
Abstract
Introduction:
Robot-assisted partial nephrectomy (RAPN) is currently the gold standard for localized renal tumors. The surgical approach can be performed using either an on-clamp or off-clamp technique. The aim of the study is to evaluate differences in positive surgical margins (PSMs) and perioperative complications between on-clamp and off-clamp approaches of RAPN, at all levels of tumor complexity.
Methods:
We retrospectively enrolled 478 patients who underwent RAPN between 1/2020 and 6/2024 and divided into two groups: A (on-clamp) and B (off-clamp). We stratified tumor complexity according to the RENAL score and analyzed all perioperative and oncological outcomes: PSMs, post-operative creatinine changes, intra- and post-operative complications, duration of procedures. For multivariate statistical analysis we used the Chi-square test.
Results:
In 83 procedures clamping of the main renal artery was performed (in no case was selective clamping performed). Median value for duration of clamping was 16 minuts. In patients who have undergone ischemia, the duration of ischemia is correlated with the increase in postoperative creatinine (p < 0.001). There was a significant difference in the duration of the procedures between the two groups: group A (median value 90ʹ), group B (median value 120ʹ) (p < 0.001) while no difference regarding perioperative complications (p = 0.34) or PSMs (p = 0.73).
Conclusions:
Both the on-clamp and off-clamp approaches are considered safe and feasible, provided there is adequate surgical experience. The complication rate was similar, as were the oncological outcomes and but post-operative creatinine increases proportionally to the duration of ischemia. In on-clamp procedures the increase in postoperative creatinine is directly related to the duration of ischemia. The off-clamp procedure is shorter with no difference in surgical and oncological outcomes.
Keywords
Introduction
Partial nephrectomy (PN) is the gold standard treatment for localized renal tumors, as it offers oncological outcomes comparable to radical nephrectomy (RN), while providing various degrees of preservation of renal function associated with a survival advantage.1,2 PN can be either performed with a laparoscopic, robotic-assisted partial nephrectomy (RAPN), or open partial nephrectomy (OPN) surgical approach.3 –5 In some selected cases and where there is great surgical experience it is possible to perform PN even in tumors >7 cm (cT2). 6 There are several nephrometric scores that can predict the complexity of renal masses, and therefore also the probability of post-operative complications. 7 There is no absolute superiority of one surgical approach but RAPN has shown superiority regarding post-operative complications and patient comfort. 8 There is now a great deal of discussion in the literature about the comparison between the on-clamp and off-clamp procedures, but there is starting to be evidence that there is no significant difference between the two techniques. 9 The goal of the on-clamp procedure is to prevent massive bleeding during tumor enucleation and to minimize the possibility of PSMs. 10 The off clamp procedure requires great surgical experience in managing bleeding, but minimizes renal ischemic damage, therefore very effective in patients with chronic renal failure (CRF). 11 The off-clamp procedure has demonstrated a shorter operating time in some meta-analyses with statistically significant differences and similar surgical and oncological outcomes. 12 Our aim is to compare the two techniques on surgical and oncological outcomes and, above all, to determine to what degree of complexity the two techniques can be defined as safe and feasible.
Materials and methods
In this retrospective cohort study we enrolled all patients affected by renal tumor between January 2020 and June 2024, in a single referenced center for robotic surgery (Da Vinci Xi system), which includes three different teams of urologists. All urologists who performed RAPN had a medium-high level of surgical autonomy (>100 procedures). The exclusion criteria were represented by patients’ general health conditions (for other comorbidities) that made impossible for robotic surgical approach.
All procedures were performed using the transperitoneal approach.
For each procedure, the duration, post-operative complications using the Clavien-Dindo classification, surgical complexity using the RENAL score, histological characteristics with particular attention to positive surgical margins (PSMs) were analyzed.
The complication ‘anemia’ was attributed when the patient required blood transfusion (Clavien 2).
