
Abstract
Background and objectives:
An increase in genital abnormalities in boys born via assisted reproductive technologies (ART) is possibly linked to either the technical aspects of ART or parental health, regardless of the type of ART procedure. This study aimed to describe the spectrum and prevalence of genital findings in ART-conceived male infants and to identify potential modifiable factors associated with genital development in this subpopulation.
Methods:
An observational, exploratory/hypothesis-generating case series was conducted from August 2006 to July 2007. A total of 294 consecutively born male neonates were examined by a single urologist blinded to conception method. From this cohort, 71 infants conceived via ART were identified. Obstetrician-gynecologists retrieved detailed data on parental reproductive history and newborn health status. A nested comparative analysis was performed within the ART group, using the adjusted Wald-method and the two-sided Fisher’s exact test.
Results:
Forty boys (56%) in the study group had normal genitalia, whereas 31 (44%) displayed abnormalities. Singleton pregnancy was a significant protective factor for normal genitalia (p = 0.004), while a non-significant trend was observed for the absence of maternal abnormalities other than obstructive infertility (p = 0.282). Hypospadias prevalence (4.2%), in contrast to cryptorchidism and inguinal hernia, exceeded general population rates (0.06%–0.7%) and was an order of magnitude higher than in Denmark and Sweden (0.3%–0.4%). This increased prevalence was associated with male factor infertility (p = 0.041) and with maternal subfertility in the form of preterm labor (p = 0.032). The complex of penile malformations were linked to maternal endocrine infertility (p = 0.033), dizygotic twins (p = 0.014), and preterm labor (p = 0.017), with non-significant trend for threatened miscarriage (p = 0.107).
Conclusion(s):
This blinded case series reveals a distinct spectrum of genital findings in ART-conceived neonates, with high hypospadias prevalence. Penile development appears primarily linked to parental fertility issues and preterm labor. Singleton pregnancy is likely a strong protective factor. These findings indicate underlying parental subfertility as the potential determinant of genital malformation risk, with ART procedures as a possible confounder.
Keywords
Introduction
The proportion of children conceived via assisted reproductive technologies (ART) has become a significant socio-demographic trend, raising important questions about their long-term health outcomes. Currently, ART accounts for approximately 1% of annual births in the USA and 3%–4% in Europe and Australia. 1 A consistent finding in this subpopulation is a moderately increased risk of congenital anomalies and malformation compared to naturally conceived children. According to a meta-analysis by Hoorsan et al., 2 the odds ratio (OR) for congenital malformations is highest for the genitourinary system at 1.58 (95% CI 1.28, 1.94), compared to 1.43 (95% CI 1.27, 1.62) for the cardiovascular system, 1.36 (95% CI 1.10, 1.70) for the central nervous system, and 1.35 (95% CI 1.12, 1.64) for the musculoskeletal system. This elevated prevalence, particularly concerning urogenital anomalies, in this subpopulation makes the identification of underlying causes and contributing factors a key priority for urology, reproductive, and pediatric medicine.
The causes of these congenital abnormalities are actively debated. Many experts relate them to the technical aspects of ART procedures. For instance, the increase in the prevalence of imprinting-associated syndromes of Beckwith-Wiedemann, 3 Angelman 4 and Silver-Russell 5 is linked with standard techniques for ART, such as the stimulation of super-ovulation, gamete extraction and artificial insemination, and the use of chemicals for the in vitro embryo culture, etc. In the case of intracytoplasmic sperm injection (ICSI), the risk is considered potentially higher 6 due to factors such as the possible use of sperm with genetic abnormalities or morphological defects and the circumvention of natural selection.7,8 Conversely, other experts state that more frequent congenital abnormalities are associated with parental health, 9 late reproductive age, 10 underlying subfertility/infertility,1,11–13 multiple pregnancy, 11 etc., independent of ART procedures. However, the relative contribution of these factors to the risk of specific genital anomalies remains poorly quantified, especially in a clinical setting with blinded assessment.
Therefore, the aim of this blinded case series was to describe the spectrum of genital findings in ART-conceived male neonates and to analyze the association of these findings with ART-related and parental factors, in order to identify potential targets for risk reduction.
