
Abstract
Background:
Individuals with psychotic disorders face an elevated risk of suicide, yet current assessment tools often lack adaptations for this population's unique clinical realities. No standardized guidelines exist specifically for assessing suicide risk in psychosis, contributing to variability in clinical practice.
Methods:
A two-round Delphi survey was conducted with 42 professionals specializing in suicide prevention or psychotic disorders. Participants rated the relevance of 100 items related to suicide risk assessment and potential systemic facilitators. The top 35 items from the first round were retained for further prioritization in the second round. Descriptive statistics were used to analyze consensus levels.
Results:
Only eight out of 29 systemic factors received strong support, mostly related to the availability of practical tools and structural supports. Of the 71 risk assessment items, 35 surpassed the 4.25/5 relevance threshold. Highest consensus was found for items related to suicidal ideation and planning, such as intent, method, and access to means. Protective factors were also endorsed, while psychological/internal states (e.g., burdensomeness) were rated less relevant.
Discussion:
Findings underscore clinicians’ emphasis on immediate risk and practical tools over abstract internal states. Results advocate for developing standardized, population-specific assessment protocols that balance risk and protective factors in individuals with a psychotic disorder.
In Canada in 2023, more than 3,800 person died by suicide, 1 representing a rate of 11.8 suicides per 100,000 people. 2 Individuals with mental disorders are disproportionately affected by suicide risk.3–5 A meta-analysis 6 revealed that the likelihood of dying by suicide is approximately eight times higher among individuals with mental health conditions, especially those diagnosed with psychotic disorders, when compared to the general population. Research has identified a range of contributing factors including feeling like a burden to others, experiencing social isolation, and developing the psychological capacity to engage in suicidal behavior. 7 Additionally, both positive and negative psychotic symptoms,8–11 the presence of comorbid conditions,12,13 and a prior history of suicide attempts 14 are frequently cited as specific risk factors of people with psychotic disorders. While some factors are nonmodifiable (e.g., sex, childhood trauma, history of suicide attempts), they remain crucial to prevention efforts. They can help identify high-risk groups and inform tailored prevention strategies. 15 Despite the fact that suicide risk in individuals with psychotic disorders is well established, no studies specifically focusing on suicide risk assessment in this population were identified in the current review.
The process of assessing suicide risk in individuals with psychotic disorders requires special attention due to the unique characteristics of psychosis that can influence the evaluation. Negative experiences associated with psychiatric treatments or involuntary hospitalizations may deter individuals from disclosing suicidal thoughts, out of fear of similar consequences.16–18 Individuals with psychotic disorders often face intense stigma, which can become a barrier to care and safety. Stigma can encourage secrecy and isolation—for example, a community-based study found that among people labeled “mentally ill,” perceived stigma, alongside secrecy and hopelessness were direct contributors to suicidal ideation. 19 Moreover, deficits in metacognition, poor insight, and command hallucinations have also been documented as increasing suicidal risk in people with psychotic disorders.20–22
In some Canadian provinces, namely Quebec, suicide risk assessment training for the general population has been offered for more than a decade, 23 yet few participants report feeling fully confident in conducting these assessments. 24 Clinicians often use varied approaches based on personal judgment, underscoring the lack of a common standardized assessment. Among available tools are the Columbia-Suicide Severity Rating Scale (C-SSRS 25 ), the Modified Scale for Suicide Ideation (SSI-M 26 ), the Geriatric Suicide Ideation Scale (GSIS 27 ), and the Reasons for Living Inventory (RFL 28 ). Suicide risk assessments must consider a wide range of psychological, social, and historical factors—which become even more multifactored in the context of psychotic disorders. For instance, lack of sleep, substance misuse, and history of trauma can exacerbate psychotic symptoms, such as demeaning or command hallucinations, and increase suicidal ideation.14,29 Similarly, discrimination experiences and difficulties in attaining recovery goals (e.g., linked to work, independent living, and social connections) can also increase suicidal risk.19,30 There is no single cause that explains or predicts suicide, as suicidal thoughts and behaviors result from a complex interplay between multiple variables. 31 Consequently, professionals may find it difficult to determine which factors are most relevant in any given situation, due to the multitude of risk factors, the variety of existing assessment tools and individual differences. This uncertainty highlights the need for a systematic approach to guide clinicians working with people with psychotic disorders in their assessments and interventions.
