (Figure 2) that improves therapeutic outcomes and anticipates resistance before clinical progression-pushing the boundaries of personalized medicine in PCa. It highlights how genomic profiling identifies actionable mutations and copy-number alterations in prostate cancer, enabling the selection of targeted therapies such as BRCA and AR pathway modulators, including PARP inhibitors. These insights help identify vulnerabilities and guide the use of targeted therapies such as PARP inhibitors or next-generation AR-directed agents.
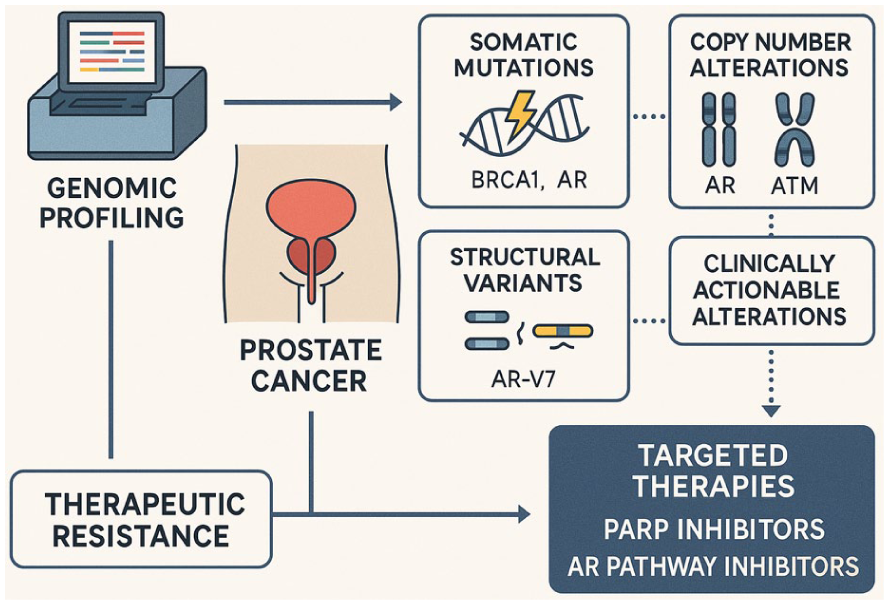
Genomic profiling-guided targeted therapy in prostate cancer.
Transcriptomics
Transcriptomics offers a dynamic lens into the gene expression alterations driving medication resistance in prostate cancer (PCa), especially in the progression to mCRPC. Unlike static genomic mutations, transcriptomic profiles capture real-time cellular responses to therapeutic pressure, unveiling adaptive mechanisms such as AR signaling reactivation, lineage plasticity, and epithelial-mesenchymal transition (EMT).59,60 Advanced RNA sequencing (RNA-seq) technologies have identified resistance-associated transcriptional signatures, including overexpression of AR splice variants (notably AR-V7), neuroendocrine differentiation markers (e.g. CHGA, SYP, ASCL1), and stemness-associated pathways (e.g. SOX2, NANOG) that emerge under androgen-deprivation or AR-targeted therapies. 61 These signatures stratify patients into molecular subtypes with distinct therapeutic vulnerabilities, guiding personalized treatment regimens. AR modulates lineage plasticity and epithelial–mesenchymal transition (EMT), enabling tumor cells to bypass AR dependence, acquire invasive traits, and develop therapy resistance. It emphasizes the value of RNA-based analyses for identifying predictive biomarkers and guiding personalized treatment strategies (Figure 3).
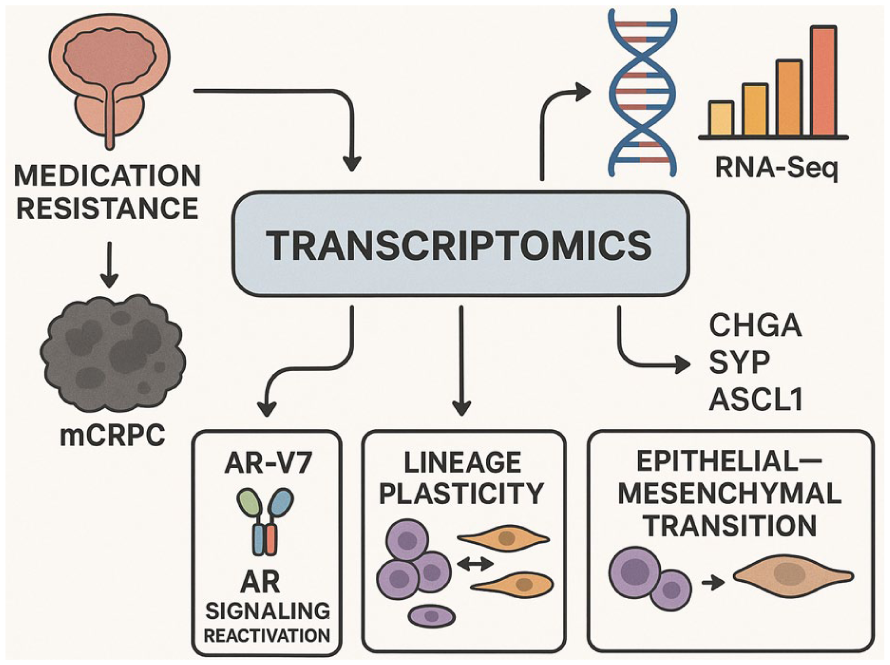
Role of transcriptomics in understanding resistance mechanisms in prostate cancer.
