
Abstract
Therapeutic factors in group therapy are a series of action mechanisms that contribute to change in therapeutic processes. They are inherent to group dynamics and interaction, yet are not necessarily associated with a therapist’s intervention. These factors are elemental components of a therapeutic change phenomenon derived from the group matrix.
We present five studies that thoroughly evaluate these therapy factors within groups of patients diagnosed with psychosis. All factors are measured with the Yalom Q-sort questionnaire that defines factors based on their value given by the patients. We evaluate and report these value differences between group context, patient diagnosis, and therapeutic orientation.
Therapeutic factors act independently of diagnoses, theoretical framework, and classification; they are intrinsic components of unique group dynamics. In general, the factor claimed to be most important in patients with severe mental disorders was the instillation of hope.
Introduction
Group psychotherapy has been demonstrated useful in the treatment of psychotic patients (Kanas, 1996) because it mainly instigates a series of unique elements favouring the better evolution and knowledge of patients. The most prominent elements are mirroring, context, and group therapy factors (González de Chávez, 2009). Within these group therapy factors, there exists a series of therapeutic action mechanisms that serve as change procedures that contribute to the therapeutic process and are inherent to group interactions or dynamics. They are not directly linked to the therapist’s action, but are elemental components of the therapeutic change phenomenon derived from the group matrix (Yalom, 1985). Bloch and Crouch define a therapeutic factor as ‘an element of group therapy that contributes to improvement in the patient’s condition and that is a function of the actions of the group therapist, the other group members, and the patient himself’ (Bloch and Crouch, 1985), which differentiates these factors from conditions or techniques that bring forth any change.
Therapeutic factors were first studied in the mid-1950s after Corsini and Rosenberg (1955) reviewed more than 300 articles on group psychotherapy in an attempt to classify the mechanisms identified by each author as essential elements for therapeutic success. More than two decades passed, however, before relevant research development began. Collected cornerstone publications were those of Bloch and Crough (1985), Yalom (1985), and MacKenzie (1990). Notably, Yalom designed a valid, reliable questionnaire based on his interpersonal group psychology, which established his studies as reproducible. This questionnaire is the instrument most researchers use in their relevant study of therapeutic factors and is a cornerstone in group therapy research.
The last decade has seen renewed interest in the study of therapeutic factors, which has given rise to new questionnaires and classifications. The utility of these has yet to be determined. Examples include the Therapeutic Factors Inventory (TFI) of Lese and MacNair-Semands (2000) and the recent classification of Dierick and Lietaer (2008). However, few studies exist regarding group therapy factors in psychotic patients. Moreover, older studies failed to survey homogeneous diagnostic groups, but included patients with affective and personality disorders, usually in a hospital setting (Maxmen and Hanover 1973; Schaffer and Dreyer 1982; Leszcz et al., 1985; Kahn et al., 1986). Highlighted among the studies performed in an outpatient setting were those by Butler and Fuhriman (1980), which included psychosis among other serious mental disorders. To our knowledge, the studies conducted in our centre are the only surveys that express complete diagnostic homogeneity (González de Chávez et al., 2000; García Cabeza and González de Chávez, 2009).
Over the past 25 years, we have been conducting a group therapy programme for psychotic patients. Currently, we have outpatient groups for patients with psychosis in both the schizophrenic and bipolar spectrum as well as group therapy in the Acute Unit for psychotic and affective patients. Herein, we have aimed to summarize the findings of five of our studies, two of which have been published, and three composed of unpublished results. All studies are conducted within our research interest umbrella and include:
Comparison of the therapeutic factors between psychotic and affective inpatient groups.
Comparison of therapeutic factors between schizophrenic and bipolar outpatient groups.
Comparison of therapeutic factors within schizophrenic inpatient and outpatient groups (González de Chávez et al., 2000).
Comparison of the therapeutic factors in schizophrenic outpatient groups with the consideration of insight level (García Cabeza and González de Chávez, 2009).
Evaluation of differences in therapeutic factors between therapists and schizophrenic patients in outpatient therapy.
The purpose of this work is thus to determine the therapeutic factors that patients value most, and to determine if these factors change according to the group context, group type, and therapist orientation.
Material and Methods
Intervention Model
1. Inpatient groups
Patients with Psychosis
This was an open group with a high rate of turnover, as patient number notably varied over time, and attendance was mandatory. Three 45-minute sessions per week were held and the duration of a patient’s stay was determined by his/her time in the acute unit. The therapist played an active role that included verbalization, working with the ‘here and now’, and examining a patient’s psychotic experiences to desingularize the psychosis and exit perceptive egocentrism.
