
Abstract
Using Social Structure of Accumulation (SSA) theory, I analyze how structural economic changes shaped two cases of US healthcare legislation: the Clinton Health Security Act (HSA) of 1994 and the Patient Protection and Affordable Care Act (ACA) of 2010. I argue that the failure of the HSA and the passage of the ACA must be understood in relation to their contemporary SSA—the set of dominant institutions and ideas that facilitates capitalist accumulation. In each case of reform, the structures of the proposed policies, as well as their support, opposition, and ultimate legislative outcomes, all reflect the concurrent restructuring of US capitalism. This analysis clarifies the interplay of neoliberal capitalism and US healthcare and contributes to our understanding of the connections between capitalist economic relations and the provision of healthcare.
1. Introduction
President Obama’s signing of the Patient Protection and Affordable Care Act (ACA) in March 2010 was hailed as a major success in a century-long struggle over healthcare reform in the United States. 1 Just some sixteen years earlier, healthcare reform had been named an unwinnable political fight following the demise of the Clinton Health Security Act (HSA). 2 Why was such a significant healthcare reform able to pass after withstanding the proposed changes of the 1990s? What factors influence the success or failure of healthcare reforms? Clear answers to these questions are essential for elucidating the interconnections between capitalist economic relations and healthcare reform and how they change over time. The most popular analyses of these reforms examine the interrelated roles of culture, institutions, and group conflict in shaping the different outcomes. An analysis of these two healthcare reforms in the context of the changing structures of capitalism yields important insights.
2. Abbreviated Literature Review
Many accounts of the Obama administration’s success highlight lessons learned from Clinton’s failure. Altman and Starr, both political insiders during these reforms, each document how the Obama administration intentionally developed their healthcare policy strategy as the antithesis of Clinton’s (Altman and Schactman 2011; Starr 2011). In their accounts, both the legislative process and the financing details were calculated with the HSA’s failure in mind. Other researchers suggest that some of the cultural features present in the 1990s were different by 2010. For instance, Jacobs and Skocpol (2010) suggest that the increasing income inequality and the public awareness of that inequality made the American public more supportive of healthcare reforms, especially after the rapidly increasing unemployment numbers throughout 2008 and 2009.
Other analyses discuss how the stakeholders credited with blocking reform in the 1990s responded differently during the Obama presidency. Brown (2011: 425) recounts the “decision of previous enemies of reform to play a different game.” Hacker (2011) and Swenson (2018) discuss the changed interests of health insurance companies, employers, and medical providers. Brill (2015) and Quadagno (2011) analyze the ways in which stakeholder coalitions were successfully organized to support reform. Work by Hacker (2011) and Tuohy (2018) suggests that political institutions were more adaptable to the reforms of the ACA because of the feedback effects of previous policies.
Although this literature includes persuasive analyses of the policy outcomes, the literature is so far incomplete. Suggestions of the political savviness of the Obama administration are dampened by the partisan nature of the vote and the continued struggles over the ACA. The connections between public sentiment and the passage of healthcare reform are also not convincing. Gilens and Page (2014) have demonstrated that public sentiment is not often correlated with public policy decisions, and Navarro (1995) has documented evidence of support of national healthcare reform among the so-called American public. Similarly, if the HSA’s failure and the ACA’s success are attributed to various groups’ power waxing and waning over time, some explanatory framework for these shifts in power is required. It is not sufficient to name changes of group power, attitudes toward healthcare reform, and the adaptability of political institutions as the explanatory variables in the outcomes of reform. These changes and their effects on healthcare reform must themselves be analyzed.
3. Social Structure of Accumulation Theory
I suggest that social structures of accumulation (SSA) theory, which yields insights into how and why the changes in institutions, ideas, and the relative power of groups came about, is well suited to answer the questions posed above. Most importantly for our purposes, SSA theory offers an account of why and how these changes produced different outcomes for healthcare reform in different times. Section 3.1 briefly discusses the main characteristics of SSA theory. Section 3.2 specifies the concept of neoliberal capitalism. Section 3.3 introduces the two case studies of how the dynamics of neoliberal capitalism shaped healthcare reforms.
3.1. SSA theory overview
Political economists developed SSA theory in the late 1970s and early 1980s as a framework to analyze capitalism’s alternating periods of stability and crisis and the distinct features of capitalism as it developed. Gordon et al. (1982), who present the first systematic definition of an SSA, explore the relationship between the dynamics of capitalism and changes in the labor process and labor markets. SSA theory has since been further developed and modified in the works of Bowles et al. (1990), Kotz and McDonough (1994), and McDonough et al. (2010). I draw from this series of books to present the main characteristics of SSA theory below.
SSA theory analyzes the various distinct forms of capitalism that have arisen as comprising of a cohesive set of long-standing practices or behavior patterns. According to SSA theory, a mutually reinforcing set of economic, political, and cultural institutions and dominant ideas emerges in each period to support the existence and reproduction of the capitalist economic system. This set of institutions and ideas, referred to as the SSA, functions jointly to regulate the key aspects of the capitalist economy. For example, an SSA helps promote positive rates of profit, maintains total demand growth, and creates stability for investment decisions. O’Hara (2000) identifies five key institutional spheres of an SSA: the capital-labor relationship, the international regime, the domestic household order, the state-citizen accord, and the financial system.
The success of an SSA in regulating the key processes and relationships of capitalism is limited. Historically, periods of recession have followed long periods of relatively stable capitalist accumulation. SSA theory understands these occurrences as distinct phases within an SSA. Each SSA is marked by a period of consolidation and a period of decay. In the initial consolidation period of an SSA, the joint set of economic, political, and cultural institutions and dominant ideas are mutually reinforcing and effectively promoting stability and profitmaking. Eventually, however, the institutions will break down and stop promoting effective accumulation.
The inability of the institutional structure to continue to promote accumulation marks the transition to the crisis phase of an SSA, or its period of decay. This definition of crisis distinguishes the term from an economic recession or downturn, which may happen during the consolidation period of an SSA but can be resolved through the normal policy tools. According to SSA theory, only the construction of a new SSA and its corresponding set of institutions can resolve such a crisis and accommodate continued capitalist accumulation. Until a cohesive and mutually reinforcing set of institutions and dominant ideas emerges, the crisis prompts a prolonged conflict in society over how to best restore the conditions of stable accumulation. Various groups will take advantage of that destabilization to pursue their own interests, and each institution will become an area of competition.
