
Abstract
Objective:
To evaluate how standard operating procedures (SOPs), modification in puncture techniques, advancements in preoperative imaging to better understand calyceal anatomy have revitalized standard percutaneous nephrolithotomy (PCNL) for large kidney stones (>2.5 cm).
Methods:
At our center, renal stones are managed with extracorporeal shock wave lithotripsy (ESWL), percutaneous nephrolithotomy (PCNL), and retrograde intrarenal surgery (RIRS) according to stone characteristics and patient profile. Renal stones larger than 2.5 cm are managed with standard PCNL. In this retrospective study patients undergoing standard PCNL at a tertiary healthcare center from January 2018 to December 2023 having complete records were included. Data on demographics, stone characteristics, operative details, and outcomes were assessed using SPSS v26, with ethical approval ensuring confidentiality.
Results:
A total of 766 patients were included. Mean age was 43.75 ± 16.0 years; 69.7% were male. Mean stone size was 3.8 ± 1.2 cm, with 46.7% complex (Guy’s Stone Score [GSS] ⩾ 2). Using a 24 ± 3 Fr sheath and 1.3 tracts per procedure, operative time averaged 92.5 ± 20.3 min. Stone clearance was 91.3%, with significant intraoperative bleeding (requiring transfusion) in 1.7%. Overall complication rate was 16.4%, and hospital stay averaged 3.6 ± 1.2 days; 8.7% required additional interventions, including RIRS in 44.3% of those cases.
Conclusion:
Modern standard PCNL achieves high clearance (91.3%) with minimal morbidity, reaffirming its role for large stones despite mini-PCNL’s rise.
Introduction
Nephrolithiasis, affecting 5%–15% of the global population, remains a significant challenge, particularly in regions with high stone burdens where large, complex calculi (>2.5 cm) predominate. 1 Since its introduction in 1980, standard percutaneous nephrolithotomy (PCNL) with 24–30 French (Fr) sheaths has been the gold standard for such stones, outperforming extracorporeal shock wave lithotripsy (ESWL) and ureteroscopy (URS) in clearance rates. 2 Early iterations of the procedure were associated with significant complications, including blood transfusion rates of up to 14%. 3 This prompted the development of smaller, less invasive alternatives, such as mini-PCNL (14–20 Fr). 4
Yet, standard PCNL has undergone a profound evolution, driven by innovations in endoscopic equipment, preoperative CT imaging, deeper understanding of calyceal anatomy and modifications in the initial puncture. These advancements have reduced blood loss, minimized the number of punctures, lowered transfusion needs, improved clearance rates, postoperative pain management, and intraoperative endoscopic vision. 5 Initial challenges, such as a splenic injury during tract dilation in an early left-sided PCNL case, prompted the creation of SOPs to minimize morbidity. At the start of our program in one patient of left sided PCNL, tract dilation was through the spleen, then we made SOPs to make standard PCNL a procedure with minimal morbidity. At a tertiary healthcare center with a high prevalence of large stone burden, these improvements underscore standard PCNL’s enduring relevance. This study examines how these developments have transformed standard PCNL into a safer, more effective option, challenging the narrative of mini-PCNL’s supremacy. 6
Materials and methods
This retrospective study assessed the outcomes of standard percutaneous nephrolithotomy (PCNL) performed at a tertiary care center in Western Rajasthan, India, from January 2018 to December 2023. The research was conducted with ethical approval from the Institutional Review Board (IRB approval number: AIIMS/IEC/2025/5165), ensuring adherence to the Declaration of Helsinki and strict patient confidentiality protocols.
The study enrolled patients who met specific inclusion criteria: renal stones ⩾ 2.5 cm confirmed by computed tomography (CT) scan, complete medical records, and treatment with standard PCNL within the study period. Patients undergoing alternative procedures (such as supine PCNL, extracorporeal shock wave lithotripsy (ESWL), retrograde intrarenal surgery (RIRS), or laparoscopic-guided PCNL for ectopic kidneys) were excluded. Patients with ectopic or pelvic kidneys were excluded, as they underwent laparoscopic-guided PCNL or RIRS. Additionally, individuals with incomplete documentation or those treated outside the specified timeframe were not included.
Our center use hospital information system (HIS) where evaluation of renal stone disease (RSD) patients includes a detailed history, comorbidities, and prior interventions (e.g. ureteroscopy, previous PCNL). A comprehensive physical examination is followed by baseline investigations, including complete blood count (CBC), renal function tests (serum creatinine, estimated glomerular filtration rate), urine analysis (microscopic examination and culture sensitivity), X-ray of the kidneys, ureters, and bladder (X-ray KUB), and ultrasonography of the kidneys, ureters, and bladder (USG KUB) with full bladder. A CT urogram is performed unless contraindicated in nearly all cases, except for small lower ureteric stones. Abbreviated stone work up including intact parathyroid hormone (iPTH), serum calcium, venous blood gas (VBG) are performed before surgery and 24-h urinary work up in follow up period at 4 weeks post tube free status. Stone density (Hounsfield units) was not routinely assessed in this study due to focus on size and complexity via GSS.
Once work up is complete treatment options are discussed with the patient and RSD size > 2.5 cm offered standard PCNL as our center lacks mini-PCNL facilities. The PCNL procedure adheres to a standardized protocol at our center, typically conducted under general anesthesia. All procedures were performed within a high-volume tertiary urology unit at AIIMS Jodhpur, India. Senior urology residents served as primary surgeons for the majority of cases. All procedures were performed under the direct supervision of attending urological faculty (Assistant Professors, Associate Professors, and Professors), each with more than 10 years of PCNL experience and individually having performed over 200 PCNL procedures. Faculty members actively participated in all key operative steps, including initial renal puncture, tract dilation, and stone retrieval, particularly in complex cases (GSS ⩾ 2) and supracostal punctures. This study thus reflects the outcomes of an established multi-surgeon institutional program with consistent SOPs applied across the entire team, rather than the results of a single surgeon.
