
Abstract
Background
Limited evidence guides fitness-to-drive decision-making following an episode of acute psychosis.
Method
We used population-based administrative health and driving data from British Columbia, Canada, to identify all police-attended motor vehicle crashes between 2000 and 2016. Drivers were considered exposed if a hospitalization for acute psychosis ended in the 6-week interval prior to the crash. We assessed the association between psychosis and crashes using a case-crossover design that controls for relatively fixed individual characteristics like personality and routine driving habits. We also conducted a responsibility analysis that accounted for changes in road exposure (kilometres of driving per month) that might occur soon after hospital discharge. Outcomes included involvement in a crash as a driver (for the case-crossover analysis) and driver responsibility for contributing to their crash (for the responsibility analysis). We used logistic regression to evaluate associations between these outcomes and recent hospitalization for acute psychosis, with adjustment for potential confounders.
Results
Among 9,842 crashes in the case-crossover analysis, a hospital stay for acute psychosis ended in 199 pre-crash intervals and in 147 control intervals, suggesting acute psychosis was temporally associated with subsequent crash (2.0% vs. 1.5% of intervals; adjusted odds ratio (aOR), 1.32; 95% CI [1.05–1.66]; P = 0.02). Among 819,348 drivers with a police-attended crash and determinate crash responsibility, 178 of 235 drivers with a recent hospitalization for acute psychosis and 440,543 of 819,113 drivers without recent psychosis were deemed responsible for their crash (75.7% vs. 53.8%; aOR, 2.38; 95% CI [1.75–3.24]; P < 0.001).
Conclusions
The 6-week interval following a hospitalization for acute psychosis is associated with increased odds of crash and increased likelihood of driver responsibility for contributing to their crash. More stringent temporary driving restrictions after an episode of acute psychosis might reduce crash risk.
Plain Language Summary Title
Are drivers at a higher risk of crash after recent hospitalization for acute psychosis?
Plain Language Summary
Acute psychosis can affect how people think and make choices. This can make driving unsafe. But there is little information about when it is safe to drive again after being admitted to the hospital for acute psychosis. In this study, researchers wanted to know if drivers who were recently in the hospital for acute psychosis had more car crashes. To do this, they looked at 20 years of health records and driving data from British Columbia, Canada. The researchers found that crashes happened more often than expected in the first six weeks after leaving the hospital. These drivers were also much more likely to be considered 'responsible' for contributing to their crash than drivers who had not been in the hospital for psychosis. These results show that the time immediately after hospitalization for acute psychosis comes with higher crash risk. Checking if someone is ready to drive and restricting driving for a short period of time after acute psychosis may help reduce crashes and keep roads safer.
Key Points
Introduction
Acute psychosis is a disorienting mental state that often requires hospitalization and typically improves after several weeks of psychiatric treatment.1,2 Psychosis can impair the perception and judgment required to safely operate a motor vehicle, but extremely limited prior evidence specifically examines this issue. An uncontrolled case series of 94 drivers with a psychotic disorder who were killed in vehicle collisions in Finland (1990–2011) found that half were hospitalized for psychosis in the 3 months prior to death. 3 We recently published a population-based study which found that 2,551 crash-involved drivers with schizophrenia were modestly more likely than 805,881 crash-involved drivers without schizophrenia to be deemed responsible for their crash (66.2% vs. 53.7%, respectively; aOR, 1.67; 95% CI [1.53–1.82]), but the effect of acute psychosis on crash risk and crash responsibility was not specifically examined. 4 Most other prior studies of mental illness and crash risk enrolled few patients,5–7 are several decades old,5–8 focus on a heterogenous mix of chronic mental illnesses,5,8,9 and fail to examine acute psychosis as a distinct risk factor for crash.5–10 As a result, vanishingly little empirical evidence informs clinical fitness-to-drive decision-making for patients recovering from an episode of acute psychosis.3,10–12 The lack of evidence contributes to considerable variation in reporting requirements across Canada, with some provinces (e.g., Ontario) indicating that a diagnosis of acute psychosis should trigger mandatory physician reporting and automatic licence suspension, while others (e.g., British Columbia) emphasize that most physician reporting is discretionary and that licence suspension should focus on functional driving ability rather than diagnosis.13–15
Acute psychosis typically occurs among individuals with chronic conditions that can independently influence driving safety, including schizophrenia spectrum disorders, mood disorders and substance use disorders. 4 Individuals experiencing acute psychosis may also substantially increase or decrease their road exposure (the hours or kilometres of driving per month) relative to their baseline.12,16 Cohort studies on this topic are highly likely to produce biased or misleading results because (1) available data may not capture fundamental baseline differences between drivers with psychosis and control drivers without psychosis, and (2) temporary changes in road exposure during convalescence from acute psychosis might produce a “crash risk per year” that obscures a clinically meaningful change in “crash risk while driving.”17,18
Other study designs avoid these shortcomings. Case-crossover studies use self-matching to compare an individual's exposure status in the period immediately before a crash to their exposure status in earlier control periods, thereby avoiding bias arising from the selection of control patients and eliminating confounding from relatively fixed individual characteristics such as genetics, personality, occupation, driver training, driving experience, and daily travel routines (Supplemental Appendix, eFigure 1).19–23 Responsibility analyses use police-reported crash data to categorize crash-involved drivers as cases (deemed “responsible” for their crash) or controls (deemed “non-responsible” for their crash), comparing the prevalence of a potential risk factor between these groups (eFigure 1).24–27 Because all individuals are driving when they crash, responsibility analyses inherently account for between-group differences in road exposure.21,28
We hypothesized that acute psychosis produces a transient elevation in crash risk that persists for several weeks after hospital discharge. Evidence of heightened crash risk might prompt psychiatrists to advise patients to avoid driving during this interval. We examined this hypothesis using a self-matched case-crossover study (to address confounding that might arise from the selection of control patients) and a responsibility analysis (to address bias arising from unmeasured differences in road exposure between drivers recently hospitalized for psychosis and controls).
