
Abstract
Objectives:
Achieving both relief of urinary obstruction and preservation of ejaculatory function is a key goal of modern surgical management for benign prostatic hyperplasia (BPH). However, standardized definitions of success that integrate multiple clinical domains remain limited. This study introduces a composite definition of clinical success and explores its predictors using a multicenter dataset of minimally invasive, ejaculation-preserving procedures.
Methods:
Multi-institutional data were combined, including patients who underwent urethral-sparing robot-assisted simple prostatectomy (usRASP; n = 94), Aquablation (n = 95), or Rezum (n = 308). Complete clinical success (CSS) was defined as: (1) ⩾30% International Prostatic Symptoms Score (IPSS) reduction at 12-months; (2) preserved ejaculation, based on a positive response to the Male Sexual Health Questionnaire Ejaculatory Dysfunction (MSHQ-EjD Q3); and (3) absence of ⩾Grade III Clavien–Dindo complications. Partial clinical success (PCS) was defined as the achievement of any two of the three criteria. A multivariable logistic regression analysis identified independent predictors of CCS.
Results:
The final cohort included 497 patients. CCS rates were 66.0% (usRASP), 73.6% (Aquablation), and 68.8% (Rezum); PCS rates were 28.7%, 14.7%, and 20.1%, respectively. No significant differences were observed among groups for IPSS (p = 0.455), ejaculation rates (p = 0.07), or complication rates (p = 0.445). On multivariable analysis, prostate volume < 110 mL (OR 0.52; p = 0.034), higher MSHQ-EjD Q3 (OR 1.07; p < 0.001), and shorter catheterization time (OR 0.91; p = 0.02) independently predicted CCS at 1 year.
Conclusions:
This composite endpoint offers a pragmatic and clinically relevant framework for evaluating success in minimally invasive BPH surgery. Its adoption may enhance cross-technique comparisons and inform individualized treatment strategies.
Introduction
Benign prostatic hyperplasia (BPH) is one of the most common urological conditions among aging men and accounts for a substantial portion of operative workload in daily practice. 1 Beyond relieving obstruction, modern treatment strategies increasingly aim to preserve ejaculatory function as a meaningful, patient-centered outcome.2,3 Nevertheless, ejaculatory dysfunction remains a frequent and often underreported adverse event—even after procedures promoted as minimally invasive or designed to spare sexual function.4,5 This persistent limitation highlights the need for outcome metrics that integrate both symptomatic relief and preservation of quality of life.
To date, efforts aimed at standardizing outcome reporting in BPH therapy have been limited. Published studies reflect marked procedural variability and still lack practical, consensus-based definitions of therapeutic success. The BPH6 index, introduced to capture six functional and safety domains, has seen only limited clinical integration due to its conceptual complexity and implementation demands. 6 Despite its conceptual appeal, the BPH6 index has struggled to translate into routine practice, limiting its clinical uptake. By contrast, composite endpoints have been successfully adopted in several areas of urology such as nephron-sparing surgery, radical prostatectomy and also water vapor thermotherapy where they support reproducibility and meaningful comparison among techniques pursuing similar objectives.7–9
In this setting, a multidimensional outcome measure encompassing symptom control, maintenance of ejaculation, and procedural safety may provide a clinically useful reference for evaluating and comparing treatment performance. Such a framework allows physicians and patients to interpret results in a more integrated and actionable way, moving beyond isolated metrics toward a comprehensive understanding of treatment benefit. It also facilitates comparability across interventions with varying degrees of invasiveness, an increasingly important consideration as procedural options continue to diversify.
Within this context, we propose and apply a novel composite endpoint—Complete Clinical Success (CCS)—to evaluate three contemporary ejaculation-preserving techniques for BPH: urethral-sparing robot-assisted simple prostatectomy (usRASP), Aquablation, and Rezum™ convective water vapor therapy.4,5,10 The CCS combines three clinically relevant domains: significant improvement in lower urinary tract symptoms (LUTS), preservation of ejaculatory function, and absence of major perioperative complications. In this multicenter retrospective study, we analyzed a cohort of 497 patients who underwent one of these procedures, comparing CCS rates across treatment groups and identifying independent predictors of success.