Before surgery every patient’s CT Urogram/NCCT KUB is viewed on RadiAnt DICOM viewer to look at stone burden, pelvicalyceal system (PCS) anatomy and relationship to adjacent viscera in axial, coronal and sagittal sections to plan PCNL tract/tracts. After general anesthesia, a ureteric catheter is placed in the supine position (Figure 1(a)), and then the patient is made prone with two bolster supports and a 10° head-low table setting. PCS was delineated using contrast (diatrizoate meglumine and diatrizoate sodium 76% with concentration of 1:1) followed by air in 5 ml increments, and fluoroscopy was used to take the desired puncture (Figure 1(b)). In our SOPs, the preferred puncture is the superior posterior calyceal puncture, and dilatation with Alken/fascial dilators, depending on the surgeon’s choice, reaches 24–30 Fr depending on stone burden. A 22 Fr 30° nephroscope was used to view the stones. Three lithotripters are available; depending on the surgeon’s choice, pneumatic, ultrasonic lithotripter, or 100 W Ho LASER are used. In special situations like infected stones or stones impacted at PUJ/upper ureter, ultrasonic lithotripsy was used. After completion of the procedure, stone clearance was ensured by endoscopy and fluoroscopy contrast pyelogram (Figure 1(c)). In case of residual fragments that could not be approached, a flexible nephroscope (16.5 Fr) was used to re-review these stones, though the success rate was low, nearly 40%. Ureteric stent (Figure 1(d)) and/or PCN tube (Figure 2) were placed depending on the case and surgeon’s preference. In case of supracostal puncture, communication with the anesthetist was made to rule out urinothorax, and if detected, a chest tube was placed. Postoperative management includes vigilant monitoring for complications, effective pain control, and next-day imaging (such as X-ray KUB, USG, or NCCT KUB) to evaluate stone clearance and ensure procedural success.
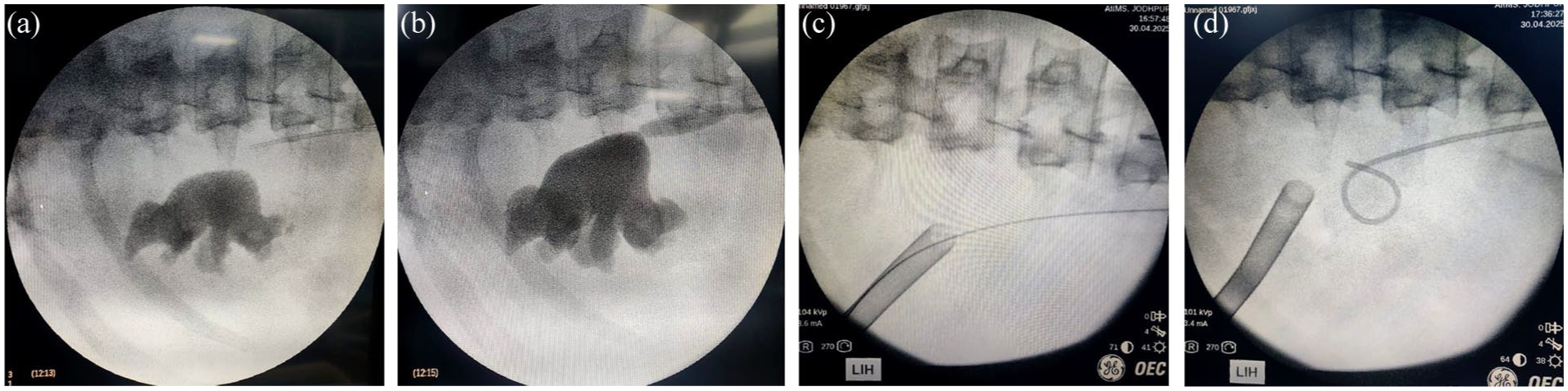
Fluoroscopic images during percutaneous nephrolithotomy: (a) Retrograde ureteric catheter placed with the patient supine prior to prone positioning, (b) Puncture of the desired calyx under fluoroscopic guidance after opacification of the pelvicalyceal system with contrast and air, (c) Fluoroscopic contrast pyelogram confirming stone clearance after completion of lithotripsy, and (d) Placement of a ureteric stent at the end of the procedure.
