
Abstract
Aims:
The purpose of this study was to explore how mentalization-based group therapy (MBT-G) for patients with borderline personality disorder may be both different and similar to a more traditional psychodynamic group psychotherapy approach.
Material and methods:
The study is a comparative case-study examining a supposedly representative clinical example of MBT-G and a supposedly representative clinical example of a psychodynamic group (PDG). Both groups were composed mainly of patients with borderline personality disorder. The study used a mixed methodological approach with quantitative research methods, including MBT-G Adherence and Quality Scale and Reflective Functioning Scale (RF-scale), and qualitative content analysis.
Results:
1) The MBT-G therapists focused consistently on mental states and emotions. This was reflected both in a significantly higher intervention frequency, and in a higher proportion of theoretically assumed mentalizing-promoting interventions. 2) We observed an increase in mentalizing (defined as RF) among some patients in the MBT-G group. In the PDG session, RF development were less systematic, and had lesser impact. 3) Interventions with ‘demand’ characteristics might play an important role in developing a mentalizing group discourse. 4) In both groups, therapists and patients actively structured the sessions, but the MBT-G session more explicitly engaged in ‘meta’ discussions about it, i.e. discussing whether a topic should or should not be put on the agenda.
Conclusion:
Despite similarities between the approaches, differences in choice of therapeutic focus and consistency suggest that the two methods engage patients in different therapy processes. The results warrant studies that include more sessions in order to validate or falsify the resulting hypotheses.
Keywords
Introduction
Mentalization-based treatment (MBT) belongs to the psychodynamic tradition (Bateman and Fonagy, 1999). The main target for MBT, borderline personality disorder (BPD), is conceptualized as a disorder of temperament, attachment and self-consciousness, with typical affect regulation and mentalizing deficits. MBT is a conjoint kind of treatment, composed of individual and group therapies. The dynamic group component developed from a British group analytic/psychodynamic group therapy matrix. How far is modern mentalization-based group therapy (MBT-G) from its siblings?
The topic has been discussed in previous issues of Group Analysis (Potthoff and Moini-Afchari, 2014). Potthoff and Moini-Afchari (2014) write that, on the one hand it has been maintained that MBT-G represents a paradigm shift in the way of conducting group therapy and that MBT-G could replace traditional group analysis (Schultz-Venrath, 2010). However, others have been more sceptical and doubted that MBT-G offers anything new (Rudolf, 2006) and argued that MBT and psychoanalytic-interactional approaches are very similar and that the traditional repertoire always has included interventions that intend to foster mentalizing. These are clarification (Glover, 1955), mirroring (Kohut, 1983; Winnicott, 1971) and detailed inquiry (Sullivan, 1954) to name a few.
Already in the early development of group analysis, Foulkes (1984 [1964]) emphasized the unique potential groups had to mirror self-states, object relations and emotions, which he gives priority in his communication theory (Potthoff and Moini-Afchari, 2014). Later, others have pointed to the dangers of malicious, false mirroring (‘malignant mirroring’), e.g. when a group member feels consistently misunderstood or overlooked (Zinkin, 1992). These and other challenges with borderline patients in psychodynamic group therapy have long been known, e.g. through descriptions of how the group can be dominated by projective identification (Zender, 1991). In such groups, therapists will often find themselves confronted with complicated group situations that need to be cleared up and resolved. Recent group analytical thinking has therefore realized that it would be counter-productive to keep an attitude of evenly suspended attention in such situations, and that the BPD-patients’ typical structural weakness sometimes will require more intensive work individually, which in periods might affect the free flow of group processes (Berghaus and Potthoff, 2009; Foulkes, 1964; Potthoff and Moini-Afchari, 2014).
The above-mentioned considerations are mainly based upon clinical reports and risk being speculative. We lack empirical studies, which can enlighten the topic. In this article, we present a relevant clinical study. We have compared, head on, a MBT group session (from 2014) with a psychodynamic group session (from 2006). Both groups were conducted at the same clinical department, with the same type of clientele, but at different periods of time, which hosted different treatment regimes. In what respects are these therapeutic approaches similar or different? Answers to these questions may be helpful in explicating the nature of these group methods, and what kind of processes they elicit in their members. Answers may thus be useful for a more enlightened discussion of how groups should be designed for different purposes. E.g., should group analysis adopt elements from MBT-G when the patient population is predominantly personality disorders? What elements should that be?