Methods
Data Sources
We set our study in British Columbia (BC), Canada (2016 population: 4.6 million). 29 De-identified individual-level data were obtained from population-based administrative health and driving databases (eMethods 1).4,18,20,25,28,30 We obtained data for all police-attended crashes in BC from the Traffic Accident System. Police in BC are required to attend all fatal crashes, most serious injury crashes, and some crashes with property damage only. The attending officer completes a structured crash report that identifies each crash-involved driver and records detailed information on the circumstances of the crash. We obtained driver data including licence type and traffic contravention history. We used hospitalization and physician billing data to identify medical comorbidities and recent health services use. Medication use was established using data on dispensation date and days supplied for all outpatient prescriptions filled at any community pharmacy in BC.
Study Population
The study population included all individuals involved as a driver in a police-attended crash that occurred in BC between 1 January 2000 and 31 December 2016. We excluded individuals if they did not hold a BC driver licence or if driving data could not be linked to health data. By anchoring on involvement as a driver in a police-attended crash, all study analyses pragmatically focus on the clinically relevant group of individuals who are active drivers at risk of crash. Each anchoring eligible police-attended crash is hereafter termed an ‘index crash’.
Exposure: Recent Episode of Acute Psychosis
The exposure of interest for both analyses was a recent hospitalization for acute psychosis with a discharge date in the 6-week interval immediately prior to the index crash. Hospitalizations with a primary (“most responsible”) diagnosis of acute psychosis were identified using International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Canada (ICD-10-CA) diagnostic codes (eTable 1). This included hospitalizations for psychosis arising from schizophrenia spectrum disorders, mood disorders with psychotic features, substance-induced psychosis, delusional disorders, brief psychotic disorder and other nonorganic psychotic disorders. 31 We focused on the first 6 weeks after hospital discharge because individuals may continue to experience residual distortions in perception and judgement after discharge, and because hospitalization itself presents a clear opportunity for the provision of driving advice.3,18,28
Analysis 1: Case-Crossover Analysis
The cohort for the case-crossover analysis included all crash-involved drivers from the study population who had ≥1 police-attended crash as a driver between 1 April 2000 and 31 December 2016 plus ≥1 hospitalization for acute psychosis between 1 January 1997 and 31 December 2016 (eFigure 1). The outcome of interest was police-attended crash. For each index crash, we used the crash date (t0) to establish a seasonally matched “no crash” control date exactly 52 weeks earlier (t0−52wk). Exposure lookback intervals were the 6-week periods before the crash date (“pre-crash interval”) and the control date (“control interval”). Case-crossover designs require control intervals to be free of the outcome, so we prespecified that crashes were only eligible if there was no additional crash in the 37.5 months prior to the index crash (to ensure the same cohort could accommodate the main analysis and a sensitivity analysis with a t0−3y control date). Drivers were required to have an active licence in all pre-crash and control intervals. Drivers could contribute multiple eligible crashes to the analysis.
We used conditional logistic regression to compare the likelihood of a psychosis hospitalization discharge date (exposure; 1 = yes, 0 = no) occurring in the pre-crash interval to the likelihood of a psychosis hospitalization discharge date occurring in the control interval, as for a conventional case-control study. We adjusted for potential time-varying confounders assessed on both crash and control dates: residential neighbourhood income quintile, residential urbanicity, and number of active prescription medications. We also adjusted for other potential time-varying confounders using a 90-day lookback interval from each crash and control date: number of impairment-related traffic contraventions, number of non-impairment-related traffic contraventions, number of hospital admissions, and number of physician visits or hospitalizations for “alcohol use” and “other substance use” (eFigure 2, eTable 2).
Analysis 2: Responsibility Analysis
The cohort for the responsibility analysis included all crash-involved drivers from the study population who had ≥1 police-attended crash as a driver between 1 January 2000 and 31 December 2016. The outcome of interest was driver responsibility for the crash (eFigure 1). We categorized crash-involved drivers as “responsible” or “non-responsible” for their crash using a validated crash responsibility scoring tool that considers unsafe driving action by the index driver plus six external factors that potentially contribute to a crash: road type, driving conditions, vehicle condition, contribution from other parties, type of collision, and task involved. 24 When several external factors contribute to a crash (score ≥16), the responsibility tool concludes that the driver could not have reasonably avoided the crash and the driver is deemed “non-responsible” for the crash. Unsafe driving by the index driver or absence of external contributing factors (score ≤13) suggests that the driver should have been able to avoid the crash; the driver is deemed “responsible” for contributing to the crash. Drivers with “indeterminate crash responsibility” (score 14 or 15) are excluded from further analysis. In this context, crash responsibility is independent of determinations of criminal, civil, or insurance-based responsibility for the crash.