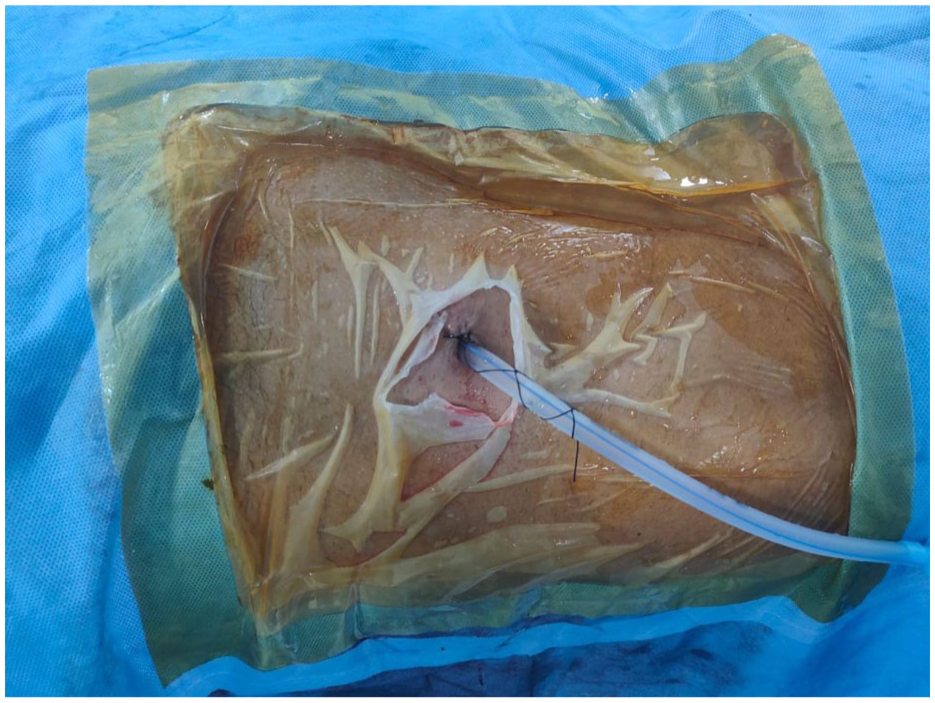
Showing placed nephrostomy tube post completion of PCNL
Data were collected from medical records, covering demographics (age, gender, comorbidities like hypertension, diabetes, and hyperlipidemia, and BMI), stone characteristics (size, location in the upper, mid, or lower pole, complexity defined as Guy’s Stone Score [GSS] ⩾ 2, and anatomic abnormalities), surgical parameters (sheath size, number of tracts, operative time, intraoperative complications such as bleeding, transfusion needs, chest tube placement and postoperative outcomes (stone clearance defined as residual fragments ⩽ 3 mm on X-ray), complications, pain score on the Numeric Rating Scale [NRS] from 0 to 10 at 24 h, hospital stay duration, and additional interventions like RIRS or ESWL). After ensuring complete clearance or non-obstructive fragment is there and planned for adjunct procedure like ESWL, nephrostomy tube was removed after clamping it for 4 h and per urethral catheter on next day. Statistical Analysis: All data were analyzed using IBM SPSS Statistics, Version 26.0 (IBM Corp., Armonk, NY, USA). As this was a single-arm descriptive study without a comparative control group, inferential statistical tests were not applied. Continuous variables with approximately normal distributions are presented as mean ± standard deviation (SD); non-normally distributed continuous variables are reported as median with interquartile range (IQR). Categorical variables are reported as absolute frequencies and percentages. Stone complexity was stratified using the Guy’s Stone Score (GSS), with GSS ⩾ 2 classified as complex. Perioperative complication severity was graded using the Modified Clavien-Dindo classification system. Stone-free status was defined radiologically as the absence of residual fragments greater than 3 mm on postoperative imaging (X-ray KUB, USG KUB, or NCCT KUB).
Results
Patient demographics
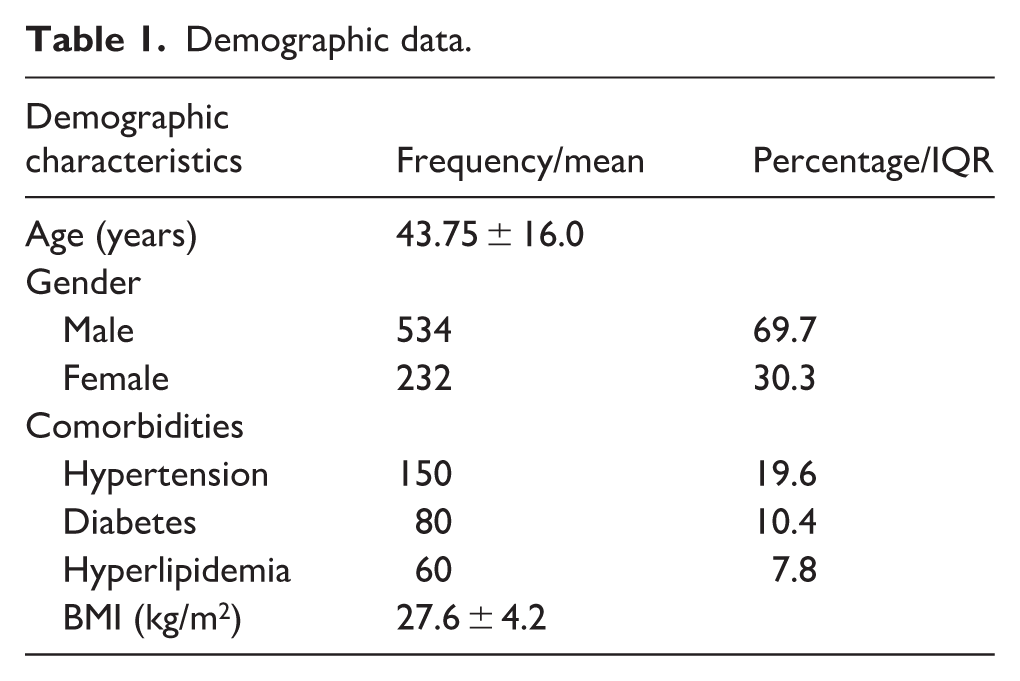
The demographic characteristics of the 766 patients are summarized (Table 1). The mean age was 43.75 ± 16.0 years, with a gender distribution of 534 males (69.7%) and 232 females (30.3%). Comorbidities were prevalent, with hypertension affecting 150 patients (19.6%), diabetes 80 patients (10.4%), and hyperlipidemia 60 patients (7.8%). The mean body mass index (BMI) was 27.6 ± 4.2 kg/m2 (Table 1).
Demographic data.