3.2. The concept of neoliberal capitalism and its crisis
This article builds on previous work that uses the concept of neoliberal capitalism to refer to a particular structural form of capitalism that emerged in the late 1970s and early 1980s and entered into crisis in 2008 (Kotz 2009; 2015; Kotz and Basu 2019; Kotz and McDonough 2010). A detailed analysis of the characteristics of the neoliberal SSA and its crisis appears in Kotz (2015) and cannot be fully summarized here. However, two key features of the neoliberal SSA’s consolidation and crisis phases are relevant for the case studies and require articulation: the dominant ideology and associated class relationships. These two features of neoliberal capitalism and evidence of their destabilization following the crisis that began in 2008 are briefly explained below. 3
The dominant ideology of the neoliberal SSA, called neoliberalism or neoliberal economic theory, differed from the Keynesian economic theories that successfully promoted accumulation in the previous SSA. Neoliberal economic theories focus on individuals and their choices as expressed in market relations. Market forces, as opposed to institutions like the government or labor unions, play a stronger role in economic regulation and allocation. Neoliberal economic theories viewed government regulations as inefficient and repressive and instead promoted the deregulation of many industries, including electric power, airlines, and the financial industry. In areas where the government had taken a significant role in providing public services, many of these services were privatized or contracted out to private companies.
The labor market under neoliberal capitalism changed significantly as well. As efforts by capital under neoliberalism to decrease rates of unionization were effective, employers gained significant power in defining the terms of employment and creating “flexible labor markets.” In the neoliberal SSA, the labor market was characterized by wage stagnation and declining employer-sponsored benefits. 4 It is important to note, however, that the promotion of market relations does not entirely erode the government’s role in allocation and regulation. Neoliberal ideology should not be interpreted as strictly antagonistic to the state. Certain activities of the state, such as its enforcement of intellectual property rights and its promotion of policing and military activities, have expanded significantly alongside the retrenchment of public services and social programs. This trend suggests that the neoliberal state is not a state with diminished capacity, but instead a state that strongly enforces the promotion of private property rights.
Kotz (2015: ch. 5) argues that the crisis that began in 2008 is best understood as a structural crisis of the neoliberal SSA. Following SSA theory, the structural crisis of the SSA is defined by the inability of the institutions and ideas of the neoliberal SSA to continue to promote effective accumulation. Several developments illustrate the destabilization of the dominant ideas and institutions of the neoliberal SSA, including the massive government bailout, the public denunciation of neoliberal ideology by its strongest supporters, and the reinstitution of regulations in the financial sector (Kotz 2015: 144–60).
4. Case Study Introduction
The following two case studies analyze two healthcare reform proposals in the context of the phase of neoliberal capitalism in which it was proposed. The Clinton administration’s HSA was proposed in neoliberal capitalism’s consolidation phase, when the institutions and ideas of neoliberal capitalism were well entrenched and effectively promoting capitalist accumulation. The Obama administration’s ACA, on the other hand, was enacted after neoliberal capitalism had been destabilized by the economic crisis of 2008. In each case study, I analyze how the proposed healthcare reforms—and the corresponding dynamics of interest group support or opposition—reflect neoliberal capitalism’s changing boundaries.
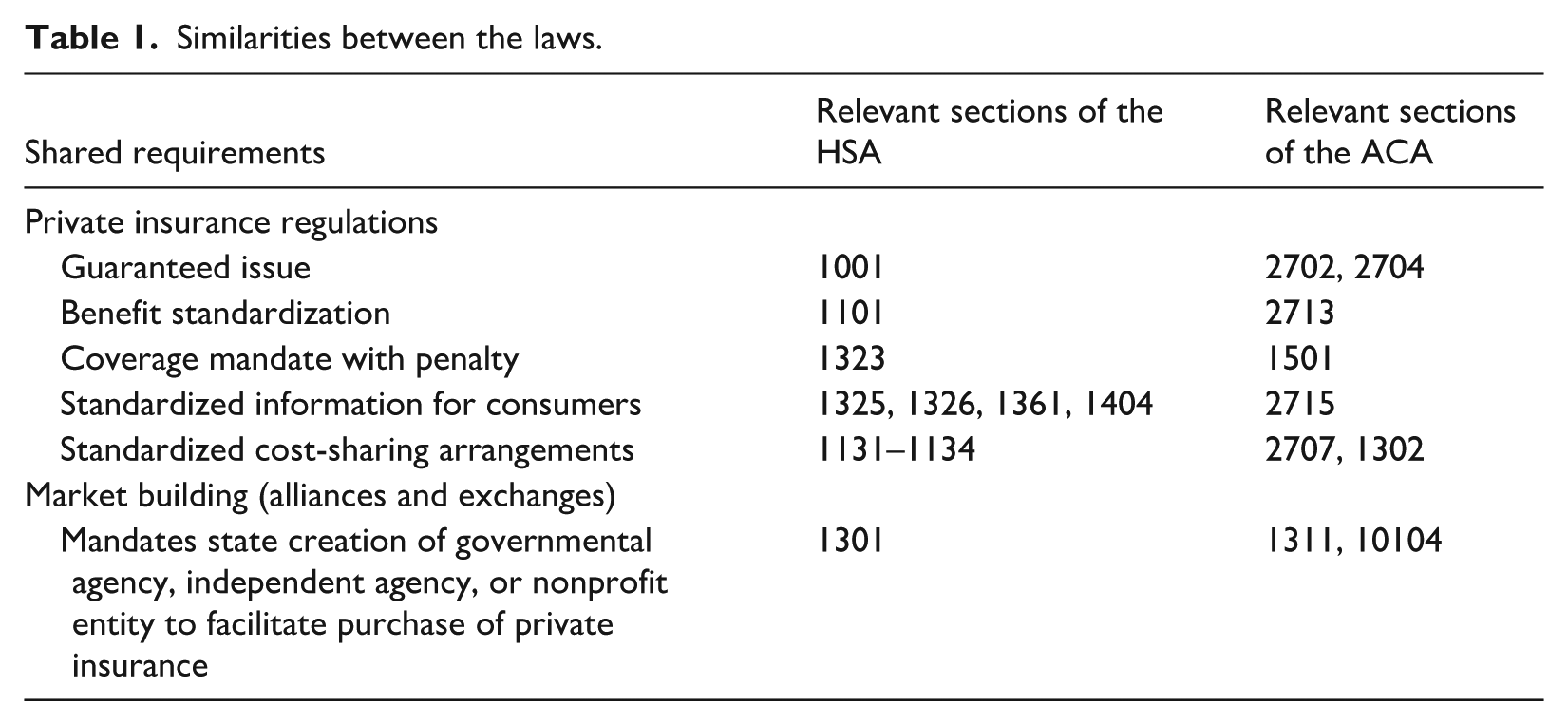
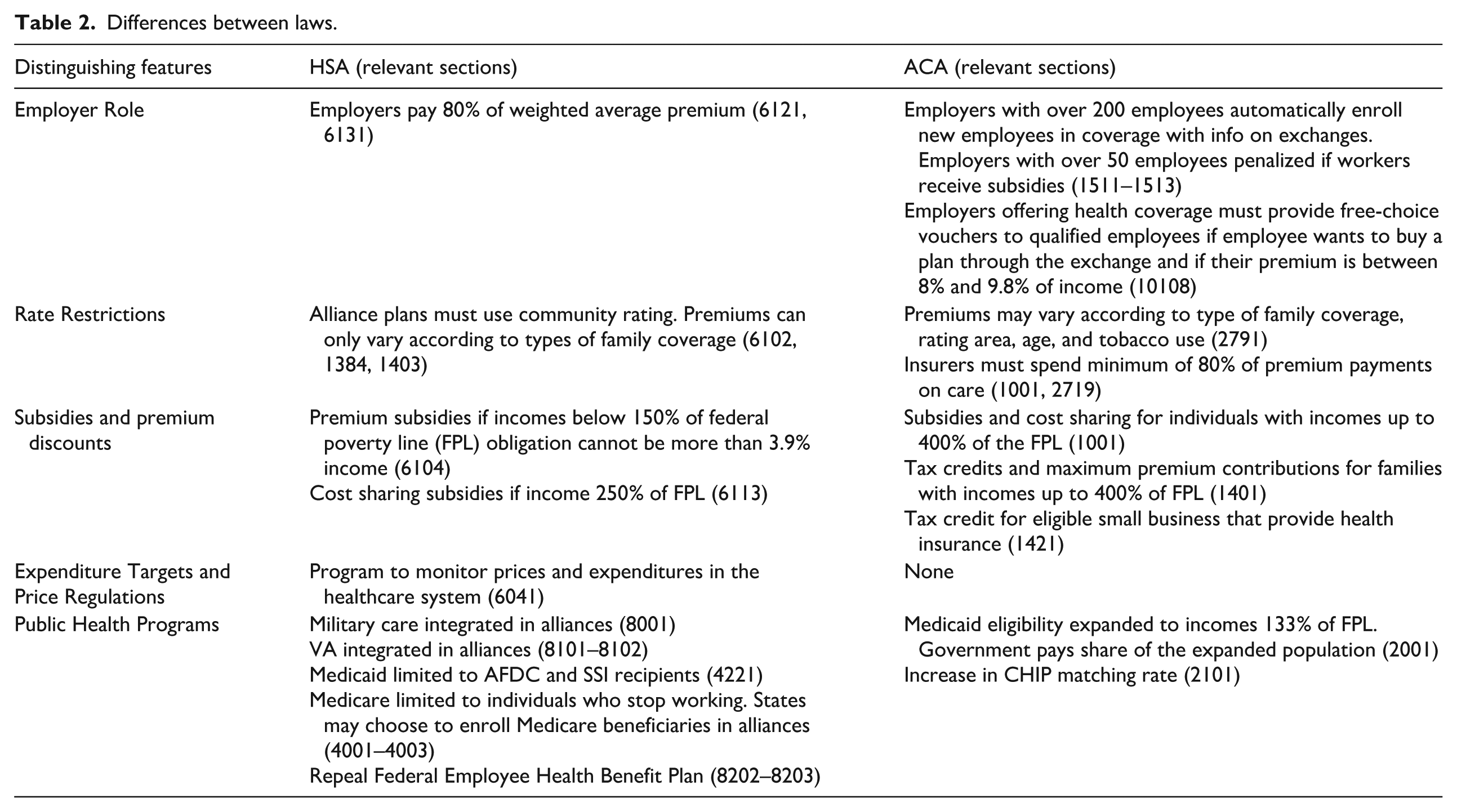