Material and methods
Study design and setting
Obstetrician-gynecologists from the Kulakov National Medical Research Center for Obstetrics, Gynecology, and Perinatology (NMRC OGP) proposed a collaborative study with urologists from the Department of Pediatric Surgery at Pirogov Russian National Research Medical University (RNRMU). The study design was classified as an observational, retrospective, exploratory/hypothesis-generating case series in clinical epidemiology. 14 The study protocol was reviewed and approved by the Local Independent Ethics Committees of the RNRMU, approval number 79. This work is prepared in accordance with the PROCESS guidelines from 2018. 15
Study population and blinded examination
The source population comprised all male neonates born at the NMRC OGP between August 2006 and July 2007. Data extraction was performed independently by two researchers to minimize transcription errors. During this period, a single pediatric urologist from RNRMU performed a standardized, sequential physical examination of all live-born male infants (n = 294) as part of routine neonatal care. To eliminate diagnostic bias, the examiner was fully blinded 16 to the method of conception. Information regarding the use of ART or natural conception was concealed in the medical records subsequently provided for assessment.
Assessment of genital anomalies and comparison with population data
The urologist’s careful examination focused on the assessment of external genitalia. Diagnosed anomalies (cryptorchidism, hypospadias, inguinal hernia, etc.) were recorded. The prevalence of these anomalies in the ART-conceived group (n = 71) was described and contextually compared with published ranges for the general population, drawn from reviews,17,18 cohort studies,13,19 and meta-analyses. 20 In the general population, the prevalence of inguinal hernia in children ranges from 1:10 to 1:30 (3%–11%), 17 cryptorchidism in full-term newborns from 1:25 to 1:100 (1%–4%), reaching 45% in preterm neonates 18 ; and hypospadias from 1:135 (USA, Israel) to 1:1650 (Japan), corresponding to an overall prevalence of 0.06%–0.7%. In Sweden and Denmark, whose populations we considered to be close to Russia in terms of race and geographically, the prevalence of hypospadias is 1:250 (0.4%) and 1:330 (0.3%), respectively. 20 Moreover, in the subpopulation of ART-conceived boys in these Scandinavian countries, the reported prevalence ranged from 1:166 to 1:200 (0.5%–0.6%).13,19
Case identification and data extraction
From this examined cohort of 294 boys, the study group was formed. Obstetrician-gynecologists, who were not involved in the neonatal examination, retrospectively reviewed the complete obstetric and neonatal records. They identified 71 boys born via ART. For these 71 cases, detailed data on potential risk factors for genital abnormalities were extracted from parental reproductive histories, as discussed in the literature.1,9–11,13,19 The extracted variables included:
Preconception data: parental ages, including late fertile parental age (over 35 years), 10 maternal endocrine disorders prior to pregnancy, 9 male infertility, 13 etc.;
Conception data: specific ART procedures, including controlled ovarian stimulation (COS), artificial insemination by husband (AIH) or donor (AID), frozen-thawed embryo transfer (FET), oocyte donation (DO), in vitro fertilization (IVF) and ICSI;
Pregnancy and perinatal data: multiple pregnancy, 12 indicators of female subfertility.1,12
Anthropometric parameters and definition
Newborn anthropometric measurements and their gestational age at birth were recorded. Preterm birth was defined as delivery before 37 completed weeks of gestation. 21 “Small for gestational age infants (SGA)” was diagnosed when the birthweight was below the 10th percentile. 22 These values were obtained from Table Dependence of a single newborn’s weight on the term of delivery by Alexander et al. 22
Definitions of parental reproductive history factors
In this study, we also took into account the fact that the concept of female subfertility/infertility is much broader than that of males and includes both the impaired ability to conceive and the difficulty in carrying a pregnancy to full term and childbirth. 23 The clinical distinction between infertility and subfertility is often fluid. Therefore, for the purposes of this analysis, the term “subfertility” was applied operationally to characterize conditions associated with compromised pregnancy maintenance. Documented indicators included the signs of the metabolic and hormonal dysfunction of the mother-placenta-fetus system: lower abdominal pain, uterine hypertonus, vaginal bleeding, placental insufficiency, and the delivery of preterm and/or SGA infants.
Statistical analysis
Statistical data processing was performed using Excel spreadsheets (Office 2003, Microsoft Corporation) and the STATISTICA software package for Windows v. 6.0 (StatSoft, Inc.).
Descriptive Statistics: Categorical variables are presented as absolute numbers (n) and relative frequencies (%). Continuous variables are reported as median and interquartile range (IQR) due to the non-normal distribution of data in this small sample.