We used logistic regression to examine the association between crash responsibility (outcome; 1 = “responsible,” 0 = “non-responsible”) and a recent hospitalization for acute psychosis (exposure; 1 = yes, 0 = no). Our final model adjusted for potential confounders and sources of variability: driver age group and sex; characteristics of the driver's residential neighborhood including urbanicity, median household income quintile, and regional health authority; hospitalizations or physician visits for substance use in a 3-year lookback; Charlson Comorbidity Index ≥2; driver licence type (none, learner, novice, or full); number of years with a full licence; number of crashes in a 3-year lookback; number of impairment-related traffic contraventions in a 3-year lookback; number of non-impairment-related traffic contraventions in a 3-year lookback; crash severity (fatality vs. injury vs. property damage only), location (highway vs. rural road vs. city streets), and timing (night vs. day); documented impairment by alcohol or drugs at the time of crash (yes vs. no); and season and calendar year of crash
Additional Analyses
We performed prespecified exploratory subgroup and sensitivity analyses for both study designs. For the case-crossover study, we examined subgroups based on age (≤44 vs. >44 years), sex (male vs. female), history of alcohol and/or drug misuse (yes vs. no), and impairment by alcohol or drugs at the time of the crash (yes vs. no). We also performed case-crossover sensitivity analyses, varying the exposure lookback interval length (examining 2, 4, 8, and 12 weeks), examining additional control dates (1 and 2 years prior to crash; 1, 2, and 3 years prior to crash), and examining subsets of the outcome based on crash consequences (crashes resulting in injury or fatality vs. crashes resulting in property damage only). For the responsibility analysis, we examined subgroups defined by age (<30 vs. 30–64 vs. ≥65 years; we prespecified different age categories than for the case-crossover study because we anticipated a much larger sample size), sex (male vs. female), and history of alcohol and/or drug misuse (yes vs. no). We performed responsibility sensitivity analyses, varying the exposure lookback interval length (examining 2, 4, 8, and 12 weeks) and examining subsets of the exposure (based on the etiology of psychosis) and subsets of the outcome (crashes resulting in injury or fatality vs. crashes resulting in property damage only). We also calculated the “absolute annual crash rate” and the “responsible crash rate” (proportion of drivers responsible for their crash) for crash-involved drivers with and without a hospitalization for psychosis.
Research Process
The University of British Columbia Clinical Research Ethics Board approved the study and waived the requirement for individual consent (H12-02678). We did not involve patients or the public in the design, conduct, reporting, or dissemination of our research. Data were deidentified before release to investigators. All inferences, opinions, and conclusions drawn are those of the authors and do not reflect the opinions or policies of the Data Stewards.
Results
Analysis 1: Case-Crossover Analysis
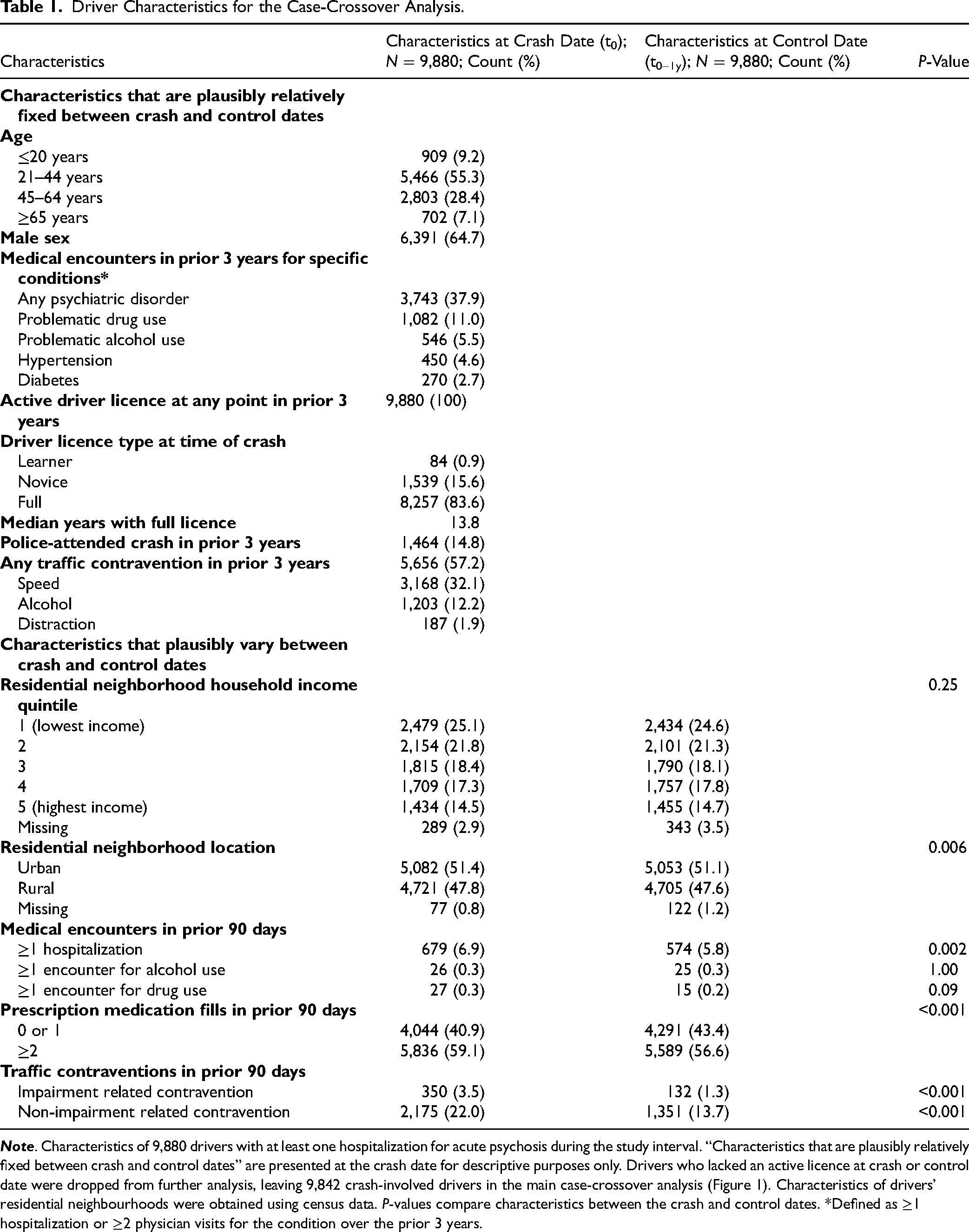
The case-crossover cohort included 9,880 crashes among drivers with ≥1 hospitalization for acute psychosis (Figure 1). Two-thirds of the cohort were male; median age was 38 years (Table 1). Almost half of the crashes resulted in an injury, 60 (0.6%) resulted in a fatality, and almost two-thirds involved multiple vehicles, highlighting that crashes often have serious consequences for other road users (eTable 3). A total of 38 crashes were dropped from further analysis because the driver lacked an active driver licence at either the crash or control date.