Clinically, AR-V7 mRNA detection in circulating tumor cells is now a validated predictive biomarker, indicating resistance to enzalutamide and abiraterone and prompting a shift toward taxane chemotherapy. 62 Moreover, transcriptomic analysis of tumor biopsies or liquid biopsies enables real-time monitoring of treatment adaptation, offering critical insights into emerging resistance phenotypes before radiographic progression. Integration of transcriptomics with other omics layers and machine learning models enhances the predictive precision of resistance pathways and uncovers novel therapeutic targets, including non-coding RNAs and alternative splicing events. As transcriptomics becomes increasingly accessible and clinically actionable, it is poised to play a pivotal role in precision oncology for drug-resistant PCa. 63
Proteomics
Proteomics offers a powerful, functional perspective on the molecular underpinnings of drug resistance in prostate cancer (PCa), complementing genomic and transcriptomic insights by capturing post-translational modifications (PTMs), protein-protein interactions, and signaling cascades in real-time. Unlike nucleic acid-based methods, proteomics directly interrogates the effector molecules of resistance proteins and their dynamic modulation under therapeutic pressure.64,65 Mass spectrometry-based proteomics and phosphoproteomics have revealed distinct resistance-associated protein signatures, including hyperactivation of the PI3K-AKT-mTOR axis, upregulation of stress response proteins (e.g. HSP90, GRP78), and adaptive modulation of AR co-regulators. 66 These findings elucidate key mechanisms by which tumor cells evade androgen receptor-targeted therapies or develop tolerance to taxanes. Furthermore, proteomic profiling has uncovered phenotypic transitions, such as neuroendocrine differentiation and lineage plasticity, contributing to treatment escape. 59
Clinically, proteomics is increasingly leveraged for biomarker discovery and therapeutic stratification. For example, differential expression of AR splice variant proteins and co-chaperones has been linked to resistance, guiding the use of chaperone inhibitors or PI3K pathway blockade. 67 Integrating proteomics with artificial intelligence and multiomics platforms also supports the development of predictive models for treatment response and resistance evolution. As proteomics technologies advance in sensitivity and throughput, they hold immense promise in tailoring real-time, personalized interventions-ushering in a new era of precision oncology for drug-resistant PCa. In this context, Figure 4 shows how proteomics approaches measure protein modifications and signaling pathway activity to reveal mechanisms of drug resistance in prostate cancer. In particular, mass spectrometry-based approaches enable the identification of protein signatures linked to drug resistance mechanisms in cancer. These protein profiles can uncover biomarkers that guide therapeutic stratification, helping match patients to the most effective treatments. By integrating such proteomic insights, precision oncology advances toward personalized and adaptive treatment strategies.
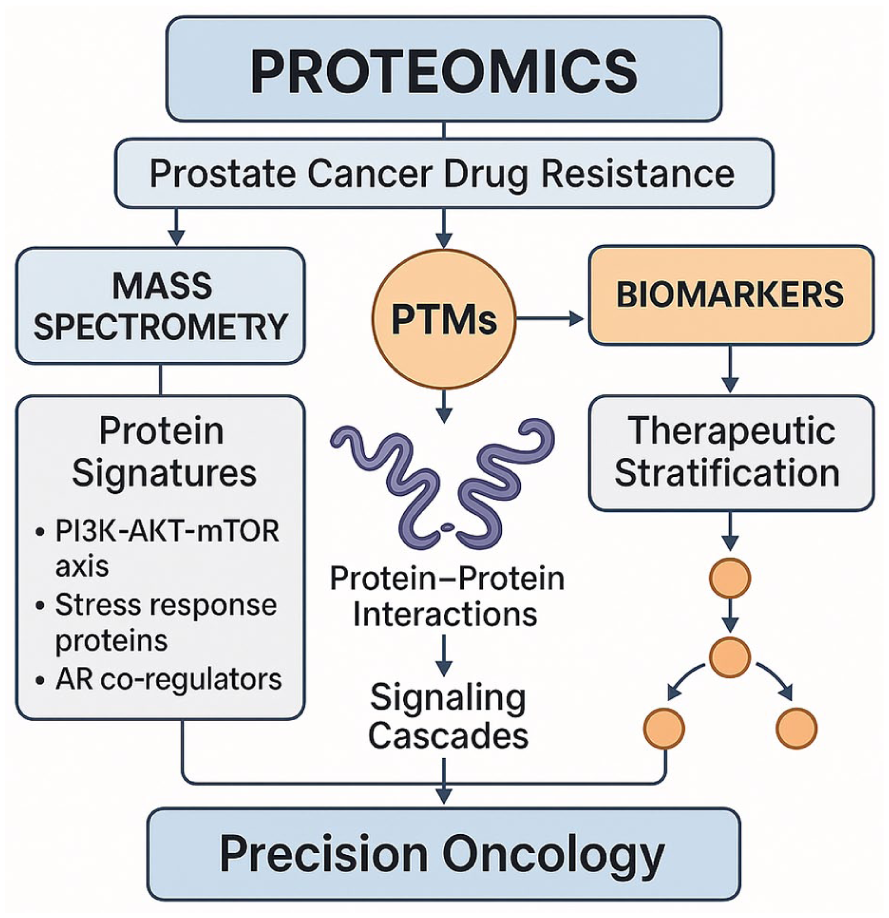
Proteomics approaches in understanding prostate cancer drug resistance and enabling precision oncology.
