
Abstract
This study, using state data, empirically examines the factors affecting the availability of abortion providers over the period 1992–2011. The empirical results found that the labor force participation of women and the percentage of women of reproductive age in the 18–24 age group were positively associated with the number of abortion providers in a state. The level of antiabortion activities and antiabortion attitudes were negatively associated with the number of abortion providers in a state. Also, a state’s abortion rate was positively associated with the number of abortion providers. The enforcement of a parental involvement law by a state significantly deters physicians or organizations from becoming or remaining abortion providers.
Introduction
Abortion has been legal in all states since 1973 when the U.S. Supreme Court ruled in Roe v. Wade that a woman’s right to choose to have an abortion was a constitutionally protected right of privacy. After the 1973 Roe v. Wade decision, the incidence of abortion increased steadily, peaking in 1981. Since 1981, the number of abortions declined from 1.57 million in 1981 to 1.05 million in 2011. The abortion rate (the number of abortions per 1,000 women of reproductive ages 15–44) declined from 29.3 in 1981 to 16.9 in 2011. The abortion ratio (the number of abortions per 1,000 pregnancies) declined from 301 in 1981 to 212 in 2011. Between 1981 and 2011 the number of abortions and the abortion rate fell in every state (Jones & Jerman, 2014).
Until 1992, the Supreme Court permitted little regulation of abortion by states. In 1992, the Supreme Court, in Planned Parenthood of Southeastern Pennsylvania v. Casey, established new parameters for state regulation of abortion. The Supreme Court ruled that states could impose restrictions on a woman’s abortion access provided that the restrictions did not impose an undue burden on a woman’s right to obtain an abortion. The Court defined the undue burden standard as a policy that “. . . has the purpose or effect of placing a substantial obstacle in the path of a woman seeking an abortion of a nonviable fetus” which is the prevailing legal standard today. The vagueness of the undue burden standard resulted in an expansion of state laws and regulations that were intended to reduce a woman’s access to an abortion. As a consequence, there is considerable variation in regulation of abortion and the availability of abortion providers across states.
Researchers in the social sciences (e.g., political science, economics, sociology, public policy, psychology, demography) have focused almost exclusively on the impact of state abortion policies on women with unwanted pregnancies (i.e., the demand side). Surprisingly, there has been virtually no empirical analysis of the factors that influence the availability (number) of abortion providers. We know very little about the factors, including the regulatory environment (restrictive abortion laws), that influence the number of abortion providers.
This article addresses the following questions: (a) Does a greater level of abortion demand increase the number of abortion providers or induce greater regulation of abortion providers reducing their availability? (b) Does the enforcement of state-level abortion restrictions impact the availability of abortion providers? (c) Do antiabortion activities reduce the number of abortion providers? (d) Does a state’s antiabortion attitudes impact the number of abortion providers?
The answer to these questions merits attention for several reasons. First, there are public and social policy concerns about the availability of abortion services. Access to abortion is a major factor in the fertility of women. In the 1992 Casey decision, the Supreme Court acknowledged that “. . . the ability of women to participate equally in the economic and social life of the Nation has been facilitated by their ability to control their reproductive lives.” Second, the number of abortion providers and the geographical distribution of abortion providers determines access to abortion. Greater availability of abortion providers impacts the demand for abortion by reducing the search costs, time costs, and the out-of-pocket travel costs associated with obtaining an abortion. Third, the constitutional right of a woman to obtain an abortion is meaningless if, because of a restrictive abortion law, there are too few abortion providers to perform the procedure. Fourth, the determinants of the availability of abortion providers are of interest to those on both sides of the abortion debate.
Clearly, investigation of the factors that influence the number of abortion providers adds to the literature on abortion. This study fills the gap in the literature by empirically analyzing the determinants of the number of abortion providers over the time period 1992–2011.
Restrictive Abortion Laws
There are five types of restrictive abortion laws that the Supreme Court has held to be constitutional.
Medicaid is the federal health insurance program run by the states for low-income households. Each state has its own program, combining federal and state funding, that provides medical services for those qualifying. In 1980, the Supreme Court ruled that a law passed by Congress (i.e., the Hyde amendment), prohibiting federal Medicaid funds from being used to pay for an abortion and gave states the right to deny state funding of abortions, was constitutional. Many states then enacted laws that prohibited the use of their public funds to pay for Medicaid abortions for low-income women.