The goal of this study is to gather expert opinions in the fields of suicide prevention in people with psychotic disorders regarding the key elements that should be included in a suicide risk assessment, with the aim of formulating recommendations toward a standardized assessment.
Method
Participants
A total of 42 professionals with expertise related to psychotic episodes or suicide prevention from various disciplines, such as nurses, psychologists, social workers, and psychiatrists were invited to answer a Delphi survey. Inclusion criteria were: (a) at least 18 years old, (b) have clinical or research expertise related to psychotic disorders or suicide prevention, and (c) understand French or English. In the context of this study, professionals were considered experts if they had at least 5 years of clinical or research experience in the relevant domains. This experience may pertain to suicide prevention, psychotic disorders or both. Recruitment was conducted through professional networks at an international level and existing contacts among professionals with recognized experience in suicide prevention and/or the care of individuals with psychotic disorders. Participants were also invited to share the study with colleagues who met the same criteria, using a snowball sampling approach to reach additional experts.
Procedure
The survey was distributed in a targeted manner, with experts in the concerned areas being contacted directly. Once the responses were collected, the results guided the development of questions for the second round. The survey was sent again to participants to identify which elements are considered most important. The entire survey process was conducted online via the secure Limesurvey platform. The first round of the survey took around 15 min to complete, and the second round about 10 min. The study was approved by the IRB: CIUSSS-de-l’Est-de-Montreal (Ethical Approval Reference Number: 2025-3855).
Measures
The full Delphi survey involved two rounds. Both rounds included sociodemographic questions, such as years of experience at work, workplace, and caseload. The first round consisted of 100 questions divided into two categories. The first category (29 questions) covered possible solutions to difficulties most frequently identified in the literature related to suicide risk assessment in the general population. Items in this section were separated in three subcategories: professional training and development, tools and available resources, and work condition and support. The second category (71 questions) addressed factors considered relevant to include in a suicide risk evaluation, such as previously mentioned risk factors and elements from current assessment tools such as the C-SSRS, the SSI-M, the RFL, the GSIS, the Patient Health Questionnaire (PHQ-9 32 ), the Nurses’ Global Assessment of Suicide Risk (NGASR 33 ), the Suicidal Behaviours Questionnaire-Revised (SBQ-R 34 ), and the guide from Intervenir auprès de la personne suicidaire à l’aide des bonnes pratiques (“Providing care to individuals at risk of suicide using evidence-based practice” 24 ). Factors were divided in four subcategories: Suicidal ideation and planning, protective factors, psychosocial risk factors, and psychological state and internal factor. Responses were collected using a 5-point Likert scale (1—would not influence me at all to 5—would influence me a lot for the first category and 1—not at all relevant to 5—very relevant for the second category). Each section ended with an open-ended question allowing respondents to add any unmentioned elements.
The second round consisted of 35 questions from the second category based on the results of the first round. Questions for the second round were selected based on the most relevant items identified in the first round. Items were separated according to their subcategories. Professionals were asked to categorize each item based on whether they considered it to be essential, important (but not essential), or less of a priority when conducting a suicide risk assessment. An open-ended question concluded the survey to gather further suggestions.
Analysis
Descriptive statistics were performed on the sociodemographic data. Averages were calculated for each item from the first round to identified which items were perceived more pertinent. Given the high endorsement of several items, items with a score of 4.25/5 or higher were selected for the second round. This threshold was chosen post-hoc to balance the need for a manageable number of items in Round 2, while ensuring to represent each predefined subcategory. Of the 71 items from the second category, 35 made it to the second round. Descriptive statistics (e.g., mean rank, median rank) were calculated for each item to summarize participants’ prioritization following the second round. Given the limited number of qualitative responses received, no proper analysis method was needed but a brief description of the responses is presented.