Affective Patients
This was an open group comprised of bipolar and unipolar affective disorder patients who attended voluntarily. At any time, the mean number of patients ranged from four to eight, with a high rate of turnover, during two weekly one-hour sessions. The group was fundamentally oriented toward cognitive psychotherapy and included elements from interpersonal psychotherapy. Its main objectives were for patients to gain a better knowledge about their diseases and the particular influence of biographic aspects and relationships (family, social, work, etc) on the illness.
2. Outpatient Groups
Patients Diagnosed with Schizophrenic Psychosis
These were open groups with 90–120 minute long sessions held weekly. The patients in this group were oriented with a program consisting of combined treatments, including pharmacological therapy and individual/family intervention as necessary. Although these groups were oriented towards insight, attempts of adaptation for the patients’ individual needs were critical. Therefore, support and interpersonal or coping strategies based on the clinical condition were included. Depending on the specific style of each therapist, the final purpose was to develop a comprehensive treatment of symptoms, providing patients with an understanding of their biographical history, while stressing precipitating factors and vulnerability and studying interpersonal relationships, cognitive copings, and defence mechanisms.
Patients Diagnosed with Bipolar Disorder
These were open groups with weekly sessions lasting approximately one hour, in which interpersonal orientation was focused on the ‘here and now’. The purpose of the group was not one of personality reconstruction, but rather one focused on reaffirmation, clarification of emotional conditions, improvement of interpersonal communications, and manifestation of perceptions. Group attendance formed a combined program including drug, individual, and psychoeducational intervention.
Evaluation of Therapeutic Factors
Therapeutic factors were studied with the 12–therapeutic factor standard version of the Yalom questionnaire (Yalom, 1985). For this study, patients were administered 60 cards that each contained a sentence related to one factor. For example, an instillation of hope factor could read: ‘seeing others getting better was inspiring to me’, or ‘knowing that the group had helped others with problems like mine encouraged me’. Self-understanding factors were manifested in such statements: ‘learning that how I feel and behave today is related to my childhood and development (these are reasons in my early life that explain why I am as I am)’, and ‘learning that I react to some people or situations unrealistically (with feelings that somehow belong to earlier periods in my life)’.
Patients were instructed to order the cards into seven categories according to personal usefulness: most useful (two cards), extremely useful (6), very useful (12), useful (20), not very useful (12), of little use (6), and least useful (2). After instillation of hope, self-knowledge, universality, interpersonal learning input (feedback that the patient receives from the group) and output (new attitudes or behaviours that the patient learns, does and tests in the group microcosm), identification, catharsis, guidance, cohesiveness, altruism, origin family reenactment, and existential factor were interpreted, the factors were attributed to the twelve previously established categories of therapeutic factors.
Study C was conducted in a similar fashion. The questionnaire was administered to the therapists leading the groups of patients in an attempt to ascertain which therapeutic factors were considered most useful in the process. All instruments were implemented by professionals who were trained in their use. These technicians did not participate in any patient therapy.
Statistical Analysis
The data analysis in all studies presented was conducted using statistical procedures, including the performance of basic statistical formulas, frequency analysis, means analysis, deviations, and ranges. In order to account for the small size of some patient samples to provide a homogeneous presentation in this work, the following non-parametric tests were used for mean comparison: the Mann-Whitney U test for two independent samples, and the Kruskal-Wallis test for several independent samples. Correlations were made with Pearson’s correlation coefficient for quantitative variables and the Spearman rank correlation coefficient. The SIGMA statistical programme was used for the statistical analysis of studies a), c), and e) and the SPSS program (version 15.0) was used for studies b) and d).
Design and Sample
a) Inpatient Groups: Psychosis versus Affective
The sample included 33 patients diagnosed with psychosis and 29 patients diagnosed with affective disorder. The patients with psychosis attended a mean of 12 (5–24) group sessions and the affective disorder patients attended a mean of 13 (4–68) group sessions.
We compared the evaluation of therapeutic factors scored by the patients admitted to the Acute Unit included in the psychotic groups and those who attended the affective patient groups based on diagnoses. A summarized list of sample characteristics is listed in Table 1.