Methods
Study design and setting
This retrospective multicenter study was conducted across seven Italian urological centers, including both academic and non-academic institutions. The study period extended from July 2018 to March 2024. Institutional databases were queried to identify consecutive male patients who underwent one of three minimally invasive, ejaculation-sparing surgical procedures for symptomatic benign prostatic hyperplasia (BPH) with benign prostatic obstruction (BPO): urethral-sparing robot-assisted simple prostatectomy, Aquablation, and Rezum thermal therapy. The study protocol received formal approval from the Institutional Review Boards of all participating centers. All procedures were conducted in full compliance with the ethical standards of the Declaration of Helsinki and its later amendments.
Inclusion and exclusion criteria
Patients were eligible for inclusion if they presented with moderate-to-severe lower urinary tract symptoms (LUTS) refractory to medical therapy and completed at least 12 months of postoperative follow-up with complete clinical and functional data available.
Exclusion criteria included prior prostate surgery, diagnosis of prostate cancer, neurogenic bladder, or incomplete documentation. From the initial pooled cohort of 557 patients, 32 were excluded due to insufficient follow-up and 28 due to missing key variables, yielding a final analytic sample of 497 patients.
Baseline and preoperative variables
Collected baseline variables included:
Demographics and comorbidity: age, BMI, Charlson Comorbidity Index (CCI), ASA score.
Medication history: use of antiplatelet/anticoagulant therapy; ongoing BPH medical therapy (none, alpha-blocker monotherapy, or combination).
Prostate parameters: volume (measured by TRUS or mpMRI), median lobe presence (yes/no), PSA.
Functional status: International Prostatic Symptoms Score (IPSS), IPSS-QoL score, International Prostatic Symptoms Score Quality of Life, SHIM, Male Sexual Health Questionnaire Ejaculatory Dysfunction (MSHQ-EjD Q3; Q3 responses were dichotomized for analysis, with patients affirming the occurrence of ejaculation during sexual activity in the past 4 weeks considered to have maintained ejaculatory function [yes/no]), Qmax Uroflowmetry (Qmax), post-void residual (PVR), and history of acute urinary retention (none, single episode, or indwelling catheter).
Perioperative variables
Collected intra- and perioperative data included:
Operative time (min)
Number of vapor injections (Rezum only)
Bladder irrigation time (days)
Catheterization duration (days)
Length of hospital stay (days)
Complication rates (Clavien–Dindo classification)
Postoperative urinary retention, catheter re-insertion, 30-day readmission, and reintervention
Follow-up and outcome measures
Patients were assessed at 12 months postoperatively. The primary endpoint was Complete Clinical Success (CCS), defined as the concurrent fulfillment of:
⩾30% reduction in IPSS,
Preservation of ejaculatory function (positive response to MSHQ-EjD Q3),
Absence of Clavien–Dindo grade III or higher complications.
Partial Clinical Success (PCS) was defined as achieving two of these three criteria; Incomplete Clinical Success (ICS) as achieving only one or none.
Statistical analysis
Continuous variables were reported as medians with interquartile ranges (IQR) and compared via Kruskal–Wallis test. Categorical variables were compared using chi-square or Fisher’s exact test.
A multivariable logistic regression was built to identify predictors of CCS at 12 months. Variables with p < 0.10 at univariable analysis entered a stepwise multivariable model. Model calibration was tested with Hosmer–Lemeshow test; discrimination with the C-statistic. A two-sided p-value <0.05 was considered significant. Analyses used IBM SPSS Statistics v28.
Results
A total of 497 patients underwent one of the three ejaculation-sparing procedures: 94 usRASP (Group A), 95 Aquablation (Group B), and 308 Rezum (Group C). All outcomes were assessed at 12 months.
