
Abstract
Introduction:
If medical treatment and/or interventional methods have failed, and high intravesical pressure and urinary incontinence or recurring urinary tract infections persist combined with present vesicoureteral reflux and impaired renal function, surgical treatment in terms of bladder augmentation is indicated.
Aim of the study:
The main objective of this study was to evaluate whether we have to do ureteral reimplantation in patients with spastic neurogenic bladder during augmentation.
Patients and methods:
A total of 72 patients with spastic neurogenic bladder with VUR were included in the study. The median age at surgery was 12 years, ranging from 3 to 27 years. All of them underwent augmentation cystoplasty for the period between 2016 and 2023. The changes in VUR grade and urodynamic findings were retrospectively evaluated.
Results:
The median follow-up after AC surgery was 1.5 years, ranging from 0.3 to 2.3 years. The changes in vesicoureteral reflux (VUR) grade before and after surgery: VUR was detected in 72 patients, involving 89 ureters. Among the 89 ureters, the reflux grade was V in 31, IV in 34, III in 23, I in 11. Postoperative VCUG revealed that the reflux resolved in 74 ureters (83%) and was downgraded in 15 ureters (17%). During urodynamics, it was observed that the bladder capacity at which VUR occurred significantly increased from 50 to 450 mL (p < 0.05). However, there was no significant change in detrusor pressure at the onset of VUR.
Conclusion:
In patients with spastic neurogenic bladder undergoes augmentation cystoplasty: Routine ureteral reimplantation may not be necessary.
Keywords
Introduction
The neuropathic bladder clinically diagnosed by the patients suffer from many symptoms such as the incontinence, frequent urinary tract infection while the improper management and treatment can lead into chronic renal failure the prognosis will be an end stage renal disease. 1 The architecture of bladder affected by high-pressure and low-compliance lead to damage forming diverticulation and loss of flexibility consequently the incontinence occurs then vesicoureteral reflux eventually chronic renal failure. 2
Von Mikulicz carried out augmentation cystoplasty for the first time in 1889 on a patient who had bladder exstrophy. 3 But it wasn’t common practice until the 1950s, when Couvelaire treated tiny, contractile bladders caused by TB cystitis by performing bladder augmentation. 4 Patients with neurogenic detrusor overactivity brought on by multiple sclerosis, spinal cord injuries, and myelodysplasia have been the main target of bladder augmentation hyper the years. 5 Patients with idiopathic overactive bladder who have not responded to less invasive treatment methods may also benefit from bladder augmentation. The main objective of augmentation. 6 In order to improve bladder capacity and compliance, prevent upper tract degradation, enhance urine continence, and enhance quality of life, cystoplasty is used to establish a low-pressure storage reservoir. Since its inception, a wide variety of tissue sources have been employed, most frequently the stomach, sigmoid colon, ileum, and cecum. 7
Aim of the study
The main objective of this study was to evaluate whether we have to do ureteral reimplantation in patients with spastic neurogenic bladder during augmentation.
Patients and method
This was a prospective single-center study where a total of 72 patients with spastic neurogenic bladder with VUR who had been conservative treatment by CIC and anticholinergic agents with no response. The median age at surgery was 12 years, ranging from 3 to 27 years. All of them underwent augmentation cystoplasty for the period between 2016 and 2023.
Inclusion criteria:
Patients with spastic neurogenic bladder and vesicoureteral reflux (grade III–V)
failed conservative management.
Exclusion criteria:
active urinary tract infection at time of surgery.
renal impairment (eGFR < 30 ml/min/1.73 m2).
Primary endpoint: resolution or downgrading of VUR on postoperative voiding cystourethrogram.
Secondary endpoints: changes in urodynamic parameters (bladder capacity, compliance, detrusor overactivity), complication rates, and renal function preservation.
Two procedures were done during cystoplasty, ileocystoplasty, and ureterocystoplasty five patients had Mitrofanoff appendicovesicostomy in addition to cystoplasty.