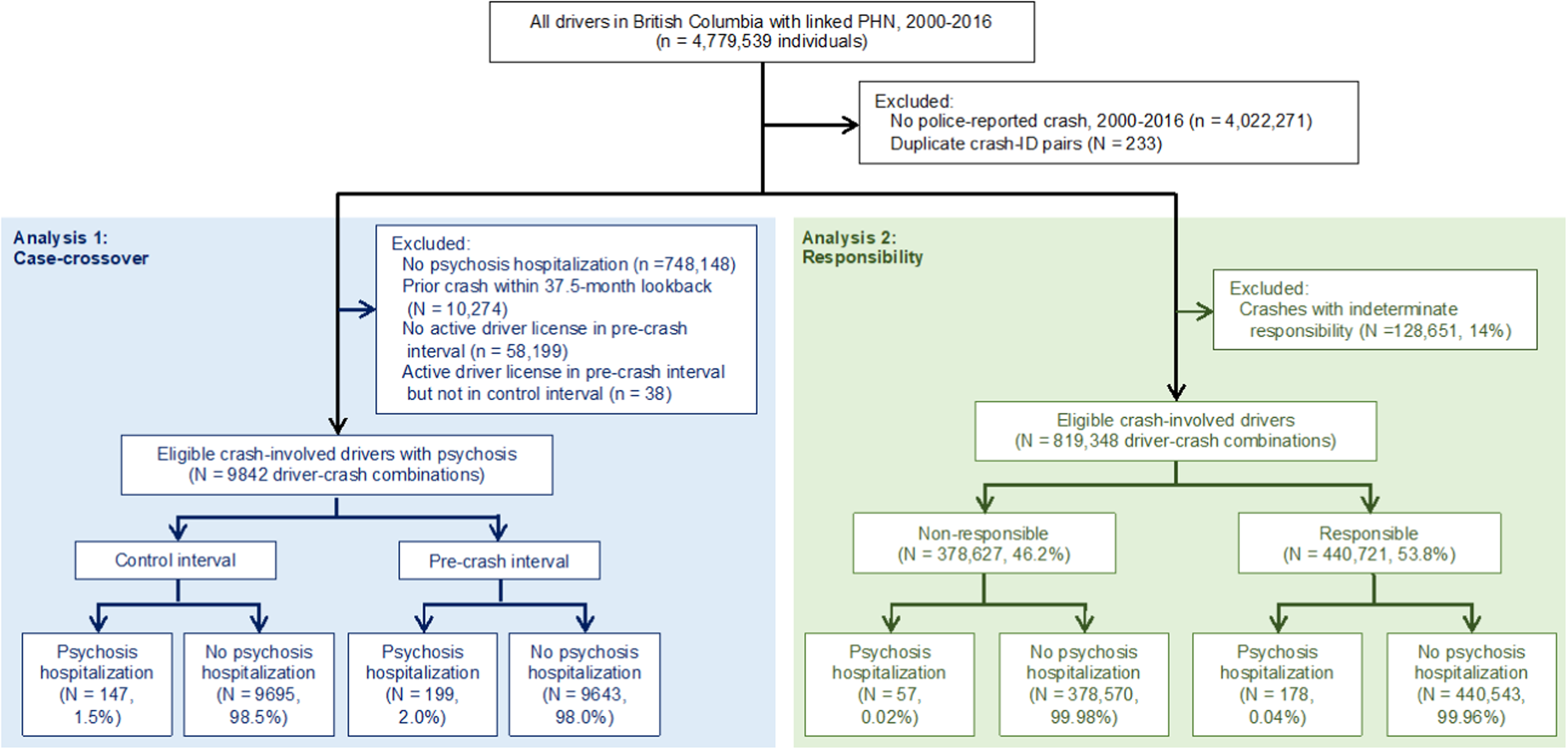
Flow diagram. PHN = personal health number; n = individuals; N = unique driver-crash combinations.
Driver Characteristics for the Case-Crossover Analysis.
In the remaining 9,842 crashes, discharge from an acute psychosis hospitalization occurred in 199 pre-crash intervals and in 147 control intervals, suggesting that acute psychosis was associated with a significant increase in subsequent crash risk (2.0% vs. 1.5% of intervals; adjusted odds ratio [aOR], 1.32, 95% CI [1.05–1.66], P = 0.02; Figure 2, eTable 4). Results from prespecified subgroup and sensitivity analyses were consistent with the main results (eTable 5). The point estimate for the association between crash and recent hospitalization for psychosis was slightly numerically higher with shorter exposure lookback interval lengths (i.e., for a 2-week lookback, aOR 1.48, 95% CI [1.06–2.07], P = 0.02). While we would expect a causal relationship to produce a similar pattern, the substantial overlap between effect estimate confidence intervals for all tested alternate exposure interval lengths indicates that no strong causal conclusions can be drawn from this sensitivity analysis alone.