It is worth noting that there are many broad similarities between the Clinton administration’s HSA and the Obama administration’s ACA. Both policies relied on expanding and maintaining the private health insurance system. As table 1 demonstrates, both proposals mandated insurance coverage for individuals, regulated the private insurance industry, and detailed the creation of market building institutions, which were either referred to as alliances or exchanges. The most significant differences between the proposals were in the role of employers and the effects on public health insurance programs, as shown in table 2. The case studies below highlight how each policy’s similarities and differences reflect the institutions and ideas of the neoliberal SSA’s consolidation and destabilization.
Similarities between the laws.
Differences between laws.
The case studies add to the existing literature on these two healthcare reforms highlighted above. They also contribute to the broader studies of the concept of health capitalism, an academic field that analyzes the interdependence of capitalist economic relations and the healthcare sector (Batifoulier et al. 2025). SSA theory’s focus on the changing institutions of capitalism provides a systematic framework for analyzing the interconnections between healthcare and capitalism and how they are reconstituted over time. 5
5. Case Study 1: The Failure of the Health Security Act
5.1. Cohesion with neoliberal capitalism
The HSA reflected the neoliberal SSA’s dominant ideas and class relationships. For example, the HSA required insurers to sell two types of managed care plans with mandated premiums and coinsurance or copayments. As discussed by Gaffney (2015) and Navarro (2008), the principles of managed care are a direct application of neoliberal ideologies of rational behavior as applied to patients and providers. The law’s design also mirrored the recent developments in the private health insurance industry. First, as employers dealt with rising healthcare costs, they became more reliant on managed care plans, which helped employers minimize their expenses in the context of rising healthcare prices (Gabel et al. 1987). Second, the changed role of the government in the economy in the neoliberal SSA had promoted regulatory rollback in health insurance, which made self-insured coverage a more attractive option for large employers. 6 The increasing trend of self-funded insurance by firms in the 1980s and 1990s further catalyzed health insurance companies to invest in the creation of managed care networks. 7 When firms use self-financed insurance, they do not necessarily cut out the role of the private insurance company. Private insurance companies can maintain their role in employer self-funded health insurance by establishing managed care networks and negotiating contracts with providers (Gabel et al. 1987).
Another significant feature of the HSA that reflected the institutions of the neoliberal SSA was the HSA’s privatization of public goods and services. The HSA did not explicitly privatize the existing programs of Medicare, Medicaid, and the Veterans Affairs (VA) facilities. However, the law did call for the integration of many aspects of these programs into the regional health alliances. These aspects of the HSA effectively redistribute a large share of healthcare costs previously paid by the state and federal governments to employers and private individuals. The redistribution reflects the changing role of the state in the neoliberal capitalist SSA and is consistent with the trend toward privatizing and contracting public services. The major changes in Medicare and Medicaid were framed as part of a strategy for reducing the government deficit and expanding domestic investment (Department of Commerce and Technology Administration 1993: 30–34; Johnson and Broder 1997: 123).
5.2. Contradictions with neoliberal capitalism
The HSA also included distinctive features that seemed to contradict the dominant ideology and associated class relationships of neoliberal capitalism. The employer mandate, which would require employers to pay for 80 percent of employees’ premium costs, subject to a cap as a percentage of their payroll, is one such example. Second, the HSA also included proposals designed to reverse the trend of rising medical care prices that exceeded the rate of inflation: premium caps and expenditure targets. These aspects of the law proved to be a contentious aspect of the legislation. The group of academics, business owners, and representatives from the healthcare industry that had worked on the prototype of Clinton’s proposal publicly rejected these elements as incompatible with their model (Ellwood and Enthoven 1993).