Comparative Statistics: Association between categorical parental/pregnancy factors and genital outcomes within the ART group were assessed using the two-tailed Fisher’s exact test. Confidence intervals (95% CI) for proportions were calculated using the adjusted Wald method.
Handling of Data and Multiple Testing: The percentage of missing data was low (<5% for all analyzed variables). Given the exploratory, hypothesis-generating nature of this study and the small sample size, no formal correction for multiple comparisons (e.g. Bonferroni) was applied. Therefore, all p-values should be interpreted with caution as indicating potential associations that require validation in larger, confirmatory studies.
Results
Clinical and obstetric characteristics of the study group
The boys in the study group were born between 30 and 40 weeks of gestation, with a median gestational age at birth of 38.5 weeks (IQR: 38–38.5). Eight infants (11.3%) were born preterm. Birth weights ranged from 1.0 to 4.55 kg, with a median of 3.29 kg (IQR: 3.0–3.54). Twenty-one boys were born from dizygotic twin pregnancies, including two pairs of male twins.
Prevalence of genital abnormalities in boys and its estimation
Forty boys (56%) had normal genitalia, whereas 31 (44%) displayed genital abnormalities.
Penile malformations were diagnosed in six cases (8.5%): isolated hypospadias in three boys (4.2%, 95% CI 0.96, 12.19) – one proximal-stem and two distal forms, concealed penis in two infants (2.8%), and penile rotation with deviation in one neonate (1.4%).
Developmental anomalies were found in 25 cases (35.2%); abnormalities of the scrotal organs in two full-term infants (2.8%) – bilateral cryptorchidism with bilateral hydrocele (n = 1) and unilateral cryptorchidism (n = 1); and abnormal obliteration of the processus vaginalis in 23 neonates – unilateral oblique inguinal hernia (n = 5, 7.0%, 95% CI 2.68, 15.81) and unilateral (n = 14) and bilateral hydrocele (n = 4).
Comparison with population data
The calculated 95% CI for the prevalence of hypospadias in our sample (0.96, 12.19) did not include the rates for Denmark (0.3%), Sweden (0.4%), the general population (0.06%–0.7%), 20 or the subpopulation of ART-conceived boys from these Scandinavian countries (0.5%–0.6%).13,19 Thus, the observed prevalence of hypospadias exceeded the reported rates in the general population and was substantially higher than in Denmark, Sweden, and even among ART-conceived boys in Scandinavia. In contrast, the prevalence of cryptorchidism 18 and inguinal hernia 17 in our cohort-based study fell within the reported ranges for the general population.
Causes of infertility, parental age, and health status
Most couples had long histories of infertility and reproductive disorders that influenced conception and, possibly, the intrauterine development of male fetuses (see Table 1 for causes).
Causes of infertility in 69 couples.
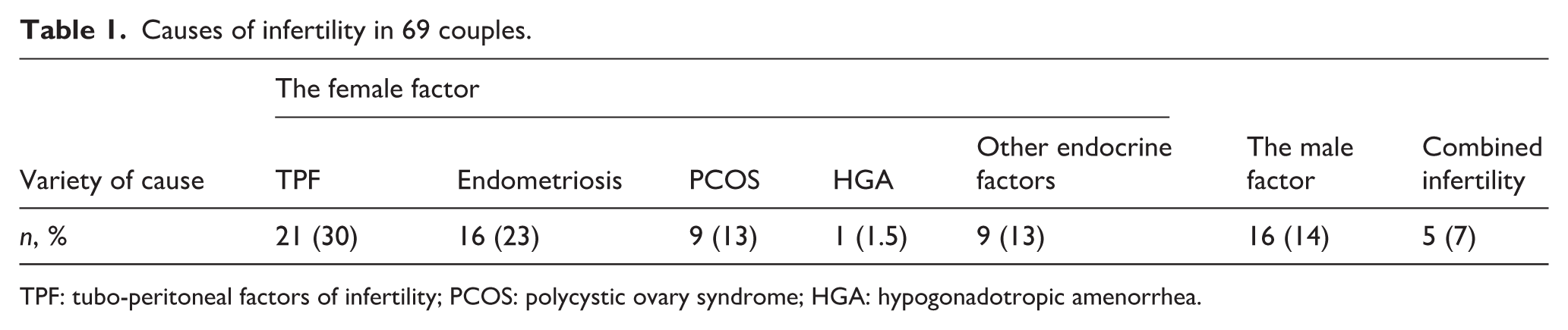
TPF: tubo-peritoneal factors of infertility; PCOS: polycystic ovary syndrome; HGA: hypogonadotropic amenorrhea.