Material and methods
The material for this study was two randomly selected group therapy sessions conducted at the Department of Personality Psychiatry, Oslo University Hospital. The first group session, recorded at 31 August 2006, was from an outpatient group, which served as continuation treatment after an initial short-term day hospital phase. The treatment ideology was psychodynamic, integrating object-relations theory and self-psychology, and treatment technique was leaning on (modified) group analytic psychotherapy. We label this group the ‘psychodynamic group’ (PDG). The two therapists were both qualified group analysts, a psychiatrist and a clinical social worker. All patients had a PD diagnosis, most often of cluster B (borderline) type. The patients ought to be considerably affected (symptomatically and functionally) in order to receive this treatment. The group was video-recorded as part of the Ullevål Personality Project (UPP). The results of this treatment were moderately good, as reported in several follow up studies (Antonsen et al., 2014; Gullestad et al., 2012).
This way of organizing and doing treatment for patients with PDs terminated in 2008 when the whole department underwent a radical reorientation and adopted MBT as its principle approach. The second group (labelled MBT-G) was recorded at 21 January 2014 and was part of this new MBT intensive outpatient programme. One of the two therapists was a qualified group analyst and trained in MBT. The other therapist was a psychiatric resident with no formal group or MBT training. The patients were similar to those in 2006, possibly with some more borderline features. The results of this treatment have been reported by Kvarstein et al. (2014) to be very good, with effect sizes that were nearly twice as high as the previous psychodynamic programme. Both groups were slow-open, the sessions lasted for 90 minutes and the maximum treatment length for both conditions were three years. The MBT-G contained six female members, and the PDG five female and one male member. The lack of male members reflects the common gender bias of patients being referred to this kind of treatment. Patients in both groups gave their written informed consent, which was approved, by the regional ethics committee and the patient ombudsman at Oslo University Hospital (OUS).
Both group sessions were carefully transcribed by the first author and analysed for content relevant to our research questions. The original work was completed as a master thesis in psychology (Kalleklev, 2015), containing lengthy quotations and discussions of qualitative issues. In this brief article format, we present a condensed summary. For more detailed verbatim material, we refer to the companion article (Karterud, this issue), which presents a full verbatim analysis of one of the sequences from the MBT-G session. In contrast to the companion article, which demonstrates how a single sequence of highly adherent MBT group therapy can look like, our mission here is more explorative in nature, aiming to formulate hypotheses about similarities and differences across sequences and therapy orientation in real sessions, hypotheses that at a later point may be tested empirically with larger samples. The exploration was mainly theory-driven, where MBT concepts played a central part in the analysis (Lincoln and Guba, 1985). Because of this, the study can be perceived as exploration through MBT-glasses (i.e. using MBT-G rating scales on a PDG session). However, the exploration also touched upon more general psychodynamic group theory. We used both quantitative and qualitative methods of data analysis. However, this does not mean that there can be drawn statistical conclusions from our study, as there was only a single case in each condition.
More specifically, all interventions in both sessions were rated according to the MBT-G Adherence and Quality Scale (MBT-G-AQS) by the Norwegian MBT laboratory (https://www.youtube.com/watch?v=hddIUpUOZdw) (Folmo et al., 2017; Karterud, 2015). Interventions that did not comply with any of the items did not receive any rating. In addition, the session as a whole was given an overall rating. It was pretty obvious from the outset that the MBT-G session would receive a higher adherence score than the PDG session. However, it was expected that also the PDG session would contain interventions that promoted mentalization, e.g. focusing on affects or interventions framed as reflections on affects.
Complementing the analysis of mentalizing content in the groups, patient statements were rated according to the Reflective Function Scale (RF-scale) (Fonagy et al., 1998). The RF-scores represent the extent to which the interviewee in an Adult Attachment Interview (AAI) address and elaborate on mental states in their responses (Hesse, 2008). Reflection on higher mentalizing levels involves adopting a tentative approach that seeks to understand one’s own and others’ feelings, thoughts and behaviour from different perspectives. The opposite, i.e. unreflective functioning, is not to relate events and behavioural expressions to internal mental states. Responses are graded on a Likert-scale from −1 to 9.