Stone characteristics, surgical details, and postoperative outcomes
Stone characteristics, surgical details, and postoperative outcomes for the 766 patients are presented (Table 2). The mean stone size was 3.8 ± 1.2 cm, with stones located on the right side in 454 cases (59.3%) and on the left in 312 cases (40.7%). Stone locations included the upper pole in 250 cases (33.3%), mid pole in 350 cases (46.7%), and lower pole in 166 cases (20.0%). Prior urinary diversion by PCN or DJ stenting was present in 243 patients (31.7%), and chronic kidney disease (CKD) was noted in 193 patients (25.2%). Anatomic kidney abnormalities were identified in 48 patients (6.3%), including horseshoe kidney (14), ectopic kidney (7), mal-rotated kidney (11), and pelvic kidney (15). However, patients with ectopic kidney (7) and pelvic kidney (15) were excluded from the study as they underwent laparoscopic-guided PCNL or RIRS. The included abnormalities were horseshoe kidney (14; 56%) and mal-rotated kidney (11; 44%). Stones were classified as simple (GSS < 2) in 400 cases (53.3%) and complex (GSS ⩾ 2) in 366 cases (46.7%; Tables 2 and 3).
Stone characteristics, surgical details, and postoperative outcomes.
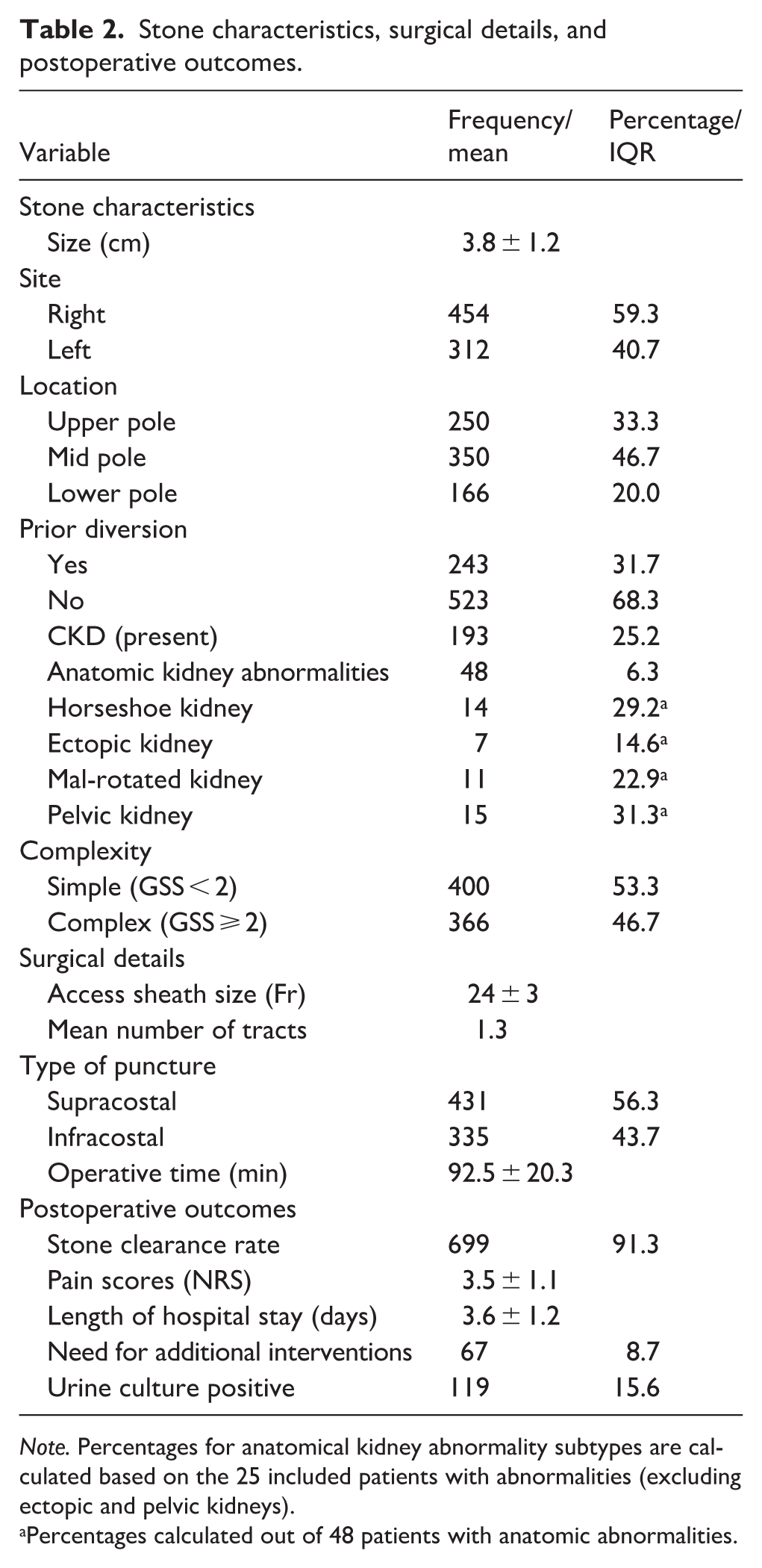
Note. Percentages for anatomical kidney abnormality subtypes are calculated based on the 25 included patients with abnormalities (excluding ectopic and pelvic kidneys).
Percentages calculated out of 48 patients with anatomic abnormalities.