Results
Sociodemographic Information
A total of 42 professionals (57% women) participated in the study, with age ranging from 26 to 69 years old (M = 41.24, SD = 10.89). Psychologist and psychiatrist (38% and 24% respectively) accounted for most of the sample, followed by social workers (12%), nurses (5%), occupational therapist (5%), and other mental health professionals (16%). Most of our sample worked either in first-episode psychosis or an outpatient's clinics (26% each), followed by hospital setting (17%), any form of community health centers (5%), private clinics (5%), and others such as rehabilitation centers, university settings, or specific programs (21%). The median years of experience of professional working with people with a psychotic disorder (N = 38) was 9.5 years and 10 years (N = 26) for professional working in suicide prevention, with more than half of the sample (N = 24) saying that they work with both populations. Interestingly, while 92.9% of our sample received training on suicide assessment, only 16.7% received training on suicide assessment specifically for psychotic disorders. For the second round, 35 professionals participated in the survey, representing a participant retention rate of 83.3% from the first round.
Factors Influencing Systematic Assessment
Participants highlighted a range of factors that could facilitate more frequent suicide risk assessments with individuals living with a psychotic disorder. Only eight factors (on a total of 29) had an average score of 4 or higher. From the three original subcategories (Training and professional development, tools and available resources and work condition and support), items from the subcategory “Tools