In AAI, it is expected that patient responses will depend on whether the question posed addresses explicitly what patients feel and think about themselves and their attachment figures (demand question), as opposed to more open questions (permit question). A characteristic of demand questions is that they require a mentalizing response, while permit questions do not. Recent research has showed that interventions directed toward exploring mental states predict higher RF of subsequent patient responses (Möller et al., 2016). In our study, all interventions that required a mentalizing response were coded as demand interventions. Questions that did not were coded as permit interventions. The RF ratings in this study were done by the first author, consulting with the second author.
Results
A simple counting of therapist interventions clearly differentiated the groups. In the MBT-G session, there were 294 therapist interventions versus 130 interventions in the PDG session. It is not surprising that MBT therapist are more active than PDG therapists. However, the sheer size of the difference surprised us. Furthermore, according to our ratings of the sessions on the MBT-G-AQS (Table 1), only 16 of the 130 interventions in the PDG session complied with the MBT items, compared to 228 of 294 interventions in the MBT-G session. This indicates that these therapists actually did quite different things. As we can see from Table 1, the MBT therapists, to a much larger extent, focused on affects, explored with a not-knowing stance, and engaged patients in mentalizing external and internal group events. We had expected that also therapists in the PDG session would adhere to this. However, they did not. They did different things. The overall rating of the MBT-G session was seven on adherence and six on quality, demonstrating that the MBT-G session was conducted in a high degree of accordance with the manual. The PDG session was given an overall score of one for adherence and two for quality when rated by the MBT-G-AQS. These overall ratings also indicate possibly large differences between the groups.
Frequency of therapist interventions in the PDG session versus the MBT-G session.
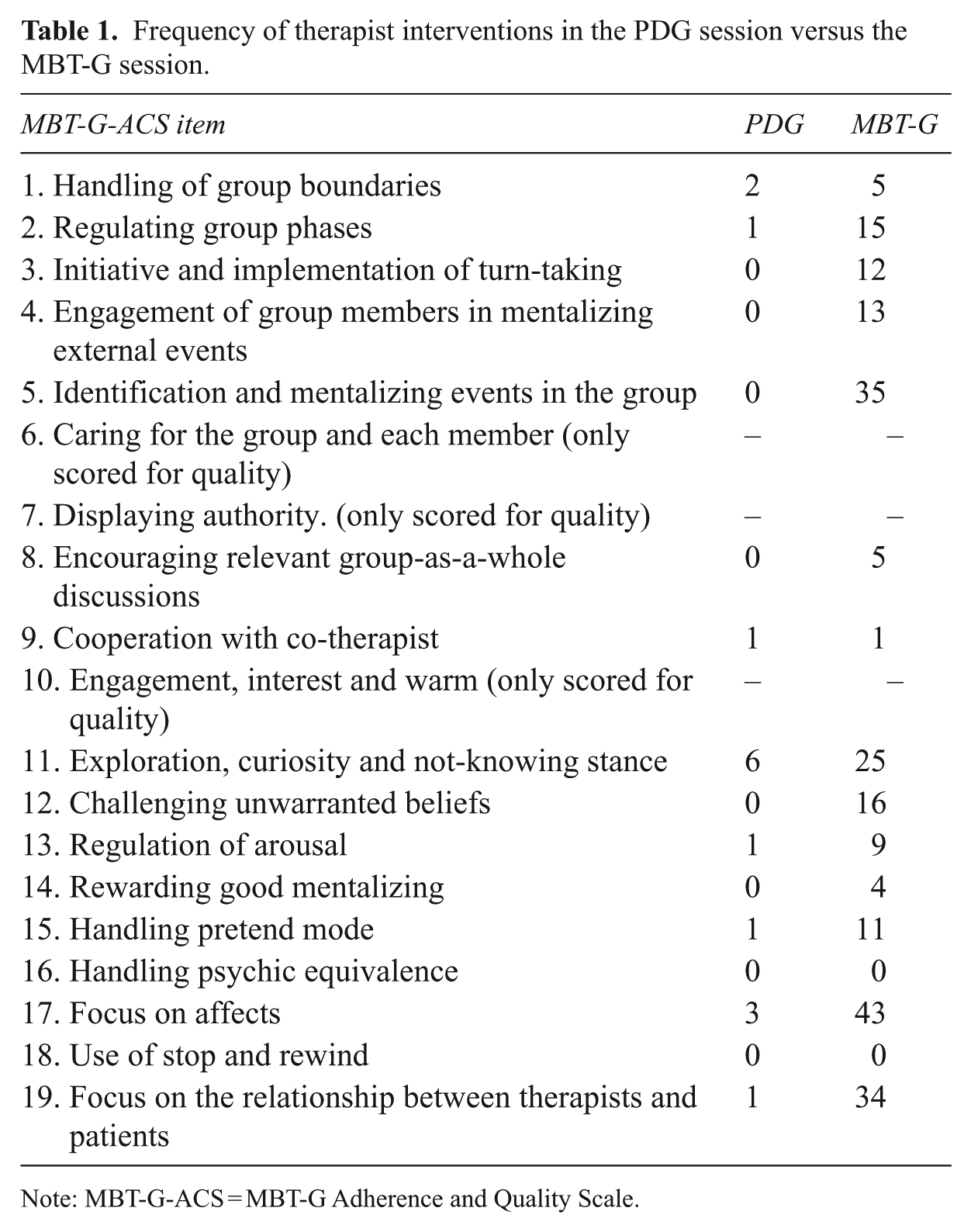
Note: MBT-G-ACS = MBT-G Adherence and Quality Scale.
Across both sessions, the RF level in the dialogues were generally very low at the beginning of the sequences (RF = 1–3). In general, patients described situations and events, rather than feelings and mental states. However, the range of RF in the MBT-G span from one to seven, while the PDG ranged between one to five. Furthermore, two of the sequences in the MBT-G session showed a gradual increase in RF. In the remaining sequences, the pattern was less systematic.