All those Patients were followed regularly by: routine basic investigations especially urinalysis and renal function tests, abdominopelvic ultrasound and urodynamic study and voiding cystourethrogram minimum follow-up required was 3 months postoperatively. Follow-up assessments were conducted at 3 months, 6 months, 1 year, and annually thereafter.
Surgical procedure
In ileocystoplasty; detubularised segment of the distal ileum (about 20 cm) is inserted into the bivalved bladder wall.
Teapot ureterocystoplasty is done in patients with non-functioning or poor-functioning kidney to make full use of the ipsilateral tortuous ureter and renal pelvis for augmentation
Mitrofanoff appendicovesicostomy was done in addition to cystoplasty in patients with intrinsic sphincter deficiency.
Statistical analysis
Continuous variables are presented as median and range due to non-normal distribution. Categorical variables are expressed as frequencies and percentages. Pre- and postoperative urodynamic parameters were compared using the Wilcoxon signed-rank test for paired data. A p-value <0.05 was considered statistically significant. Statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA).
Results
A total of 72 patients were included in the study. The median age at surgery was 12 years, ranging from 3 to 27 years. The median follow-up after AC surgery was 1.5 years, ranging from 0.3 to 2.3 years. The causes of neurogenic bladder were myelomeningocele, spinal cord lipoma, and imperforate anus (Table 1).
Demography and postoperative complication.
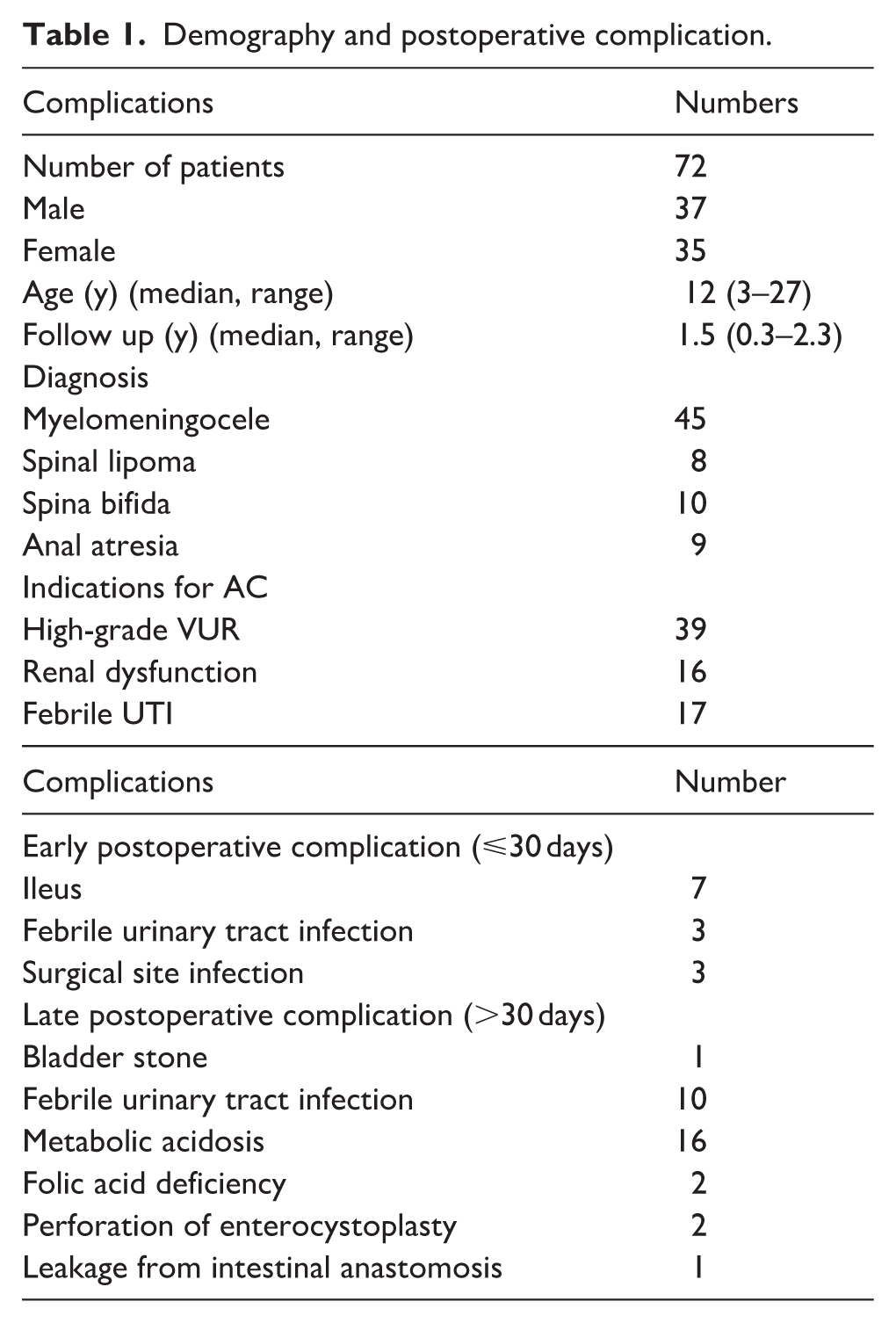
Two procedures were done during cystoplasty, ileucystoplasty, and ureterocystoplasty five patients had Mitrofanoff appendicovesicostomy in addition to cystoplasty
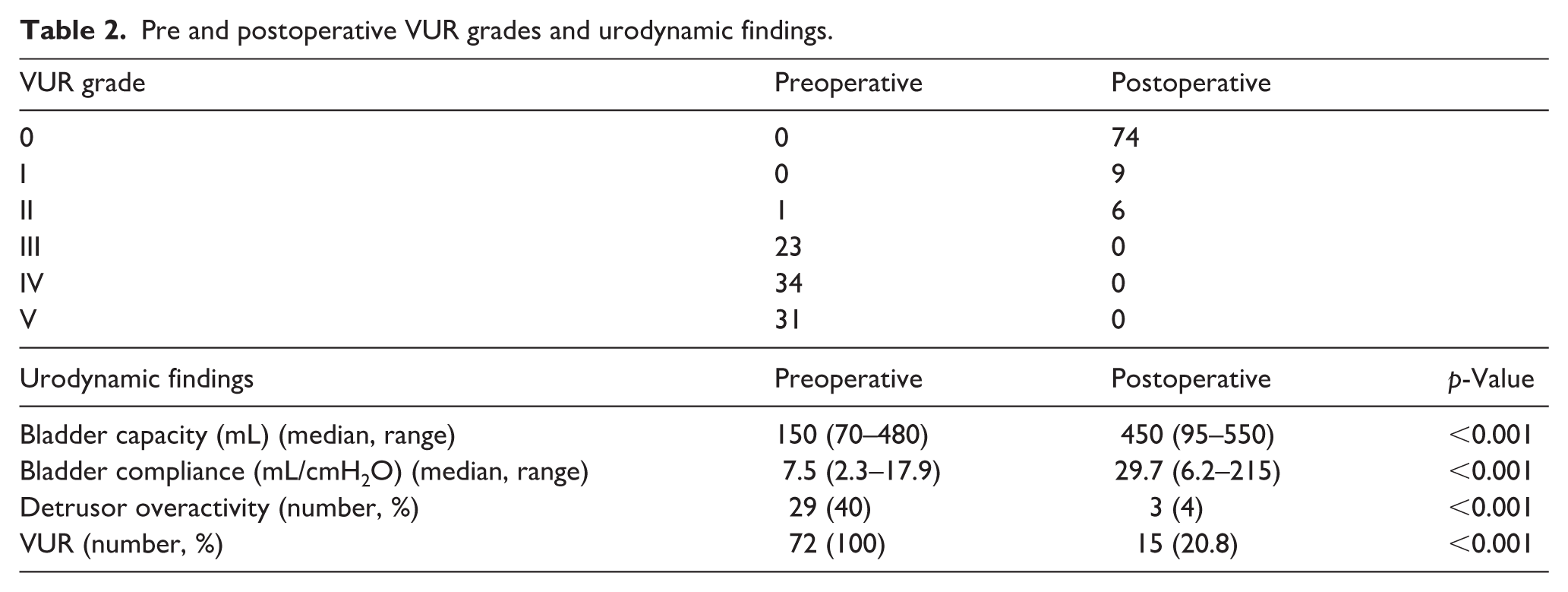
Preoperatively, VUR was detected in all 72 patients, involving 89 ureters (17 patients had bilateral reflux). Among these 89 ureters, preoperative reflux grade distribution was: grade V in 31 ureters (35%), grade IV in 34 ureters (38%), grade III in 23 ureters (26%), and grade II in 1 ureter (1%).