Inpatient groups: psychosis vs. affective
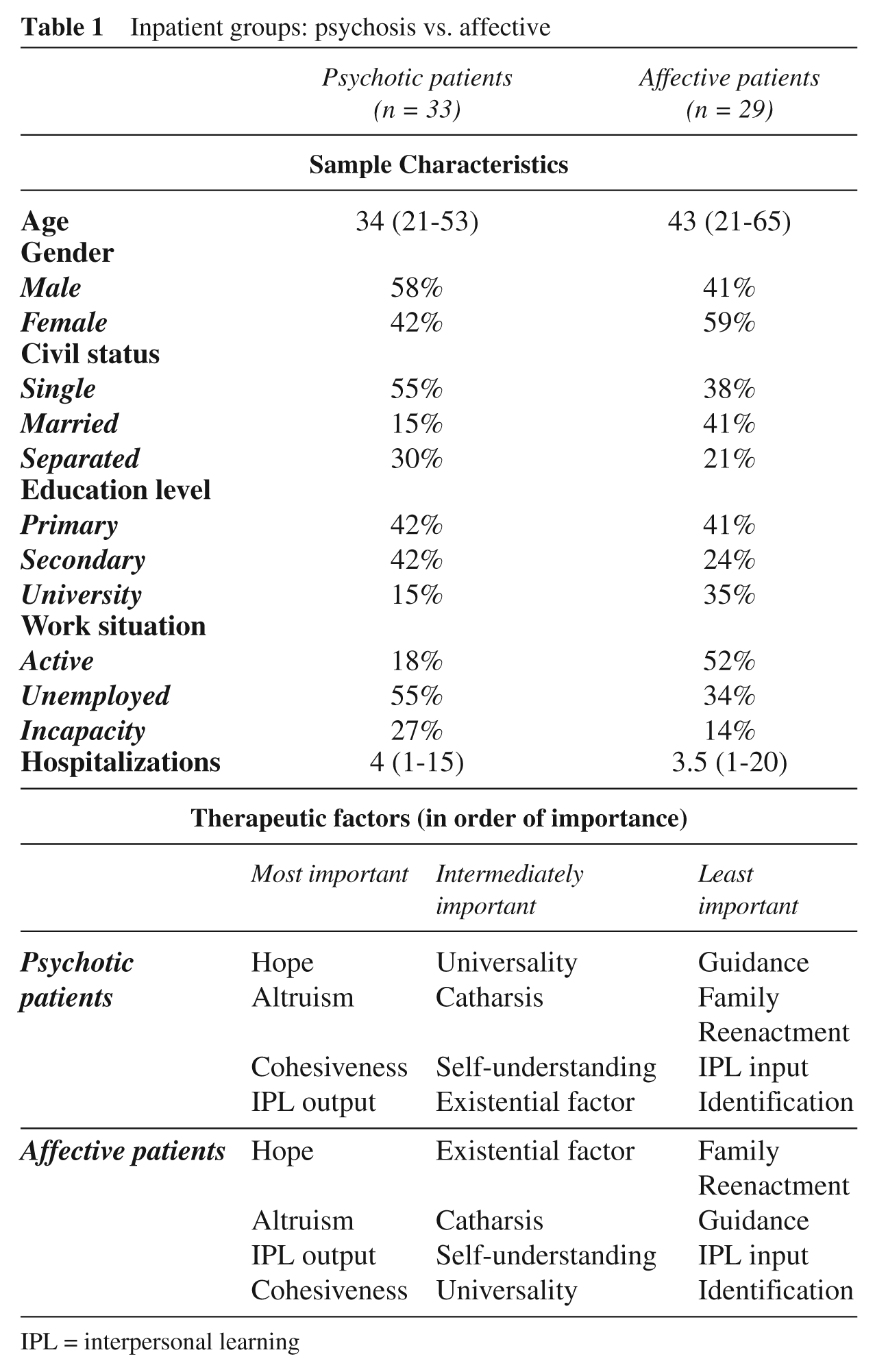
IPL = interpersonal learning
b) Outpatient Groups: Schizophrenic Psychosis versus Bipolar Disorder
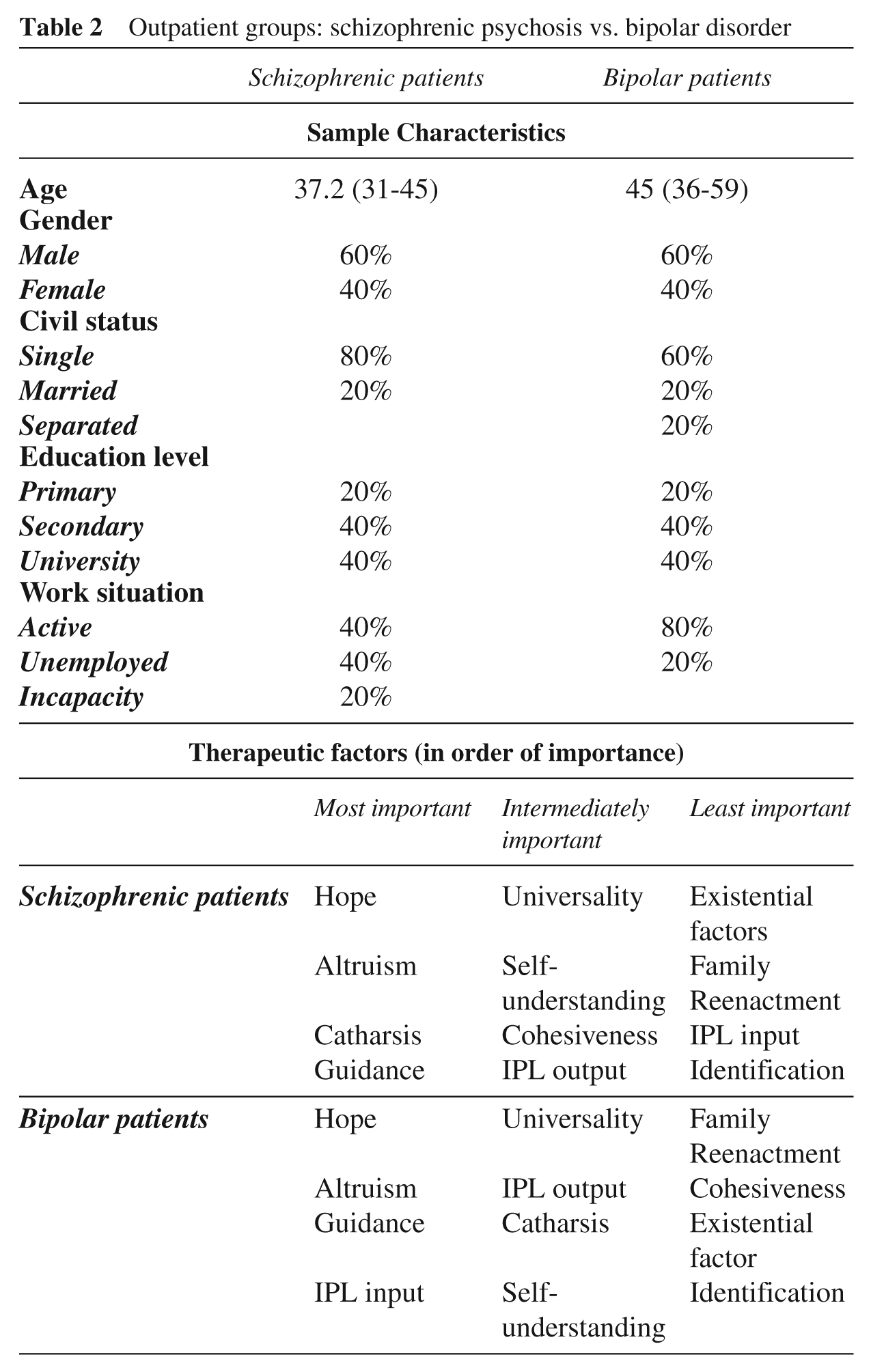
Five patients in the outpatient group of bipolar disorder were compared to five others who were in the schizophrenic patient group based on insight level, as measured by the Camarillo scale (May and Dixon, 1969) described below. The duration of stay for schizophrenic patients was 18.2 months (6–24) and 64.5 (18–108) months for bipolar patients. Sample characteristics are highlighted in Table 2.
Outpatient groups: schizophrenic psychosis vs. bipolar disorder
c) Schizophrenic Patients: Inpatient versus Outpatient Groups (González de Chávez et al., 2000)
We compared factors that were most positively evaluated by schizophrenic patients in both inpatient and outpatient groups. Inpatients participated in 14 (5–24) group sessions and outpatients in 109 (30–264). Sample characteristics are shown in Table 3.