More specifically, the gradual increase in RF witnessed in two of the MBT-G sequences, systematically fell in a context of a series of challenging therapist interventions (demand interventions), seemingly scaffolding the mentalizing focus over a considerable timespan. One of these sequences has been described in detail in a companion article (Karterud, this issue). The particular sequence demonstrates how patient L (a woman in her 30s), at first responds in non-mentalizing manner (empty, having nothing to talk about, refers to external events) to the initial demand intervention that put her on the agenda, and thereby addressed her motives for participating in the group. Scaffolded by recurring reformulations of the initial demand intervention, L gradually turned her attention inward and arrived at defining her difficulties in a more therapeutically operational manner. In turn, we found that the patient gradually recovered her mentalizing abilities and got involved in a complex and highly meaningful interaction with her fellow group mates around important borderline dynamics. However, the process was not a smooth road, and at times when the specifics of the demand questions were not yet answered adequately, the dialogue came to a standstill or was going in circles. In this void, both therapists and participants became engaged in helping her fill in the ‘missing pieces’ (scaffolding), and often collectively arrived at a more elaborated mentalizing account of the problem. Gradually, this group process seemed to help break the entrenched pre-mentalizing habitual thinking which stalled her therapeutic process.
In contrast, the PDG session did not demonstrate consistent patterns of recurring demand interventions (questions demanding a mentalizing answer). If occasionally posed, the demand questions (or other interventions identified through the MBT-G-ASQ), were not further addressed, but were rather diverted by therapists or group members by imposing alternative routes of exploration. An example is when patient C was queried about the depression she experienced. Her labelling it as ‘just an ordinary depression’ was not further challenged by explicitly inviting her to investigate the underlying context. Instead, a co-patient was mirroring that her eyes were wet with tears, to which C replied affirmative, ‘yes, a little bit’, before continuing about the effects of medication and how the depression discouraged her from going out.
Seen through MBT-glasses, the example demonstrates a less focused approach in exploring underlying mental states that could explain her behaviour, possibly reinforcing the pseudo-mentalizing stance, which is observed throughout her sequence. Concluding from this, the intervention strategy in the PDG session could possibly be described as more supportively oriented than challenging.
