
Abstract
Introduction:
Radical cystectomy followed by urinary diversion is the standard of care for patients with muscle-invasive bladder cancer (MIBC). Cutaneous ureterostomy has emerged as an alternative to ileal conduit diversion, particularly in high-risk patients. The present study aimed to evaluate the outcomes and complications of cutaneous ureterostomy versus ileal conduit in patients with MIBC.
Methods:
This was a retrospective, descriptive cross-sectional study performed at Shahid Modarres Hospital in Tehran between 2018 and 2021. The study population consisted of patients who underwent radical cystectomy with either ileal conduit or cutaneous ureterostomy. Baseline characteristics, operative data, and postoperative complications were compared between the two groups.
Results:
The results showed that cutaneous ureterostomy was significantly utilized in patients with high creatinine levels, renal failure, and metastatic disease (p < 0.05). Analysis revealed that 30-day, 90-day, and 6-month survival rates, as well as surgical complications, were not significantly different between the two groups. Multivariable regression analysis was performed to adjust for baseline imbalances, indicating that the choice of diversion was not an independent predictor of early mortality, though it was heavily influenced by preoperative frailty. One-year survival, the number of preoperative transfusions, length of hospitalization, and operation duration were significantly higher in the ileal conduit group.
Conclusion:
Cutaneous ureterostomy appears to be a viable and “hypothesis-generating” alternative for elderly and frail patients. It is associated with shorter surgery duration, less blood loss, lower transfusion rates, and shorter hospital stays. Although early mortality rates are comparable, cutaneous ureterostomy may offer a safer profile for high-risk individuals, though long-term comparative studies with multivariable adjustment are warranted.
Keywords
Introduction
Bladder cancer (BC) is the fourth most common cancer in men and the ninth most common malignancy overall, accounting for approximately 150,000 deaths worldwide. 1 Urothelial (transitional cell) carcinoma is the most prevalent histological subtype, representing approximately 90% of cases. 2 A wide array of genetic, anatomical, hormonal, social, and environmental factors contribute to its pathogenesis. 3 Established risk factors include male sex, advanced age, ethnicity, exposure to industrial chemicals, pelvic radiation, cyclophosphamide use, chronic bladder irritation, family history, and smoking. 4
According to the TNM staging system, bladder cancers are categorized into non-muscle-invasive (NMIBC) and muscle-invasive bladder cancer (MIBC), defined by invasion into or beyond the muscularis propria. 5 While NMIBC has a high recurrence rate, it carries a relatively favorable prognosis with standard care. Conversely, a significant subset of MIBC patients progresses to metastatic disease despite perioperative chemotherapy. Guidelines from the EAU, NCCN, and AUA recommend radical cystectomy (RC) and urinary diversion (UD) as the standard treatment for MIBC and high-risk recurrent NMIBC.6 –10 Despite diagnostic advancements, approximately 25% of patients present with MIBC at initial diagnosis. 11 Without timely intervention, 38% of these patients develop metastasis within 6 months, with 5-year overall survival rates as low as 5% in untreated cases. 12
Although RC is the gold standard, it is a complex, invasive procedure associated with significant morbidity and mortality, particularly in the elderly and frail population. Recent evidence highlights that while orthotopic diversions are often preferred for younger patients, the choice of diversion in the elderly must be carefully individualized to balance oncological outcomes with the patient’s physiological reserve. 13 Urinary diversion methods are broadly classified into continent and incontinent types. The ileal conduit (IC) remains the most common incontinent diversion due to its perceived simplicity and established safety profile. 14 However, in high-risk patients, especially those presenting with obstructive uropathy or renal insufficiency, the extensive intestinal manipulation required for IC can lead to severe metabolic and surgical complications. 15
In such high-risk scenarios, cutaneous ureterostomy emerges as a viable, simplified alternative. By avoiding bowel resection and reducing operative time, this method potentially minimizes blood loss and intensive care requirements, thereby improving safety in patients with multiple comorbidities. 16 Given the lack of robust comparative data in this specific high-risk subgroup, the present study aimed to compare the outcomes and complications of cutaneous ureterostomy versus ileal conduit in patients with MIBC undergoing radical cystectomy.