We divided all patients in two groups, Group A (on-clamp) and Group B (off-clamp), and we performed a comparative measurement between the groups looking for any correlations between surgical complexities and complications or PSMs. In the Group A, ischemia time was also evaluated.
Statistical analysis
For multivariate statistical analysis we used the Chi-square test, looking for statistically significant differences in the two groups regarding PSMs, postoperative morbidity (with greater attention to anemia), changes in creatinine levels and duration of procedures. The level of significance was established for p value ⩽ 0.05.
Results
Median value for age was 67 years (range 28–87). In six cases the procedure was bilateral. The median value for procedure duration was 90 min (σ: 40.03; range 30–285), for hospitalization 3 days (σ: 1.02; range 2–13). Histology and TNM classification are described in Figures 1 and 2. The tumors were predominantly localized masses and T3 tumors were classified only after analysis of the specimen and finding involvement of the perirenal fat. In 83 procedures (29.8%), clamping of the main renal artery was performed (in no case was selective clamping performed). Median value for duration of clamping was 16 min (σ: 8.23, range 7–65). In patients who have undergone ischemia, the duration of clamping is correlated with the increase in postoperative creatinine (p < 0.001).
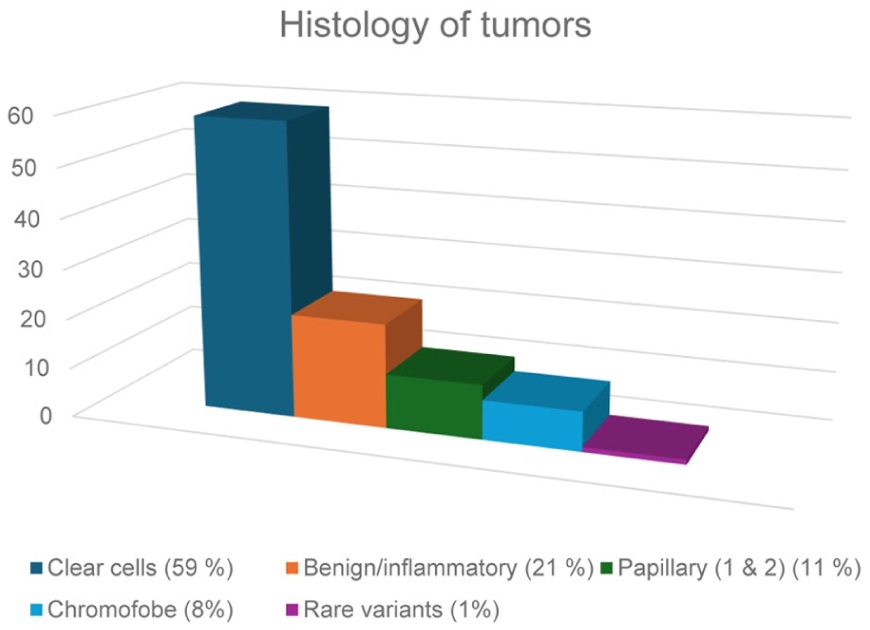
The graph shows the distribution of the histological variant.