Since the 1973 Roe v. Wade decision, the Supreme Court, in a series of cases, has consistently held that unmarried teen minors (less than 18 years of age) have a constitutional right to have an abortion. But, states may require that a parent be involved—be notified or give consent—before an abortion is performed.
Many states have enacted mandatory counseling laws that require an abortion provider give or offer to women state-mandated medical information about abortion (e.g., fetal development, future health risks, adoption options). Most mandatory counseling states allow the information be provided to the patient by mail, fax, video, telephone, or the internet before the day of the procedure (i.e., not in person).
Several states have enacted a more proscribed type of mandatory counseling that requires women receive the medical information in person, usually 24 hr before the procedure. These two-visit laws require that women make two separate trips to the abortion provider.
Since the mid-1990s, some states have enacted Targeted Regulation of Abortion Provider laws (more commonly known by the acronym TRAP laws). TRAP laws impose on abortion providers, but not other comparable medical professionals, unnecessary and burdensome physical plant and staffing requirements. For example, North Carolina requires that abortion providers must hire a registered nurse with experience in post-operative and post-partum care, who is on duty at all times as well as provide a nourishment station for serving snacks.
Literature Review
Most empirical studies use multivariate regression on pooled time-series cross-section state data to estimate the impact of various restrictive abortion laws. Virtually all the studies on the impact of Medicaid funding restrictions consistently find that a state funding restriction of Medicaid abortions reduces a state’s abortion rate by 3% to 5% (Blank et al., 1996; Levine et al., 1996; Medoff, 2007). Empirical estimates of the numerical impact of a parental involvement law are ambiguous. Some studies find that parental involvement laws had no statistically significant impact on the abortion rate of women of childbearing age (Bitler & Zavodny, 2001; Blank et al., 1996; Haas-Wilson 1997). Other studies find that parental involvement laws reduce the abortion demand of women of childbearing age by between 3% and 6% (Medoff, 2007, 2008).
Much less attention has been directed to the study of the impact of mandatory counseling laws. The few studies have found that mandatory counseling laws represent a negligible increase in the total cost to women of obtaining an abortion (Joyce, 2011; Medoff, 2008). Mandatory counseling laws have no statistically significant impact on abortion demand. This empirical result is not surprising. The reason is that in most states that require mandatory counseling, the abortion provider does not have to furnish the state-approved medical information in person and there is no requirement that women actually read the material given to them.
Abortion rights supporters argue that the implicit or explicit intent of TRAP laws is, by imposing medically unnecessary, burdensome and costly regulations on abortion providers, to deter physicians from becoming abortion providers or drive abortion providers out of practice and make abortion services more difficult to obtain. The handful of empirical studies on TRAP laws appear to support their contention. Joyce (2011) found that a Texas TRAP law on facilities that performed abortions after 16 weeks resulted in a decrease in the number of abortions performed at 16 weeks or more on Texas residents 1 year after the law was in effect. Although women did become more likely to travel out of state to obtain an abortion, the net effect was Texas women had fewer abortions. Similarly, Jones and Weitz (2009) reported that a TRAP law enacted in Mississippi in 2005 caused the only out-patient abortion provider in Mississippi to stop providing abortions after 12 weeks of gestation resulting in an increase in unwanted births.
Taken together, the body of empirical results reported above suggests that, other than financial barriers, state abortion rates are largely unaffected by these demand side policies. These demand side policies dissuade very few women with unwanted pregnancies from having an abortion. However, the regulatory environment in a state may have an indirect effect on abortion demand, decreasing the availability of abortion services by reducing the number of abortion providers.
Model
Because of the paucity of research on the supply side of the abortion market, there are no formal theoretical models of the determinants of the number of abortion providers. The number of abortion providers in a state is posited to be a function of the antiabortion activities, antiabortion attitudes, antiabortion interest group strength, and the abortion environment in a state. The abortion provider equation to be estimated is

The dependent variable is the number of abortion providers per 100,000 pregnancies in state i for the years t = 1992, 1996, 2000, 2005, 2008, and 2011. Thus, there are 300 observations. The Guttmacher Institute periodically conducts a thorough survey of the number of abortion providers in each state. The sample years 1992, 1996, 2000, 2005, 2008, and 2011 are examined because these are the only years the Guttmacher Institute conducted their abortion provider survey. The dependent variable is a relative measure rather than an absolute measure because the number of abortion providers for a given number of pregnancies controls for differences across states and over time in the number of women who are pregnant.