The Clinton administration framed the employer mandate as consistent with the dominant ideology of neoliberalism. The opening sentences of an overview of the HSA illustrates:
The Health Security Act rejects the idea of a government-run health care system. Health care will remain rooted in the private sector.. . . The vast majority of money comes from the same place it comes from today: employers and individuals. But under the health security plan, every employer and every individual will be asked to contribute to health care. Everyone takes responsibility, and everyone gets security. (Domestic Policy Council and Clinton 1993: 26–27)
Having explicitly rejected a government-run healthcare system, expanding health insurance coverage through workplaces was an obvious alternative. Employment-based health insurance was the most common way for individuals to access private insurance in 1993 (Fronstin 1996). However, the employer mandate was not heralded as a safeguard against government-run health insurance; it was criticized as an excessive additional cost that was not cohesive with the neoliberal economic ideology’s promotion of market relations. 8 The Clintons and their proxies similarly maintained that the use of premium caps were intended as tools to maintain the private market and lower the budget deficit. They described the use of premium caps and global budgets as a way to “aggressively control costs through market-based competition backed up by an enforceable budget” (Department of Commerce and Technology Administration 1993: 98). However, the contradiction between price and spending controls and market forces undercut the effectiveness of these arguments. In a letter to Ira Magaziner, Paul Ellwood and Alain Enthoven predicted that government price setting will halt “investment in corporate restructuring, service expansion, and performance reporting” (Ellwood and Enthoven 1993: 2).
Neoliberal capitalism offers a coherent framework for understanding major aspects of the HSA. Nevertheless, the complexities of the concept, particularly with respect to the government’s role in promoting private property rights, do present tensions with some of the strategies of the Clinton administration. The apparent tensions inherent in using the authority of the government to cement the existence of a private insurance industry are nontrivial but ultimately do not undermine the coherence of the HSA with neoliberal ideology.
5.3. Neoliberal capitalism and group conflict
The dominant ideas and institutions of the neoliberal SSA also were reflected in how the group conflict over the HSA played out. The conditions of neoliberal capitalism shaped the perceived interests of groups, how they articulated these interests, and the success of their strategies.
5.3.1. Health insurers
Because many of the proposed reforms mirrored the changes that large insurance companies had already been making, CEOs of large insurance companies publicly expressed support for many of the Clinton administration’s changes. A Prudential Insurance Company newsletter from 1993 explicitly identified a managed competition proposal as “the best scenario for reform—preferable even to the status quo” (qtd. in Navarro 2008: 208). The five largest insurance companies created the Alliance for Managed Competition, which established a media campaign to promote reform, as well as published research and conducted opinion polls about managed competition models for healthcare reform and shared their results with the Clinton administration (The Alliance for Managed Competition 1993).
Small and medium-sized insurers, on the other hand, were threatened by aspects of the proposed Clinton healthcare reforms. Although the HSA maintained a commitment to preserving the private insurance industry, small insurers feared that the proposed reforms were not compatible with their existing business practices. Unlike the large insurers, small insurers had not invested in creating managed care networks and their business practices differed substantially from the large insurers. Instead of profiting by creating managed care networks, they profited by managing risks (The Center for Public Integrity 1995b: 598). However, the industry’s lobbying group, the Health Insurance Association of America (HIAA) understood that defending the status quo was not a good political strategy. So, the group was not in outright opposition to the Clinton proposal. Instead, the group released their own proposal for health insurance reform. Later remarks from the group’s leader, William Gradison, revealed that the HIAA’s public statements were part of a strategy of blocking reform, not signals of the group’s “willingness to accept significant changes,” as the New York Times had previously speculated (Pear 1992: A1). In a keynote address, Gradison commented that, “From a political point of view, you can vote against another plan and convince your constituents that you want something done about healthcare reform as long as you have a plan you are for” (Gradison 1993a: 325).
In the context of the consolidated neoliberal SSA, the HIAA no longer felt that their public reputation would be best managed by remaining on the sidelines of the healthcare debate. The new dominance of market forces over state allocation allowed the insurers the possibility of publicly participating in the debate. They used that opportunity to cultivate an image of an industry working to reform itself. Such an outcome was not considered impossible. On the contrary, the dominant neoliberal ideology supported the claim that private businesses that did not adjust to meet public needs would go out of business.
While the insurers ran a public campaign cultivating an image of supporting aspects of reform, the insurers simultaneously publicly prompted doubt in the government’s capability to enact reform through bankrolling the “Harry and Louise” television advertisement campaigns. These ads feature a middle-class couple expressing support for President Clinton’s reforms, alongside reservations framed in terms of lack of choice or fear of government. An investigation by the Center for Public Integrity credited them as “almost single handedly responsible” for a twenty-point drop in public opinion regarding the Clinton healthcare reform plans (The Center for Public Integrity 1995a: 413). However, part of the advertisement’s effectiveness is attributed to the Clinton administration’s public condemnations of the ads (Clymer et al. 1994). In a speech to a group of pediatricians, Hillary Clinton said:
They [private insurers] like being able to exclude people from coverage because the more they can exclude, the more money they can make. Now they have the gall to run TV ads that there is a better way, the very industry that has brought us to the brink of bankruptcy because of the way they have financed health care. (Clymer 1993)
The comments were printed on the first pages of the Washington Post and the New York Times the following day, igniting national news coverage of the advertisements (Clymer 1993; Priest 1993). The comments added additional publicity to the advertisements but did not effectively critique the implications of the messages. The contradictory strategy of the Clinton administration to simultaneously recommend a health insurance reform based on expanding private health insurance while also publicly condemning the industry was unsuccessful. The inconsistency highlights the conflicting institutions of the neoliberal era. After adhering to the economic logic that private markets are the socially optimal means of allocation, the Clinton administration’s attempts to establish the reforms as the means to perfect market allocation were ineffective.
5.3.2. Business groups
As the neoliberal SSA emerged from the crisis of regulated capitalism, big business owners had gained a tremendous amount of lobbying power and became actively involved in shaping the state (Volscho 2017). In the new climate, legislation was thought unlikely to pass without capitalist support. The Clinton administration accordingly was persistent in their efforts to work with big business groups. In a speech to the Business Roundtable (BRT), a lobbying organization whose members are chief executive officers of major companies, Hillary Clinton discussed the reform proposal as fundamentally shaped by the needs of big business (Clinton 1993). Evaluations by consultants supported Clinton’s claims and predicted that the reforms—even the mandatory payment of 80 percent of their employee’s premium payments—would save them millions in healthcare costs annually (Mandelker and Findlay 1994). Despite the advantages to reform in the healthcare industry and the persistent efforts of the Clinton administration to work with big business groups like the BRT, ultimately the influential group of business executives distanced themselves from the Clinton reform. The group publicly endorsed a competing and more limited healthcare reform bill but took no visible actions to ensure the passage of the piece of legislation (Ifill 1994). This bill, sponsored by Representative Jim Cooper, was referred to as “Clinton-lite” and would not mandate any employer payment toward employee’s health insurance premiums.