Materials and methods
Study design and population
This retrospective, comparative study was conducted on patients who underwent radical cystectomy followed by either ileal conduit (IC) or cutaneous ureterostomy (CU) at the Urology Department of Shahid Modarres Hospital, Tehran, between 2018 and 2021. Out of 500 radical cystectomies performed during this period, 128 patients met the inclusion criteria: 62 underwent ileal conduit and 66 underwent cutaneous ureterostomy. Patients who underwent cutaneous ureterostomy as a secondary or salvage procedure (re-surgery; n = 15) were excluded to maintain the homogeneity of the primary diversion groups.
Data collection
Comprehensive clinical data were extracted from electronic medical records, including demographic characteristics (age, sex), oncological status (metastatic vs non-metastatic), and perioperative parameters (operative time, intraoperative complications, and blood transfusion requirements). Postoperative outcomes included short-term mortality (30-day), postoperative complications, length of hospital stay, and the need for secondary surgical interventions. Long-term follow-up data, including laboratory tests, ultrasonography findings, and patient satisfaction, were also recorded. For patients with incomplete records, missing data regarding survival status, cause of death, and diversion-related issues (e.g. catheter dependency in the CU group) were obtained via direct telephone interviews.
Outcome measures
The primary outcomes were survival rates (30-day, 90-day, 6-month, and 1-year) and the incidence of surgical and medical complications. Secondary outcomes included operative duration, length of hospitalization, and perioperative transfusion rates. Additionally, the association between clinico-pathological features (e.g. hydronephrosis, pathological stage, and positive surgical margins) and 30-day mortality was assessed.