Baseline characteristics
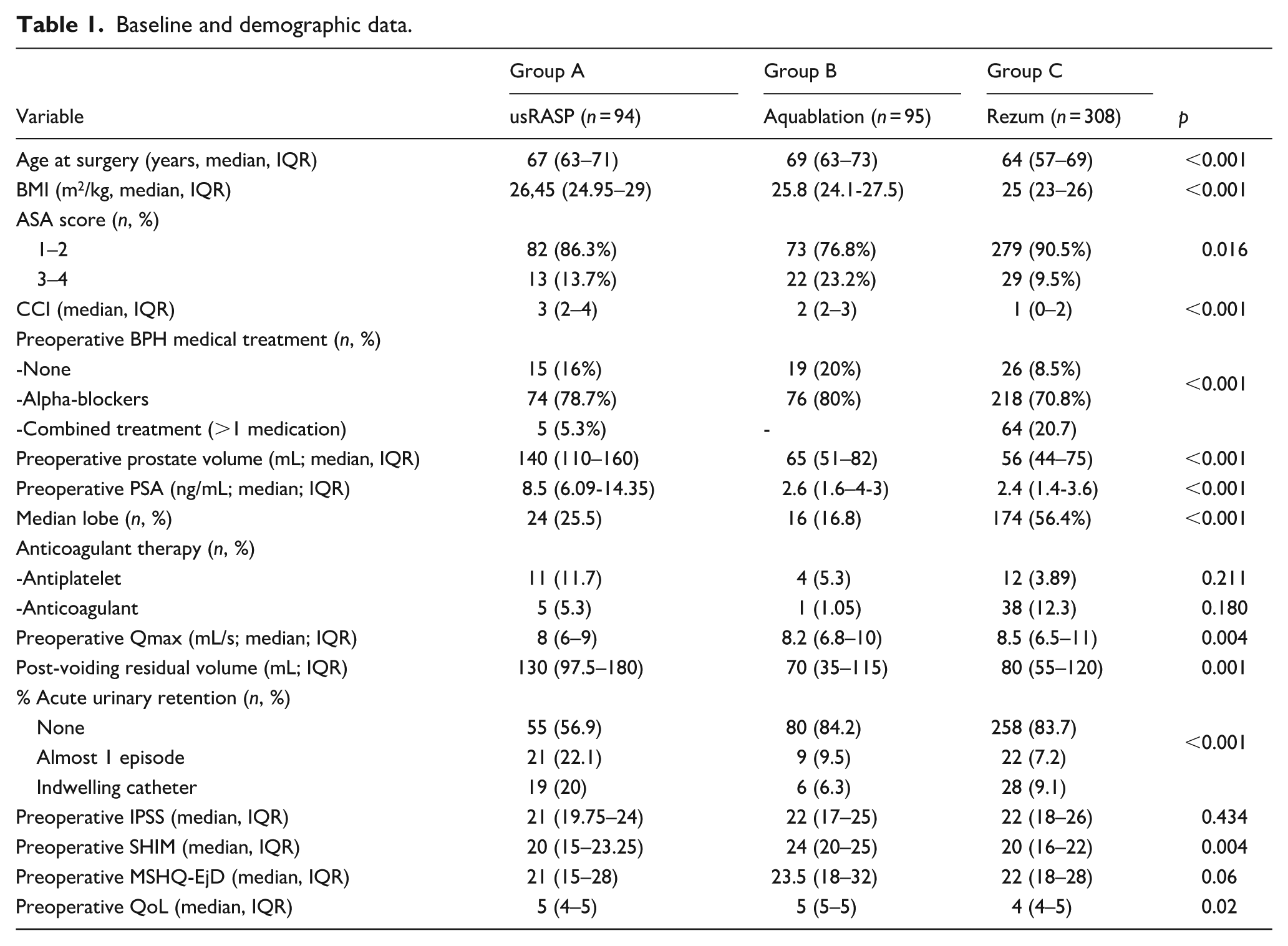
Significant intergroup differences were observed (Table 1). Rezum patients were younger (median 64 vs 67 and 69 years, p < 0.001), had lower BMI, lower CCI, and smaller prostate volume. Median lobe presence was most frequent in Group C (56.4%, p < 0.001). SHIM scores were higher in Group B (p = 0.004). IPSS was similar across groups; QoL was worse in Group C (p = 0.02). Qmax and PVR favored Group C. Prevalence of urinary retention or indwelling catheter was highest in Group A (p < 0.001).