Schizophrenic patients: inpatient vs. outpatient groups
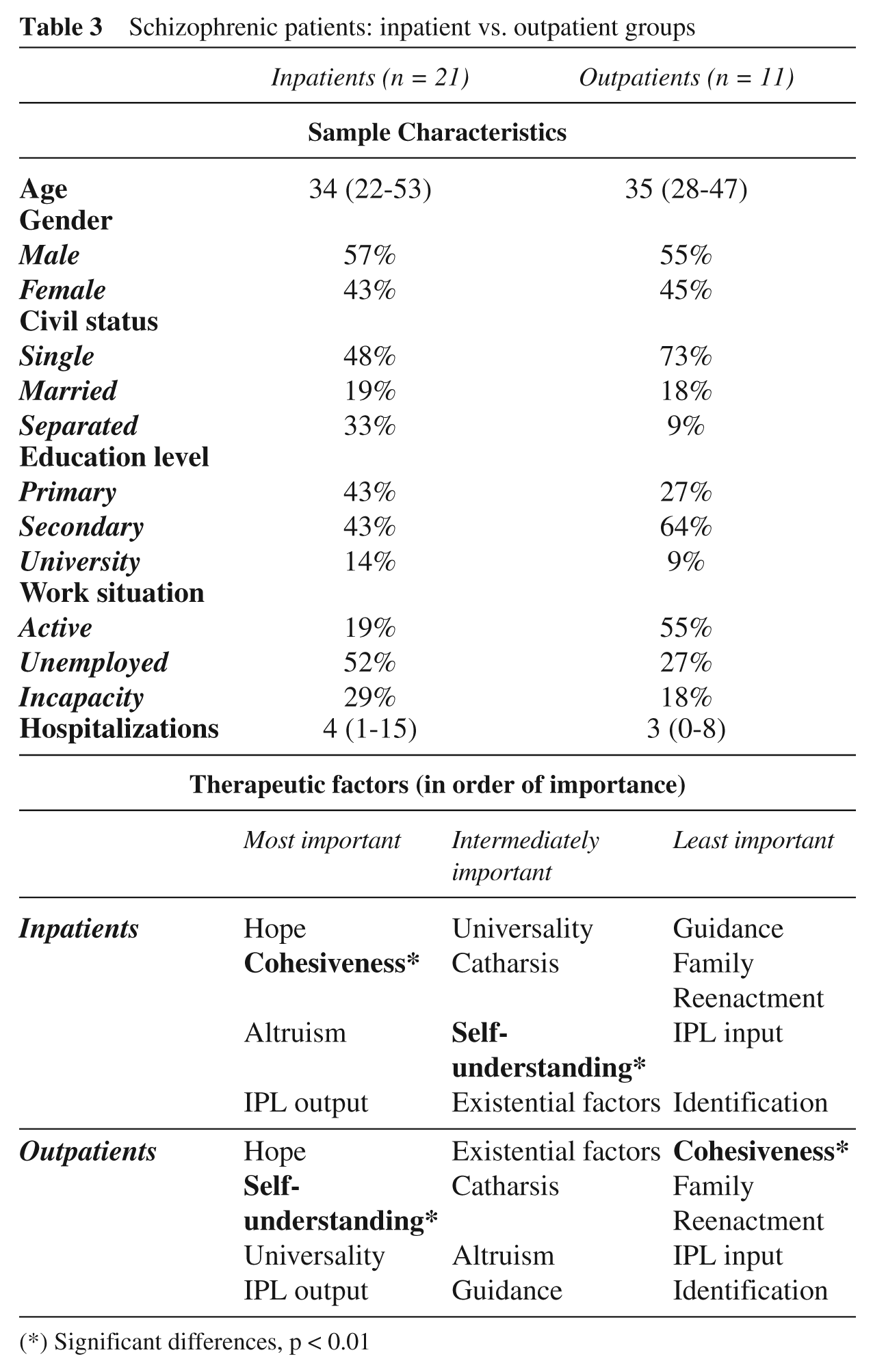
(*) Significant differences, p < 0.01
d) Schizophrenic Outpatient Group According to Grades of Insight (García Cabeza and González de Chávez, 2009)
A total of 17 schizophrenic patients who attended outpatient group therapy for at least six months (mean number of months in therapy was 24.6; mean of 130.15 sessions) were evaluated. In addition to surveying therapeutic factors, insight level was determined by the qualitative scale of Camarillo (May and Dixon, 1969), which made it possible to classify the patients into nine grades of insight, from one (where the patient denies having any disorder) to nine (with psychological insight). This test only determined five insight levels, since the intermediate scores indicated transitions. For statistical analysis, we considered only these five groups and added the intermediate values to the immediately superior score. The sample characteristics are shown in Table 4.