The variable LFP is the labor force participation rate of women aged 16+. Women in the labor force are more likely to have an abortion than women not in the labor force because of the higher opportunity cost of childbearing/childrearing due to the loss of job training and work experience. As a consequence, higher rates of labor force participation of women should be associated with more abortion providers in a state.
Abortion providers have frequently been subject to violence, protests, and harassment. These antiabortion activities are designed to confront, intimidate, harass, or create a climate of fear against abortion providers and staff. According to statistics compiled by the National Abortion Federation (2012), an organization of abortion providers, there have been eight murders of abortion providers and staff (the last was the assassination of Dr. George Tiller in Wichita, Kansas in 2009), 17 attempted murders, 42 abortion clinic bombings, 182 arsons, 429 death threats, 554 stalking incidents, and 176,112 picketing incidents over the period 1977–2014. These antiabortion activities increase the perceived risk to abortion providers and may have caused a reduction in the number of abortion providers or restricted the entry of abortion providers. The variable Antiabortion Activities is the percentage of abortion clinics in state i that experienced harassment (i.e., picketing, blockades, vandalism, stalking of physicians or staff) during time period t.
The antiabortion attitudes of a state may influence the number of abortion providers. States with greater antiabortion attitudes are more likely to have fewer abortions and, concomitantly, few abortion providers. There may be differences in the antiabortion attitudes between states and the failure to control for the antiabortion attitudes in a state may result in spurious estimates. Each year NARAL 1 Pro-Choice America (2001) assigns a letter grade (i.e., A, B, C, D, F) to each state based on the total number of laws/regulations/policies a state has that restricts a woman’s access to reproductive health care. A state’s Antiabortion Attitudes score was calculated by converting these letter grades into numerical values (A = 4, B = 3, C = 2, D = 1, F = 0). For ease of interpretation, these scores were multiplied by 100 and transformed so that the greater a state’s numerical value the more antiabortion a state’s public attitudes.
Evangelical Christian fundamentalism has been found to have a significant effect on women’s views and commitment about premarital sexual activity, contraception, abortion, childbearing, and the proper role of women in the family. Evangelical Christians also are the religious group most associated with organized antiabortion activities against abortion providers. These deeply held religious beliefs of Evangelical Christians may be a significant factor in the decision of abortion providers to supply abortion services. The variable % Evangelicals is the percentage of a state’s population that belongs to a religious denomination that believes in the literal interpretation of the Bible. The increased presence of Evangelical Christians may reduce the number of abortion providers in state i.
Sexual activity/unintended pregnancies are not constant across the reproductive age span of women of reproductive age (15–44 years). Women aged 18 to 24 are much more likely to be sexually active, have an unintended pregnancy, and have an abortion than women in any other reproductive age group (Henshaw, 1998). Abortion providers may be more likely to locate in states that have a higher percentage of women aged 18 to 24, where the need for their services is greater. The variable % Women 18–24 is the percentage of women of reproductive age (15–44 years) who are 18 to 24 years old, the group with the highest unintended pregnancy rate.
Women in states with few abortion providers can travel to neighboring states with more abortion providers. The number of abortion providers in neighboring states may be inflated if women in states with few abortion providers are traveling to neighboring states to obtain an abortion. The variable % Out-of-State Abortions is the percentage of abortions in state i, year t, that were performed on out-of-state residents.
The variable of particular interest in this study, Abortion Rate, is the abortion rate—the number of abortions per 1,000 women of reproductive age (15–44)—in state i, time period t. A positive coefficient would suggest that the availability of abortion providers is directly related to the market demand for abortion. That is, the demand for abortion increases the number of abortion providers. A negative coefficient would be an indication that state legislators respond to high abortion rates by enacting regulations/policies that reduce the availability of abortion providers.
Data
The number of abortion providers, the abortion rate, and the number of pregnancies for the years 1992, 1996, 2000, 2005, 2008, and 2011 are from the Guttmacher Institute. All the socioeconomic data used in this study are available in the United States Bureau of the Census & U.S. Census of the Population (1993, 2003, 2013) or the Statistical Abstract of the United States (1993, 1997, 2001, 2006, 2009, 2011). The data on Evangelical Christian religious membership in each state are from the Association of Religious Data Archives (2015). Data on antiabortion activities were provided by the Feminist Majority Foundation (2011). The status of restrictive abortion laws in each state is from the Guttmacher Institute’s State Policies in Brief. Summary statistics for all variables appear in Table 1.