Statistical analysis
Data analysis was performed using SPSS version 22.0. Continuous variables were expressed as mean ± standard deviation (SD) or median (range), while categorical variables were presented as frequencies and percentages. The Chi-square test (or Fisher’s exact test) and independent t-test (or Mann-Whitney U test) were used for group comparisons. To identify independent predictors of mortality and complications, multivariable logistic regression analysis was performed. All associations were reported with 95% confidence intervals (CIs). Two-sided p-values < 0.05 were considered statistically significant.
Results
The baseline characteristics of the patients are shown in Table 1. As indicated in Table 1, most of the baseline characteristics in the two groups were in good agreement with each other. The incidence of renal failure and metastasis in patients who underwent cutaneous ureterostomy was significantly higher than in patients with an ileal conduit (both with p < 0.001). This is due to the fact that cutaneous ureterostomy was the preferred option for most high-risk patients. Additionally, it was found that the cutaneous ureterostomy method was significantly more frequently performed in patients with NX lymph node involvement (p = 0.05).
Basic characteristics of the MIBC patient who underwent ileal conduit or cutaneous ureterostomy following radical cystectomy.
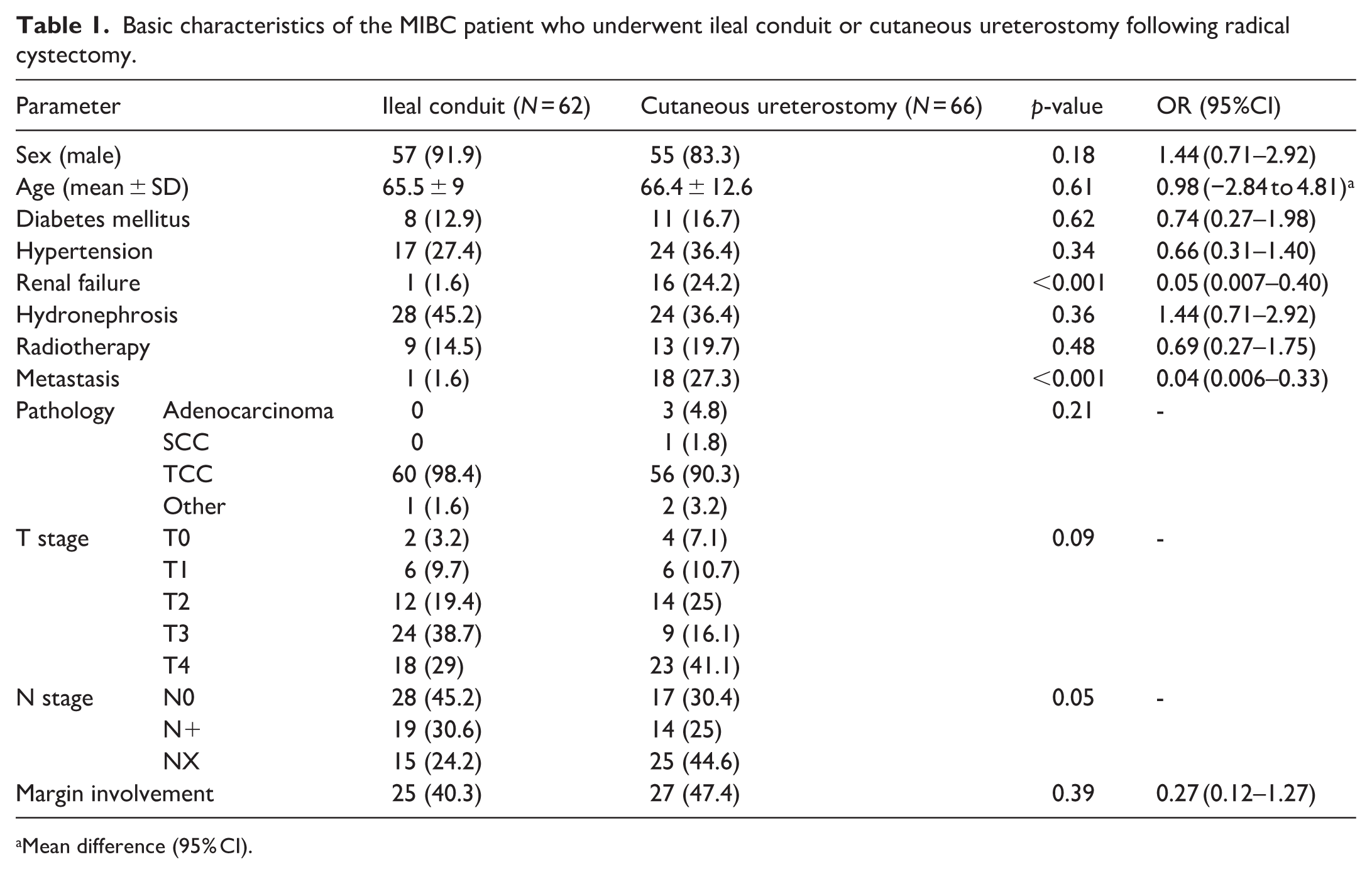
Mean difference (95% CI).