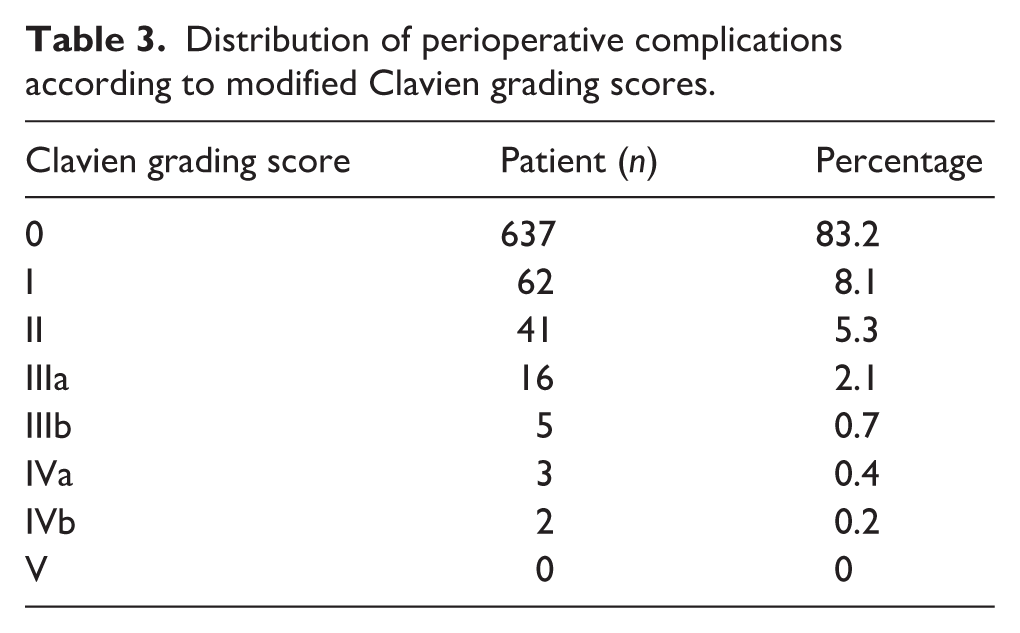
Distribution of perioperative complications according to modified Clavien grading scores.
Surgical details indicated a mean sheath size of 24 ± 3 Fr, with an average of 1.3 tracts per procedure. Puncture approach was supracostal in 431 cases (supra 12, supra 11 and supra 10; 56.3%) and infracostal in 335 cases (43.7%). The mean operative time was 92.5 ± 20.3 min. Stone clearance rate was 91.3% (699 patients). The mean pain score on the Numeric Rating Scale was 3.5 ± 1.1, and the mean hospital stay was 3.6 ± 1.2 days. Additional interventions were required in 67 patients (8.7%), including ESWL in 17 cases (25.4%), RIRS in 30 cases (44.3%), and re-PCNL in 20 cases (30.3%). Urine culture was positive in 119 patients (15.6%; Table 2).
Complications
Complications occurred in 126 patients (16.4%), classified by the Modified Clavien Grading System:
Grade 0: 637 patients (83.2%), no complications.
Grade I: 62 (8.1%), minor issues (e.g. fever, mild pain managed conservatively).
Grade II: 41 (5.3%), bleeding requiring transfusion (13, 1.7%), urinary tract infections needing antibiotics.
Grade IIIa: 16 (2.1%), Intercostal drainage for urinothorax (4, 0.5%), DJ stent repositioning (2, 0.3%), bedside bladder clot evacuation (1, 0.1%).
Grade IIIb: 5 (0.7%), angioembolization for bleeding (5, 0.7%).
Grade IVa: 3 (0.4%), urosepsis requiring ICU care (subset of 21 total cases, 2.8%).
Grade IVb: 2 (0.2%), severe complications requiring prolonged ICU stay.
Grade V: 0 (0%), no mortality.
Intraoperative bleeding, defined as visible hemorrhage during tract dilation, stone fragmentation, or nephroscope manipulation, occurred in 52 patients (6.8%), with 13 (1.7%) classified as significant (requiring transfusion).
Discussion