A total of 69 couples participated in this study, including the parents of two sets of male twins (n = 4). Female infertility was caused by non-endocrine disorders (n = 19) and endocrine disorders (n = 18) or endometriosis (n = 16). The causes of male infertility included decreased sperm motility (n = 14), teratozoospermia (n = 2), and azoospermia (n = 2). Five couples had combined infertility issues. Furthermore, nine couples presented with isolated male infertility, and 53 couples had isolated female infertility. In four couples, the underlying causes of infertility were undetected.
The parents who participated in our study also often had a history of unfavorable contributing factors. In 42 couples (62%), at least one parent was of late fertile age (>35 years). The median paternal age was 35 years (IQR: 33–39) and median maternal age was 32.5 years (IQR: 29–37). Twenty mothers (29%) had various comorbid conditions, including lipid metabolism abnormalities (n = 1), thyroid disorders (n = 1), adrenal gland disorders (n = 2), hyperandrogenism (n = 3), arterial hypertension (n = 2), asthma (n = 1), chronic venous insufficiency (n = 2), hypercoagulation (n = 3), urolithiasis (n = 1), the presence of antibodies against chorionic gonadotropin (n = 3), and chronic viral infections (n = 6), including hepatitis B (n = 1), CMV (n = 1), HSV (n = 3), as well as their combinations.
The relation between genital and parental factors is detailed in Table 2.
The genitalia assessment of 71 boys with regards to the parents’ health.
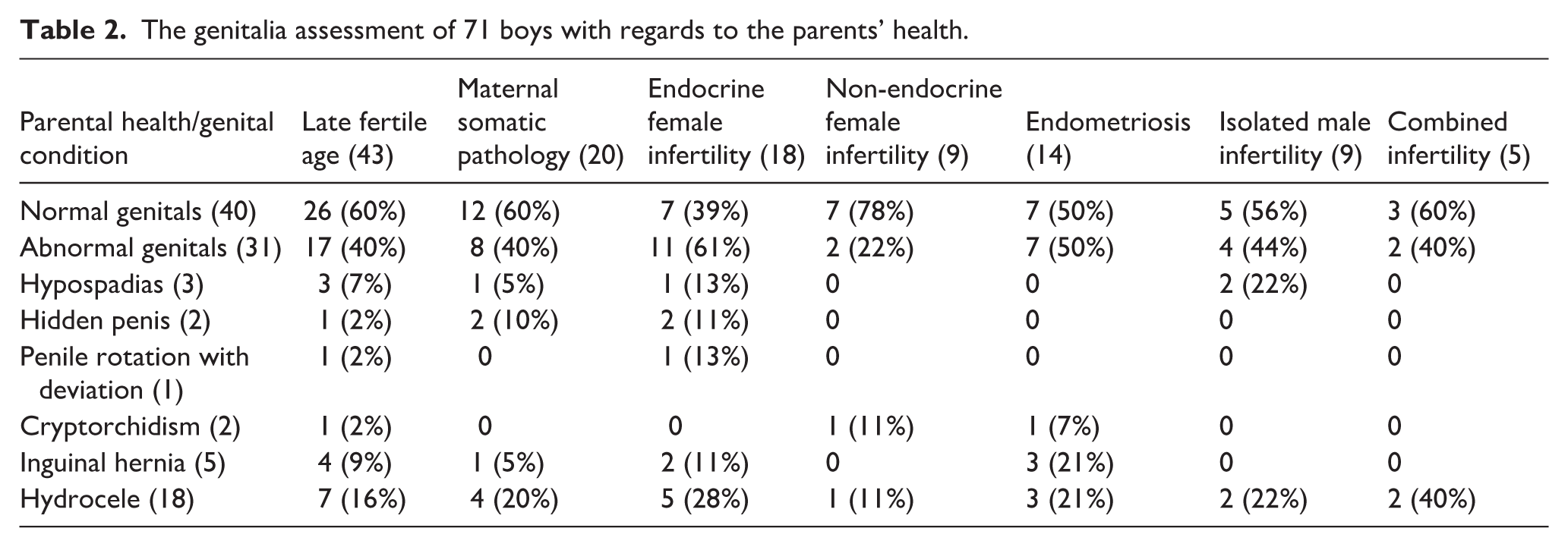
Infants born to mothers with isolated non-endocrine infertility due to pelvic adhesions and obstructed fallopian tubes quite often had normal genitalia (n = 7 (78%), p = 0.282). Infants born to mothers with endocrine infertility were significantly more likely to have penile abnormalities (n = 4 (22%), p = 0.033), including hypospadias (n = 1), concealed penis (n = 2) and penile rotation with deviation (n = 1). Penile anomalies were also observed in neonates born to women with internal diseases (n = 3 (15%), p = 0.34).