The differences in qualitative data between the two groups were evaluated (Table 2). Our data showed that there was no significant difference between the two groups (ileal conduit vs cutaneous ureterostomy) regarding complications during and after surgery, 30-day, 90-day, and 6-month survival, stoma stenosis, or the number of deaths due to cancer.
The differences in qualitative data between MIBC patients who underwent ileal conduit or cutaneous ureterostomy following radical cystectomy.
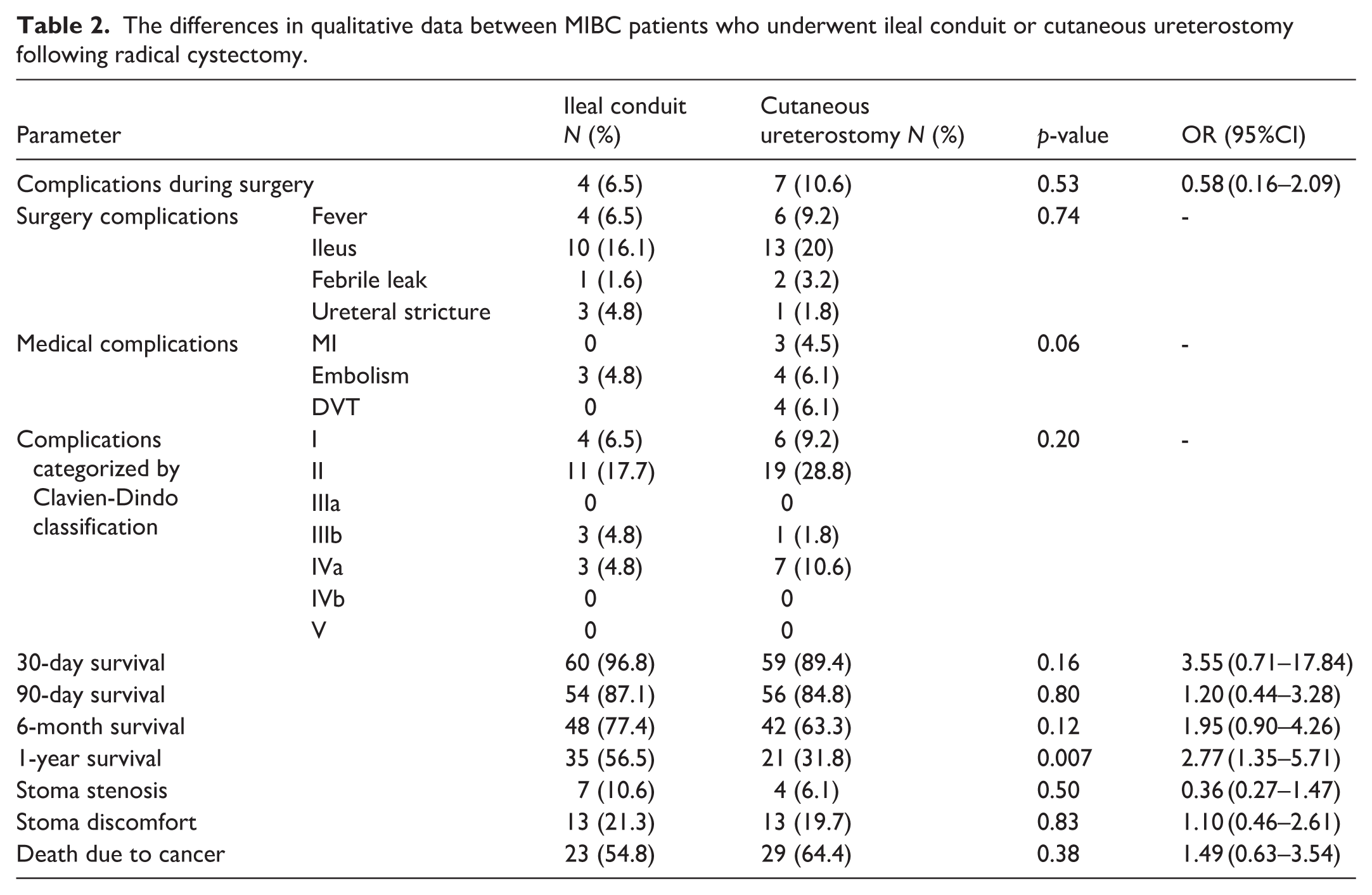
Postoperative complications were categorized according to the Clavien-Dindo classification. Although the CU group showed a lower frequency of adverse events, this difference did not reach statistical significance (p = 0.208). The majority of complications in both groups were minor (Grade I–II). Major complications (Grade III–IV) occurred in 9% of the CU group compared to 12.3% of the IC group.
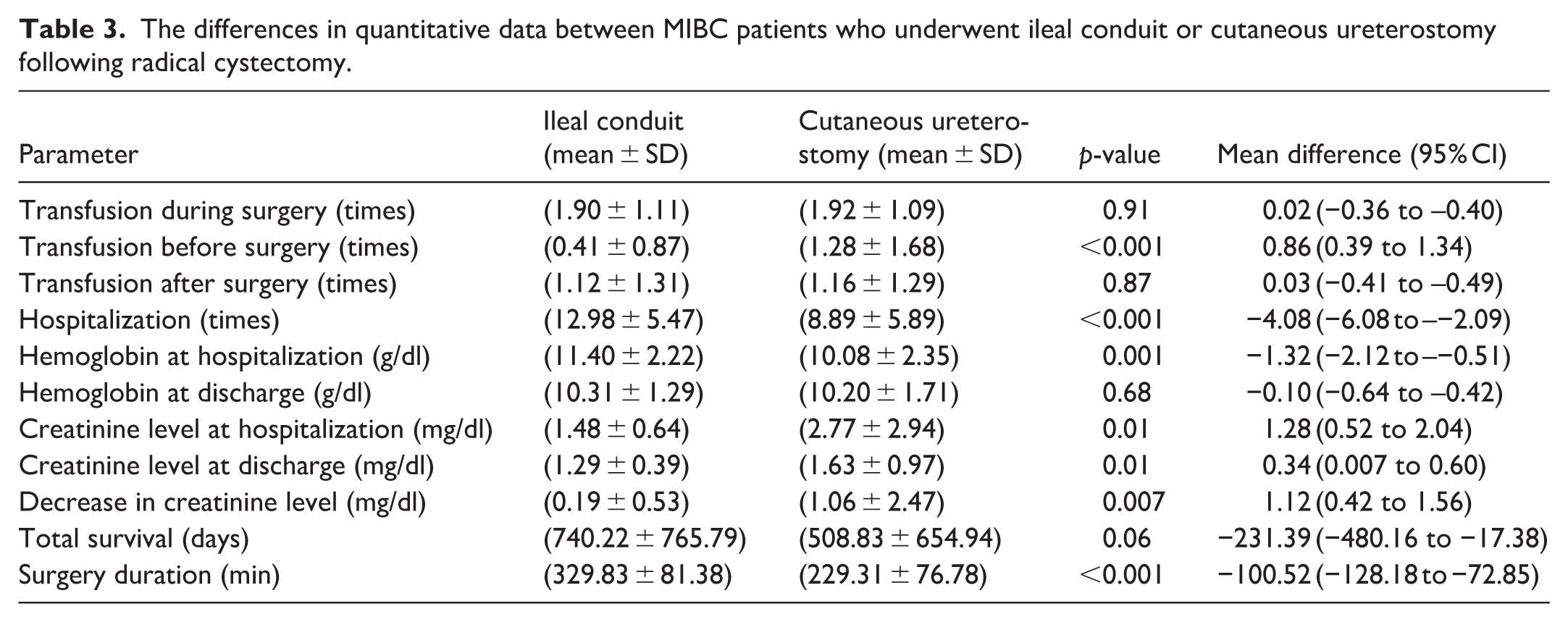
In follow-up studies after discharge, our findings showed that 1-year survival was significantly higher in patients who underwent ileal conduit. As shown in Table 3, the results of the quantitative data analysis showed that the duration of hospitalization after surgery, hemoglobin levels during hospitalization, and duration of surgery were significantly higher in the ileal conduit group. On the other hand, the number of transfusions before surgery, creatinine levels during hospitalization, and the creatinine level and creatinine drop at the time of discharge were significantly higher in patients undergoing cutaneous ureterostomy.
The differences in quantitative data between MIBC patients who underwent ileal conduit or cutaneous ureterostomy following radical cystectomy.