Metabolomic
Metabolomics has emerged as a cutting-edge approach to understanding and managing medication resistance in prostate cancer (PCa), offering a functional readout of cellular phenotype by profiling metabolites that reflect dynamic alterations in metabolic pathways (Figure 5). It exemplifies how metabolomic profiling uncovers metabolic reprograming in mCRPC under therapeutic pressure. Key pathways such as glycolysis, lipid metabolism, and amino acid turnover are shown to adapt in response to treatment, contributing to drug resistance. The figure highlights the potential of metabolomic insights to identify novel vulnerabilities and guide metabolic-targeted interventions. Unlike genomic or transcriptomic data, metabolomic signatures capture real-time cellular adaptation to therapeutic pressure, revealing metabolic reprograming as a hallmark of therapy resistance. 68 In advanced PCa, particularly mCRPC, drug resistance is often accompanied by profound shifts in lipid metabolism, glycolysis, and amino acid utilization. Resistant tumors upregulate de novo lipogenesis, fatty acid oxidation, and glutaminolysis to sustain proliferation under androgen-deprived or chemotherapeutic conditions. 69 Recent studies using high-resolution mass spectrometry and nuclear magnetic resonance (NMR) spectroscopy have identified distinct metabolomic fingerprints associated with resistance to androgen receptor signaling inhibitors (ARSIs), such as enzalutamide and abiraterone. 70
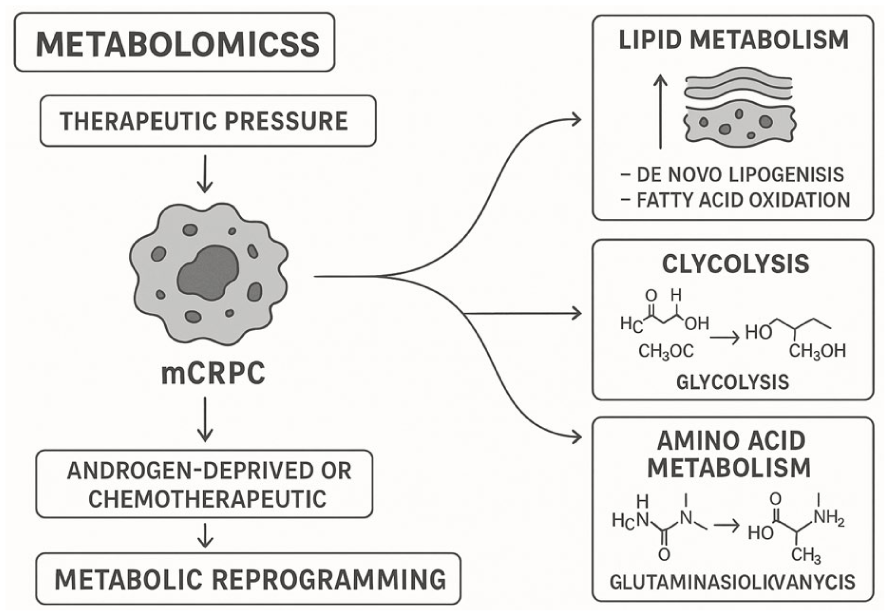
Metabolomics reveals therapeutic pressure-induced metabolic reprograming in mCRPC.
Clinically, metabolomic profiling of plasma, urine, or tumor tissue enables the identification of non-invasive biomarkers predictive of treatment response. For instance, elevated sarcosine and choline derivatives have been linked to aggressive, treatment-resistant PCa phenotypes. Moreover, integrating metabolomic data with multiomics platforms enhances patient stratification. It facilitates the discovery of actionable metabolic vulnerabilities such as targeting fatty acid synthase (FASN) or glutaminase (GLS1) for precision intervention. 71 As metabolomics advances toward clinical translation, it offers novel avenues for real-time monitoring, early resistance detection, and personalized metabolic targeting in drug-refractory prostate cancer.
Radiogenomic
Radiogenomics is a cutting-edge field integrating quantitative imaging features with genomic data, offering an unprecedented approach to deciphering and managing medication resistance (Figure 6) in PCa. It displays the integration of imaging features from multiparametric MRI with genomic and transcriptomic data to uncover mechanisms of drug resistance in prostate cancer. Radiogenomic analysis links spatial heterogeneity observed on imaging with molecular alterations, helping to identify resistant tumor regions. This approach emphasizes the potential of non-invasive, image-guided molecular insights for precision therapy planning.
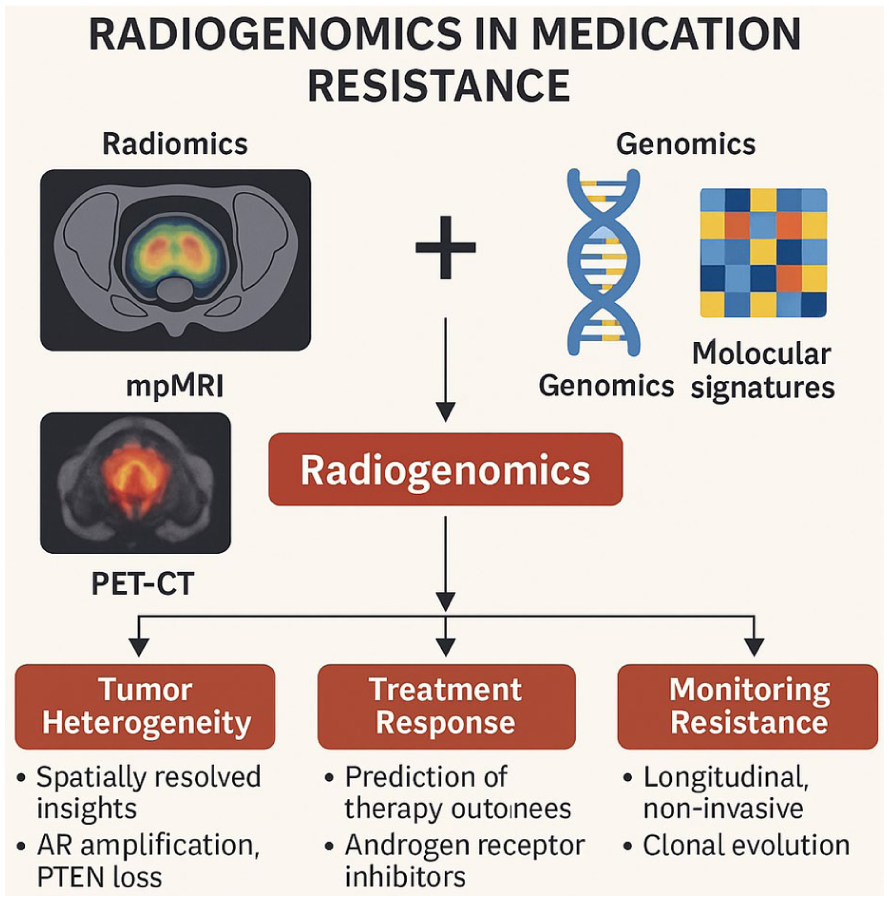
Radiogenomics in unraveling medication resistance in prostate cancer.