The large business organization’s lack of public support for healthcare reform that they predicted would save them millions of dollars in healthcare costs is counterintuitive. However, there are several potential explanations which suggest that this behavior was in line with the joint set of institutions and ideas that promoted successful capitalist accumulation in this period. One possibility is that the big business groups were motivated and positioned to drag their feet on healthcare reforms because of the renewed profit rate and the growing political strength of the neoliberal SSA (Kotz 2015: 99). Leaders of organizations representing business owners often cited rapidly rising healthcare costs as a significant problem in business (Long-Term Strategies for Health Care 1991). However, the refusal to actively support healthcare reforms in the 1990s can be interpreted as an indication that even healthcare reforms that were designed to their interests were deemed unnecessary for continued profitability. Relatedly, business leaders seemed to not fear negative repercussions from maintaining the status quo. The administration warned big business about potential negative consequences of the failure of market-based healthcare reform. Later in her remarks to the BRT, Hillary Clinton revealed that she expected “the political pressure will build for the single-payer government solution, because people will be fed up and frustrated” (Clinton 1993). However, this was not a plausible threat in that period. Big business had no obvious competition from groups with opposing goals, and there was no indication that other groups, such as labor or consumers, were likely to gain enough strength to influence reforms that could pass without big business input. Finally, big business groups had allied with small business groups in their efforts to establish the institutions and ideas of neoliberal capitalism (Kotz 2015: ch. 2). Small businesses were also predicted to benefit from the HSA’s 3.5 percent payroll cap for health premium costs (Wartzman and Saddler 1994). However, the organizations that represented small business owners, like the Chamber of Commerce, the National Restaurant Association, and the National Federation for Independent Businesses announced opposition to the Clinton plan (Clymer et al. 1994; Mathis 1994). Ultimately, big business groups acted as though they expected the benefit of maintaining fidelity to their allies in the neoliberal era would be greater than the benefits of passing healthcare reforms.
It should be noted that healthcare costs are far from the only determinant of a firm’s profitability. Thus, the lack of these organizations’ public support for these reforms may be in reaction to other dynamics of national politics or efforts to support or undercut the main political parties. For instance, given the lack of broad popular support for the Clinton administration, it is possible that the leaders of the BRT were trying to curry favor with a stronger Republican party in the future. Perhaps, the BRT suspected that the Republican party would reward their businesses with favorable conditions if they did not actively support the Democratic party. This would be a reasonable expectation, since there were reports of Republican politicians admonishing business groups or companies that publicly supported aspects of reform (Mathis 1994; Priest 1994; Weisskopf 1994). These admonishments would be particularly threatening for small business owners, who may reasonably assume that they will have little control relative to big business groups over the way a strengthened state will intervene. Another possibility is that these groups were lobbying for or against healthcare in other underreported ways, potentially facilitated by the concurrent relaxation of campaign finance rules. Nevertheless, it is notable that business groups did not fear negative ramifications of the failure of healthcare reform to pass, nor of their lack of action to support reform.
5.3.3. Labor and citizen groups
Many labor groups supported a single-payer healthcare reform or an expansion of the public Medicare programs. 9 These proposals also had significant popular support. Results of Gallup opinion surveys published in the New England Journal of Medicine found that 72 percent of Americans surveyed favored a tax financed national health insurance system in 1990 (Blendon and Donelan 1990). Each of these policy proposals, which were more compatible with the institutions and ideas of the prior regulated capitalist SSA, were summarily dismissed by policymakers. In a May 1993 memo, Mike Lux, a Special Assistant to the President, states: “the single-payer no deductible/co-pay position in my view is absurd” (Lux 1993: 3). Other reports from those close to the Clinton administration revealed single-payer–style health insurance reform was never seen as a realistic option (The Center for Public Integrity 1995a: 423).
Perhaps the most public exhibit of the dismissal of single-payer advocates occurred in an October 1993 Ways and Means Committee hearing. Following testimony supporting a single-payer system from the policy manager from Consumers Union, the nonprofit organization that publishes Consumer Reports, Representative Bill Thomas replied:
But if you want to hang on the [single-payer] position. . . you are not going to be a player in this initial round of trying to determine how we change the health care system. And if that is going to be your position, fine. Then I understand how I need to deal with you. That is, you’re not going to be a player. (President’s Health Care Reform Proposals: Impact on Providers and Consumers 1993: 279)
The dismissal of the single-payer option, despite the significant public and labor support, speaks to the strength and cohesion of the institutions and ideas of the neoliberal SSA. The minimal attention given by the administration to a single-payer system did not launch labor and citizen groups into a united campaign against the Clinton HSA.
10
However, even these organizations’ arguments in support of the HSA were ineffective in the neoliberal SSA. As noted by Gottschalk (2000), labor’s simultaneous campaign against the North American Free Trade Agreement (NAFTA) disrupted their support of healthcare reform. Some legislators implied that their opposition to NAFTA undercut their arguments in favor of healthcare. For instance, Representative Thomas asked John J. Sweeney, a representative from the American Federation of Labor and Congress of Industrial Organizations (AFL-CIO):
Would you please explain to me why your organization supports a plan which will raise the costs to 80 percent of employers in the United States and arguing that, in fact, it will produce jobs when you are opposing the North American Free Trade Agreement, when the economy of Mexico is 4.5 percent of the United States—smaller than the State of Illinois—but argue that NAFTA is going to lose hundreds of thousands of jobs over the same period? (President’s Health Care Reform Proposals: Impact on Labor 1993: 27)
The strength of the institutions and the dominant ideas of the neoliberal SSA rendered the preferred healthcare reform approach of organized labor and citizen groups to be considered unviable in this period, despite the significant public support for such a system. In this context, healthcare reform was limited to approaches that relied on private market institutions and business support. Organized labor, already embattled in trade policy negotiations, offered qualified support of the Clinton HSA. The organizations also consistently opposed many legislative alternatives to the HSA, like the Cooper legislation supported by business groups (Johnson and Broder 1997: 331). Yet their positions did little to sway big business executives, who had abandoned the prior capital-labor accord.
5.4. Discussion
Histories of the demise of the Clinton health plan demonstrate many causes of the HSA’s failure, such as the ineffectiveness of the administration’s communication strategies and outreach, the effectiveness of media created by their opponents, and the political struggles of the administration (Morone 1995; Navarro 2008; Skocpol 1997; Starr 2011; The Center for Public Integrity 1995a; 1995b; 1996). The above discussion deepens our understanding of the reasons for the failure of this major attempt at healthcare reform. Belief in unregulated markets and a distrust of the government has not been a consistent feature of American culture that can be held responsible for cases of health reform’s failure. However, these ideas were compatible with the dominant ideology of the neoliberal SSA. As such, the Clinton administration crafted and marketed their healthcare reforms to highlight the virtues of markets and individual responsibility. They expected that appealing to business’s bottom lines would gain support from the business owners. However, big business lobbying groups could not be persuaded to support significant healthcare reform. The health insurance industry’s lobby launched a public campaign against healthcare reform. Labor and citizen groups, which played an important role in the success of Medicare and Medicaid, were limited in the reforms they could support and had their positions undermined by their weakening economic power.