All infants with hypospadias were born to parents of older reproductive age, although this association did not reach statistical significance (p = 0.275). Hypospadias also was more common in cases of isolated male infertility (n = 2 (22%), p = 0.041).
Assisted reproductive technologies used
The applied ART methods are summarized in Table 3. In cases of female infertility, IVF (n = 36), DO (n = 4), and surrogacy (n = 1) were used. For male infertility, ICSI (n = 15), AIH (n = 1), and AID (n = 1) were employed. COS (n = 13) was used in cases of female endocrine fertile issues or suboptimal semen parameters. FET was also utilized in two cases.
The genitals of 71 male infants and ART method used.
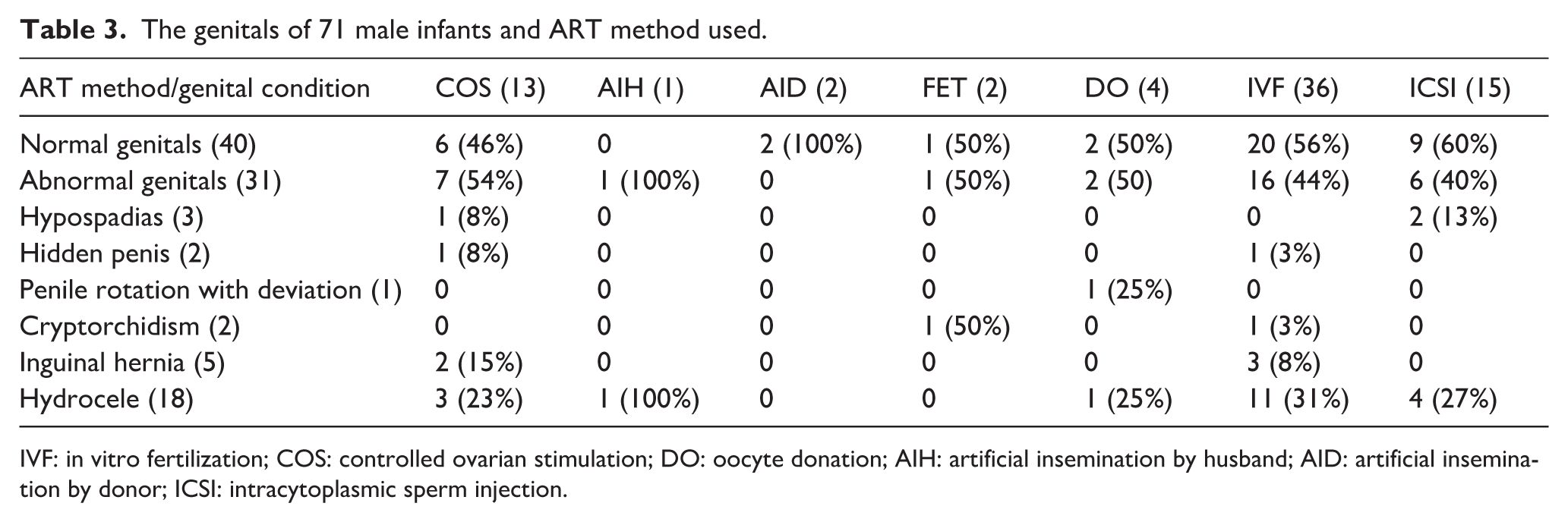
IVF: in vitro fertilization; COS: controlled ovarian stimulation; DO: oocyte donation; AIH: artificial insemination by husband; AID: artificial insemination by donor; ICSI: intracytoplasmic sperm injection.
In IVF programs, gonadotropins (rFSH, hMG) were prescribed to stimulate ovaries according to either the GnRH-a long protocol, or GnRH-ant protocol. In some cases, clomiphene citrate was administered as a part of AIH/AID procedures to stimulate the ovaries. All patients received progesterone-containing luteal phase support, with 50% receiving combined estrogen-progesterone therapy. This maintaining therapy was discontinued only in the second trimester, meaning that the entire period of organogenesis occurred under hormonal therapy.