Baseline and demographic data.
Perioperative outcomes
Operative time was longest in Group A and shortest in Group C (p < 0.001; Table 2). Catheterization duration and hospital stay followed similar patterns. Bladder irrigation was routinely performed in Groups A and B. Complication rates were highest in Groups A (14.8%) and B (15.7%) and lowest in Group C (10%) (p < 0.001). The majority of complications were Clavien–Dindo grade I and II (Table 2). Readmission rates were higher in Group A (4.3%) compared with both Group B (2.1%) and Group C (0.3%).
Perioperative outcomes.
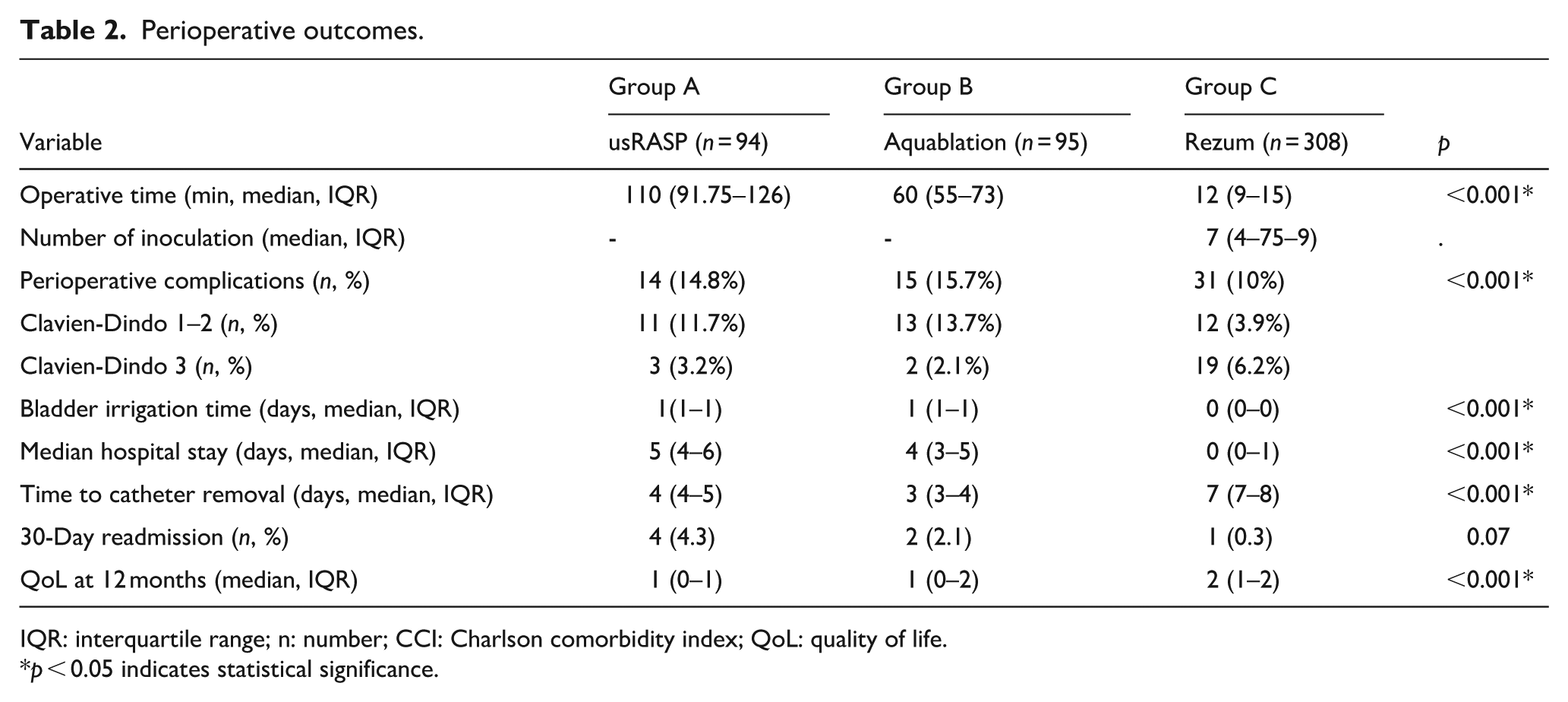
IQR: interquartile range; n: number; CCI: Charlson comorbidity index; QoL: quality of life.