6. Case Study 2: The Passage of the Affordable Care Act
The discussion below analyzes the ways in which the policy elements of the ACA and the rhetoric used to support it reflect the changed context of the crisis of neoliberal capitalism. In this case study, we see that there are characteristics of the ACA, as well as changes in the strategies and arguments of important stakeholder groups, that defy the boundaries of the consolidated neoliberal SSA. As noted earlier, the crisis phase of an SSA is characterized by ineffective capital accumulation that cannot be remedied by the normal tools of fiscal and monetary policy. SSA theory highlights the lack of natural mechanisms to adjust the economy back to one that promotes accumulation or stability. However, a crisis should not be interpreted to suggest that none of the institutions and dominant ideas of the consolidated SSA remain. The rates at which these institutions and ideas change are variable and subject to the dynamics of the struggle that unfold in the crisis phase.
6.1. Cohesion with neoliberal capitalist SSA
The rhetoric used to discuss the ACA reflects the enduring but weakened ideology of neoliberal capitalism. At a White House forum in early March of 2009, President Obama said:
If there is a way of getting this done where we’re driving down costs and people are getting health insurance at an affordable rate and have a choice of doctor, have flexibility in terms of their plans, and we could do that entirely through the market, I’d be happy to do it that way. If there was a way of doing it that involved more government regulation and involvement, I’m happy to do it that way, as well. (Obama 2009)
Like Obama’s remarks, the ACA is not a total denunciation of the neoliberal SSA. It adheres to many of the principles of neoliberal ideology. Most notably, the ACA is designed to support the private for-profit health insurance industry. The law requires individuals to have health insurance coverage, maintains insurance companies’ abilities to offer limited provider networks, and forgoes tools of price regulation. Although the individual mandate can reasonably be interpreted as the creation of an enforced market that violates the sanctity of an individual’s purchasing decisions, the mandate continues to frame health insurance as a commodity that individuals purchase, not a public guarantee from the government.
6.2. Contradictions with neoliberal capitalism
It is notable that Obama’s remarks at the forum reflects a much greater acceptance of the government’s role than was evident in the Clinton administration. Important features of the ACA can be considered similarly contrary to the norms of neoliberal capitalism. First, instead of emphasizing the success of private competition to create benefits for consumers and society, the ACA includes significant constraints on private insurers, including a mandated minimum percentage of premium revenues that must be spent on medical claims. Second, the ACA also includes a massive expansion in subsidies and premium tax credits that shield individuals from the costs of their health insurance. Third, the law massively expanded the Medicaid program. The Congressional Budget Office predicted that the ACA would lead to roughly 16 million more people enrolled in Medicaid and the Children’s Health Insurance Program, the largest expansion of public insurance for lower-income people since Medicaid’s creation in 1965 (McDonough 2011: 141).
Despite the meaningful shifts, the ACA was notably limited relative to other proposals considered during this time, such as a proposal to expand Medicare for All or to create a publicly run health insurance program often called the public option. The public option had not been a dominating feature of previous debates over healthcare reform. 11 However, it became an important point of debate in the lead up to the passage of the ACA and emerged as a serious possibility for reform. It was ultimately excluded from the final legislation, but some version of the public option was included in bills passed by the House of Representatives, as well as bills passed by three House committees and a Senate committee (Halpin and Harbage 2010). The serious consideration of the public option further exemplifies the ways in which the broader context of economic restructuring and uncertainty of the time helped facilitate discussion over legislation that moved beyond the previous constraints of the neoliberal SSA. Its omission reflects the aspects of neoliberal capitalism that were able to withstand the challenge of the crisis. A government health insurance plan could ostensibly outcompete and eliminate the private health insurance industry.
6.3. Group conflict
Following the challenge to neoliberal capitalism, the organizations representing insurance companies and big business executives responded differently than they had in the 1990s. Why would these organizations oppose the Clinton health reforms, but then support reforms in 2008? Did employers and insurance companies become more generous than their 1990s counterparts? Was the ACA more beneficial to their industry’s bottom line? Or was the Obama administration more effective at negotiating with these groups? The discussion below analyzes how the passage of the ACA was conditioned by the concurrent destabilization of the set of institutions and ideas that had constituted the neoliberal capitalist consolidation.
6.3.1. Health insurers
The main lobbying organization for health insurers in this period, American Health Insurance Plans (AHIP), deployed a different strategy from that of its predecessor organization in the 1990s. Although the lobbying group for insurers voiced nominal support for healthcare reforms in the 1990s, the organization had simultaneously run a public campaign criticizing the reform, which called into question the government’s ability to productively regulate insurance companies. Instead, AHIP acknowledged their previous role in deterring reforms and pledged cooperation. See, for example, the language from the group’s 2008 reform proposal’s introduction:
Although health care reform has been on the nation’s agenda for many years, the varied interests of stakeholders have held back progress.. . . We offer our proposals with a pledge to work in a spirit of cooperation and determination, with physicians, hospitals, consumers, employers, unions, lawmakers, and government leaders who want to work toward the day when all Americans can count on being served by a health care system second to none. Working together—starting in 2009 —can achieve the goal. (America’s Health Insurance Plans 2008)
This sentiment was repeated in March 2009, at President Obama’s first public event regarding healthcare reform, when AHIP president Karen Ignani stated:
We want to work with you. We want to work with the members of Congress on a bipartisan basis here. You have our commitment. We hear the American people about what’s not working. We’ve taken that seriously. You have our commitment to play, to contribute, and to help pass health care reform this year. (Obama 2009)
Over the next few months, the proposals that the organization publicly supported continued to deviate from their positions in the 1990s. For example, in the 1990s, AHIP’s predecessor organization argued that without being able to price individuals according to their risk, that their industry may not be able to pay for their policyholders’ claims (Gradison 1993b). In June of 2009, AHIP announced their support for discontinuing rating based on health status or gender (America’s Health Insurance Plans 2009). By not charging individuals based on their gender or health status, the insurers were supporting a move to a system that socialized the costs of providing care to people likely to need more. Notably AHIP announced their support for not having ratings based on health status or gender in the same press release that they publicly announced their opposition to the public option. Their statement said, “We share the concerns that providers, employers, and patients have raised about the significant unintended consequences of a government-run plan. It would dismantle employer-based coverage, add additional liabilities to the federal budget, and turn back the clock on efforts to improve quality and safety” (America’s Health Insurance Plans 2009).
The language and tone used in this announcement is mild, and the organization notes that they are only echoing others’ concerns. They do not include any concerns that are specific to insurers competing against a government plan. A concern that a public plan would “dismantle employer-based coverage and add additional liabilities to the federal budget” is much more muted than the “they choose, we lose” slogan from decades previous. Their relatively subdued language against the possibility of a government-run health insurance plan is striking and speaks to the changed institutions under which insurers were now fighting. Even though the government-run competitor was potentially a graver threat to the private health insurance industry than many elements of the Clinton Health Plan, rejecting healthcare reform as they had in the 1990s was not an option for the industry in 2009.