Standard percutaneous nephrolithotomy (PCNL) has undergone a remarkable transformation over the past four decades, evolving from a procedure fraught with risks to a highly refined technique that capitalizes on technological innovation and anatomical mastery. This evolution is vividly illustrated in our retrospective analysis of 766 patients at a tertiary healthcare center. Early in our program, a case of splenic injury during tract dilation in left-sided PCNL highlighted the need for enhanced protocols, leading to the development of standardized operating procedures (SOPs) that significantly reduced morbidity in subsequent cases. We implemented standardized operating procedures (SOPs) to manage these patients. These protocols led to a decrease in transfusion rates to 1.7%, reduced the average number of punctures to 1.3, and achieved a stone clearance rate of 91.3%. These outcomes reflect a broader historical shift from early challenges to modern precision, reaffirming standard PCNL’s dominance in managing large renal stones (>2.5 cm). In its formative years, standard PCNL was a pioneering yet perilous endeavor. Stoller et al. 3 reported transfusion rates as high as 14% and blood loss averaging 407 mL in a cohort of 127 patients, with clearance rates plateauing at 87%. Surgeons often relied on multiple punctures (>2 in complex cases), guided by rudimentary plain X-rays and early fluoroscopy, which provided scant anatomical detail. Operative times frequently exceeded 90 min due to the limitations of ballistic lithotripters, and complication rates soared above 25%, with hospital stays stretching to 5–6 days. 7
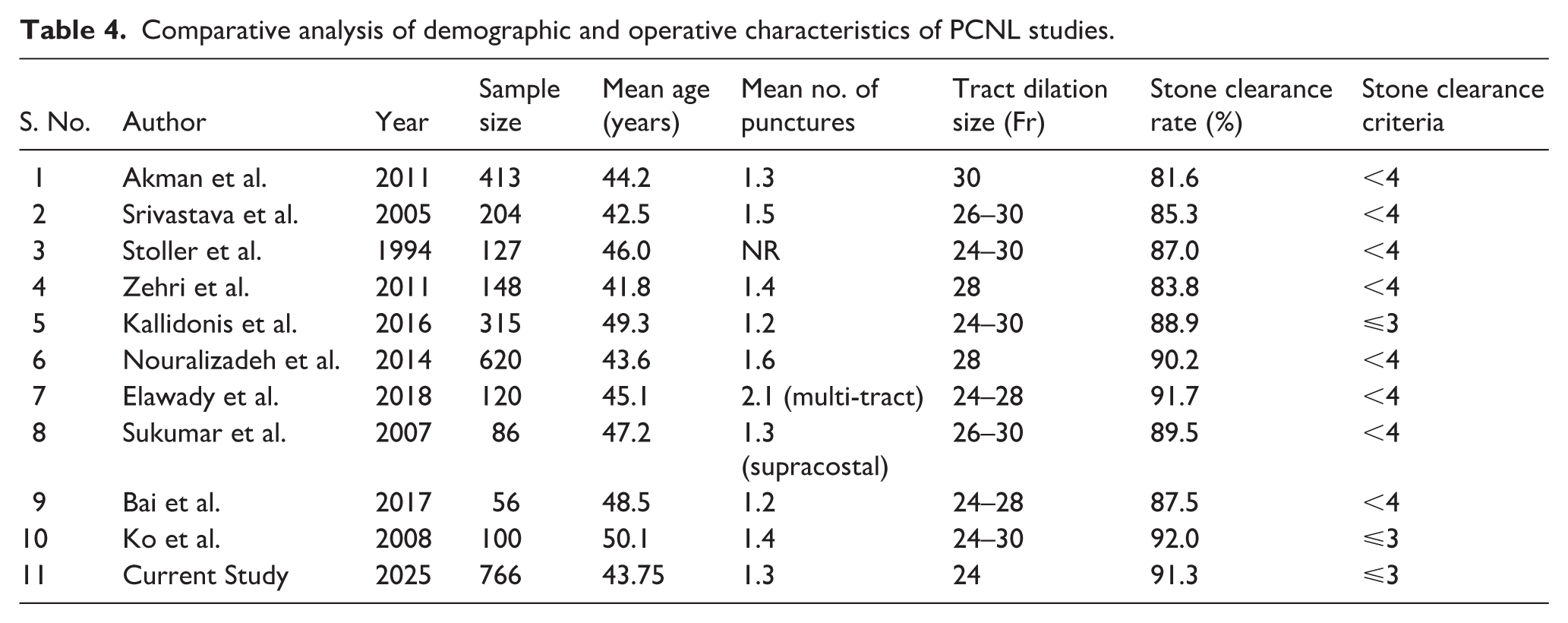
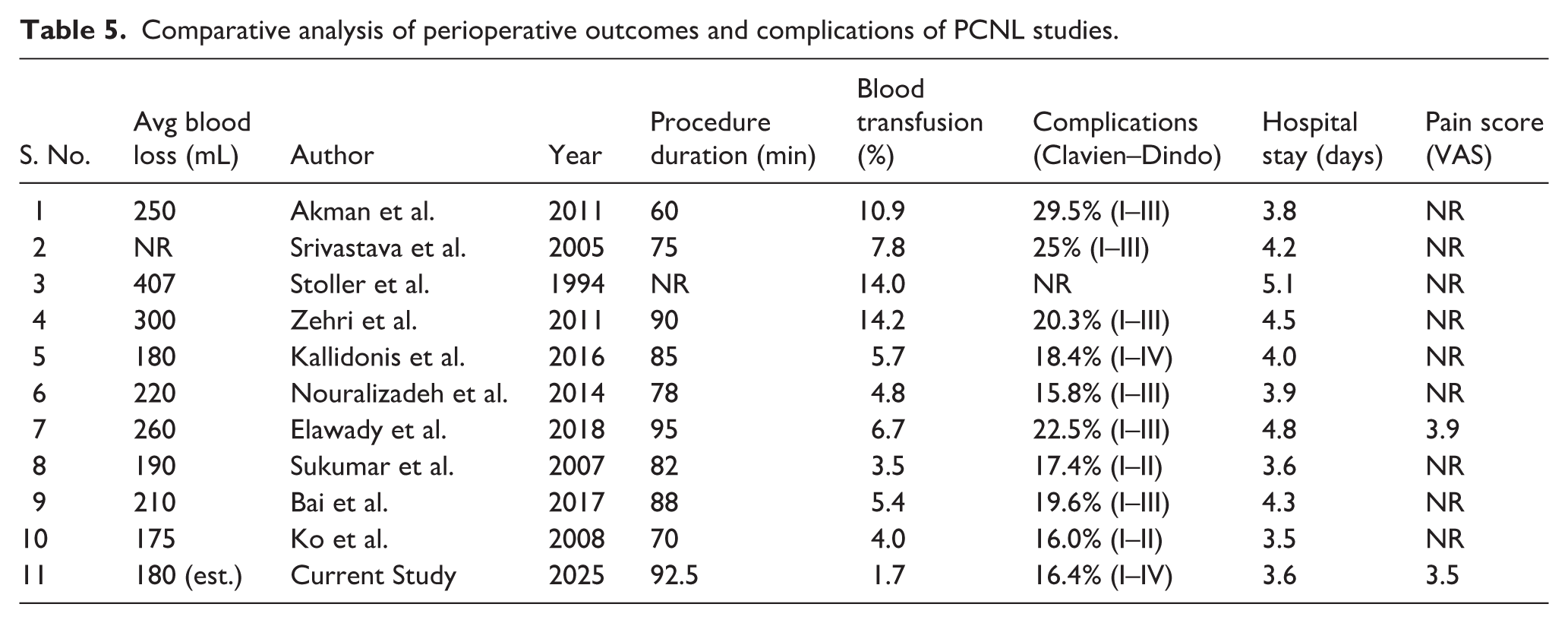
A comparative overview of key outcomes from selected studies over time, including our current series, is presented in Tables 4 and 5. This table demonstrates the progressive improvement in transfusion rates, complication rates, stone-free rates, and hospital stay lengths as techniques, imaging, and lithotripsy options have evolved.
Comparative analysis of demographic and operative characteristics of PCNL studies.
Comparative analysis of perioperative outcomes and complications of PCNL studies.