Schizophrenic outpatients group according to grades of insight
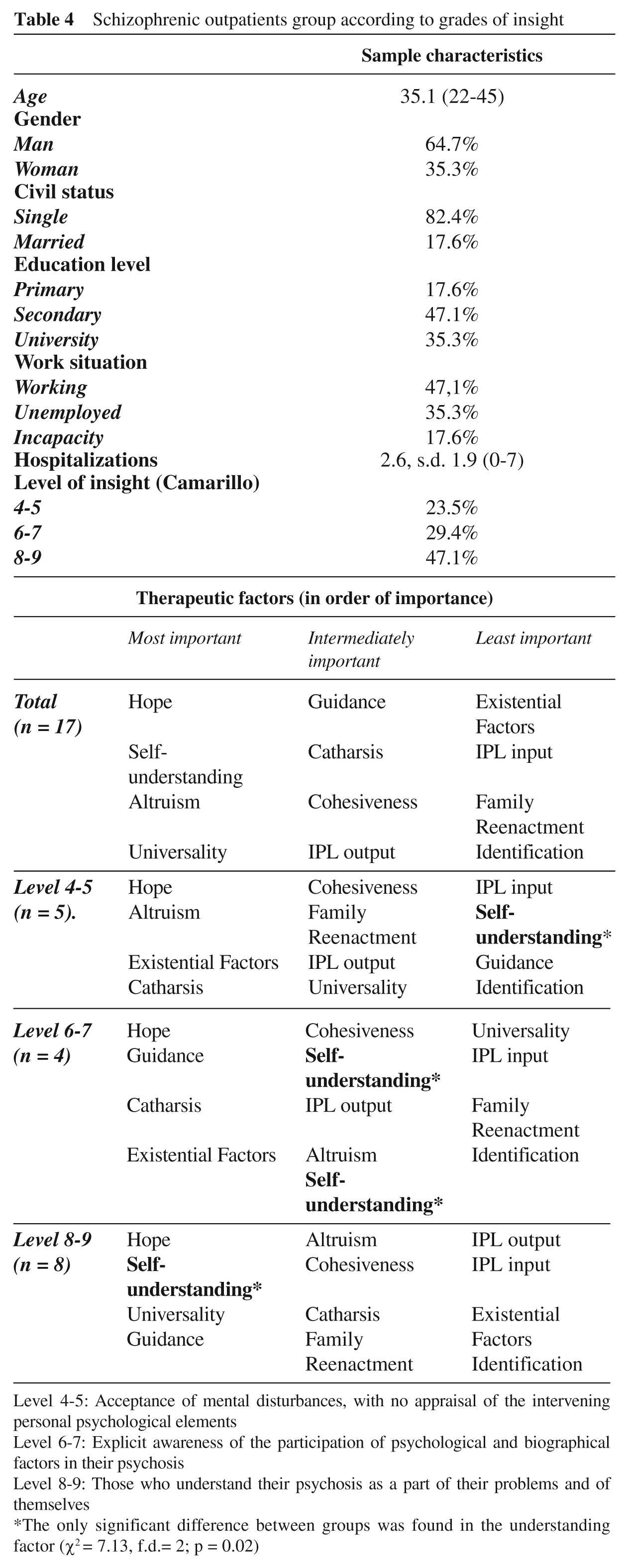
Level 4-5: Acceptance of mental disturbances, with no appraisal of the intervening personal psychological elements
Level 6-7: Explicit awareness of the participation of psychological and biographical factors in their psychosis
Level 8-9: Those who understand their psychosis as a part of their problems and of themselves
The only significant difference between groups was found in the understanding factor (χ2 = 7.13, f.d.= 2; p = 0.02)
e) Schizophrenic Outpatient Group: Patients versus Therapists
We studied 21 outpatients belonging to two groups. Patients stayed in treatment for 21 months (6–43) and all were diagnosed with schizophrenic psychosis, with the exception of one patient (schizoaffective disorder). These results were compared to those obtained by five therapists who completed the same questionnaire and who had extensive experience in our group therapy model. Sample characteristics are listed in Table 5.
Schizophrenic outpatients group: patients vs. therapists
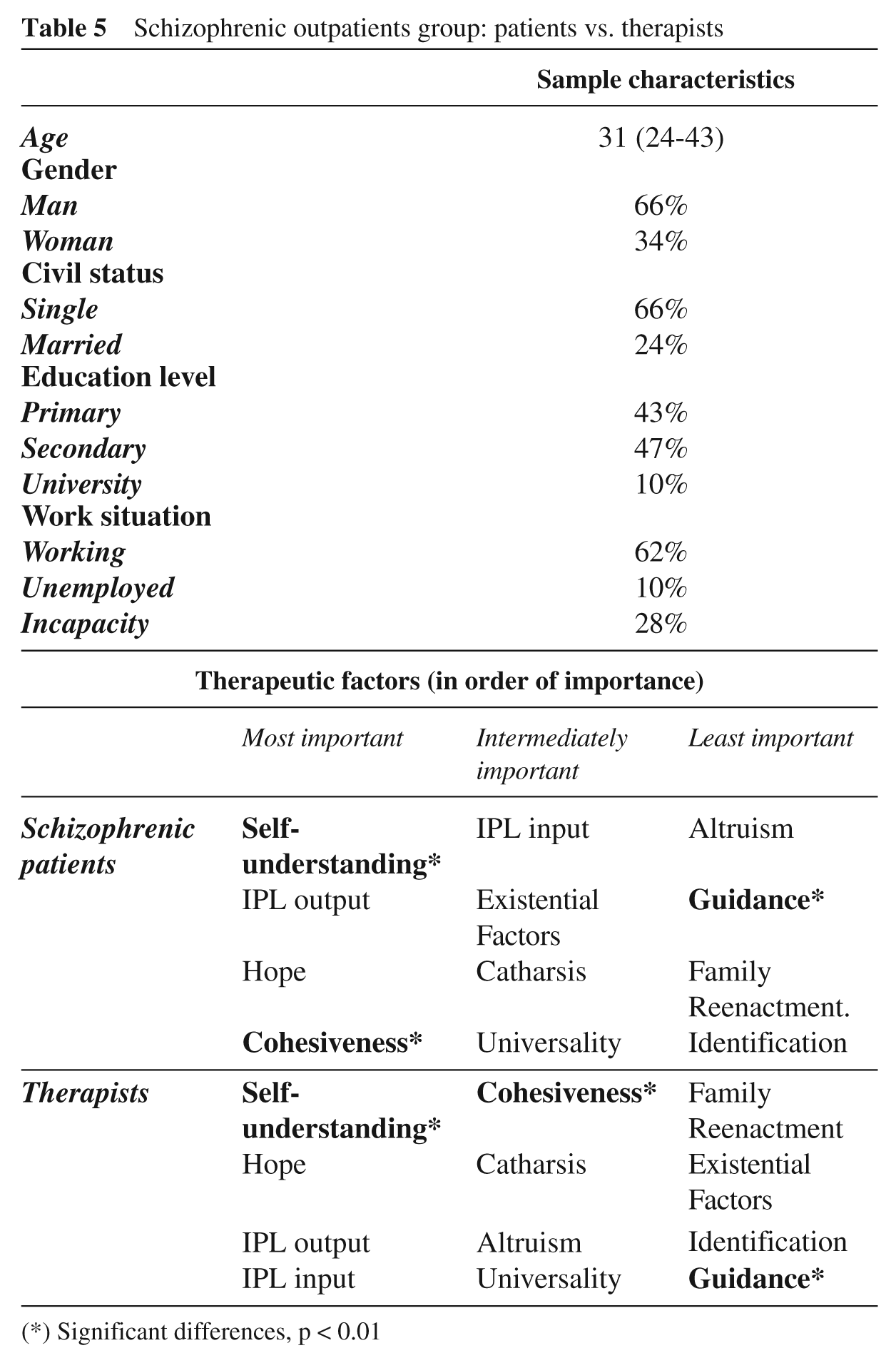
(*) Significant differences, p < 0.01
Results
a) Inpatient Groups: Psychosis versus Affective
The underlining therapeutic factor that patients in both inpatient groups considered most useful was instillation of hope. Additionally, there was also agreement in high value given to factors between the second and the fourth: altruism, interpersonal learning output, and cohesiveness. Both groups agreed on what was deemed least useful: identification, interpersonal learning input, family reenactment, and guidance. Table 1 shows the results of the values in order of importance of the therapeutic factors from both groups.
We found no significant difference between the means of the12 therapeutic factors in both groups or within significant correlations in sociodemographic variables. This suggests that the importance granted to these factors was not conditioned by these variables.
b) Outpatient Groups: Schizophrenic Psychosis versus Bipolar Disorder
In both outpatient groups, the most valued therapeutic factor was instillation of hope, followed by altruism and guidance. We found no significant differences between both outpatient groups. An evaluation of all factors is shown in Table 2.