Furthermore, we evaluated the correlation of patients’ 30-day mortality in each group with factors such as transfusion frequency before, during, and after surgery, hydronephrosis, pathological stage, and positive surgical margins. Analyses showed that there was no correlation between the aforementioned characteristics and 30-day mortality in either group.
To identify independent predictors of 1-year survival, a multivariable logistic regression model was constructed. Initially, all clinically relevant variables, including age, sex, comorbidities (DM, HTN), urinary diversion type (ileal conduit vs cutaneous ureterostomy), and tumor characteristics, were entered into the model (Table 4). To refine the model and minimize the risk of overfitting, a backward elimination process was employed.
Multivariable logistic regression analysis of potential predictors for 1-year survival (dependent variable).
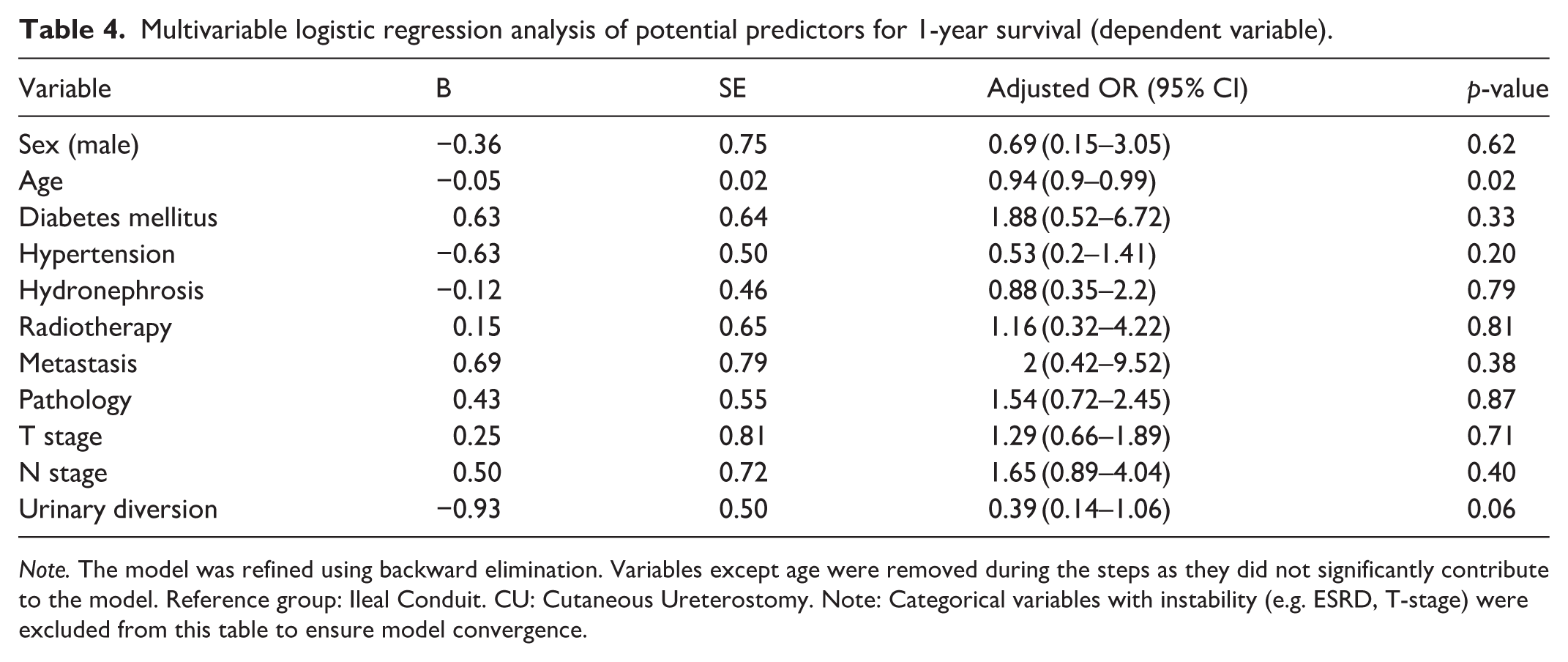
Note. The model was refined using backward elimination. Variables except age were removed during the steps as they did not significantly contribute to the model. Reference group: Ileal Conduit. CU: Cutaneous Ureterostomy. Note: Categorical variables with instability (e.g. ESRD, T-stage) were excluded from this table to ensure model convergence.
In the final step of the regression, age remained the only significant independent predictor of 1-year survival (OR = 0.953, 95% CI: 0.919–0.989, p = 0.010). This indicates that for every 1-year increase in age, the odds of 1-year survival decreased by approximately 5%. While the type of urinary diversion showed a trend toward significance in the initial model (OR = 0.394, p = 0.066), it did not remain an independent predictor in the final refined model. These findings suggest that the survival disparity observed in the univariate analysis was primarily driven by the advanced age of patients in the cutaneous ureterostomy group rather than the surgical technique itself.