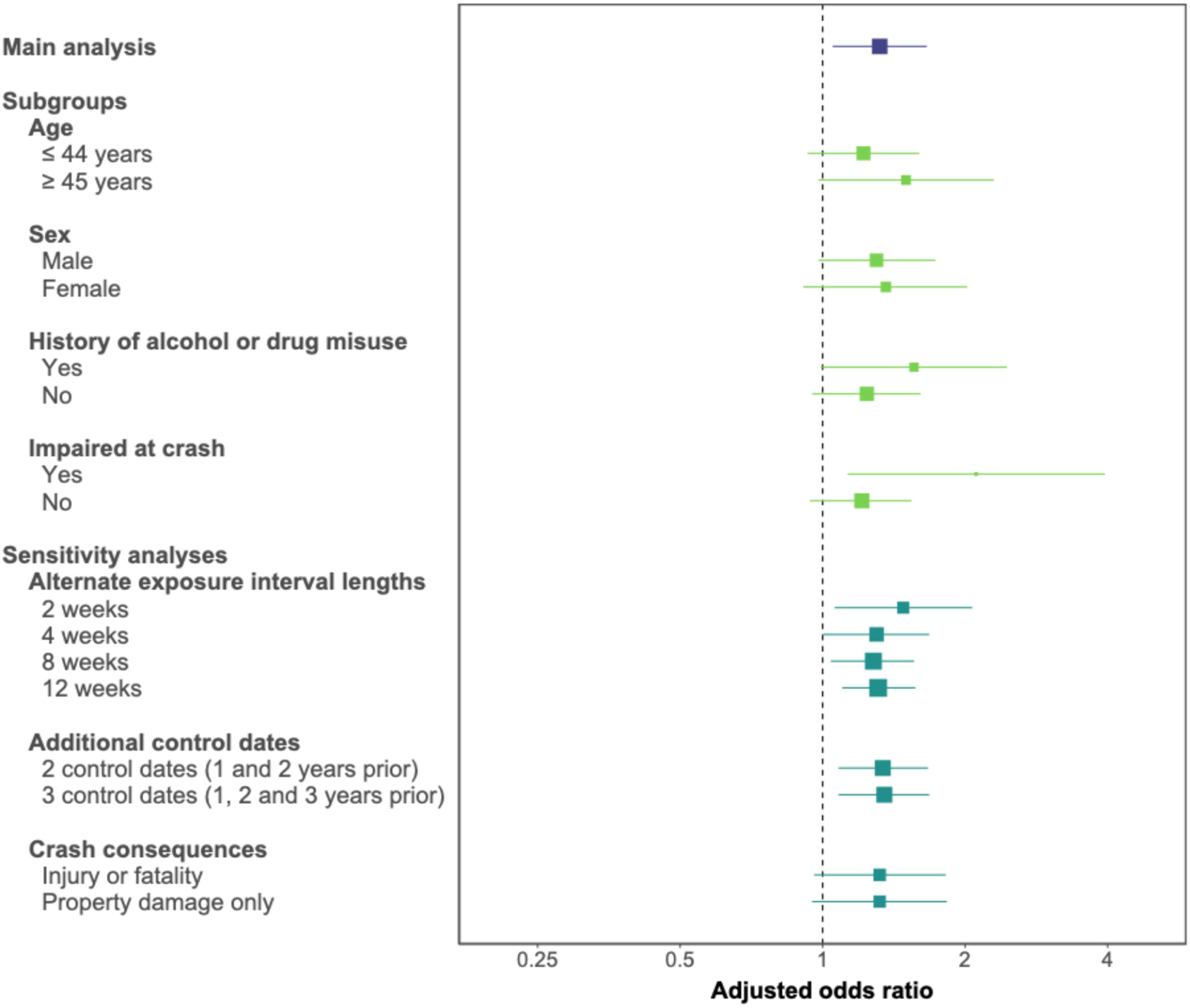
Forest plot of main, subgroup and sensitivity analyses for the case-crossover study. X-axis depicts the adjusted odds ratio on the log scale; squares, the point estimate, with size reflecting the inverse of the standard error; horizontal lines, the 95% confidence interval.
Analysis 2: Responsibility Analysis
Among the 947,999 drivers involved in a police-attended crash eligible for the responsibility analysis, 440,721 (46.5%) drivers were deemed responsible and 378,627 (39.9%) were deemed non-responsible for their crash; 128,651 (13.6%) had indeterminate responsibility and were excluded from further analysis (Figure 1). Crash-involved drivers had a median age of 39 years and 58% were male (Table 2).
Driver Characteristics for the Responsibility Analysis.