By linking radiological phenotypes (radiomics) with tumor genotypes and molecular signatures, radiogenomics enables non-invasive, spatially resolved insights into tumor heterogeneity, treatment response, and resistance evolution. 72 In advanced PCa, especially mCRPC, treatment failure often stems from intratumoral and inter-lesional heterogeneity that is difficult to capture through biopsy alone. Radiogenomic models utilizing multiparametric MRI (mpMRI) and PET-CT imaging have been shown to correlate specific imaging biomarkers such as apparent diffusion coefficient (ADC), lesion texture, or metabolic uptake patterns resistance-associated genomic alterations, including AR amplification, PTEN loss, and TP53 mutations.73,74 Recent studies demonstrate the clinical utility of radiogenomics in stratifying patients based on their likelihood of responding to androgen receptor signaling inhibitors or radioligand therapies. For example, radiomic features from mpMRI have been linked with genomic profiles of neuroendocrine differentiation-an aggressive, drug-resistant PCa subtype, enabling early intervention strategies. 75 Importantly, radiogenomics facilitates longitudinal, non-invasive monitoring of treatment adaptation across metastatic lesions, offering real-time insight into clonal evolution without repeated biopsies. As machine learning and deep learning frameworks mature, radiogenic models will become integral to precision oncology workflows, guiding personalized, adaptive therapies for drug-resistant prostate cancer.
Epigenomics
Epigenomic regulation plays a pivotal role in driving medication resistance in PCa, particularly during progression to mCRPC. Unlike genetic alterations, epigenetic modifications, such as DNA methylation, histone modification, and chromatin remodeling, are reversible and dynamically responsive to therapeutic pressure, making them attractive targets for intervention. 76 Recent studies have identified widespread epigenetic reprograming in resistant PCa, including promoter hypermethylation of tumor suppressor genes (GSTP1, NKX3.1), histone deacetylation-mediated silencing of cell cycle regulators, and enhancer reactivation that sustains AR signaling despite androgen deprivation. 77 These epigenetic changes facilitate lineage plasticity, enabling a shift toward neuroendocrine phenotypes and epithelial-mesenchymal transition (EMT), both associated with resistance to AR-targeted therapies. 78
Clinically, epigenomic biomarkers have emerged to predict resistance and stratify patients. DNA methylation signatures in cell-free DNA (cfDNA) from liquid biopsies are being developed to non-invasively monitor tumor dynamics and resistance evolution. 79 Additionally, therapeutic agents targeting epigenetic modifiers, such as EZH2 inhibitors, HDAC inhibitors, and BET bromodomain blockers, are undergoing clinical evaluation for reversing resistance phenotypes and restoring drug sensitivity. 80 As multiomics integration deepens, epigenomics is poised to serve as both a predictive and therapeutic axis in precision medicine (Figure 7), offering personalized, adaptive strategies to overcome drug resistance in prostate cancer. It represents how epigenomic alterations, including DNA methylation, histone modifications, and chromatin remodeling, contribute to therapy resistance in advanced prostate cancer. These changes can silence tumor suppressor genes or activate resistance pathways, influencing tumor behavior independent of DNA sequence. Androgen deprivation therapy induces adaptive resistance in prostate cancer, highlighting the potential of targeting epigenetic mechanisms to overcome drug resistance and improve therapeutic outcomes
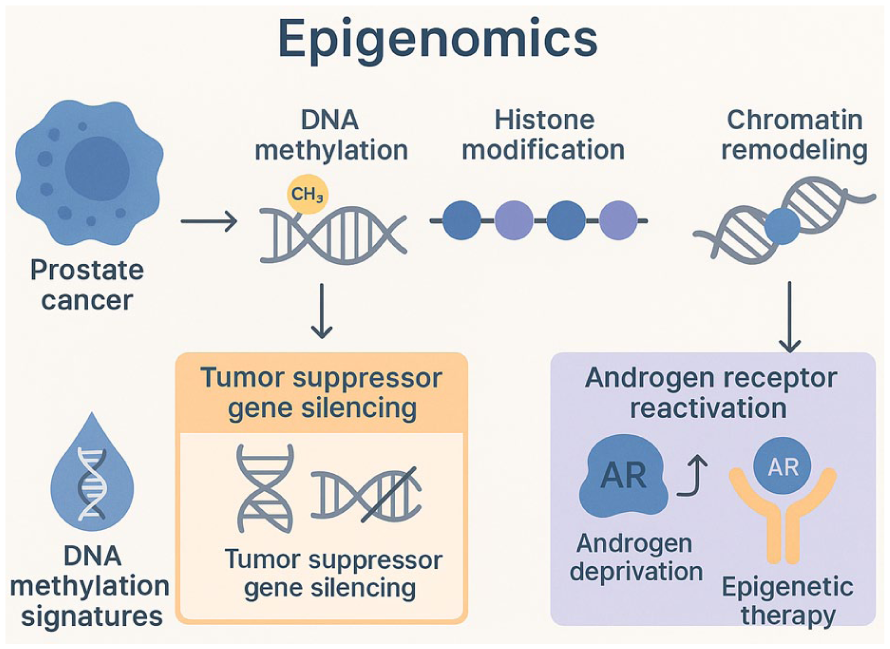
Epigenomic alterations contributing to drug resistance in advanced prostate cancer.
