
Abstract
Plain language summary
Why similar scale names can create confusion in schizophrenia research
This letter responds to comments about our recent meta-analysis on subjective cognitive complaints in schizophrenia using the SSTICS scale. One study included in the analysis used a Norwegian scale with a similar acronym (SACCS), highlighting a broader problem in the field: several cognitive complaint scales have very similar names despite being different instruments. We repeated the analyses after excluding this study, and the results remained almost unchanged. This suggests that the overall conclusions of the meta-analysis are robust. The discussion also highlights the importance of clearer scale nomenclature and transparent reporting in future systematic reviews and cross-cultural research.
We thank the authors for their comments on our recent meta-analysis1,2 and for their interest in this important topic. While we agree that methodological clarity is essential in meta-analytic work, we believe that several points raised in their letter require clarification and, in some cases, qualification.
We acknowledge that one included study used the Norwegian Self-Assessed Cognitive Complaints Scale (SACCS). This inclusion reflects a broader and well-known challenge in the field: the coexistence of instruments with highly similar acronyms and partially overlapping conceptual frameworks. Alongside SACCS, the literature also includes the Self-Assessment Scale of Cognitive Complaints in Schizophrenia (SASCCS), designation used in certain contexts to refer to Arabic adaptations of the Subjective Scale to Investigate Cognition in Schizophrenia (SSTICS).3,4 Such proximity in naming is not incidental but widespread, and it inevitably creates ambiguity when synthesizing a large and multilingual body of literature.
Importantly, this issue should not be interpreted as a deviation from our methodological intent, but rather as a consequence of inconsistent nomenclature in the literature. On the contrary, our study explicitly aimed to reduce heterogeneity by focusing on a single instrument, the SSTICS. The ambiguity arises not from a lack of rigor in the inclusion criteria, but from the absence of standardized naming conventions across studies. It is therefore a structural issue within the field rather than a methodological flaw specific to our work. One might reasonably observe that, in the absence of coordinated nomenclature, different research groups can independently converge toward remarkably similar acronyms, thereby introducing confusion even in otherwise rigorous syntheses.
It is also worth noting that we had previously engaged constructively with the Norwegian group, encouraging a more detailed description of their scale items to facilitate comparison with the SSTICS. 5 This prior exchange reflects our commitment to transparency and comparability, rather than any lack of attention to instrument specificity. Furthermore, the detailed description of the Norwegian scale items, whose clarification we had advocated, was only published after our analyses had been completed, thereby limiting our ability to distinguish it more precisely during the study selection process.
Most critically, the empirical impact of this issue is negligible. We conducted a revised meta-analysis excluding the study in question, and the results remain virtually identical (Table 1). The main effect size for subjective cognitive complaints (d = 0.746); 95% CI [0.415 to 1.077]) is unchanged. The absence of a significant association between subjective and objective cognition is preserved (r ≈ 0.10), as are the non-significant relationships with Positive and Negative Syndrome Scale (PANSS) positive, general, and total symptom scores. The association with depressive symptoms remains stable and robust (r = 0.300 vs. 0.309), and the correlation with insight into illness shows only minimal variation (r = 0.155 vs. 0.142). Although the association with PANSS negative symptoms (r = 0.088, P = .040) reaches statistical significance after correction, its magnitude remains small and does not alter the overall interpretation.
Meta-analysis of the SSTICS in schizophrenia.