Discussion
Bladder cancer (BC) ranks as the 10th most common malignancy worldwide. According to the EAU, NCCN, and AUA/ASCO/ASTRO/SUO guidelines, radical cystectomy (RC) remains the gold-standard treatment, significantly improving survival rates. 12 Research indicates that in-hospital mortality following RC is generally lower than 30-day mortality, which, in turn, is two to three times lower than the 90-day mortality rate.17 –19 While current guidelines recommend both RC and urinary diversion via an ileal conduit (IC) as standard care for muscle-invasive bladder cancer (MIBC), this study sought to evaluate whether cutaneous ureterostomy (CU) could serve as a strategic alternative to reduce morbidity and mortality in these patients.
Although clinical data on MIBC patients undergoing RC with CU are relatively scarce, existing evidence suggests that CU may significantly reduce perioperative risks. This technique minimizes operative duration and eliminates complications related to bowel manipulation, thereby potentially improving outcomes in patients with multiple comorbidities.20 –23 It is crucial to recognize that not every MIBC patient is a suitable candidate for RC, nor does every RC patient have an indication for an ileal conduit. Indeed, urinary diversion via an ileal conduit is associated with a substantial proportion of postoperative complications, 20 and mortality rates remain high across many surgical centers.20 –23 Consequently, tailored treatment decisions are essential, as meticulous management can significantly enhance life expectancy in high-risk individuals.