Cistromics
Cistromics is the genome-wide mapping of transcription factor binding sites and chromatin accessibility, which has emerged as a transformative approach in elucidating the epigenetic landscape driving medication resistance in PCa (Figure 8). Cistromic reprograming, including shifts in AR binding sites and transcription factor networks, reshapes regulatory landscapes and drives therapeutic resistance in advanced prostate cancer. Genome-wide mapping of chromatin accessibility reveals altered enhancers and chromatin states that sustain tumor growth despite therapy. These insights highlight the role of chromatin dynamics in resistance and the need for novel therapeutic strategies. By capturing the regulatory interactions between transcription factors, enhancers, and chromatin states, cistromics offers a high-resolution view of how resistant phenotypes evolve under therapeutic pressure.77,81 In advanced and mCRPC, cistromic analyses have uncovered dynamic reprograming of the AR cistrome. Treatment with AR pathway inhibitors such as enzalutamide and abiraterone induces AR binding site redistribution, enhancing transcription of alternate survival genes and bypass pathways, including FOXA1, HOXB13, and MYC-regulated loci. 82 Additionally, lineage plasticity in therapy-resistant tumors is often accompanied by activation of a neuroendocrine cistrome governed by pioneer factors such as BRN2 and ASCL1, independent of AR signaling. 60
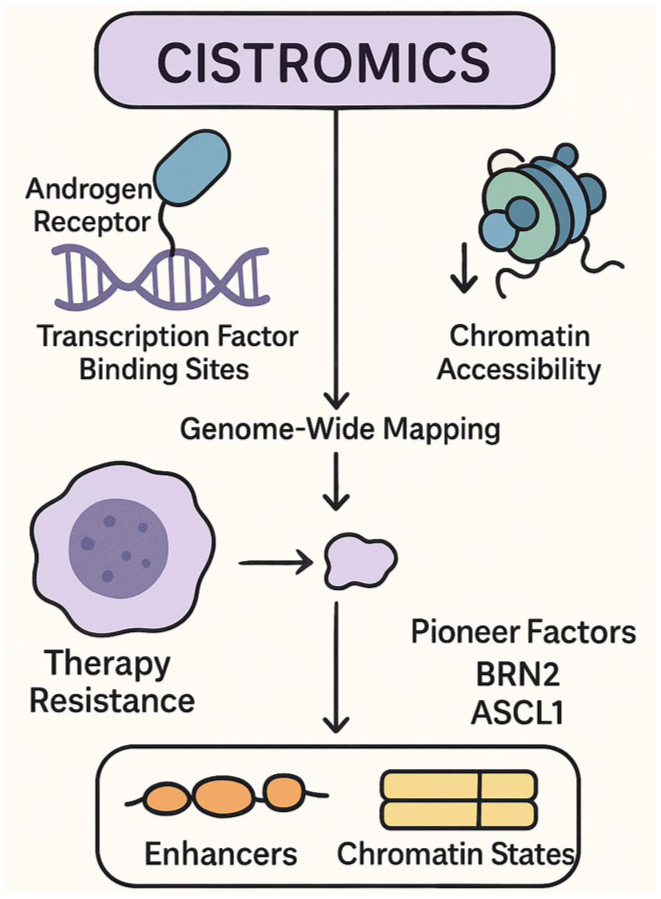
Cistromic reprograming as a driver of therapeutic resistance in advanced prostate cancer.
Clinically, cistromic profiling allows for identifying master regulators that are selectively active in resistant subtypes, facilitating patient stratification and biomarker discovery. Integrative cistrome–transcriptome analyses have enabled predictive modeling of resistance and guided therapeutic targeting of epigenetic readers like BET proteins and chromatin remodelers. 83 As single-cell and spatial historic technologies evolve, their integration into precision medicine frameworks holds promise for real-time monitoring of tumor evolution and individualized therapeutic adaptation in drug-refractory PCa.