The comparison with mini-PCNL, while narrative in earlier literature, is supported by contemporary studies. Mini-PCNL offers advantages such as shorter hospital stays (1.5–2.3 days) and lower morbidity for stones 10–30 mm, with stone-free rates (SFR) of 80%–95% in recent series.8 –10 For example, a prospective study reported 95.5% SFR for 10–30 mm stones with mini-PCNL, but often requires multiple stages for complex burdens. 11 In contrast, our standard PCNL achieved 91.3% clearance for larger, complex stones (>2.5 cm, 46.7% GSS ⩾ 2), with comparable complication rates. A meta-analysis by Mantica et al. 12 comparing PCNL to laparoscopic and robotic approaches highlights that standard PCNL remains effective for high-burden calculi, though mini-PCNL may be preferable in select cases. However, our center lacks mini-PCNL facilities, limiting direct comparison. While mini-PCNL may offer shorter stays for smaller stones,8,9 our results demonstrate standard PCNL’s superiority for complex burdens (>2.5 cm), though direct head-to-head comparison is limited by our center’s lack of mini-PCNL facilities. 13
The advent of ultrasonic and laser lithotripsy, paired with 24–30 Fr sheaths, has boosted clearance rates and reduced operative times. 2 The larger sheath size, once a liability for bleeding, now enhances intraoperative visibility and instrument maneuverability, a benefit Sukumar et al. 14 confirmed with an 89.5% clearance rate in 86 supracostal cases. Preoperative CT imaging has revolutionized access planning, reducing transfusion rates to 1.7% in our cohort.7,15 Our use of air+contrast pyelogram for initial puncture and fewer punctures (1.3 average) aligns with modern series.16 –18 A key advancement in modern standard PCNL is the increased utilization of supracostal punctures, employed in 56.3% of our cases (431/766). This approach has significantly improved outcomes by enhancing safety and efficacy, particularly for upper pole stones (33.3% of our cohort). Historically, supracostal punctures were associated with pleural complications; Sukumar et al. 14 cited a 3%–5% rate of hydrothorax requiring intervention. However, preoperative CT has transformed this landscape by enabling surgeons to map the pleural cavity, diaphragm position, and upper pole calyceal anatomy with unprecedented accuracy. In our study, this precision reduced pleural complications to a mere 0.5% (4 cases requiring intercostal drainage), with no instances of pneumothorax or significant lung injury. This safety profile is a testament to CT-guided planning, which allows puncture sites above the 12th rib to skirt the lung fields and diaphragm, often performed under controlled expiration to further minimize risk. Beyond safety, supracostal access provides a straight-line trajectory along the renal axis, reducing the need for excessive nephroscope angulation or torque, maneuvers that historically increased mucosal trauma and bleeding. This alignment enhances stone fragmentation efficiency, as the lithotripter can target upper calyceal and staghorn calculi with minimal resistance, contributing to our 91.3% clearance rate. Moreover, supracostal puncture facilitates access to the upper ureter and adjacent calyces through a single tract, reducing the need for multiple punctures, a common necessity in infracostal approaches for complex stones. In contrast, infracostal punctures for lower calyceal stones (20.0% of our cohort) pose unique challenges, particularly in female patients (30.3% of our sample). The wider pelvic structure and prominent hips in females can impede nephroscope maneuvering, as the instrument’s angle is constrained by the iliac crest and soft tissue, often requiring additional torque or repositioning. This difficulty contributed to longer operative times in some cases and underscores the need for tailored approaches based on patient anatomy. In our series, the overall average of 1.3 punctures, even with 46.7% complex cases (GSS ⩾ 2), highlights the versatility of combining supracostal and infracostal techniques. Intraoperative use of flexible nephroscope also has its own limitations, such as poor field and angle, which make entry to parallel calyces challenging, with a success rate of nearly 40% in our series. For patients with large upper pole burdens, supracostal access shortens operative time by streamlining stone retrieval. Our mean of 92.5 min compares favorably to historical benchmarks and reduces residual fragments, lowering the 8.7% rate of additional interventions (e.g. RIRS in 44.3% of those cases). Anecdotally, surgeons in our center report improved ergonomic ease, as the supracostal angle aligns naturally with the operator’s stance in prone positioning, potentially reducing fatigue in lengthy procedures. These benefits, grounded in anatomical optimization, position supracostal puncture as a cornerstone of standard PCNL’s resurgence, challenging the perception that smaller tract techniques like mini-PCNL are inherently superior. Additionally, our use of mix-and-match lithotripters combining pneumatic, ultrasonic with suction, and laser technologies optimizes stone fragmentation efficiency. Ultrasonic lithotripsy excels at clearing large stone volumes rapidly, while laser lithotripsy provides precision for harder or smaller fragments, contributing to our high clearance rate and shorter operative times compared to historical reliance on single modalities. Supracostal punctures (56.3%) improved efficacy for upper pole stones, with pleural complications at 0.5%, thanks to CT guidance. 14 Infracostal approaches posed challenges in females due to anatomy, but overall, the mix-and-match lithotripters optimized fragmentation.