Summary Statistics for Multiyear Sample.

Per 100,000 pregnancies.
Per 1,000 women of reproductive age.
Empirical Results
In Equation 1, the number of abortion providers and the abortion rate reflect the interaction of supply and demand. That is, abortion availability (number of abortion providers) is determined by both the willingness of those who supply abortion services as well as the willingness of women with unwanted pregnancies to purchase abortion services. As such, the number of abortion providers is determined simultaneously with the quantity of abortions (i.e., the number of abortion providers and the abortion rate in Equation 1 are endogenous).
The econometric solution to this problem is to find instruments (variables) for the abortion rate in Equation 1 that are correlated with the abortion rate, but do not directly affect the number of abortion providers. The instruments selected are the number of non-OBGYN physicians per 100,000 residents, the number of nurses per 100,000 residents, and the average weekly wage of employees in the offices of physicians. These variables are related to the overall level of accessibility, availability, and cost of general medical services in a state, but are unlikely to affect the number of abortion providers. The bivariate correlation between the abortion rate and (a) the number of non-OBGYN physicians per 100,000 residents was .417 (t = 7.92), (b) the number of nurses per 100,000 residents was .112 (t = 1.96), and (c) the average weekly wage of employees in the offices of physicians was .095 (t = 1.65).
Equation 1 is estimated using a two-stage procedure, whereby the abortion rate is estimated in a first-stage equation with all the exogenous variables in Equation 1 and the three instruments. In the second stage, the abortion rate variable in Equation 1 is replaced with the predicted values of the abortion rate from the stage one estimation and Equation 1 is then estimated using ordinary least squares. The regression coefficients (and the absolute value of the t-statistics in parentheses) of the two-stage least squares estimation of Equation 1 appear in Table 2, Column 1.
Regression Results: Determinants of Suppliers.

Note. Absolute value of t-statistics in parentheses: *p< .10, **p< .05, ***p< .01, ****p< .001.
As hypothesized, Antiabortion Activities (p < .05) and Antiabortion Attitudes (p < .001) are significantly negatively associated with the number of abortion providers in a state. The labor force participation (LFP) of women (p < .01) and the percentage of women of reproductive age in the 18–24 age group (p < .001) are significantly positively associated with the number of abortion providers in a state.
Since these four independent variables are measured in different units, the estimated values of the unstandardized regression coefficients cannot be directly compared. For example, a one-unit change in the percentage of women of reproductive age in the 18–24 age group is not comparable to a one-unit change in the level of antiabortion activity. This problem can be addressed by computing standardized regression coefficients, which adjust the estimated slope coefficient of an independent variable to the standard deviation of the dependent variable. Standardized regression coefficients describe the relative importance of the independent variables on the dependent variable in terms of standard deviation units and thus make it possible to compare the impact of each independent variable on an identical metric.
The standardized regression coefficients show that for a change of one standard deviation in the percentage of women of reproductive age in the 18–24 age group, labor force participation of women, the level of antiabortion activities, and the level of antiabortion attitudes will cause a change in the standard deviation of the number of abortion providers per 100,000 pregnancies by .281, .168, −.093, and −.321, respectively. The standardized regression coefficients show that Antiabortion Attitudes in a state are the largest single determinant in reducing the number of abortion providers in a state. This finding is consistent with the anecdotal evidence that the public’s antiabortion attitudes in a state have been successful in preventing some providers from offering abortion services.
A state’s Abortion Rate is significantly (p < .05) positively associated with the number of abortion providers in a state. The demand for abortion in a state increases the number of abortion providers. The responsiveness in the number of abortion providers with respect to a change in a state’s abortion rate is .48. A decrease in a state’s abortion rate by 5% is associated with a decrease in the number of abortion providers per 100,000 pregnancies by 2.4%. This suggests that, as the abortion rate falls, the number of abortion providers decreases at a decreasing rate (i.e., there are diminishing returns). The reason for this finding may be that, because of economies of scale (cost savings that result from larger scale of operation), abortions are increasingly concentrated among a small number of very large providers. 2 Over the period 1996–2011, large abortion providers (+1,000 abortions) consistently performed 80% of all abortions (Jones & Jerman, 2014).