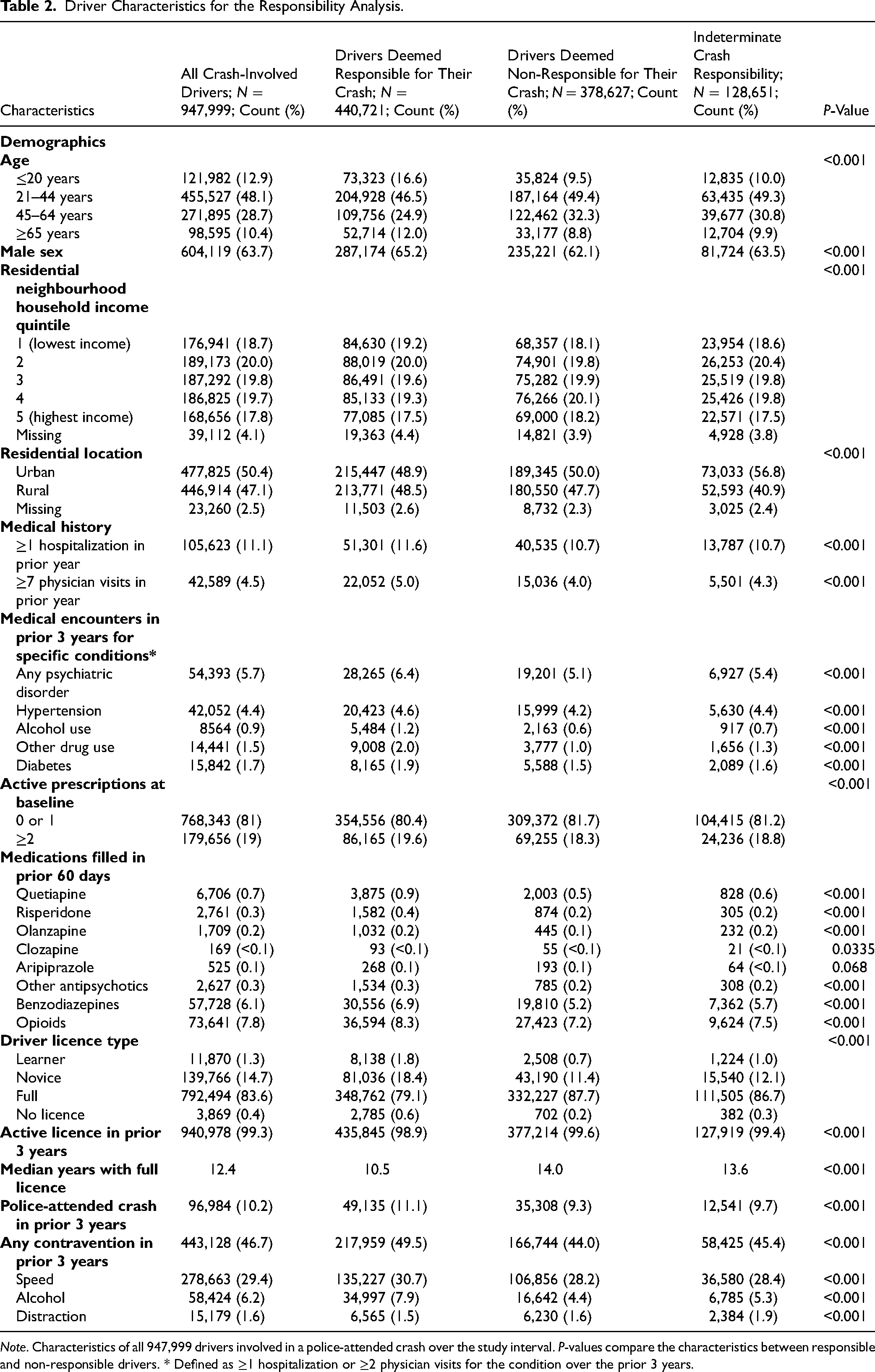
Note. Characteristics of all 947,999 drivers involved in a police-attended crash over the study interval. P-values compare the characteristics between responsible and non-responsible drivers. * Defined as ≥1 hospitalization or ≥2 physician visits for the condition over the prior 3 years.
Drivers deemed responsible for their crash were more likely to have established risk factors for crash that do not influence responsibility scores, supporting the validity of responsibility analysis (e.g., more likely to be younger, to be male, and to hold a learner or novice driver licence; Table 2). Police were also much more likely to report suspected impairment by alcohol or drugs at the index crash (unadjusted prevalence, 11.0% vs. 2.2% among non-responsible drivers; uOR, 5.58; 95% CI [5.45–5.71]; P < 0.001; eTable 6).
In total, 178 of 235 drivers with a recent hospitalization for acute psychosis and 440,543 of 819,113 drivers without recent psychosis were deemed responsible for their crash, corresponding to a significant association between recent acute psychosis and crash responsibility (75.7% vs. 53.8% deemed responsible; aOR, 2.38; 95% CI [1.75–3.24]; P < .001; eTable 7).
Results from prespecified subgroup and sensitivity analyses were generally consistent with the main results (eTable 8, Figure 3). Point estimates for the adjusted odds ratios describing the association between crash responsibility and recent hospitalization for psychosis were numerically larger for crashes resulting in injury or fatality (aOR, 2.89; 95% CI [1.85–4.52]; P < .001), when psychosis was attributed to schizophrenia (aOR, 6.20; 95% CI [2.16–17.77]; P < .001), and when exposure lookback intervals were shorter (e.g., with a 2-week exposure lookback from crash, aOR, 3.12; 95% CI [1.95–4.99]; P < .001). These findings are intriguing but imprecise, and the fact that the effect estimate confidence intervals substantially overlap with those of other subgroups and sensitivity analyses indicate that few strong conclusions can be drawn from these observations alone.