Postoperative VCUG revealed that the reflux resolved in 74 ureters (83%) and was downgraded in 15 ureters (17%) (Table 2).
Pre and postoperative VUR grades and urodynamic findings.
Discussion
All subjects with dysfunctional neurogenic bladder and the high-grade reflux augmentation cystoplasty procedure typically carried out with ureteral reimplantation nevertheless it is challenging to do that interested in bladder thick-wall also considered long hours surgery with high morbidity very complex augmentation procedure. The present study evaluated whether augmentation cystoplasty alone—without routine ureteric reimplantation—could achieve adequate VUR management and favorable functional outcomes in patients with spastic neurogenic bladder.
While Zhang et al. 8 claimed that not all patients need reimplantation of ureteral with VUR; the study found 24/29 (83%) patients complete resolve, where 3/29 (10%) improved, and no change found 2/29 (7%). These results are remarkably similar to those of the present study, supporting the hypothesis that prevention of urinary tract infections and renal deterioration through effective clean intermittent catheterization and augmentation of bladder capacity may be achieved without concurrent antireflux surgery.
Several small study series hypothesis this standard procedure for future guideline. Nevertheless, Nasrallah et al confirmed in a study of 14 patients having different degrees of reflux starting grade II to grade V; the bladder that have poor capacity that is, (functional capacity between 40 and 210 mL), and poor compliance (leak point pressure > 40 and <80 cm H2O) augmentation only can resolve reflux, in the follow up at recovery period of 72 months. 9 These findings provide additional support for our approach.
López Pereira et al. 10 reported that in patients with augmented bladders, vesicoureteral reflux—regardless of grade—resolved or improved in 87.5%–100% of cases without routine ureteric reimplantation.
This observation supports the mechanistic hypothesis that high intravesical pressures contribute significantly to VUR in neurogenic bladder. Our urodynamic findings demonstrated substantial improvement in bladder compliance (median increase from 7.5 to 29.7 mL/cmH2O, p < 0.001) and capacity (median increase from 150 to 450 mL, p < 0.001) postoperatively. The dramatic increase in bladder capacity effectively creates a low-pressure reservoir, which likely reduces the mechanical stress on the ureterovesical junction and allows intrinsic antireflux mechanisms to function adequately. However, it is important to note that our data show VUR resolution occurred even in cases where detrusor pressure patterns did not normalize completely, suggesting that increased bladder capacity and compliance—rather than pressure reduction alone—may be the critical factors. The precise mechanism remains incompletely understood and likely involves multiple factors including altered bladder geometry, reduced peak detrusor pressures during filling, and improved viscoelastic properties of the augmented bladder wall.
Conclusion
Our findings suggest that routine ureteral reimplantation during augmentation cystoplasty may not be necessary in selected patients with spastic neurogenic bladder and high-grade VUR, particularly when adequate bladder capacity and compliance are achieved.
Study limitations
This study has several important limitations that warrant consideration. First, it is single-center design without a control group limits causal inference and generalizability. Second, the heterogeneous patient population—spanning a wide age range (3–27 years) and multiple etiologies (myelomeningocele, spinal lipoma, spina bifida, anal atresia)—introduces clinical variability that may affect outcomes. Third, the relatively short median follow-up of 1.5 years.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.