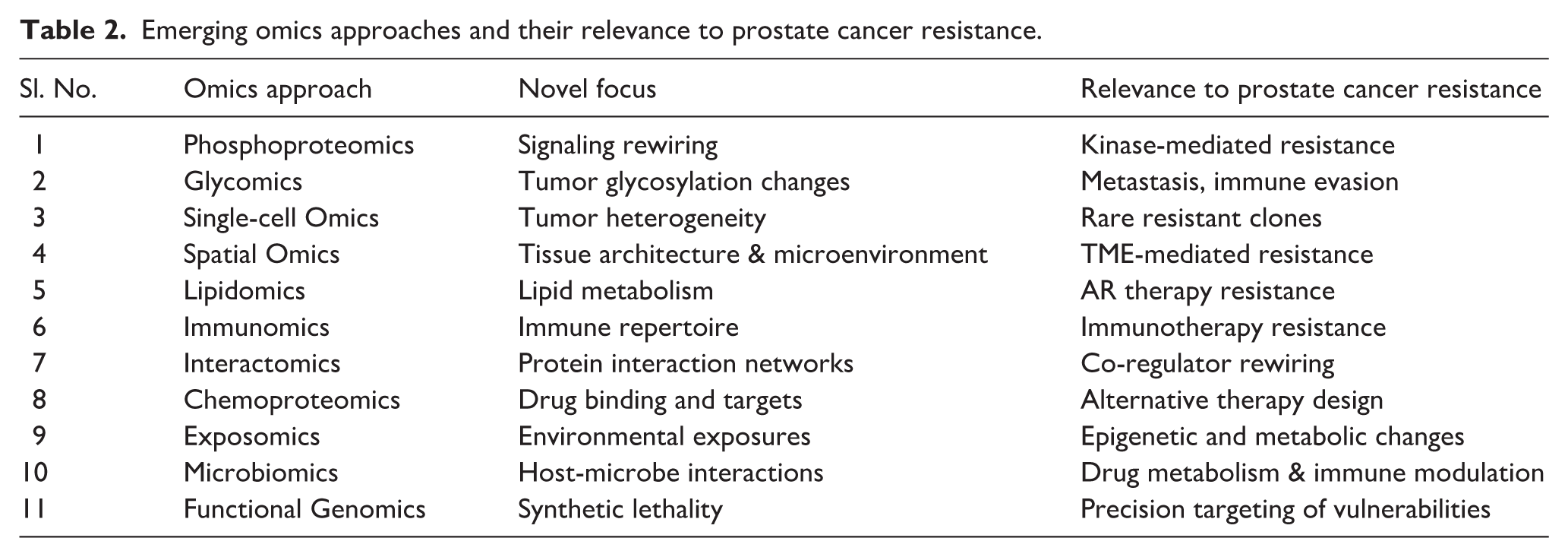
Beyond genomics, transcriptomics, proteomics, metabolomics, epigenomics, cistromics, and radiogenomics, other omics approaches like glycomics, lipidomics, microbiomics, and interactomics etc, also contribute valuable insights, as shown in Table 2. These additional layers enhance our understanding of cellular processes, disease mechanisms, and treatment responses, improving personalized medicine and precision oncology strategies.
Emerging omics approaches and their relevance to prostate cancer resistance.
Integrating multiomics to enhance drug resistance prediction and management
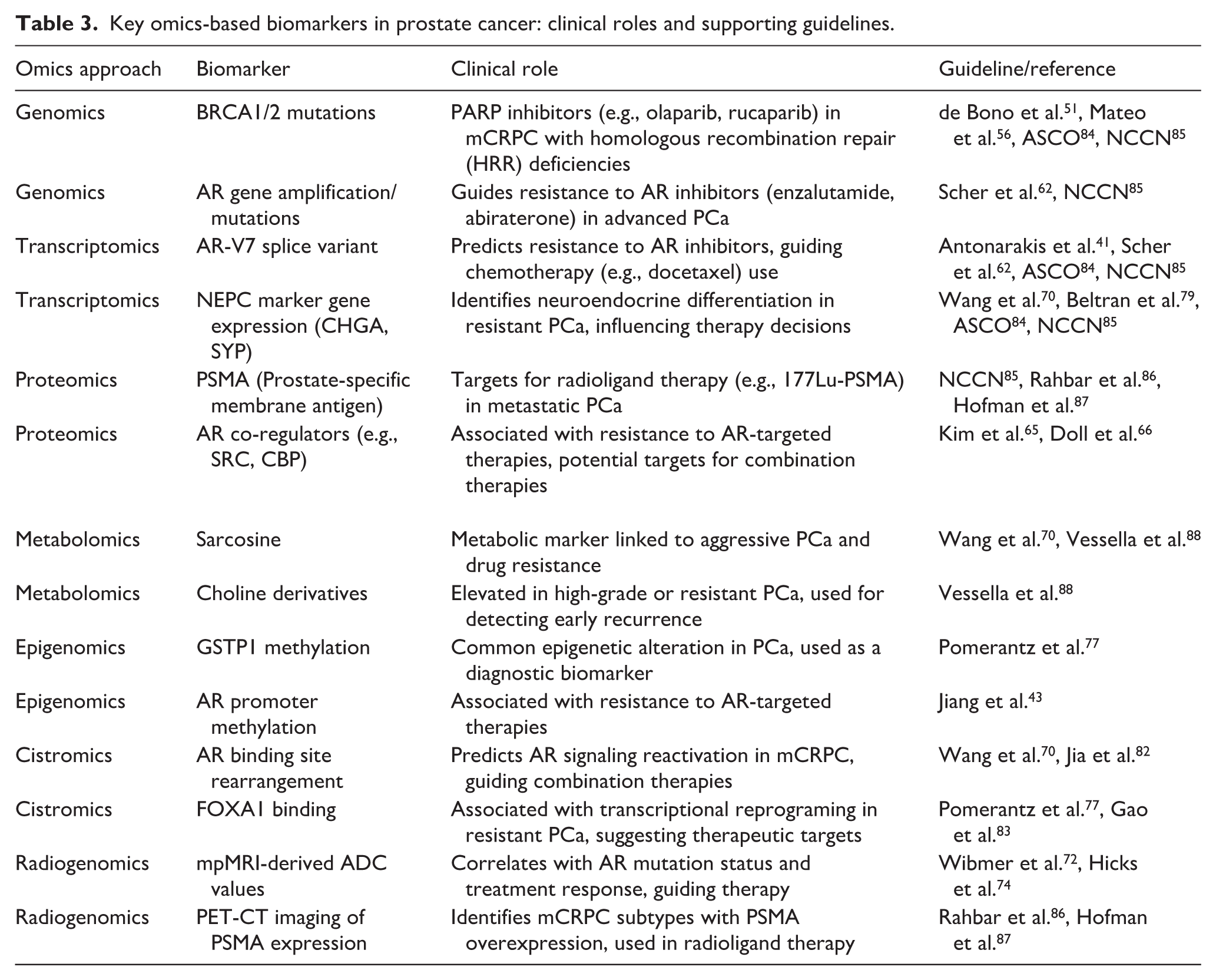
Integrating multiomics data analysis for predictive drug resistance in advanced prostate cancer represents a paradigm shift in personalized oncology. Therefore, a consolidated overview of these pivotal biomarkers, their clinical significance, and the current level of endorsement in international guidelines is very important, as shown in Table 3. In this scenario, real clinical settings will increasingly leverage high-throughput technologies, combining genomics, transcriptomics, proteomics, metabolomics, and spatial omics, alongside emerging fields like phosphoproteomics and immunomics, to decode the complexity of drug resistance. By integrating data from these diverse omic layers, a more holistic view of tumor biology can be attained, addressing the genetic, epigenetic, proteomic, and metabolic factors that drive resistance to therapies, such as androgen receptor inhibitors or chemotherapy.