p < 0.05 indicates statistical significance.
Functional and composite outcomes at 12 months
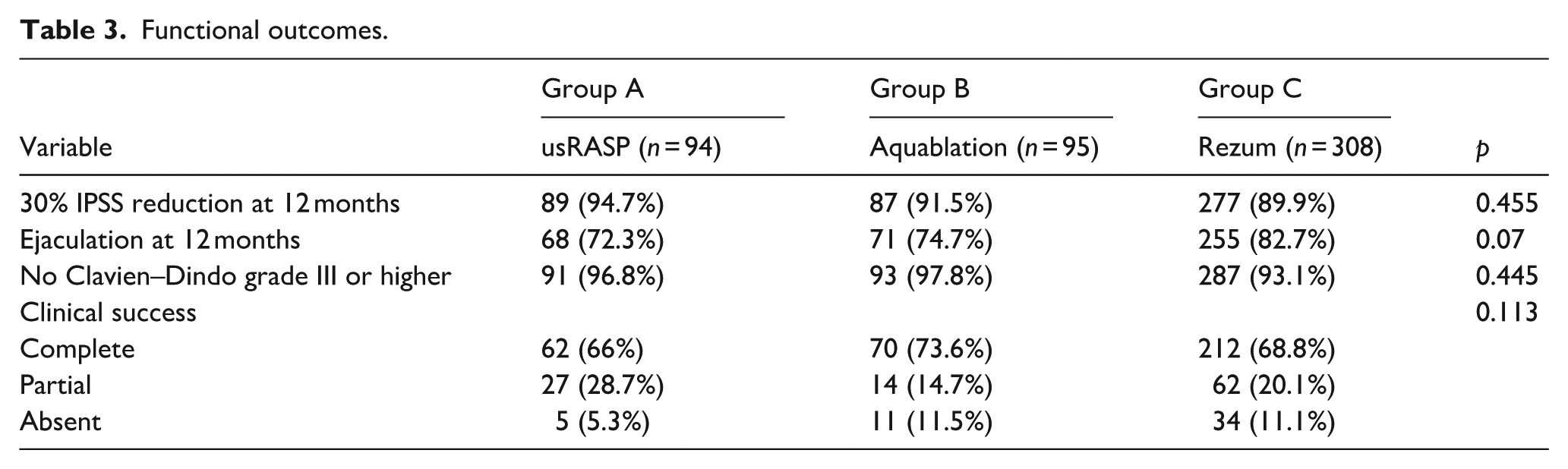
Rates of IPSS reduction ⩾ 30%, ejaculatory preservation, and absence of major complications did not differ significantly among groups (each p > 0.05). CCS was achieved in 66.0% (Group A), 73.6% (Group B), and 68.8% (Group C; p = 0.113). PCS was observed in 28.7%, 14.7%, and 20.1%; ICS in 5.3%, 11.5%, and 11%, respectively (Table 3).
Functional outcomes.
Predictors of CCS
At multivariable analysis, three independent predictors of CCS emerged (Table 4):
Univariable and multivariable logistic regression analysis to identify predictors of complete 1-yr clinical success for usRASP (n = 94), Aquablation (n = 95), and Rezum (n = 308).