Incontinent urinary diversion offers a feasible and technically simpler approach to reestablishing urinary excretion post-RC, particularly for elderly patients. Among available options, the ileal conduit and cutaneous ureterostomy provide effective and optimal choices for selected patients. 24 Given the lack of head-to-head comparative studies, the present study evaluated these two methods. Our findings indicated that while demographic characteristics were well-matched, patients with higher baseline creatinine, renal failure, and metastasis were significantly more likely to be selected for CU. No significant differences were observed regarding 30-day, 90-day, and 6-month survival, or in surgical complications. However, while univariate analysis showed higher 1-year survival in the IC group, the CU group benefited from significantly shorter hospital stays and operative durations. Specifically, our study found the operative time for CU to be approximately 100 min shorter, which is consistent with other reports showing a reduction of about 80 min 25 although some studies, such as Knap et al., reported a shorter duration for the ileal conduit without statistical significance.
Regarding blood loss, previous research suggests that patients undergoing CU lose approximately 23% less blood than those undergoing IC, leading to lower transfusion requirements.21,25 In contrast, our study found comparable intra-operative transfusion rates, though pre-operative transfusions were significantly higher in the CU group—a reflection of the higher baseline frailty and clinical complexity of these patients. Furthermore, our results showed that the decrease in creatinine levels was more pronounced in the cutaneous ureterostomy group, likely due to the superior ultra-drainage provided by this method, making it a potentially better choice for patients with renal impairment.
A pivotal finding of our study emerged from the multivariable analysis, which clarified the relationship between the type of urinary diversion and patient survival. While univariate analysis initially suggested a survival advantage for the ileal conduit (IC) group, this effect was not sustained after adjusting for potential confounders. Our final regression model identified advanced age as the sole independent predictor of 1-year survival (OR = 0.953, 95% CI: 0.919–0.989, p = 0.010), rather than the surgical technique itself. This indicates that for every 1-year increase in age, the odds of 1-year survival decreased by approximately 5%.
This distinction is clinically significant and suggests that the lower survival rates observed in the cutaneous ureterostomy (CU) group are a reflection of “confounding by indication” or selection bias. Specifically, CU was predominantly offered to significantly older and frailer patients who already possessed a higher baseline risk of mortality. When these factors were accounted for through a stepwise backward elimination process—a method we employed to minimize the risk of overfitting and ensure the robustness of our model—the choice of diversion (CU vs IC) did not independently jeopardize survival outcomes.
Our results align with the growing body of evidence suggesting that for elderly patients with multiple comorbidities, the priority should be the minimization of surgical stress. The significantly shorter operative time and reduced blood loss associated with CU provide a crucial physiological advantage for high-risk individuals. By avoiding bowel-related complications and reducing the overall surgical burden, CU serves as a safe and pragmatic alternative to the more invasive ileal conduit in the “frailest” patient populations. However, we acknowledge that the trend toward significance for urinary diversion type in our initial model (p = 0.066) suggests that larger, prospective studies are still needed to further delineate these associations and establish precise clinical criteria for diversion selection.
Despite these insights, our research has limitations, including its retrospective design and potential selection biases. Future prospective, multicenter studies with randomized designs and standardized complication grading (e.g. Clavien-Dindo) are warranted. Moreover, subsequent research should focus on evaluating quality of life and establishing precise clinical criteria for selecting diversion techniques based on individual risk profiles post-radical cystectomy. In conclusion, cutaneous ureterostomy represents a safe, efficient, and competitive alternative to ileal conduit for elderly and high-risk patients. Its perioperative advantages—including shorter operative time, reduced hospitalization, and rapid creatinine decline—make it a reasonable choice when minimizing surgical stress is clinically paramount.
Conclusion
In conclusion, cutaneous ureterostomy serves as a safe and efficient alternative for elderly and frailer patients requiring urinary diversion. Our study demonstrates that this technique offers significant perioperative advantages, including shorter operative time, reduced blood loss, and shorter hospital stays. Crucially, multivariable analysis revealed that the observed differences in 1-year survival were driven by advanced age and baseline comorbidities rather than the surgical technique itself. Given that complications and mortality rates remain comparable to ileal conduit after adjusting for confounders, cutaneous ureterostomy should be considered a viable, less invasive option for high-risk patients.
Footnotes
Ethical considerations
An ethical code approved the preparation of this paper and project (IR.SBMU.MSP.REC.1400.448.) Shahid Beheshti University of Medical of science.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that supports the findings of this study are available in the article.