Despite this approach to mental states, we still found examples of RF development in the PDG session. However, this development did not demonstrate the systematically gradual increase we observed in some of the MBT-G sequences. Instead, in the PDG session, the RF levels seemed to vary more, e.g. going frequently up and down, and typically did not arrive at a stable higher point (RF) toward the end of the sequence. An illustrating example is when patient F was queried about her underlying motives of her recent shopping spree. After having explained that she had inherited some money, the discussion moved towards exploring and clarifying her conflict with spending money on herself and her economic dependency on her parents, which concluded in identifying her distrust of her abilities to care for herself. From there, the discussion moved toward exploring topics like whether there are sex differences in typical patterns of spending money (buying few expensive things versus buying lots of cheap stuff). The exploration relied heavily on clarification and mirroring, including some more challenging questions from fellow patients.
Even though F occasionally arrived on a more developed mentalizing account, there were no instances of demand interventions, except possibly for the one asking for underlying motives. Clearly, the above mentioned mentalizing-promoting approach was not a central part of this PDG sessions strategy. Instead, sporadic mentalizing therapeutic foci were quickly abandoned for the benefit of other foci, e.g. clarifying of events, or a more general exploration of a subject, etc. The process was more like a free-floating explorative group discussion, with little therapist involvement (compared to the MBT-G session).
From the PDG session, there is also worth mentioning how patient A’s highly frustrated feelings of hopelessness and self-denigration, were met with empathic responses and fellow patients’ self-disclosure of similar experiences. These responses, which possibly created room for containing and acceptance of these difficult feelings, seemed to calm down patient A (Bion, 1970). Curiously, her calming down was not accompanied by explicit RF development.
Regarding session structure, our analysis revealed a breakup of the group sessions in sequences. Both sessions consisted of a total of five sequences, however, with variations in length. Most of the sequences were ‘typically’ therapeutic in nature, i.e. consisting of efforts aimed at exploring and/or treating the presenting problems of particular patients. However, the opening and closing sequence of the MBT-G session had a distinctively metacognitive quality, involving discussions as to whether a topic should or should not be put on the agenda. In contrast, there were no explicitly agreed upon agenda in the PDG session. Instead, the participants themselves spontaneously initiated sequences, or were invited in by the therapists along the way. Both groups also contained several smaller in-between exchanges with other patients touching on the same or related themes. It was distinctive for the MBT-G that the legitimacy of such in-between exchanges were a subject for group discussions.
Discussion
The main findings from the study were that:
The MBT-G therapists focused consistently more on mental states and emotions. This was reflected both in the significantly higher intervention frequency (294 in the MBT-G session versus 130 in the PDG session), and in the higher proportion of theoretically assumed mentalizing-promoting interventions (228 versus 16 MBT-G-ASQ rated interventions).
Some patients in MBT-G were observed to increase their mentalizing capability (RF) during the session. In the PDG session, RF development were less systematic (going more frequent up and down), and had lesser impact.
Interventions with ‘demand’ characteristics seemed to play an important role in the development of the mentalizing group discourse.
Therapists and patients in both groups actively structured the sessions, but the MBT-G session more explicitly engaged in meta-discussions about it, i.e. discussing whether a topic should or should not be put on the agenda.
In the following, we will discuss these results in more detail:
Focus on mental states in therapist interventions
The consistent therapist focus on mental states and emotions (228 of 294 interventions), which we found in the MBT-G session, but not in the PDG session, suggests that the MBT-G therapists and the PDG therapists did different things. A high frequency of mentalizing interventions are to be expected in MBT-G, but we had also expected a larger proportion of mentalizing interventions in the PDG session. In fact, according to the MBT-G-ASQ ratings, an explicit focus on mentalizing in the PDG session was almost absent (only in 16 of 130 interventions).
However, the interpretation of this seemingly dramatic difference should be somewhat nuanced. In MBT, the goal of explicating mentalizing is a clearly formulated therapeutic strategy. This means that interventions that are targeting mentalizing in a less explicit manner will lower the MBT-G-ASQ scores. As we have seen in the PDG session, it is possible and also plausible that PDG therapy leans more heavily on strategies that addresses mentalizing in a more implicit manner. For instance, a high proportion of the PDG interventions were clarifying in nature. According to Kernberg (1984), clarifying the course of events, makes it possible to reconsider the ‘true’ nature of events, which may foster the patient’s ability to perceive, interpret, remember, think, consider, decide and then act appropriately in the face of a real life problem. Thus, clarification implies some mentalizing promoting processes, although not necessarily in an explicit MBT manner. We find remnants of clarification in item 11 (‘exploration, curiosity and not-knowing stance’) of the MBT-G-ASQ (Karterud, 2015) and item 16 (‘therapists checking out their understanding with the patients’) of the MBT-ASQ (Karterud and Bateman, 2011), but these interventions direct more explicitly towards mental states, rather than aiming for clarity on a more general level. Another common denominator with MBT interventions might be simply to ask questions (preferably on mental states), which may be a potent means of stimulating an explicit mentalizing discourse. In the PDG session there is less therapist questioning, and more ‘commenting’ through clarification, mirroring, and interpretations.