It might be argued that the empirical results in Column 1 of Table 2 may be spurious since, over the time period examined, there may be time-varying factors such as welfare reform, more federal government support of family planning services for low-income households, a growing awareness about the possible harmful effects of HIV/AIDS and other sexually transmitted diseases, and the use of more efficacious methods of contraception that may have affected sexually active women equally in all states. If these time-varying factors were correlated with a state’s abortion rate, then the estimated coefficient of the abortion rate variable in Column 1 would be overstated since it would include some of the effects of the omitted time-varying factors.
To account for this possibility, a year fixed effects model (i.e., a separate dummy variable for the years 1992, 1996, 2005, 2008, 2011) was included in the estimation of Equation 1. The empirical results, reported in Table 2, Column 2, show that even after controlling for time-varying factors, a state’s Abortion Rate is still significantly (p < .05) positively associated with the number of abortion providers. The coefficient of the Abortion Rate variable is half the value of the coefficient of the Abortion Rate variable in Column 1. A decrease in a state’s abortion rate by 5% is associated with a decrease in the number of abortion providers per 100,000 pregnancies by 1.2%. Again, this suggests that the number of abortion providers decrease much more slowly than decreases in the abortion rate, presumably because the abortion market consists of a small number of providers who perform almost the entire market output.
One obvious concern in estimating Equation 1 is that there may exist unmeasured or unobserved differences that are specific to each state. If this occurs, the estimate between the abortion rate and the number of abortion providers reported in Table 2, Column 1, may not be causal. Rather, it may be a result of the abortion rate being correlated with the unmeasured or unobserved factors within a state which, in turn, influences women’s abortion decisions, resulting in a spurious estimate of the impact of the abortion rate on the number of abortion providers.
The most common econometric technique to control for these unmeasured or unobserved factors, used with virtual unanimity by researchers, is to use a state fixed effects model (i.e., inclusion of a dummy variable for 49 of the 50 states). A state fixed effects model controls for unmeasured time-invariant differences across states that are not captured by the independent variables in the model. Moffitt (1994) argues that a state fixed effects model merely measures the effects of some of the explanatory variables that are poorly measured or omitted from the true model because of the unavailability of data. As a consequence, it is argued that state fixed effects are inadequate proxies or imperfect controls for the poorly measured or omitted explanatory variables. In addition, a state fixed effects model implicitly (and incorrectly) assumes that these unobserved, unmeasured or omitted variables that are specific to each state are constant or unchanged over time.
Nevertheless, Column 3 of Table 2 shows the regression coefficients when state fixed effects are included in the two-stage least-squares estimation of Equation 1. The empirical results in Column 3 show that even after controlling for state fixed effects, the abortion rate is still significantly (p < .05) positively associated with the number of abortion providers and its regression coefficient is virtually identical (null hypotheses of equality of coefficients cannot be rejected) to its respective counterpart in Column 1 (no state fixed effects).
Whether or not time fixed effects or state fixed effects are included in the estimation of the abortion provider equation, the reported significantly positive coefficients of the abortion rate in Columns 1, 2, and 3 of Table 2 indicate that the abortion rate in a state is directly related to the availability of abortion providers. The demand for abortion services increases the number of abortion providers. In addition, the empirical results show that there are diminishing returns to the number of abortion providers—decreases in the abortion rate decrease the number of abortion providers at a decreasing rate.
Restrictive State Abortion Laws and the Number of Abortion Providers
The available empirical evidence in the literature indicates that other than Medicaid funding restrictions, restrictive state abortion laws have had a modest impact on the national abortion rate. However, restrictive state abortion laws may have had an indirect effect on abortion rates by reducing the availability of abortion providers. Restrictive abortion laws may decrease the availability of abortion services by increasing the costs incurred by abortion providers to comply with the restrictive abortion laws.
As noted by Althaus and Henshaw (1994), some of the extra costs imposed on abortion providers because of the enforcement of Medicaid funding restrictions, parental involvement laws, mandatory counseling laws, two-visit laws, and TRAP laws include (a) the hiring of more staff personnel; (b) longer hours for nurses and medical technicians; (c) greater physician consultation time; (d) additional mailing, telephone, fax, and video expenses; (e) additional report and record-keeping expenses; (f) licensing fees; (g) remodeling expenses; and (h) the legal expenses incurred to insure that abortion providers are in strict compliance with the restrictive abortion laws.