and available resources” were most frequently identified as potentially helpful for professionals. Participants emphasized the importance of having access to specific tools for assessing both protective and risk factors, specifically tailored to individuals with a psychotic disorder, as well as clear emergency protocols within their work settings. Several also underscored the value of having sufficient resources—such as time, staffing, and materials—to implement effective suicide prevention strategies. While training needs were also mentioned, including tailored education and ongoing professional development, it was the availability of practical tools and structural support that emerged as most critical. Finally, some participants expressed the importance of peer support networks to manage the emotional and clinical challenges associated with caring for suicidal patients. The few qualitative answer of this section also reveals the need for more resources in work settings and a consensus or clearer data on assessment tools available.
Relevant Items to Assess Suicide Risk According to Professionals
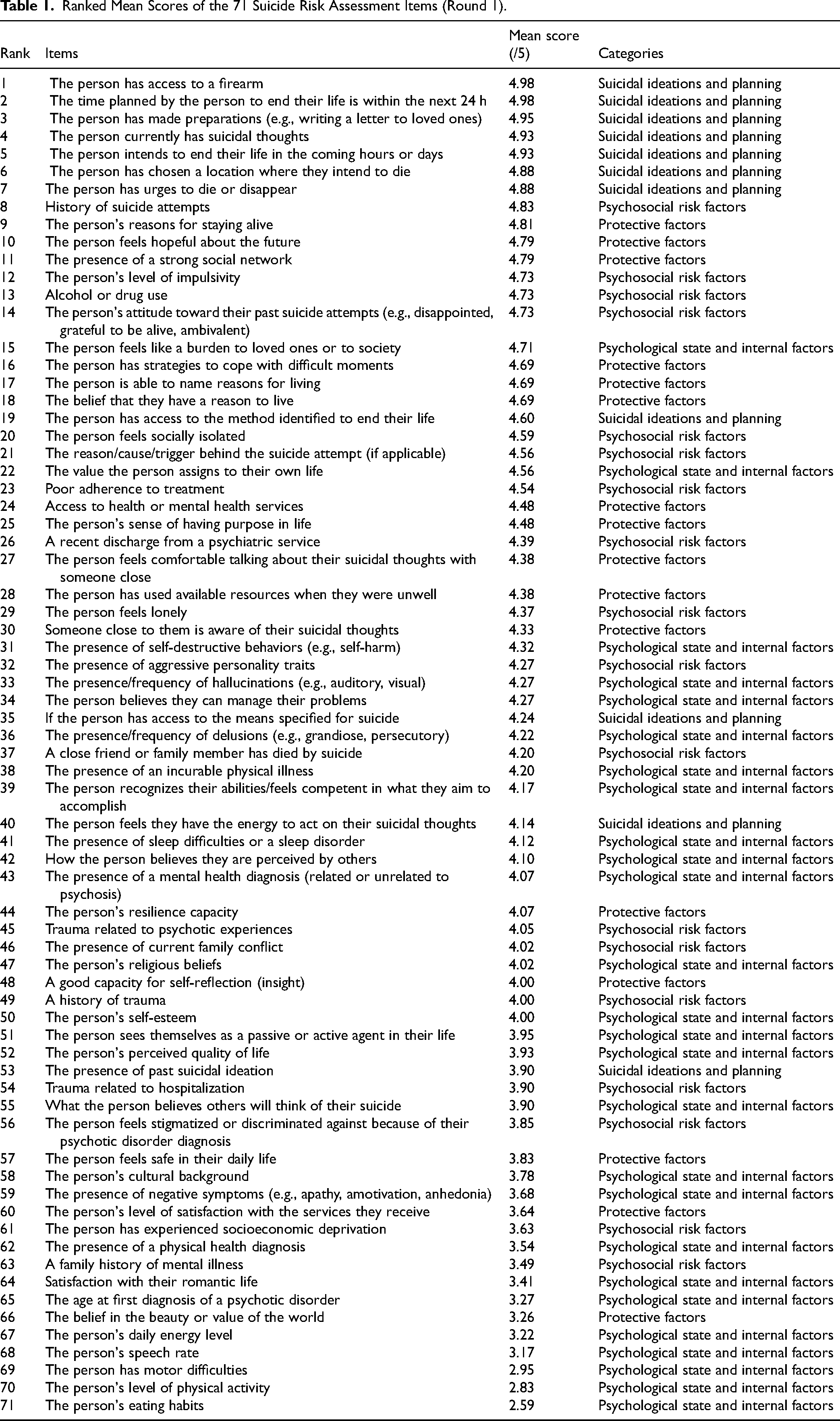
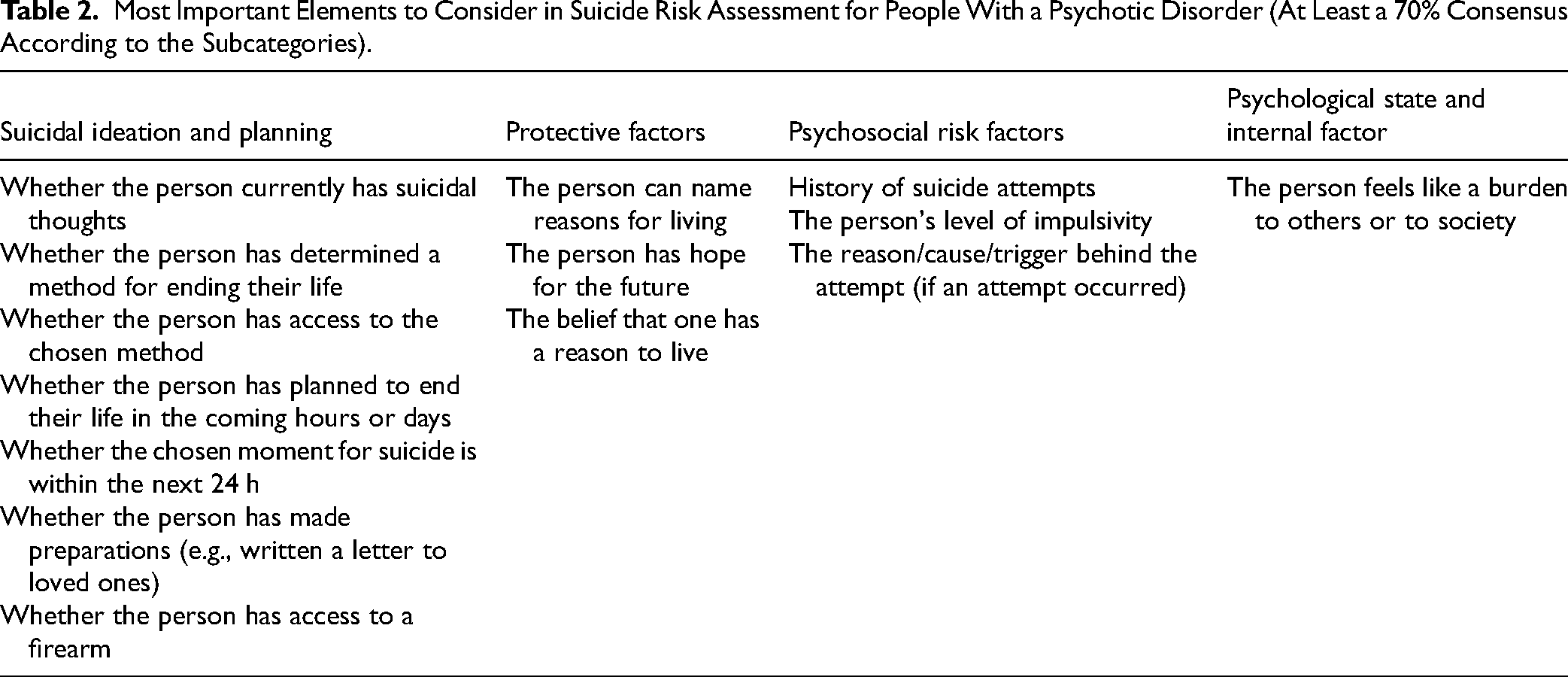
In the first round, 35 of 71 items reached a mean relevance ≥4.25 and were retained for Round 2. Items related to suicidal ideation and planning, and several protective and psychosocial risk factors, tended to receive the highest mean relevance scores. A complete ordered list of the 71 items is provided in Table 1. In Round 2, we observed strong consensus (≥80% rating “essential”) for items capturing acute planning and access to means; 11 items exceeded the 80% threshold and 14 exceeded 70% (Table 2).