Key omics-based biomarkers in prostate cancer: clinical roles and supporting guidelines.
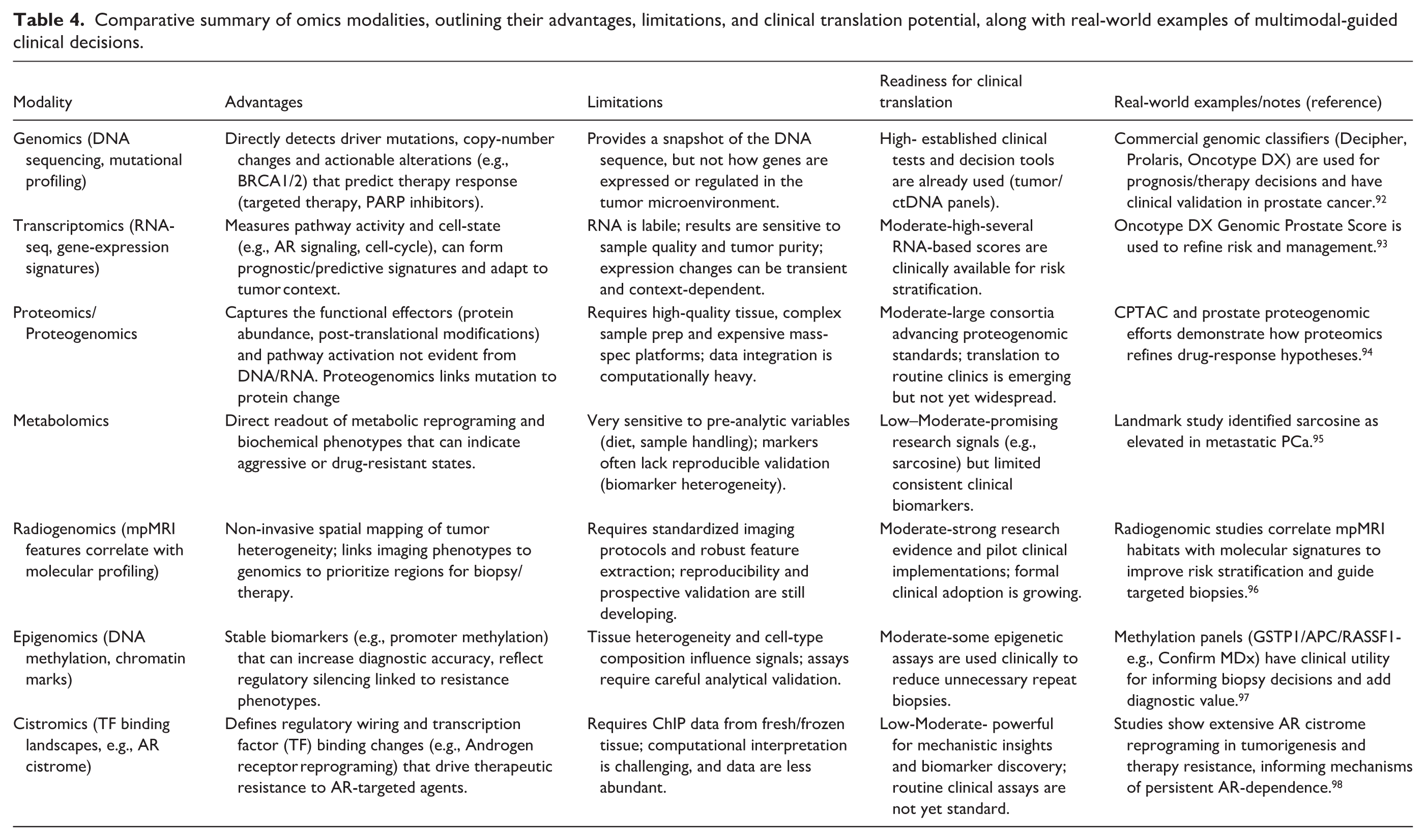
Recent studies have shown that the Prostate Cancer Model Repository generated primary patient-derived cells, including prostate cancer and benign prostatic hyperplasia samples, enabling multiomics profiling. Whole exome sequencing, RNA sequencing, and proteomics were applied to capture mutations and gene expression, providing a holistic view of tumor biology. This integrated approach using the pharmacoproteome analysis identified 14,372 significant protein-drug correlations that would benefit precision treatment for PCa. 89 In addition, advanced machine learning models, such as a deep learning-based multiomics integration model that combined genomic, transcriptomic, and clinical data, predict relapse risk in prostate cancer. 90 These models may predict drug efficacy and provide insights into adaptive resistance pathways, which are often missed in traditional approaches. Furthermore, incorporating spatial omics and single-cell technologies will allow for examining the tumor microenvironment and heterogeneity, which play crucial roles in resistance dynamics. In clinical practice, this multiomics framework will facilitate dynamic, real-time therapeutic adjustments, moving toward precision medicine that is both individualized and responsive to evolving resistance profiles, ultimately improving patient outcomes in advanced prostate cancer. Furthermore, integrating proteomics with histopathology and magnetic resonance imaging (MRI) has identified signatures linked to progression from hormone-sensitive to castration-resistant prostate cancer. This model offers prognostic insights that can guide personalized therapy and patient management. 91 Given these insights, a comparative study succinctly highlights each omics modality’s advantages, limitations, and clinical translation potential, supported by real-world examples of successful multimodal guided clinical decisions as shown in Table 4.