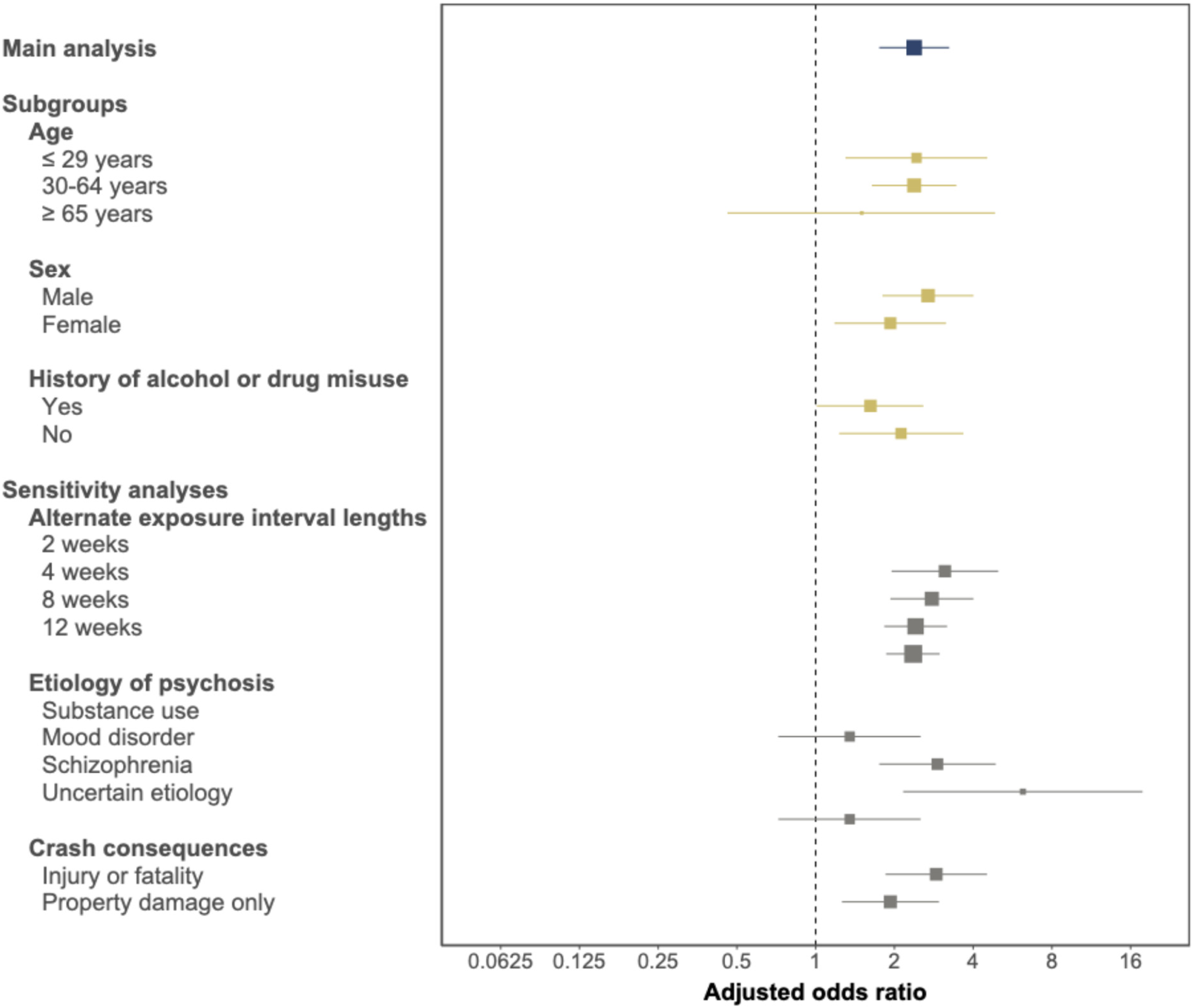
Forest plot of the main, subgroup and sensitivity analyses for the responsibility study. X-axis depicts the adjusted odds ratio on a log scale; squares, the point estimate, with size reflecting the inverse of the standard error; horizontal lines, the 95% confidence interval.
Drivers with psychosis exhibited a lower absolute annual crash risk but a higher responsible crash rate relative to controls, strongly suggesting they have reduced road exposure relative to controls and highlighting a key advantage of responsibility analysis (eTable 9).
Discussion
In a population-based cohort of drivers involved in police-attended crashes over a 17-year study interval, we found an association between recent hospitalization for acute psychosis and subsequent motor vehicle crash. A self-matched case-crossover study of 9,842 crash-involved drivers found that a recent hospital stay for acute psychosis was temporally associated with a 1.3-fold increase in the odds of crash. A responsibility analysis examining 819,348 crash-involved drivers found those with a recent hospital stay for acute psychosis had a 2.4-fold increase in the odds of being deemed responsible for their crash. The consistent association across multiple study designs supports the notion that acute psychosis causes a transient increase in crash risk that typically has not returned to baseline by the time of hospital discharge. 32 Notably, most studies indicate that antipsychotic medications have a neutral or beneficial effect on crash risk among individuals with psychotic conditions, suggesting it is the psychosis itself (rather than treatment with anti-psychotic medications) that causes the transient increase in crash risk.32–34 Taken together, these findings suggest that efforts to reduce traffic injury after an episode of acute psychosis are warranted.
Two additional aspects of our findings merit particular consideration. First, hospitalization for psychosis was rare: only 235 of 819,348 drivers with determinate responsibility (0.03%) had a hospitalization for acute psychosis ending in the 6 weeks prior to crash. While steps to reduce traffic injury after an episode of psychosis are warranted, a meaningful reduction in the overall burden of traffic injury among individuals with psychotic disorders will require a broader suite of interventions that target more common crash risk factors such as speeding, alcohol-impaired driving, distracted driving, and failure to use seatbelts. 35 Second, acute psychosis appears to increase crash risk, but context is important. The association between recent hospitalization for psychosis and subsequent crash was similar in magnitude to the association between a recent ticket for speeding or distracted driving and subsequent crash (aOR 1.3 vs. 1.3); the association between recent hospitalization for psychosis and driver responsibility for subsequent crash was similar in magnitude to the associations between age ≥65 years or possession of a learner licence and subsequent crash (aORs 2.0, 2.4, and 2.4, respectively). It would generally be considered disproportionate and unfair for a 65th birthday to prompt an automatic licence suspension; similar considerations for fairness and proportionality should apply to individuals recovering from an episode of psychosis, in whom severe restrictions may unnecessarily intensify social and occupational marginalization. 36 For context, non-zero blood alcohol concentrations <0.05% are thought to double crash risk but are not subject to any penalty in many jurisdictions. 37
Our study has many strengths. We focused on road safety in the clinically relevant group of individuals who continue to drive after an episode of psychosis. We used population-based data for a large cohort of crash-involved drivers, yielding highly generalizable results. Use of empirical crash data minimized outcome misascertainment, avoiding biases arising from crash self-reporting and circumventing concerns about the uncertain applicability of driving simulators to real-world road safety. We used population-wide hospital records to identify psychosis hospitalizations, limiting exposure misascertainment. The case-crossover analysis perfectly controlled for relatively fixed individual characteristics (such as driving experience and routine driving behaviours) and adjusted for important time-varying confounders (such as problematic alcohol and drug use resulting in health encounters). The responsibility analysis fully accounted for road exposure, thus mitigating a major bias of existing studies of driving safety among individuals with psychotic disorders. Analysis of alternate exposure intervals strengthened causal inference, and multiple sensitivity analyses suggested results were robust to changes in study design.