Summarized, it seems an important difference between the two approaches is that the therapists are actively and explicitly addressing different contents. On a superficial level, these differences may be overlooked, conveying the impression of similarity between these different group modes. Both groups contained six similar patients sitting in a circle with two therapists who tried to stimulate collective reflections on their life experiences. However, the lack of a consistent explicit focus on mental states in the PDG session suggests that we are talking about different therapeutic purposes and different therapeutic processes.
Patient mentalizing
The higher occurrence and greater increase in RF in the MBT-G session may not be surprising since explicitly stimulating mentalization is the primary target of MBT. Even though there exist similar findings from individual MBT (Möller et al., 2016), to our knowledge, no previous studies have explored this particular topic in group therapy. Thus, the finding complies with basic assumptions about the mechanisms of MBT-G. Speaking conversely, an absence of positive correlation between a highly adherent MBT group and RF development in patient responses could have raised doubts about the MBT-G’s suitability in fostering mentalizing abilities.
As already touched upon, the PDG may not have shared the specific ambition of stimulating explicit mentalizing. Also, when assessing mentalizing in patient statements, the RF scale is predominantly sensitive to explicit evidences of mentalizing. Nevertheless, it is still possible that important mentalizing processes in the PDG patients occurred on an implicit level. However, the design of this study was not adequately rigged to explore this question in depths, so we can only speculate. A possibility is that more implicit factors of the established group culture may have had an impact in facilitating patients to recognize or touch upon a mentalizing discourse. The containment episode we witnessed in the PDG session, should possibly according to theory, help restore the patient’s capacity to think under activation of strong negative emotions (Bion, 1970). However, this hypothesized process within the patient could not be detected by the RF-scale. Consequently, the episode could be an example of a group processes that may foster mentalizing in a more implicit fashion.
On a more general level, it is also worth noticing that the low RF levels at the start of the sequences may underscore the fact that establishing a mentalizing discourse is not the default modus operandi with these patients. Taking into account that the members of the MBT group also had completed a psychoeducational MBT group, had received parallel individual MBT sessions, and had frequently been exposed to a mentalizing group discourse, suggest that initiating and engaging in an explicit mentalizing group dialogue is predominantly non-automatic and requires great efforts to achieve (Bateman and Fonagy, 2004). In the context of MBT-G, reminding the patients of the purpose of MBT group psychotherapy should possibly be a routine requirement during each session.
Role of demand interventions
Identifying interventions and strategies for maximizing mentalizing in groups are important topics for further developments in group psychotherapy. In this study, demand interventions emerged as a candidate factor in facilitating mentalizing. Possibly, it may be that the explicitness of demand interventions more effectively guides patients into a mentalizing mindset. The specificity of these questions, also make it more conspicuous if patients fail to respond to them. In response to permit interventions, which involves querying in a more open manner, patients may more easily respond in avoiding or habitual ways, without it being noticed by the rest of the group. As we saw from the sequence of patient L in the MBT-G session, the focus of the recurring demand interventions were already touched upon in the opening sequence, and were sustained through reformulations throughout the whole sequence. Plausibly, this triggered the patient’s mentalizing effort, either due to perceived external pressure from the group or from internal dissonance, to fill the gap between her spontaneous sparingly elaborated mentalizing answers and the explorative possibilities embedded in the questions. A key point of understanding, we believe, is that the possible transformative power of these demand interventions not only lies in the demand interventions’ characteristics, but also in the efforts to maintain a challenging and demanding focus over a time span, through repeating and reformulating demand interventions with tailored precision. Possibly, this combination pays off and evolves the discourse further, overcoming standstills or deadlocking, due to a growing discontent with the limitations of the quick, habitual, often pseudomentalizing answers. In this way, the above-mentioned qualities of demand interventions can function as a framework for a mentalizing therapy process—a process, which may be considered beneficial for a wide range of patient groups. Due to special challenges of borderline patients, keeping a focused streak of demand interventions on the agenda, and not slipping on the subject, also warrants intensive efforts on the therapists’ behalf.