Comparative summary of omics modalities, outlining their advantages, limitations, and clinical translation potential, along with real-world examples of multimodal-guided clinical decisions.
Despite promising evidence, multiomics approaches face a number of challenges, including data standardization, integration complexities, and limited multicentric validation studies. Overcoming these translational bottlenecks might accelerate the translation of multiomics discoveries into actionable strategies for prostate cancer therapy.
Conclusion
The integration of multiomics approaches marks a transformative shift in unraveling the complex mechanisms underlying drug resistance in advanced prostate cancer. By converging multi-layered datasets spanning genomics, transcriptomics, proteomics, metabolomics, and epigenomics, this review underscores an emergent framework for dynamic molecular stratification, enabling ultra-early prediction of therapeutic resistance and unveiling cryptic biomarkers with clinical translatability. Beyond merely mapping static molecular snapshots, this integrative omics approach facilitates real-time trajectory modeling of tumor evolution, illuminating context-specific signaling rewiring such as aberrant androgen receptor crosstalk, PI3K-AKT-mTOR axis perturbations, and metabolic plasticity. While barriers like inter-patient heterogeneity, temporal sampling constraints, and ethnically skewed datasets remain, the convergence of systems biology, machine learning, and multiomics analytics is set to redefine the landscape of precision oncology, driving the discovery of next-generation targets and tailoring bespoke interventions for therapy-refractory prostate cancer subtypes.
Future perspectives
The future of overcoming drug resistance in advanced prostate cancer lies in the convergence of multiomics with next-generation technologies that transcend conventional boundaries of molecular profiling. As the field evolves, several transformative directions are poised to reshape how we understand, predict, and therapeutically intercept resistance phenotypes.
a. Single-Cell Multiomics and Spatial Profiling: Next-gen multiomics will transition from bulk-tissue analyses to single-cell and spatially resolved omics, enabling the deconvolution of intratumoral heterogeneity with subcellular resolution. This may uncover rare, drug-tolerant persister cells and microenvironmental niches that orchestrate resistance, allowing for earlier, spatially targeted interventions.
b. Multiomics plus AI for Predictive Modeling: Integrating machine learning and AI-driven analytics with longitudinal multiomics will generate predictive avatars of tumor evolution. These “digital twins” of prostate cancer can simulate future resistance trajectories, test therapeutic combinations in silico, and optimize real-time treatment decisions, pushing the envelope toward anticipatory oncology.
c. Integration of Liquid Biopsy-Derived Multiomics: Non-invasive platforms like liquid biopsy multiomics (cfDNA, exosomes, CTCs) will allow continuous, real-time surveillance of resistance evolution, minimizing the need for invasive tissue biopsies. When layered with machine learning, these circulating biosignatures can flag resistance onset at a preclinical stage, redefining the timing of therapeutic interventions.
d. Epitranscriptomics and Non-Coding RNA Omics: Emerging omics layers such as epitranscriptomics (e.g. m6A modifications) and non-coding RNA interactomes offer untapped potential in deciphering post-transcriptional and regulatory resistance networks. Future investigations will explore how RNA modifications, miRNA, lncRNA, and circRNA orchestrate adaptive resistance to targeted and hormonal therapies.
e. Organoid-Based Multiomics Platforms: Patient-derived organoids coupled with multiomic profiling will serve as ex vivo avatars for testing therapy responsiveness and resistance mechanisms in real-time. Integration of drug screening data with omics signatures from organoids can personalize and accelerate therapy development pipelines.
f. Inter-Omic Crosstalk and Network-Based Therapeutics: Future research will move beyond isolated omics to explore inter-omic crosstalk—how genomic, epigenomic, and metabolic aberrations co-operate in modular resistance networks. This will pave the way for network pharmacology and polypharmacological interventions designed to destabilize resistance circuits rather than single targets.
g. Equity and Omics Diversity: In this new era, equitable access to multiomics technologies and greater inclusion of diverse ethnic backgrounds in prostate cancer cohorts will be critical to generalize findings and ensure translational success across global populations.
Footnotes
Acknowledgements
We thank the Director, AIIMS-Bathinda, for valuable support. This article benefited from using OpenAI ChatGPT for preliminary literature searches and refining the schematic structure.
Author contributions
MP, SKG: Conceptualization, Review & Editing; AA, and AG: writing the original draft. Overall, all authors agreed to communicate this article for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors wish to acknowledge the Indian Council of Medical Research (ICMR), New Delhi, Government of India, for providing funding (Proposal Reference ID: 2022-03035) for Short Term Studentship (STS) fellowship to Archit Goel.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sharing does not apply to this article as no new data were created or analyzed in this study.