Our study has limitations. Analyses were restricted to drivers involved in a police-attended crash. Results may not apply to individuals who never drive or to those involved in less serious crashes. We identified psychosis requiring hospitalization using comprehensive population-based hospital records, but we could not identify less severe psychosis that did not receive medical attention or that was treated as an outpatient. 1 Psychosis hospitalization in the control interval might influence the likelihood of subsequent psychosis hospitalization in the pre-crash interval, potentially biasing our results. We lacked granular data on road exposure. The case-crossover study might find a spurious positive association if individuals drove greater distances in the first few weeks after acute psychosis, but we think it is more likely that psychosis reduces road exposure and that our case-crossover results instead underestimate the association between acute psychosis and crash risk.5–9,12,16 Our case-crossover study might underestimate crash risk after hospitalization for acute psychosis because patients with the most severe symptoms are the most likely to be subjected to limitations on vehicle access imposed by family members, warnings from physicians not to drive, and licence suspensions imposed by driver licensing authorities. The specific driving advice provided to each study subject and the degree of adherence to recommendations remain unknown. We lacked granular clinical data on alcohol and drug use, mental health history, and socioeconomic status. Results may be subject to residual confounding. We focused on private (i.e., non-commercial) drivers and our findings do not apply to professional drivers who have vastly greater road exposure and more severe crash consequences if driving large vehicles or those with many passengers.
Using case-crossover and responsibility analyses to examine all eligible police-attended crashes over a 17-year study interval, we found the 6-week interval following a hospital stay for acute psychosis is associated with increased odds of subsequent crash and increased likelihood of the driver being deemed responsible for the crash. Clinicians should advise all patients recovering from an episode of acute psychosis to wear a seatbelt, leave ample headway, adhere to posted speed limits, avoid distracted driving, and avoid alcohol- and drug-impaired driving. Clinicians should also thoughtfully consider driving safety when discharging patients from a psychiatric hospitalization, advising patients judged to be at higher risk of crash to limit or temporarily cease driving during their convalescence.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437261454782 - Supplemental material for Acute Psychosis and the Risk of Motor Vehicle Crash: Psychose aiguë et risque d’accident de la route
Supplemental material, sj-docx-1-cpa-10.1177_07067437261454782 for Acute Psychosis and the Risk of Motor Vehicle Crash: Psychose aiguë et risque d’accident de la route by John A Staples, Daniel Daly-Grafstein, Mayesha Khan, Shannon Erdelyi, Herbert Chan, William G Honer and Jeffrey R Brubacher in The Canadian Journal of Psychiatry
Supplemental Material
sj-pdf-2-cpa-10.1177_07067437261454782 - Supplemental material for Acute Psychosis and the Risk of Motor Vehicle Crash: Psychose aiguë et risque d’accident de la route
Supplemental material, sj-pdf-2-cpa-10.1177_07067437261454782 for Acute Psychosis and the Risk of Motor Vehicle Crash: Psychose aiguë et risque d’accident de la route by John A Staples, Daniel Daly-Grafstein, Mayesha Khan, Shannon Erdelyi, Herbert Chan, William G Honer and Jeffrey R Brubacher in The Canadian Journal of Psychiatry
Footnotes
Ethics Approval
The University of British Columbia Clinical Research Ethics Board approved the study and waived the requirement for individual consent (H12-02678). All data were deidentified before release to investigators.
Author Contributions
JS, MK, SE, HC and JB were responsible for the study concept. All authors contributed to the study design. JS, SE, HC, DD and JB designed the analytic strategy; JB, HC, and SE were responsible for the acquisition of the data; DD had full access to all study data and was responsible for the integrity of the data and accuracy of the data analysis; SE contributed to the data analysis; and JS was responsible for drafting the manuscript. All authors were responsible for the critical revision of the manuscript.
Funding
This study was supported by the Canadian Institutes of Health Research (Grant No. PJT-180343). JS received research salary support as a Health Professional-Investigator from Michael Smith Health Research BC. JB received research salary support from Michael Smith Health Research BC and the British Columbia Emergency Medicine Network. Funding organizations were not involved in the design and conduct of the study; collection, management, analysis and interpretation of the data; or preparation, review and approval of this manuscript. All inferences, opinions, and conclusions drawn are those of the authors and do not reflect the opinions or policies of the Data Stewards.
Declaration of Conflicting Interests
WGH is a consultant to Translational Life Sciences, AbbVie, Newron, and Otsuka. All other authors report no competing interests.
Data Availability Statement
Access to data provided by the Data Stewards is subject to approval but can be requested for research projects through the Data Stewards or their designated service providers.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.