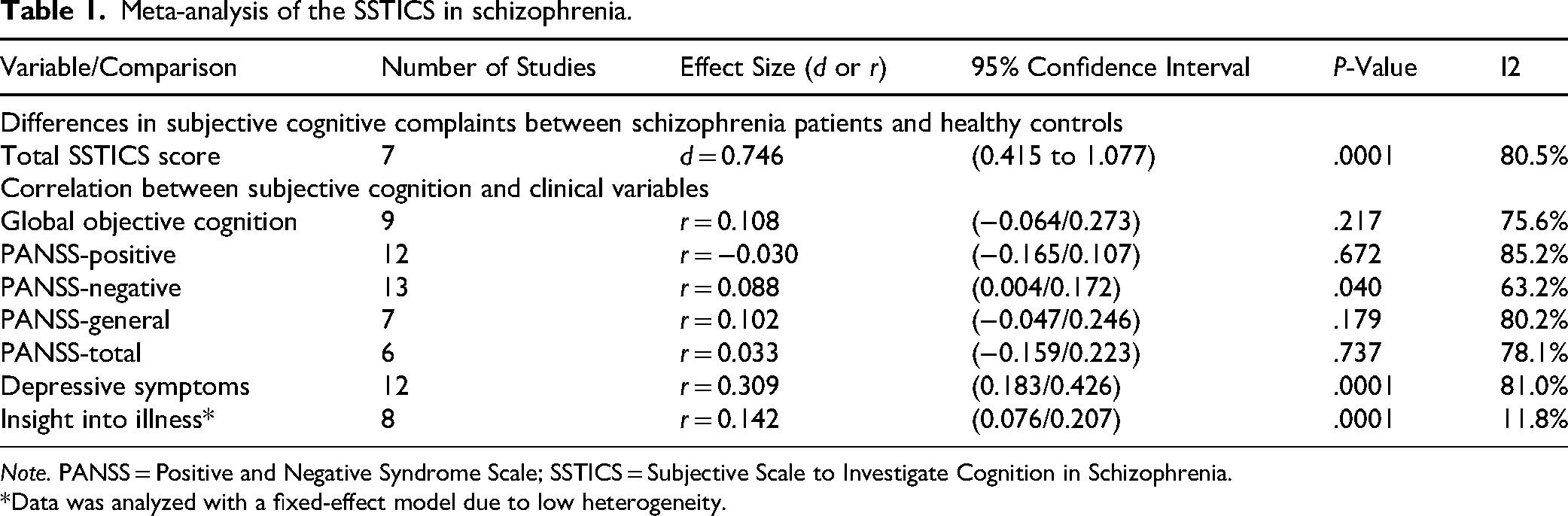
Note. PANSS = Positive and Negative Syndrome Scale; SSTICS = Subjective Scale to Investigate Cognition in Schizophrenia.
*Data was analyzed with a fixed-effect model due to low heterogeneity.
Importantly, reanalysis excluding the SACCS-based study yielded highly similar results, indicating that the overall conclusions of the meta-analysis remain unchanged. We therefore acknowledge the nomenclature-related ambiguity while noting that it had minimal impact on the reported findings.
The issue of preregistration is also raised by the commentary. 1 While preregistration in platforms such as PROSPERO enhances transparency by specifying inclusion criteria and analytic strategies a priori, it should not be conflated with methodological validity. 6 Importantly, preregistration does not ensure adherence to the protocol or prevent post hoc modifications, as inconsistencies between registered protocols and published reviews have been documented in the methodological literature. Our study followed PRISMA guidelines, with clearly defined inclusion criteria and reproducible analytic procedures. Moreover, preregistration would not have resolved the underlying ambiguity related to instrument naming, nor would it have altered the results. It is therefore important to avoid overstating its role in addressing issues that are, in essence, structural.
This discussion also reflects broader concerns regarding methodological choices in systematic reviews. For example, restricting inclusion to post-2014 publications may exclude a substantial body of SSTICS-based research validated across multiple cultural and linguistic contexts. 7 Such decisions, while sometimes justified, may inadvertently influence the visibility and interpretation of SSTICS-related findings.
This issue extends beyond the present meta-analysis. Recent literature continues to reflect ambiguity regarding the distinction between the SSTICS and similarly named instruments such as the SASCCS, which corresponds to an Arabic adaptation derived from the SSTICS framework. For example, Øie 8 et al. (2025) discuss the SSTICS and SASCCS as separate instruments in schizophrenia research. Such inconsistencies in nomenclature and reporting may contribute to confusion in future reviews and meta-analyses unless instrument lineage and adaptation processes are more explicitly described.
In conclusion, we appreciate the opportunity to clarify this issue. We acknowledge that similarities in scale nomenclature contributed to ambiguity during study selection. However, reanalysis excluding the SACCS-based study produced highly similar findings, supporting the consistency of the original conclusions. This exchange also highlights the importance of clear reporting and standardized instrument nomenclature in future research.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.