No cases of hypospadias were identified in the standard IVF subgroup. Concealed penis was revealed in one neonate. In the COS subgroup, penile malformations (hypospadias, n = 1; concealed penis, n = 1) were observed in 2 of 13 cases (15.4%, p = 0.33). The frequency of hypospadias in the ICSI subgroup was notable (2 of 15, 13.3%), though not statistically significant (p = 0.105).
Pregnancy course and outcomes
The relationship between pregnancy characteristics and genital findings is presented in Table 4.
The genitals of 71 male infants with regard to the course of pregnancy.
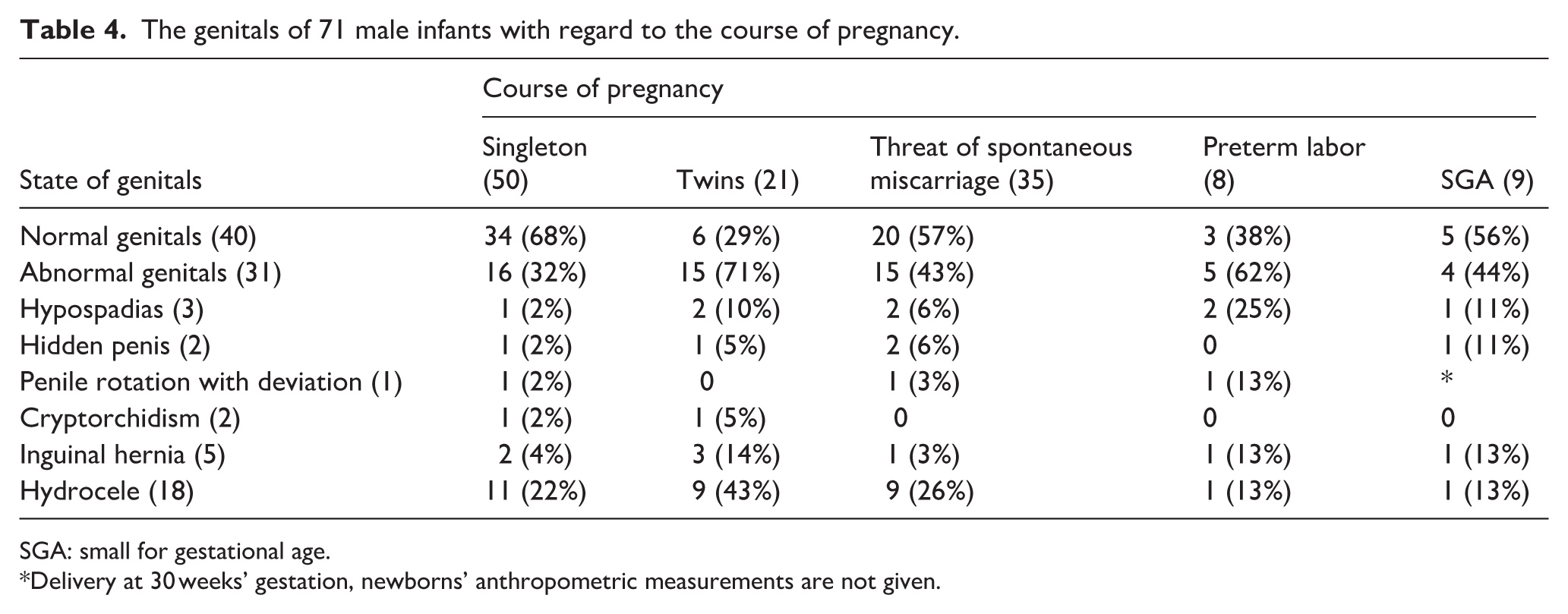
SGA: small for gestational age.
Delivery at 30 weeks’ gestation, newborns’ anthropometric measurements are not given.
Singleton pregnancy was a significant protective factor for normal genitalia (n = 34 (68%), p = 0.004). In contrast, boys from multiple pregnancies (dizygotic twins was the only type in this study) mainly had abnormal genitalia (n = 15 (71%), p = 0.004), including a higher frequency of penile malformations (n = 3 (14%), p = 0.014).