A Bloomberg journalist later reported that AHIP had donated over $86 million to the Chamber of Commerce to finance advertisements and events to publicly oppose the healthcare bill (Armstrong 2010). Based on the secret funding, it is reasonable to assume that the insurers’ comments supporting healthcare reform were disingenuous, and that they maintained the fierce opposition to healthcare reform in 2008–2010 as they did in the early 1990s. However, even though the health insurance companies were secretly funding advertisements to delay or block healthcare reform, it does not indicate that the insurers were merely repeating their previous ploys. In the nineties, the health insurer’s lobbying organizations did not have to secretly fund television advertisements. The Harry and Louise ads were explicitly funded by the Coalition for Health Insurance Choices, a group that HIAA publicly addressed creating. The fact that insurers kept these payments secret supports the notion that the destabilization of the neoliberal SSA had created an environment where insurance industry executives had to act differently than they had previously. One potential explanation is that the rising numbers of unemployed may have made the executives more fearful of public backlash for being perceived as opposed to reform. From December 2007 to June 2009, over seven million workers became unemployed (Bureau of Labor Statistics 2009).
A second reason why AHIP reacted to proposals for healthcare reform differently in this period is that private health insurance companies seemed to need reform and additional government support to continue. This was partly because private health insurers were themselves challenged with the contradictions of neoliberal capitalism within their industry. Labor’s declining power was reflected in the declining rates of employment-based health insurance (Vistnes et al. 2012). Insurers were no longer able to count on selling employer-based health plans as their main source of revenues. This trend was compounded by the fact that large employers continued to be more likely to use self-funded health insurance (Crimmel 2013). Only offering administrative services generated less money for insurance plans and necessitated a shift in business models for insurers away from administering employer-based health plans and toward administering government programs. By November 2007, three major health insurance companies, WellPoint, UnitedHealth Group, and Coventry, each reported that the growth in their government-related earnings outpaced the decline in the commercial sector (Berry 2008a). In 2007, Humana’s CEO identified Medicare as “a growth opportunity for many years to come” (qtd. in Berry 2008b).
Beyond adjusting their business models to administer more government services, insurers also diversified their business by offering money management and banking services as well. Their increased involvement in financial services also reflects their adaptation to neoliberal institutions and norms. As the costs of healthcare were shifted to consumers, the growth of health savings accounts increased. Large health plans, including WellPoint, UnitedHealth Group, and the BlueCross BlueShield association accordingly established FDIC-approved banks to manage these accounts (Berry 2008c).
The development of the health insurance industry in the early 2000s reflects the unique environment of the neoliberal SSA. As the set of institutions and dominant ideas became more entrenched, they also created conditions that forced the industry to adapt. Large insurance companies expected their business to come from handling public revenues and from marketing financial products. Even prior to the recession and the rapid increase in unemployment rates, health plans acknowledged to their investors that they needed to structurally adjust how they made profits. It was in this context in which the lobbying association for the health plans publicly supported regulations of their industry and was very mild in their public opposition to health reform.
6.3.2. Business organizations
The BRT also meaningfully expanded their commitment to healthcare reform following the financial crisis. Instead of remaining on the sidelines of reform, as they had in the 1990s, in August of 2009 the organization said they were in “near constant communications with the White House and Congress. . . as an honest broker to bring about reform” (BRT 2009d). Later in the same conference, John Castellani, the president of the BRT, indicated for the first time that they could support an employer mandate for healthcare reform: “We know the direction they’re going, and we think it could be worked out to be acceptable for us” (BRT 2009d). The group’s language supporting other aspects of healthcare reform became even stronger as the healthcare debate continued. In a letter to President Obama, Castellani emphasized that his organization “strongly” supports guaranteed issue as well as limiting plans’ ability to set ratings, two regulations that the organization had not previously publicly supported (BRT 2009b). The organization followed these statements with a report titled “Health Care Reform: The Perils of Inaction.” The statement predicted dire consequences for employment-based health insurance if no reform was passed and urged legislators to “support aggressive insurance market reforms” to solve the rapidly increasing costs of health insurance (BRT 2009c).
Employers did not universally support all aspects of healthcare reform in this period, however. After the full House of Representatives passed a healthcare bill that included the public option, the BRT released a relatively mild public statement expressing disapproval for the public option (BRT 2009a). The public option, if adopted, could be a massive expansion in state power, potentially at the expense of the private health industry’s market share. However, the organization was much more vocal about their support of reform and restrained in its public opposition to the reform. This change in actions suggests that the emerging possibility of the public option, a feasible and threatening expansion of government power, may have led to the organization’s greater acceptance of healthcare reform in this period. This direction did not seem plausible in the 1990s but was plausible in the context of the destabilization of the neoliberal capitalist SSA.
The BRT dropped their opposition to the Senate bill after it became clear that the public option would not pass in the Senate. Thus, the BRT and insurers focused on stopping the public option, not on rejecting all reforms. Their ultimate support of healthcare reforms following the removal of the public option in the Senate was influential in the final passage of the bill. Passing a major reform was necessary to stave off this bigger threat of an eventual government takeover of health insurance, a precedent that they had good reason to fear in 2010.
The US Chamber of Commerce and the National Federation of Independent Businesses, two organizations that identify themselves as representing small businesses, also testified and ran ads regarding health reform in these periods. As in prior discussions of healthcare reform in the 1990s, both organizations remained steadfast in their opposition to reform in 2010. Their arguments echoed that of their previous campaigns. The National Federation of Independent Businesses threatened that an employer mandate would lead to economic recession, discourage production, and eliminate jobs for the most vulnerable employees (Roundtable Discussion 2009: 241–47). The Chamber of Commerce described an employer mandate as a “job killer” and the public option as a “backdoor way to bring single-payer, socialized medicine” (Roundtable Discussion 2009: 337–40). Both arguments were successful in stopping the Clinton administration’s healthcare legislation. However, the existing challenges to the neoliberal SSA in this period created conditions where big business groups and health insurance companies were willing to accept healthcare reform. Without the additional support of big business groups, their opposition to major healthcare reforms was unheeded.
6.3.3. Labor and citizen groups
Like the organizations representing small business groups, labor and citizen groups also maintained their stance on healthcare reform across each period of the SSA. Unions and public-interest groups were vocal proponents for many aspects of healthcare reform, including regulations on insurers, the establishment of the exchange, the expansion of Medicaid, subsidies for lower- and middle-income families, and a mandatory employer contribution. These groups were also among the most active supporters of the public option. In previous debates, which did not feature discussions of a public option, the labor unions and citizen groups demanded the establishment of a single-payer healthcare system. Some groups, for example, Disabled for Action, California Nurses Union, and Physicians for a National Health Plan, maintained a strict devotion to the establishment of a single-payer healthcare plan. Some labor organizations, such as the AFL-CIO, continued to voice support for a single-payer system but viewed the public option as consistent with their long-term support of universal coverage based on a social insurance model (Health Care Reform Roundtable 2009). Health Care for Action Now (HCAN), a coalition of the American Federation of State, County, and Municipal Employees, the Service Employees International Union, the United Food and Commercial Workers, and the Association of Community Organizations for Reform Now explicitly supported and organized in favor of the public option.