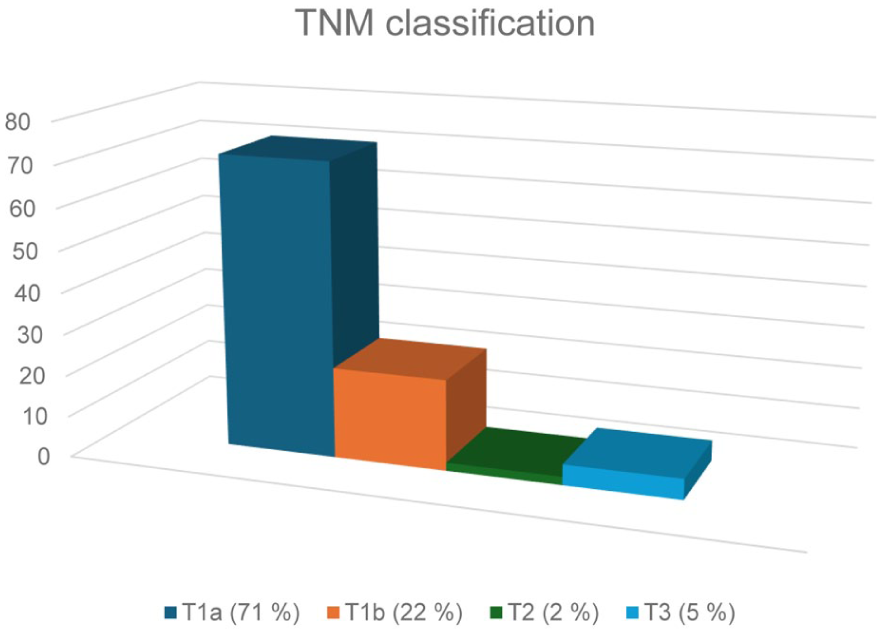
The graph shows the distribution of pathological TNM stage (pTNM).
The duration of the interventions was then analyzed in the two groups. Off-clamp had a median value of 90′ (σ: 39.36; range 30–285) and on-clamp group 120′ (σ): 35.58 range 80–240). The difference in the two groups was statistically significant (p ⩽ 0.001). The duration of the procedures increased proportionally with the progression of the RENAL score (p = 0.018).
Surgical complexity was analyzed according to the RENAL score and divided as follows: 248 cases low complexity (score 4–5), 179 intermediate complexity (score 6–7), 51 high complexity (score 8–9).
Twenty-three cases (4.8%) had a post-operative complication divided as follows: two cases with Clavien 3 where it was necessary to perform arterial vessel embolization for anemia and ureteral stent for ureteral damage with leakage, twelve cases with Clavien 2, in patients with anemia who required blood transfusion and nine Clavien 2 in patients undergoing antibiotic or infusion therapy.
In 13 procedures (2.7%) an intraoperative complication occurred with concomitant surgical repair. None of these complications required retreatment.
Considering the surgical complexity, clamping was performed in 4% of the low complexity cases, in 26.8% of the intermediate complexity cases, and in 49% of the high complexity cases. Among the on-clamp patients only three patients had post-operative complications (3.6%), and among the off-clamp patients 20 patients (5%), of which 10 had anemia (2.5%). Although there is a slight difference between the two groups, there is no statistically significant difference, especially regarding anemia (p = 0.34).
The final rate of PSMs was 4.52% (22 cases). More specifically, PSMs were evident in five procedures performed with arterial clamping (6%) in 17 procedures (4.2%) performed with off-clamp technique. Although the number of cases with PSMs is rather small, we did not find statistically significant differences between the on-clamp and off-clamp groups. Tumor size also did not have a clear correlation with PSMs (p = 0.73).
The same result was also demonstrated by correlating differences between the two groups (on-clamp and off-clamp) in histological variants, without any statistically significant difference (p = 0.59) .
Finally, there is no direct correlation between complications and tumor size.