Infants with penile malformations were more often born to mothers who were at risk of spontaneous abortion (n = 5 (14%), p = 0.107) and delivered of preterm labor (n = 3 (38%), p = 0.017). Specifically, two out of three boys with hypospadias were born preterm (p = 0.032).
Twin pregnancies were more frequently complicated by threat of spontaneous miscarriage (38%), preterm labor at 32 to 37 weeks (24%), and SGA infants (10%). All pregnant women with multiple pregnancies received pregnancy-maintaining therapy, including hormonal support. 29% of neonates weighing from 998 to 2685 g were transferred to the neonatal intensive care unit due to poor health.
Discussion
Researchers in Australia,24,25 Sweden,26,27 and Denmark19,28 have systematically studied anomalies and malformations in ART-conceived children – a topic at the intersection of urology, genetics, epidemiology, reproductive medicine, embryology, obstetrics, perinatology, etc. Study designs have ranged from case studies9,29 to meta-analyses,2,30 typically drawing cases from Birth or Congenital Malformations Registers. In this subpopulation, the incidence of hypospadias25,29,31 and cryptorchidism25,29 has been reported to be, on average, twice that of the general population, though the underlying reasons remain poorly understood. This limited understanding may partly reflect the lack of integrated communication between physicians of these specialties, the inherent limitations of registry-based data, including incomplete case ascertainment (up to 71% of cases may be missed 32 ) and underdiagnosis of mild forms of the disease, 33 etc.
In this case series study, we applied a multidisciplinary approach that allowed for the acquisition of detailed data on parental reproductive history, prior medical intervention, overall health status, and genital examination findings of male newborns. Despite the modest sample size, this approach generated clinically grounded hypotheses regarding potential factors associated with genital anomalies and malformations in ART-conceived neonates and can inform the design of future confirmatory studies to develop preventive measures.
In the study group, the ratio of normal to abnormal genitals was approximately 1:1. Normal genitals were more prevalent among boys from singleton pregnancies, following AID, and in those born to otherwise healthy women whose infertility was attributed to tubal-peritoneal factors. These observations suggest that singleton pregnancy, AID, and isolated non-endocrine (obstructive) infertility in women may have less influence on male genital development, though confirmation in larger, controlled studies is needed.
Conversely, pre-existing maternal medical conditions – particularly endocrine abnormalities – and factors associated with late parental fertile age were more frequently observed in cases with abnormal genital development. At least one of these predisposing factors, or their combinations, was present in all cases of penile malformations, including hypospadias and concealed penis. All infants with hypospadias were born to parents of late reproductive age (over 35 years). Furthermore, boys from dizygotic twin pregnancies were more likely to have abnormal genital findings, with penile malformations also more commonly observed in multiple pregnancies.
Regarding specific ART methods, the majority of infants conceived via conventional IVF had normal genitalia (20 of 36). Among the remaining 16 newborns in this group, 14 presented only minor abnormalities such as inguinal hernia and hydrocele. In the ICSI subgroup, the overall prevalence of genital abnormalities was lower than in other subgroups; however, hypospadias was observed in 2 of 15 boys. Hypospadias was also detected in 1 of 13 neonates conceived following COS. These observations, while based on small numbers, are consistent with the hypothesis that COS and ICSI procedures may be indirectly associated with an increased prevalence of hypospadias due to underlying parental reproductive issues, as suggested by our data and other researchers’ findings.7,13,26,31
Medical interventions in the delicate process of conception and pregnancy maintenance in couples with infertility-related conditions may contribute to the development of genital anomalies and malformations in male infants, regardless of the type of ART-procedures. In particular, the occurrence of hypospadias in two of nine neonates born to couples with isolated male infertility (pathospermia) suggests that male infertility may be a leading factor, with ICSI potentially representing a confounder rather than an independent risk factor. A similar pattern was observed in COS and IVF subgroups where insemination was performed with subfertile sperm, as well as in the subgroups of mothers with endocrine infertility or those with a history of threatened spontaneous abortion or preterm labor. However, intensive pharmacological interventions – including hormonal medications to support pregnancy following assisted conception, particularly in complicated cases – may also contribute to these outcomes and deserve further investigation in future studies with appropriate designs to isolate specific effects.