Table 3 shows the average number of abortion providers per 100,000 pregnancies for the 50 states, over the time period 1992–2011, in states with and without Medicaid funding restrictions, parental involvement laws, mandatory counseling laws, two-visit laws, and TRAP laws. The empirical results in Table 3 suggest the availability of abortion providers is associated with the regulatory environment in a state. There are significantly fewer abortion providers in states with parental involvement laws, two-visit laws, and TRAP laws than in states without these restrictive abortion laws. These differences are statistically significant at the .001 level using a one-tail or two-tail probability test.
Mean Number of Abortion Providers in States With and Without Specific Restrictive Abortion Law.
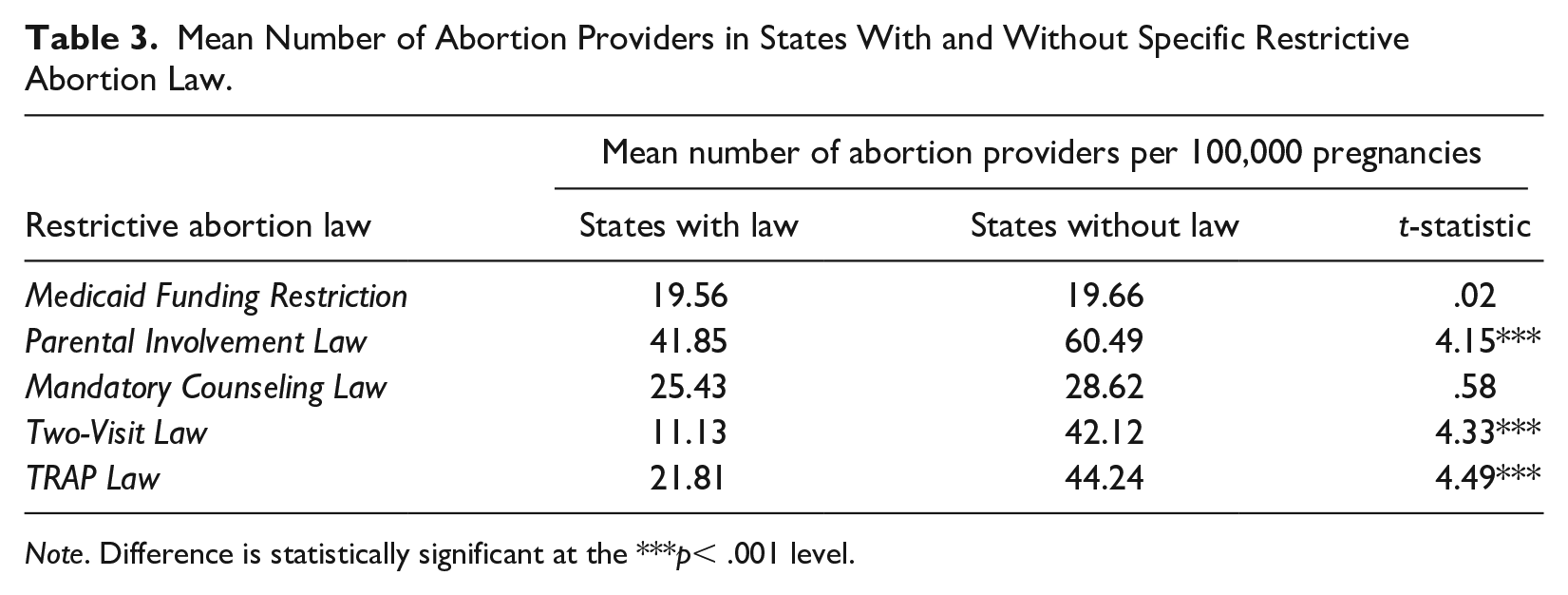
Note. Difference is statistically significant at the ***p< .001 level.
However, the evidence presented in Table 3 is merely descriptive and cannot be interpreted as necessarily a causal effect. There may be differences in socioeconomic characteristics, antiabortion beliefs, or antiabortion activities between states with and without the particular restrictive abortion law in Table 3. To determine whether a causal link exists between restrictive abortion laws and the number of abortion providers, a multivariate regression must be estimated that controls for state differences.