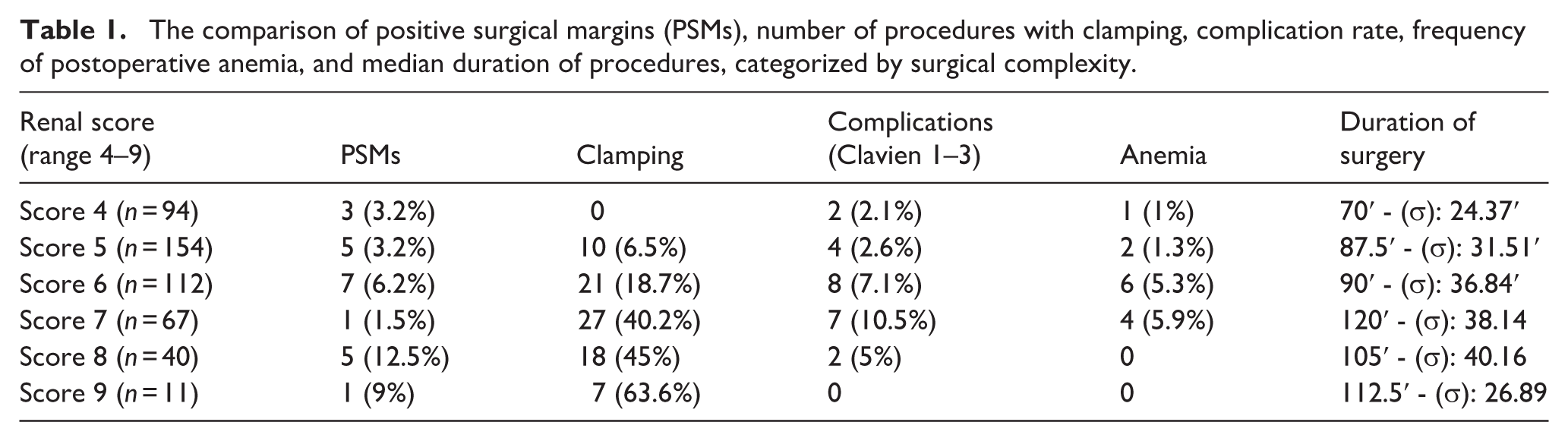
All data are illustrated in detail in Table 1.
The comparison of positive surgical margins (PSMs), number of procedures with clamping, complication rate, frequency of postoperative anemia, and median duration of procedures, categorized by surgical complexity.
Discussion
RAPN represents an evolving technique that will become increasingly preferred over OPN.13,14 The technique is, in fact, better standardized with a faster learning curve for young surgeons.15 –17 Although the robotic approach is becoming more popular, there is no clear evidence on which technique performed is more effective and safe. The aim of this work is to compare the differences regarding one part of RAPN, that is the possibility of performing the procedure with or without arterial clamping. In literature the two approaches are well compared and there are no differences in post-operative and oncological outcomes18 –20 and, sometimes, it is also possible to find a better post-operative outcome with the off-clamp technique. 21 There are no studies relating to learning difficulties in the two techniques. In the on-clamp approach the main difficulty is to obtain a good exposure of the renal arterial pedicle, so as to perform the arterial clamping safely. In the off clamp approach the main difficulty is having to perform the tumorectomy with a greater risk of bleeding, which therefore requires greater speed (a prolonged duration can cause serious anemia) and safety of the anatomical planes. Undoubtedly the best approach is the one with which the surgeon manages to obtain an excellent outcome. However, there are particular conditions, for example in patients with a single kidney, or those who have undergone previous renal surgery, where the off-clamp approach should be preferred. Currently there is no evidence of a better approach, nor of significant differences even for large tumors. 22 A very interesting finding of our work is that there is no increase in the complication rate in high-complexity patients performed off-clamp. This is possible due to an effective standardization of surgical training and robotic technique that allows increasingly complex procedures. 23 There are several limitations in our work, especially regarding the number of patients and the number of surgeons who performed RAPNs. The discussion on the surgical technique is destined to continue and our center is already working to expand the number of patients, involving other centers and giving greater robustness to the data examined so far. In fact, the extremely low number of PSMs of events reduces the statistical power and makes it difficult to identify potential predictors.
Conclusions
In the three centers where we enrolled patients, we did not find statistically significant differences between RAPNs performed on-clamp and off-clamp, both for low-complexity and high-complexity tumors. The complication rate was similar, as were the oncological outcomes but post-operative creatinine increases proportionally to the duration of ischemia. The off-clamp procedure is shorter with no difference in surgical and oncological outcomes. RAPN is still a complex surgical procedure, so it is essential that the surgeon chooses the technique that can guarantee the best clinical and oncological outcome.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.