As for the interventional style of the PDG session, which for the most part qualified as permit interventions, neither the frequency of mentalizing-promoting interventions nor intervention frequency in itself seemed to be high enough to reproduce this particular therapeutic approach, which may be a requisite for more effective mentalizing work with some patients. Consequently, if present, effective mentalizing work in the PDG session, operated under different conditions, possibly on a more implicit level.
In addition, a somewhat surprising observation was the supportive nature of the PDG session. Abandoning the traditional challenging interpretative approach in favour of a more clarifying approach reinforced this impression. Possibly, the analysis of the PDG session may illustrate a common phenomenon, i.e. that therapies tend to drift towards supportive modes due to activation of attachment/care within the therapists in response to the despair of the patients (Karterud et al., 2016). In the latter case, this suggests that there is need for something extra to maintain a more challenging demand attitude from the therapists, e.g. collegial support, supervision and a theory that justifies demand questions and explains the risk for a pseudomentalizing group discourse.
Structuring of the group
The lack of an opening agenda setting and the relatively low intervention frequency of the PDG session, may have intended to rig the group towards expressing itself spontaneously. According to psychodynamic group therapy theory, the unconscious interactional patterns that then emerge could be the focus for the group therapy (Karterud, 1999; Lorentzen, 2014). Furthermore, growing patient autonomy, is seen as a healthy part of the group process, and is therefore encouraged (Lorentzen, 2014). High therapist activity, however, which we saw in the MBT-G session, could possibly be seen as disturbance of an ‘open-ended’ process (Foulkes, 1964). In addition, setting an agenda at the start of the meeting is believed to encourage intellectualization rather than the free-floating association and interaction (Karterud, 1999).
Nevertheless, compared to traditional group analytic therapy, the PDG session demonstrated more structuring of the therapy process than we had expected. This concurs with more supportive-oriented approaches, where therapists is taking greater responsibility to include participants who for various reasons remain passive (Lorentzen, 2014). With borderline patients, this strategy may help to avoid group members feeling misunderstood or overlooked (Zinkin, 1992).
In this way, the PDG session contained a mixture of patients spontaneously putting themselves on the agenda (free-associating) and therapists structuring through addressing patients directly with questions about specific topics. As a result, this created a structure where some patients got a turn, similar to the pattern of sequences we found in the MBT-G session. However, in the PDG session there was no explicit discussion about whom and what should be put on the agenda or not. Therefore, the difference was not so much about having a turn-taking structure or not, but rather about the degree of explicitness in discussing whom and what these turns should be about. In other words, we find that this metacognitive perspective taking, stands out as a distinctive feature of MBT-G. The theory says that it will stimulate mentalizing (Karterud, 2015).
Concluding remarks
In sum, our findings suggest hypotheses about important differences between MBT-G and PDG therapy. Of course, as our analysis was based on only a single case of each condition, the differences observed may be due to peculiar characteristics of therapists, patients and group dynamics that are not necessarily representative of MBT-G and PDG in general. However, the differences mainly concur with central theoretical concepts, though a somewhat surprising observation was the supportive nature of the PDG session. In our study, the PDG had obviously drifted quite far from its group analytic ideals and origins. Furthermore, the lack of measures that specifically capture the intervention style of the PDG session, may have contributed in producing a somewhat unfair presentation of PDG therapy, and possibly skewed the results towards an overemphasis on differences, overlooking similarities. Of, course, our attempt to explore a real session of PDG therapy seen through MBT-glasses, will not be fully sensitive to the conceptual richness in perspectives of the psychodynamic group therapy tradition. Still, we believe that our approach can be a fruitful strategy to better understand certain specifics of the relationship between these two schools of group therapy.
In conclusion, before making any claims about the truth value of the findings there should be done studies that include mores sessions and more therapists, counteracting the aforementioned limitations.