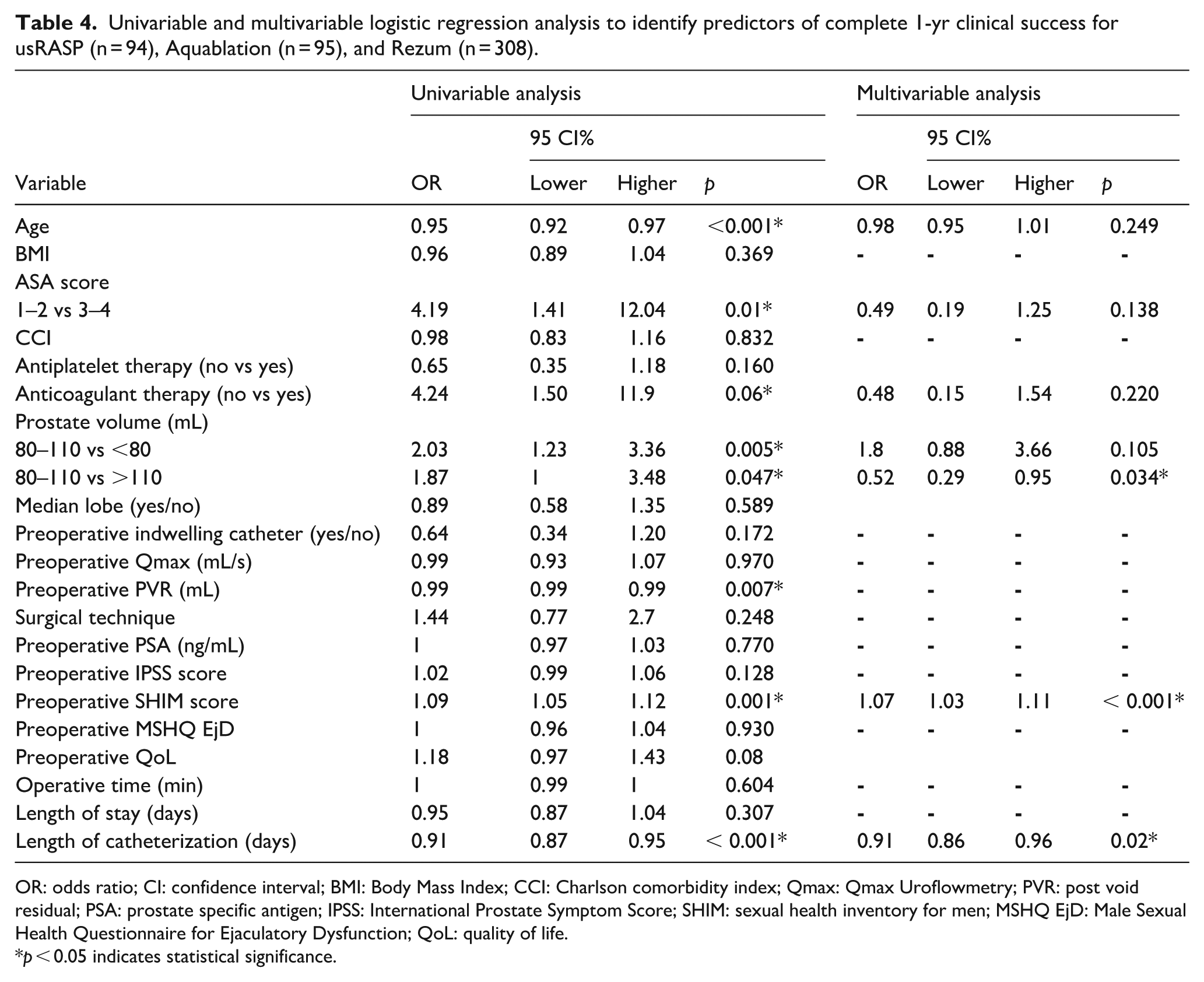
OR: odds ratio; CI: confidence interval; BMI: Body Mass Index; CCI: Charlson comorbidity index; Qmax: Qmax Uroflowmetry; PVR: post void residual; PSA: prostate specific antigen; IPSS: International Prostate Symptom Score; SHIM: sexual health inventory for men; MSHQ EjD: Male Sexual Health Questionnaire for Ejaculatory Dysfunction; QoL: quality of life.
p < 0.05 indicates statistical significance.
prostate volume < 110 mL (OR 0.52; p = 0.034)
higher baseline SHIM (OR 1.07; p < 0.001)
shorter catheterization time (OR 0.91; p = 0.02)
The model showed good calibration (Hosmer–Lemeshow p = 0.73) and excellent discrimination (C-statistic = 0.82).