Equation 1 was re-estimated with the abortion rate replaced with a vector of indicator variables (=1) that measure whether the restrictive abortion laws were in effect in each state/year. No Medicaid Funding is equal to one if state i did not allow its public funds to pay for Medicaid abortions during time period t. Parental Involvement Law is equal to one if state i required parental involvement (either permission or notification) before an unmarried teen minor can have an abortion. Mandatory Counseling Law is equal to one if state i required an abortion provider furnish to women state-mandated abortion-specific medical information before the abortion is performed, but the information does not have to be provided in person. The variable Two-Visit Law equals one if state i required the state-mandated abortion information be provided in person at least 24 hr before the procedure, thereby necessitating two separate trips to the abortion provider. The variable TRAP Law equals one if state i imposes physical plant or staffing requirements on abortion providers, but not on other comparable physicians/clinics.
One obvious concern is that a state’s restrictive abortion laws are not exogenous. Medoff (2012) found that the enactment of restrictive abortion laws depends on the political strength of well-organized interest groups opposed to abortion and when the ideologically antiabortion Republican Party controls both houses of the state legislature and the governor’s office in a state.
The empirical results, when the vector of restrictive abortion laws replace the abortion rate in the estimation of the abortion provider Equation 1, appear in Table 4, Column 1 (when there are no time fixed effects or state fixed effects), Column 2 (when time fixed effects are included), and Column 3 (when state fixed effects are included). Because of space limitations, only the regression coefficients for the restrictive abortion laws appear in Table 4.
Regression Results: Public Policy Effects on Number of Suppliers.

Note. Absolute value of t-statistics in parentheses: ***p < .01, ****p < .001. Model also includes labor force participation, antiabortion attitudes, antiabortion activities, percent Evangelicals, percent women 18 to 24, and percent out-of-state abortions as described in the text.
Of the five restrictive abortion laws, only the Parental Involvement Law has a significantly (p < .01) negative association with the number of abortion providers in a state. There are significantly fewer abortion providers in states with parental involvement laws than in states without parental involvement laws. The numerical impact of a parental involvement law is to reduce the number of abortion providers per 100,000 pregnancies by between 12 and 15 as compared with states without parental involvement laws. This section suggests that parental involvement requirements for teen minors decrease the availability of abortion services to all women, not just teen minors.
Conclusion
This study, using state data, empirically examines the determinants of the number of abortion providers over the period 1992–2011. The labor force participation of women and the percentage of women of reproductive age in the 18–24 age group were significantly positively associated with the number of abortion providers in a state. The level of antiabortion activities and antiabortion attitudes in a state were significantly negatively associated with the number of abortion providers. Examination of the standardized regression coefficients found that the public’s antiabortion attitudes were the single largest determinant in reducing the number of abortion providers in a state. The empirical evidence also indicates that a state’s abortion rate is significantly positively associated with the number of abortion providers in a state. A decrease in a state’s abortion rate by 5% is associated with a decrease in the number of abortion providers per 100,000 pregnancies by 2.4%. This suggests that as the abortion rate falls, the number of abortion providers decrease at a decreasing rate.
Examination of five restrictive state abortion laws − No Medicaid Funding restrictions, parental involvement laws, mandatory counseling laws, two-visit laws, and TRAP laws − found that the enforcement of a parental involvement law deters physicians/organizations from becoming or remaining abortion providers, resulting in less access for women to abortion services. The numerical impact of a parental involvement law is to reduce the number of abortion providers per 100,000 pregnancies by between 12 and 15 as compared with states without parental involvement laws. The enforcement of parental involvement laws by states reduces the number of abortion providers willing to offer abortion services and make abortions more difficult to obtain for all women, not just teen minors. The enforcement of a parental involvement law by a state places a burden on all women by reducing their access to abortion and inhibits their reproductive choices.
The constitutional right of a woman to make the decision to have an abortion is moot if, because of a parental involvement law, there are too few abortion providers to perform the procedure.
Footnotes
Editors’ Note
The author, Professor Marshall H. Medoff, passed away while this article was under review by The American Economist. The editorial team had issued a conditional acceptance dependent upon several minor changes in style and presentation to meet the journal guidelines. With the permission of his son, Shane Medoff, these changes were made by the editorial team and the article is presented as the author originally intended.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.