Across 766 patients, complications occurred in 126 (16.4%): intraoperative bleeding in 52 (6.8%), with 13 (1.7%) significant (requiring transfusion); postoperative complications included bleeding requiring transfusion in 13 (1.7%), urosepsis in 21 (2.8%) with 3 (0.4%) needing ICU (Grade IVa), hydrothorax requiring intercostal drainage in 4 (0.5%, Grade IIIa), angioembolization for bleeding in 5 (0.7%, Grade IIIb), DJ stent repositioning in 2 (0.3%, Grade IIIa), bedside bladder clot evacuation in 1 (0.1%, Grade IIIa), severe complications requiring prolonged ICU stay in 2 (0.2%, Grade IVb), minor issues (e.g. fever, pain) in 62 (8.1%, Grade I), and infections needing antibiotics as part of 41 (5.3%, Grade II). No mortality occurred. The notably low transfusion rate of 1.7% is attributable to several advancements: (1) preoperative CT imaging for precise puncture planning, minimizing vascular injury; (2) standardized operating procedures ensuring consistent and controlled technique; (3) use of air + contrast pyelography for accurate initial puncture, reducing misplacement; (4) fewer punctures (average 1.3) due to optimized access planning; and (5) improved lithotripsy techniques, such as ultrasonic and laser, which reduce mucosal trauma and bleeding during fragmentation. These elements collectively represent advanced control, which encompasses not only precise surgical execution but also the integration of modern imaging, intraoperative fluoroscopy, and tailored lithotripsy to minimize complications and optimize outcomes. Complications (16.4%) were low, with multimodal analgesia contributing to pain scores of 3.5 and hospital stays of 3.6 days. 21 Our results align with improved morbidity trends, with clearance exceeding 90%.2,17,21
Transfusion rates have plummeted from 14% 19 to 3.5%–5.7%,14,18 with our 1.7% reflecting advanced control through the aforementioned advancements. Complication rates, once 29.5%, 17 now hover at 15.8%–19.6%,15,20 with our 16.4% including only 2.8% urosepsis and 0.7% angioembolization. Pain scores improved to 3.5 in our cohort, near Elawady et al.’s 21 3.9, attributed to multimodal analgesia. Clearance rates, historically 81.6%, 17 now consistently exceed 90%,2,21 with our 91.3% reinforcing this upward trajectory. An emerging and important consideration in the selection of the optimal surgical approach for renal stones is the use of validated predictive models and nephrolithometric scoring systems. Such tools allow clinicians to objectively stratify stone complexity, estimate stone-free rates, and tailor the choice of intervention (standard PCNL, mini-PCNL, or RIRS) to the individual patient’s stone burden and anatomy prior to surgery. For instance, Tufano et al. 22 externally validated the Resorlu-Unsal Stone Score (RUSS) for predicting stone-free rates after retrograde intrarenal surgery, demonstrating that pre-operative scoring systems can reliably guide surgical planning and patient counseling. More recently, Sighinolfi et al. 23 externally validated a nomogram for outcome prediction across SWL, RIRS, and PNL in medium-sized kidney stones, demonstrating that predictive models can be applied across different populations and surgical modalities to guide treatment selection. The routine integration of such scoring systems into pre-operative assessment could further refine patient selection for standard PCNL versus miniaturized alternatives, potentially improving outcomes across different stone burdens. Our center’s use of the Guy’s Stone Score (GSS) to classify stone complexity represents a step in this direction; however, future implementation of more comprehensive predictive tools could further optimize surgical decision-making in units managing high volumes of complex renal stones. Findings of the current study (i.e. 91.3% clearance, 1.7% transfusion, 16.4% complications) place standard PCNL in a competitive light against mini-PCNL, which offers shorter stays (1.5–2.3 days vs our 3.6) but struggles with large stone burdens. 8 The 6.3% prevalence of anatomic abnormalities and 46.7% complex stones (GSS ⩾ 2) in our cohort highlight standard PCNL’s adaptability, bolstered by a robust sample size. Stone clearance was defined radiologically (⩽3 mm), but longer-term functional outcomes, recurrence, or patient-reported measures were not assessed, representing a limitation alongside the retrospective design and absence of standardized PCNL outcome frameworks. The 6.3% anatomic abnormalities and 46.7% complex stones highlight standard PCNL’s adaptability, but prospective studies are needed. Future prospective studies should include recurrence rates and patient-reported outcomes to standardize PCNL frameworks. Lack of routine stone density assessment limits insights into lithotripsy choice correlations.
Limitations
This study has several limitations that should be considered when interpreting its findings. First, the retrospective, single-center design introduces inherent selection and information biases. Second, the absence of a mini-PCNL cohort at our center precludes direct head-to-head comparison with miniaturized PCNL techniques, which limits the generalizability of conclusions regarding the relative merits of standard versus mini-PCNL for stones greater than 2.5 cm. Third, this study lacks long-term follow-up data; stone recurrence rates, renal function trajectories, and patient-reported quality-of-life outcomes were not assessed. Fourth, stone density (Hounsfield units) was not routinely evaluated, which prevents meaningful correlation between stone composition or density and lithotripsy modality choice or fragmentation efficiency. Fifth, the multi-surgeon design, while reflecting real-world practice, introduces variability in technique and experience that may influence outcomes; individual surgeon caseload and learning curve effects were not formally analyzed. Finally, longer-term patient-reported outcome measures and functional renal assessments are needed to fully characterize the benefit of standard PCNL in this population.
Conclusion
Standard PCNL has evolved into a precise, powerful tool for large renal stones, leveraging refined techniques in standard PCNL, technological and radiological advancements to enhance clearance and reduce complications, solidifying its role as a cornerstone of modern urology despite the rise of mini-PCNL.
Footnotes
Acknowledgements
The authors thank the Department of Urology, AIIMS Jodhpur, for institutional and academic support.
Ethical considerations
This study was approved by the Institutional Ethics Committee, AIIMS Jodhpur. Written informed consent was obtained from all participants. The study adhered to the ICH-GCP guidelines and the Declaration of Helsinki.
Author contributions
Vikram Singh: Data collection. Jaideep Singh Soni: Drafting of manuscript. Deepak P Bhirud: Statistical analysis. Mahendra Singh: Conceptualization, Study design, supervision, manuscript editing. Shiv C Navriya: Critical review, methodology refinement. Gautam R Choudhary: Senior supervision, manuscript revision, overall guidance. Arjun S Sandhu: Final editing, critical inputs, approval of final manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.