Discussion
The lack of standardized, multidimensional outcome measures has posed a longstanding challenge to the interpretation and comparison of BPH interventions, particularly in the context of emerging minimally invasive techniques that differ substantially in mechanism, indication, and target population.11–13 While symptom relief remains the cornerstone of therapeutic intent, preserving ejaculatory function has gained recognition as a clinically meaningful endpoint, with a direct impact on patient quality of life.14,15 Yet, this domain remains frequently underassessed in clinical studies and is often underreported even at baseline, due in part to patients’ reluctance or failure to spontaneously disclose dysfunction in the absence of focused questioning.
In this multicenter study, we introduced and applied a pragmatic composite endpoint—Complete Clinical Success (CCS)—designed to reflect symptomatic improvement, ejaculatory preservation, and perioperative safety in an integrated manner. These three domains were selected for their clinical relevance, patient-centered value, and direct association with both therapeutic intent and procedural trade-offs. While other variables such as Qmax or QoL scores may also reflect outcome quality, they were not retained in the CCS definition to preserve interpretability, feasibility, and consistency across diverse clinical settings. The resulting metric provides a compact, functionally relevant reference point to benchmark outcomes across interventions of varying complexity and invasiveness.
Our findings showed broadly comparable CCS rates across the three techniques analyzed, suggesting that favorable global outcomes can be achieved with any of the approaches when appropriately indicated. Aquablation demonstrated the highest CCS rate (73.6% vs 66.0% and 68.8%), although the difference did not reach statistical significance. Patients undergoing usRASP had significantly larger prostates, higher comorbidity, and greater prevalence of urinary retention, indicating that this technique was more often employed in challenging anatomical or clinical scenarios. These differences likely reflect underlying treatment allocation patterns rather than intrinsic differences in efficacy.
The safety profile was acceptable across all groups, with most adverse events being minor and self-limiting. The type and frequency of complications differed significantly across modalities, in keeping with the distinct mechanisms of tissue removal or ablation. Importantly, despite the procedural diversity, the proportion of patients achieving LUTS relief and maintaining ejaculatory function was comparable among groups, underscoring the potential value of an integrated endpoint in distinguishing complete from partial or unbalanced outcomes.
Multivariable analysis identified three independent predictors of CCS: prostate volume < 110 mL, higher preoperative SHIM score, and shorter catheterization time. Although intuitive, these predictors carry significant clinical implications.
Smaller glands may facilitate efficient and precise intervention, particularly with ablative technologies. The thresholds of 80 and 110 mL were adopted to reflect clinically meaningful strata previously identified in the literature as relevant for tailoring surgical approach in patients undergoing minimally invasive therapies for BPH. Specifically, these cut-offs have been associated with significant differences in perioperative parameters and treatment efficacy, particularly for Aquablation and Rezum, whose functional outcomes and safety profiles appear to vary according to prostate volume. Their use in this study was intended to stratify the cohort based on established size-dependent therapeutic responsiveness.
Higher SHIM scores prior to surgery suggest preserved baseline sexual function, which likely favors functional preservation after surgery. This supports the notion that earlier surgical intervention, while baseline function is still preserved, may offer more favorable outcomes.
Finally, shorter catheterization time likely reflects more favorable perioperative dynamics and may serve as a surrogate marker for both procedural efficacy and minimal invasiveness.