c) Schizophrenic Patients: Inpatient versus Outpatient Groups (González de Chávez et al., 2000)
The three therapeutic factors considered most useful by the patients from the Acute Unit group were instillation of hope, cohesiveness, and altruism, respectively. Those selected as most important by the outpatient group included instillation of hope, self-understanding, and universality. In both groups, the factor given the highest value was instillation of hope. The three factors receiving the lowest scores in both groups were identification, interpersonal learning input, and family reenactment. An evaluation of these factors is shown in Table 3.
Differences between the means of the therapeutic factors in both groups were statistically significant (p < 0.01) for only two of the 12 therapeutic factors: self-understanding (most valued by the outpatient group patients) and cohesiveness (higher scores by inpatients).
d) Schizophrenic Outpatient Group According to Grades of Insight (García Cabeza and González de Chávez, 2009)
Independent of insight grade, the factor considered most important was instillation of hope, and the factor that received the lowest value was identification. However, changes were observed in the values granted according to the insight level, but only self-understanding varied significantly (F = 4.197, p = 0.037). Self-understanding received a higher value by those patients who had a higher grade of insight. The evaluation of the therapeutic factors, as a whole as well as dependent on insight grade, is shown in Table 4.
e) Schizophrenic Outpatients Group: Patients versus Therapists
All factors are presented in Table 5. There were only significant differences (p < 0.01) in values given to guidance and existential factors (with a significantly better score given by patients) and self-knowledge (scored higher by therapists). The latter factor received the highest value by both therapists and patients. The least important factors for patients were guidance, family, and identification. For therapists, the existential factor, identification, and guidance were the lowest scoring factors.