Ranked Mean Scores of the 71 Suicide Risk Assessment Items (Round 1).
Most Important Elements to Consider in Suicide Risk Assessment for People With a Psychotic Disorder (At Least a 70% Consensus According to the Subcategories).
In the first round of the Delphi survey, professionals highlighted items that were most relevant to a suicide assessment (Table 1). A total of 35 out of 71 items had an average score of 4.25 or higher. Items corresponding to the subcategory Suicidal ideations and planning, such as questions about the presence of suicidal ideations, when, where, and how, and the availability of a firearm, were among the most identified items. Items corresponding to Protective factors were also among the most important items according to professionals. Some items from the Psychosocial risk factors were also frequently identified. Items from the Psychological state and internal factors subcategory were among the least relevant items according to professionals. The few qualitative answers of this section also revealed interest about the therapeutic alliance, the presence of command hallucinations, and the individual's plan following the appointment.
In the second round of the Delphi survey, several items achieved strong consensus among experts. Notably, 100% of participants rated the item “The person has planned to end their life in the next hours or days” as essential. In total, 11 items exceeded the 80% threshold and 14 surpassed 70%, with the highest concentration of consensus found in the subcategory of suicidal ideation and planning. See Table 2. In contrast, seven items were rated as essential by fewer than 50% of participants, items that are mostly form the Psychological state and internal factors subcategory.
Discussion
This study aimed to gather expert's opinions in the fields of suicide prevention and psychotic disorders regarding the key elements that should be included in a suicide risk assessment, with the aim of formulating recommendations toward a standardized assessment. The findings first highlight a strong emphasis on the need for practical tools and structural supports over more general training interventions. Among the three categories explored—training and professional development, tools and available resources, and work conditions and support—items related to tools and resources were most consistently endorsed as helpful by professionals, in part highlighting the need for a consensus on suicide assessment tool. This finding parallels what is found in the literature, with professionals reporting the lack of resources and the poor reliability and predictability of available tools as obstacles to conducting suicide assessment.35–37 This also aligns with prior work suggesting that having access to validated tools and structured protocols can enhance clinicians’ confidence and consistency in assessing suicide risk.38–40 Professional's needs in this study also included specific instruments tailored to individuals with a psychotic disorder, that could evaluate risk and protective factors and propose clear emergency protocols. People with psychotic disorders present with specific challenges and clinical presentations that support the need to adapt existing suicide risk assessments for this population. Professionals also expressed a desire for peer support networks, which may mitigate emotional strain and burnout when working with high-risk clients, a theme well-documented in literature on clinician well-being.41,42
In terms of item relevance within suicide risk assessments, our findings reveal that clinicians prioritize direct indicators of risk (current suicidal ideation, detailed planning, access to lethal means). This aligns with standard clinical guidelines and existing frameworks that focus on intent, plan specificity, and means availability as critical indicators.7,43 It also aligns with similar DELPHI studies in other populations, where direct indicators of risk and safety are prioritized.44,45 These results are also consistent with the notion that suicide risk assessments are typically conducted to evaluate an individual's current level of risk at the time of the clinical encounter. Protective factors were also highly endorsed, particularly those related to psychological resilience (e.g., hope for the future, reasons for living), social connection and a strong therapeutic alliance, which are well-established as safeguards against suicidal behavior.46–48 There is a growing recognition in the literature that suicide assessment should balance risk and protective factors. 49 Prioritizing these factors in assessment has practical implications: it suggests clinicians are attentive to dynamic, modifiable elements rather than only static history. This is consistent with the design of evidence-based interventions like the Safety Planning Intervention and the Providing Care to Individuals at Risk of Suicide approach, where patients collaboratively generate coping strategies to use after a crisis.24,49 In line with this, the survey's emphasis on ideation/planning items and protective resources suggests a risk management approach: gather detailed information on immediate suicide intent and bolster support/coping, which is exactly the focus of modern suicide care planning.