These findings are partially consistent with earlier reports on individual functional outcomes, but to our knowledge, no prior study has evaluated these factors within a composite framework. The BPH6 index, initially developed to integrate multiple domains of success, represented an important conceptual step toward holistic outcome assessment.13,16 However, its adoption has remained limited due to methodological complexity, stringent cutoffs, and a lack of external validation across procedural types. In our experience, BPH6 could not be retrospectively applied to this cohort due to incomplete data on some of its required domains. The CCS, in contrast, was intentionally designed to retain multidimensionality while remaining compatible with routine data collection and real-world implementation. Composite outcome frameworks have already been adopted in other areas of urologic surgery where they have improved reproducibility and enhanced cross-modality comparison.17,18 Extending this paradigm to BPH surgery, where therapeutic goals are increasingly shared but procedural strategies diverge, may help harmonize outcome reporting while preserving clinical nuance. The CCS thus represents a clinically grounded and scalable tool that may complement, rather than replace, domain-specific metrics in both research and practice.
Nonetheless, our study is not without limitations. Its retrospective design inherently carries a risk of selection bias, especially regarding differential surgical indications. The three procedures analyzed were often performed in distinct clinical scenarios, making direct comparisons exploratory rather than confirmatory. The multicenter nature of the dataset, while increasing external validity, also introduces potential variability in surgical technique, postoperative management, and patient selection. Additionally, several potentially relevant clinical variables—such as prostate shape, degree of intravesical protrusion, or standardized measures of ejaculatory bother—were not available or consistently recorded. Moreover, the use of alpha-blockers prior to the interventions—reported in 70%–80% of patients across groups—represents a potential confounder, as no wash-out period was required before treatment. A further limitation is the lack of a propensity-matched analysis to account for baseline differences, such as prostate volume, age, symptom severity, or sexual function, which could have enriched the interpretative depth of our findings. However, the available sample size within each treatment group did not allow for statistically robust comparisons without compromising analytical integrity. Given the retrospective and exploratory design of the study, we opted to preserve statistical power across the primary comparative endpoints.
Despite these limitations, our study also has important strengths. It represents one of the largest real-world multicenter comparisons of contemporary ejaculation-sparing BPH interventions, all evaluated through a unified, clinically anchored endpoint. The CCS was designed to strike a balance between multidimensionality and usability, favoring clarity and interpretability over excessive granularity. The inclusion of both ablative and resective approaches—performed by different surgeons across heterogeneous centers—enhances generalizability and provides a realistic snapshot of current practice patterns. A further limitation of this study is the lack of a matched comparison between surgical techniques. Although our analysis aimed to identify predictors of CCS, the absence of a matched-pair design may have introduced residual confounding related to differences in baseline characteristics and case selection. A more homogeneous comparison between techniques could provide more accurate insights into the true predictors of CCS and should be considered in future prospective studies.
Ultimately, the application of composite outcome measures such as CCS may support more individualized and context-sensitive surgical decision-making. Rather than suggesting one-size-fits-all solutions, this framework offers a shared evaluative language that can guide clinicians in matching procedural profiles to patient expectations and clinical anatomy. From a surgical perspective, such tools may help frame a more explicit discussion of procedural trade-offs and support shared decision-making processes that align therapeutic strategy with individual values, functional priorities, and net clinical benefit. 19
This study introduces and validates a clinically relevant, multidimensional definition of Complete Clinical Success (CCS) in the setting of ejaculation-preserving BPH surgery. By integrating symptomatic relief, functional preservation, and perioperative safety into a unified outcome measure, the CCS framework enables robust comparison across heterogeneous minimally invasive techniques and offers a pragmatic tool for both retrospective evaluation and prospective benchmarking. Our findings highlight that, regardless of surgical modality, prostate volume and baseline sexual function remain pivotal in determining the likelihood of achieving global success at 1 year. These parameters should be carefully considered during preoperative counseling and individualized treatment planning. The proposed CCS may help bridge the gap between surgical heterogeneity and shared therapeutic goals, supporting a more tailored, patient-centered approach to BPH management. Future prospective studies are warranted to validate its applicability and to assess its potential role in clinical decision algorithms.
Footnotes
Acknowledgements
None.
Consent to participate
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.