In the period after the financial crisis and Great Recession, the arguments used to support the establishment of a public option gained credibility. The language of competitive and deregulated markets were no longer effective slogans to rally opposition for healthcare reform. The deregulation of the financial industry was considered a precipitating factor in the financial crisis and Great Recession. Supporters compared opposition toward health insurance reform to support for the earlier financial services deregulation that had helped devastate the economy.
Public option supporters also benefited from a resentment toward the tremendous profits of health insurance companies. Health insurance executives were compared to the bankers receiving bonuses after their bailouts. HCAN staged a mass citizens’ arrest of insurance company executives at a conference in March of 2010. The conference hotel was covered with banners reading “Corporate Crime Scene.” Attendees were deputized to arrest the insurance executive CEOs, who were provocatively described as “a mortal threat to our democracy and the health and wellbeing of our people” because of their “greed, corporate abuses, and craven lobbying” (Kirsch 2012: 335).
Opponents of health reform repeatedly named the public option as a Trojan horse policy, which would ultimately lead to the creation of a single-payer or nationalized healthcare system. However, the establishment of a government-run health insurer was no longer exclusively considered as a radical option guaranteeing government take over. Some supporters of the public option saw the policy as an opportunity to give people choice and a chance to vote on whether the private health insurance system could be sustainable. Leadership from the AFL-CIO argued that it was no longer credible to believe that the current private health insurance system would be able to contain costs and promote universal coverage:
We think that, as soon as feasible, an immediate implementation of a public health insurance plan option is essential. The private insurers have had plenty of opportunity to [put competition into the insurance market] on their own and they have failed to do it.. . . We need to keep them honest. (Health Care Reform Roundtable 2009: 50)
The discussion of healthcare reform in this period following the financial crisis included another feature new to the debate: a stronger focus on the macroeconomy. It became common to associate healthcare reform with the reinvigoration of the economy. Proponents of healthcare reform compared their proposals to Keynesian policies to increase aggregate demand. Senator Jay Rockefeller made the most explicit comparison between the financial crisis and US healthcare:
The current economic crisis. . . is also a crisis of healthcare. They are one and the same. Stabilizing our health care system is a critical component of putting our economy back on track. Leading economists have all agreed that our costly and inefficient healthcare system is perhaps the biggest threat to the Nation’s budget. So, health care is not just health care,. . . it is also, as I say, stability for our country. (Health Care Reform: An Economic Perspective 2008: 5)
By November 2008, connecting what was described as the worst depression since the Great Depression to the problems in US healthcare is a remarkable comparison. Lehman Brother’s collapse in September and the fragility of the financial system has no obvious tangible connection to the problems of US healthcare. Politicians usually discussed the problems of healthcare in the United States in terms of the increasing numbers of uninsured individuals and the rising costs of healthcare. These trends had been in place prior to the problems in the financial industry. However, health insurance and financial markets are connected in their reliance on the institutions and ideas of neoliberal capitalism, which were currently under significant challenge. The unique economic moment strengthened the arguments of proponents of healthcare reform.
6.4. Discussion
In this case study, I analyze how the institutions and ideas of the neoliberal SSA, destabilized following the financial crisis of 2008, shaped the creation and passage of the ACA. In the context of these changing and unstable dynamics, industry stakeholders were threatened with the prospect of significant industry restructuring. The possibility of a government-run health insurance plan seemed plausible in this period. Arguments and interest groups that were ineffective in the 1990s gained power and credibility. Stakeholders, who successfully and steadfastly had previously opposed healthcare reform despite its being beneficial to their interests in some respects, softened their approach and conceded to major demands.
7. Conclusions
This article analyzes the failure and success of healthcare reforms in the context of two distinct phases of the neoliberal SSA. I argue that an analysis of the different outcomes for healthcare reform in each period must account for the changes in the institutional structure that conditioned the economy’s expansion and destabilization. SSA theory provides a means for a systematic analysis of the deep interrelationships between healthcare and the economy. It can contribute to a better understanding of the limits and the opportunities brought by each set of institutions and ideas and their destabilization.
It is also worth noting the limits of the theoretical frame of SSA theory. SSA theory does not offer a precise schema for dating the phases of the SSA, and it does not offer predictions for the future. As noted in the previous case studies, although the mutually enforcing institutions of an SSA are cohesive, they are not totally comprehensive. Some developments within an SSA may not strictly adhere to the dominant institutions and ideas associated with the SSA. SSA theory should not be interpreted as offering a deterministic account of the dynamics of capitalism. Its analytical benefit is in highlighting the cohesiveness of a rich set of institutions and ideas that is required for effective capitalist accumulation. Future research in SSA theory and analyses of the economic developments since 2008 can yield additional insights into how the ACA has been enforced and undermined after over a decade of policy proposals from Republicans and their efforts to “repeal and replace” the law.
Footnotes
Acknowledgements
I thank the reviewers and editor for their helpful comments in revising this paper.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article draws from my dissertation research, which was financially supported by the 2018 Union for Radical Political Economics dissertation fellowship.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
1
When I refer to the ACA, I am specifically referencing the nine titles of the Patient Protection and Affordable Care Act (H.R. 3590) as amended by the one title of the Reconciliation Bill (H.R. 4872).
2
When I refer to the HSA, I am specifically referencing H.R. 3600/S. 1757.
4
Kotz (2015: 88) provides evidence of wage stagnation. ![]() provides evidence of declining employer-sponsored health insurance.
provides evidence of declining employer-sponsored health insurance.
5
This is not to suggest that SSA theory provides the only lens for analyzing the dynamics of health capitalism. Nor is it to suggest that the changes in the economy in this period can only be understood as dynamics of a neoliberal restructuring. Studies of the specific impacts of financialization, globalization, and consolidation provide insights into the healthcare sector’s interconnections with capitalist economic relations. This article uses SSA theory and the concept of neoliberal capitalism, as it developed in the United States, to analyze two specific healthcare reforms.
6
7
8
9
Some groups, such as the Oil, Chemical, and Atomic Workers union, maintained strict support for single-payer reforms and could not support the HSA. Other organizations, like the American Federation of Labor and Congress of Industrial Organizations, the Service Employees International Union, Families USA, and Citizen Action, offered support of the Clinton health plan. Their members’ testimonies in support of the Clinton HSA often mentioned a preference for a single-payer style system. For a few examples, see the testimony of Ms. Shearer, Mr. Kirsch, Mr. Dornon, and Ms. Porter in ![]() .
.
10
For more detailed accounts of the debates between labor groups that supported single-payer–style health insurance reform and those that supported the HSA, see Gottschalk (2000), Lenz (2010), and ![]() .
.