However, the relative neglect of internal psychological factors in our survey is notable and raises questions about potential underestimation of their importance in some clinical settings. Those results contrast with the growing literature on the importance of subjective suffering, such as mental pain 50 evidence linking factors such as low self-worth, burdensomeness, and command hallucinations to suicide risk in psychosis,22,30,51,52 these were less frequently endorsed. One possible reason is that constructs like burdensomeness are less concrete and may not be part of standard training, whereas factors like past attempts or substance misuse are unequivocally considered “high risk” 53 and easier to evaluate. With individual with a psychotic disorder, diagnostic overshadowing and the possible presence of psychotic symptoms may shift attention away from internal factors. Moreover, clinicians may assume that by addressing suicidal ideation and social support, it implicitly covers issues of meaning and connectedness. Alternatively, it could reflect clinical pragmatism: when time is limited, which is often reported by professionals, 37 clinicians focus on what is immediately observable and therefor more practical in clinical decision-making current thoughts, behaviors, support network).
Limitations and Future Directions
One important limitation of this study concerns the sample. Although the Delphi method often relies on smaller expert panels, the sample size (N = 42) remains relatively limited and may not fully capture the diversity of professional perspectives on suicide risk assessment in individuals with psychotic disorders, which limits representativeness. Moreover, the use of snowball sampling through professional networks may have introduced sampling bias by over-representing individuals who share similar clinical environments, theoretical orientations and perspectives, or levels of engagement in suicide prevention. As participation was voluntary, the sample may also reflect the views of professionals who are particularly interested or invested in the topic, which limits the generalizability of the findings. The self-reported data introduces the possibility of a socially desirable bias, as participants may have been inclined to endorse items perceived as professionally appropriate or aligned with current best practices. Additionally, the use of a 4.25/5 cut-off score to determine which items were retained for the second round, while ensuring representation across categories, was determined post hoc and may have excluded items of potential clinical value that were rated as moderately important.
Conclusion
This study highlights the priorities of professionals when assessing suicide risk working with individuals with a psychotic disorder. Items related to suicidal ideation and protective factors were identified as most relevant, while items related to internal psychological factors were deemed less important. This highlights a priority of professionals to assess the immediate risk and safety of clients over assessing the “bigger picture” of the person's reality. Future research should mix the point of view of clients and professionals to implement changes in the way suicide risk assessment is conducted.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437261425026 - Supplemental material for Toward a Standardized Suicide Risk Assessment in Psychotic Disorders: A Delphi Study With Mental Health Experts: Vers une évaluation standardisée du risque de suicide chez les personnes atteintes de troubles psychotiques : étude Delphi auprès d’experts en santé mentale
Supplemental material, sj-docx-1-cpa-10.1177_07067437261425026 for Toward a Standardized Suicide Risk Assessment in Psychotic Disorders: A Delphi Study With Mental Health Experts: Vers une évaluation standardisée du risque de suicide chez les personnes atteintes de troubles psychotiques : étude Delphi auprès d’experts en santé mentale by Félix Diotte, Christine Genest, Hugo Thomas and Tania Lecomte in The Canadian Journal of Psychiatry
Footnotes
Acknowledgments
The authors would like to thank all the professionals who generously shared their time and expertise by participating in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.