Limitations
Several limitations should be considered when interpreting these findings. First, the absence of a control group precludes definitive conclusions about whether observed associations reflect ART procedures, underlying parental subfertility, or their interaction. Second, the small sample size (n = 71) resulted in wide confidence intervals (e.g. hypospadias prevalence: 0.96–12.19) and limited statistical power; multiple comparisons without correction increase the risk of false-positive findings. Third, data collected in 2006–2007 may not reflect current ART practices. Fourth, universal hormonal support in this cohort prevented analysis of its specific contribution to genital development. Fifth, potential residual confounding by unmeasured factors cannot be excluded. Therefore, all findings should be considered hypothesis-generating rather than confirmatory. Sixth, the single-center design may limit generalizability to other populations with different ART protocols or demographic characteristics.
Interpretation of findings in context
The apparent elevation in hypospadias prevalence compared to general population estimates should be interpreted cautiously, as the study sample may not be representative of the broader subpopulation of ART-conceived infants. Direct comparisons between studies without standardization for demographic characteristics, diagnostic criteria, and temporal trends can be misleading. The wide confidence interval around our estimate overlaps with the upper range of some population estimates, highlighting the need for larger, controlled studies with appropriate statistical power.
Notably, the prevalence of cryptorchidism and inguinal hernia in this sample fell within expected population ranges, suggesting that the observed patterns may be specific to penile development rather than reflecting a generalized increase in all genitourinary anomalies. This specificity may reflect the particular sensitivity of penile development to parental subfertility/infertility during the masculinization programming window, a hypothesis warranting future investigation.
Preliminary findings/conclusions
This blinded case series describes the spectrum of genital findings in 71 ART-conceived male neonates and explores associations with parental and pregnancy-related factors. Several patterns emerged that generate hypotheses for future research:
Normal male genital development in ART-conceived infants was more common in singleton pregnancies and in the absence of maternal abnormalities other than obstructive infertility.
In the study group of ART-conceived male newborns, the observed prevalence of hypospadias (4.2%, 95% CI 0.96–12.19) appears elevated compared to reported rates in the general population (0.06-0.7%) and in the subpopulation of ART-conceived boys from Scandinavia (0.5%–0.6%). In contrast, the prevalence of cryptorchidism and inguinal hernia in this sample fell within the expected ranges. It should be noted, however, that the wide confidence interval around our estimate reflects the small sample size and limits definitive conclusions about the magnitude of difference from population rates.
All cases of hypospadias occurred in infants born to parents of late fertile age (over 35 years).
Factors showing associations with penile malformation in exploratory analyses include male infertility, endocrine female infertility, dizygotic twin pregnancies, and female subfertility manifested as threatened spontaneous abortion and preterm labor requiring pharmacological therapy, including hormonal treatment. ART procedures (ICSI, COS) may represent confounders.
These findings suggest that parental fertility factors – particularly male infertility, maternal endocrine dysfunction, and pregnancy complications – may be more relevant to genital development in ART-conceived infants than has been previously recognized. Singleton pregnancy emerged as a potentially protective factor.
Given the exploratory nature of this study, its methodological limitations, and the small sample size, these observations should be considered hypothesis-generating rather than definitive. Well-designed studies conducted by an interdisciplinary team with appropriate comparison groups are needed to disentangle the relative contributions of parental subfertility, ART procedures, and pregnancy-related factors to the risk of hypospadias and other genital anomalies in this growing subpopulation of children conceived through assisted reproduction.
Footnotes
Acknowledgements
The authors wish to express their sincere gratitude to the following individuals for their contributions to this study: Chechurova Tatyana Nikolaevna and Tsaturova Kristina Ashotovna, researchers at the NMRC OGP, for providing clinical material. Shchelykalina Svetlana Pavlovna, MD, associate professor of the Department of Medical Cybernetics and Computer Science, MBF RNRMU and Chugueva Irina Alexandrovna, engineer, for their assistance in studying statistical analysis methods. Postnikov Sergey Sergeevich, MD, Professor of the Department of Clinical Pharmacology, RNRMU, for his valuable comments and recommendations during manuscript preparation.
Author Note
This study was carried out at the FSBI “Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology,” of Ministry of Healthcare of Russian Federation, Moscow, Russia.
Author contributions
Concept and study design – Nazarenko T. A., Nikolaev V. V. and Solontsov Yu. N. Collection and processing of material – Solontsov Yu. N. Data interpretation – Nikolaev V. V., Nazarenko T. A. and Solontsov Yu. N. Statistical analysis – Solontsov Yu. N. Writing and translating text – Solontsov Yu. N. Editing – Nazarenko T. A.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The research data are not publicly available on legal grounds but are available from the corresponding author upon request.