Discussion
We conclude from our studies that therapeutic factors act independently of diagnosis and orientation of therapists. However, there exists a somewhat more dependent relationship between these therapeutic factors and framework (inpatient and outpatient, with more homogeneous results within each setting than between them). Both the therapeutic factors and group framework are intrinsic elements of group dynamics.
Our studies, like others that have included psychotic patients, found that support factors received the highest value (Maxmen and Hanover, 1973; Marcovitz and Smith, 1983; Kahn et al., 1986; Leszcz et al., 1985; Mushet et al., 1989). Notably, instillation of hope received the highest value independent of patient type and therapist orientation and setting, with the exception for those patients having greater insight and existing in long-term groups. In the case of the long-term group, this factor may have been influenced, since the purpose of the group approach is insight, and the patients in this group reach a higher grade of introspection compared to short-term or inpatients groups.
Instillation of hope contributes both to retaining the patient in his/her group and inspiring optimism, as the patient observes progress in others who have gone through parallel experiences (Yalom, 1985). The actual weight of this factor has always increased when psychotic or hospitalized patients are included (Maxmen and Hanover, 1973; Leszcz et al., 1985; Kahn et al., 1986).
Support factors synergize to provide a therapeutic climate or alliance ultimately to favour cohesiveness. Universality allows patients to prevail over withdrawal and relieve feelings of singularity as they interact with others who have overcome similarities. This enables patients to initiate a process of forming a new and rejuvenated concept of themselves. Moreover, the group also provides patients with the opportunity to assist others (altruism), where they can learn about their own individual feelings and positive aspects of themselves that will also be evaluated by other members of the group. These exercises are dominant in the first stages of the therapeutic process and are also important during therapy process, opening the way to interpersonal learning and self-knowledge factors (Liberman, 1983; Yalom, 1985; Bloch and Crouch, 1985).
In outpatient groups, where priority is not given to psychotic patients, the self-knowledge factor received the highest value (Berzon et al., 1963; Butler and Fuhriman, 1980, 1983; Bloch and Reibstein, 1980; Kapur et al., 1988; Vlastelica et al., 2001). In our groups, there existed a correlation between insight reached and the evaluation of self-understanding. As a patient acquires greater insight, he/she places higher value on this element. In turn, when he/she considers self-knowledge to be a useful interest, the potential to acquire greater insight increases (García Cabeza and González de Chávez, 2009). Furthermore, the time the patient spends in the group favours the greater evaluation of self-knowledge (Rico and Sunyer, 2001), which most likely reflects the longitudinal evolution from support to self-knowledge. Even an important factor such as self-knowledge, however, cannot be understood without collaboration of others. A key commandment within group therapy is that personal knowledge is largely obtained through interpersonal understanding. These two features are inseparable in the change mechanism regarding both the level of development in the subject’s personality and the correction of psychopathological problems (Anthony, 1971). Importantly, this relationship would not exist without factors of self-disclosure and catharsis, which are preconditions for self-understanding and learning (Bloch and Crouch, 1985; Yalom, 1985; Stricker and Fisher, 1990).
Separate mention should be given to the comparative evaluation of the patients compared to those made by therapists. Although both considered self-understanding as the most important therapeutic factor, therapists gave it a much higher score, while patients seemed to place a higher value on existential and guidance factors. This trend has been described previously, showing that the therapist does not always share the perception of utility with patients (Bloch and Reibstein, 1980; Diereck and Lietaer, 2008). Because our groups were oriented toward insight, we may have over evaluated the need for patients to achieve self-understanding. Conversely, we potentially may have placed too little value on other factors, such as advice giving, which is one that is more typical of psychoeducative groups, or even existential factors. In agreement with Liberman (1983), we appreciate that the factor noted by patients as most useful is not always associated with the best results of group treatment. Even factors undervalued in our studies and in others, such as identification (Kapur et al., 1988; Vlastelica et al, 2001; García Cabeza and González de Chávez, 2009), can also serve as a potential source of stimulation and learning for some patients.
In conclusion, we consider that any group intervention, regardless of the therapist’s orientation or type of patient and setting, should always consider the support factor. Special emphasis should be placed on instillation of hope, as this is considered a critical element by patients for their treatment and recovery. Moreover, it is also a key factor for group adherence, which is necessary to achieve all other objectives of therapy.