
Abstract
Background and Objectives
Illicit prescription painkiller use among university students is a growing concern, influenced by a range of demographic, mental and physical health, academic, and co-substance use factors contributing to the elevated risk. However, Canadian evidence specific to university students remains limited. This study examined correlates of self-reported illicit prescription painkiller use among Canadian university students.
Method
A secondary analysis of data from the American College Health Association National College Health Assessment II Canadian university edition was conducted. The dependent variable was past-year illicit prescription painkiller use, defined as a yes or no response to self-reported use of prescription painkillers without a prescription from a healthcare provider in the past 12 months. Descriptive statistics and binary logistic regression were used to examine associated demographic, academic, physical health, mental health, and co-substance use factors.
Results
Among the analytical sample of 44,508, 5.8% (n = 2,585) reported illicit prescription painkiller use in the past 12 months. Significant predictors included race, sex, sexual identity, international student status, mental health factors, chronic illness, academic factors, and co-substance use. Higher odds of use were observed among West Asian and Black students, international students, students with chronic illness, students reporting hopelessness, feeling overwhelmed, depression with functional impairment, or suicidal ideation, and students reporting tobacco, alcohol, e-cigarette, or cocaine use.
Conclusions
Illicit prescription painkiller use among Canadian university students was associated with demographic, mental health, physical health, academic, and co-substance use factors. Findings support campus-based prevention and support strategies that integrate substance use education, mental health services, and equitable access to care.
Plain Language Summary Title
Understanding Prescription Painkiller Use Without a Prescription Among Canadian University Students: The Role of Mental Health, Student Characteristics, Physical Health, Academics, and Substance Use
Prescription painkiller use such as opioids is an important concern among university students. This study used Canadian data from the American College Health Association National College Health Assessment II to examine which student characteristics were associated with this behaviour.
Among the analytic sample, 5.8% reported using prescription painkillers without a prescription in the past 12 months. Higher odds of use were seen among students with mental health concerns, chronic illness, international student status, and use of other substances such as tobacco, alcohol, e-cigarettes, and cocaine. Differences were also observed by race, sex, sexual identity, academic year, and grade point average.
These findings suggest that prescription painkiller use without a prescription is linked to broader health, social, and academic factors. Universities may benefit from prevention strategies that combine substance use education, mental health support, and improved access to care.
Introduction
Irrespective of the many emerging global policies to limit the current prescription painkiller crisis,1,2 the frequency of prescriptions, overdoses, and related deaths have increased over the past decade.3,4 Much of this rise is believed to date back to the 1990s as a result of the billion-dollar pharmaceutical industry campaigns. 1 In 2013, it was estimated that 207 million opioid prescriptions were written globally, an increase from the 76 million prescribed in 1991. 5 In 2015, 4.7% of those with opioid prescriptions misused them, 6 and treatment admissions for substance use disorders more than doubled between 2002 and 2010. 5 Notably, approximately a third of admissions were among individuals aged 18 to 34. 5 Young adults between the ages of 18 and 25 are particularly vulnerable to opioid use disorders, with this age group reporting the highest use in recent national surveys. 7 Further, the risk of developing opioid use disorders tends to occur commonly among adolescents and young adults, which coincides with most college/university students. 8 While limited research has examined painkiller misuse, a study using the fall 2008 National College Health Assessment (NCHA) data, though outdated, found that 13% of students had used prescription drugs without a prescription. 9
Substance use during university has been associated with a range of adverse outcomes, including decreased academic performance, higher unemployment rates post-graduation, increased risk of committing or experiencing sexual assault, greater risk of engagement in illegal behaviours, psychological distress, and higher dropout rates.5,8,10 Mental health is a particularly relevant factor, as students with anxiety, depression, or other mental health disorders are at a greater risk of substance misuse 11 ; conversely, substance use itself may worsen or trigger symptoms of anxiety and depression, suggesting a bidirectional relationship.12,13 To add, this age group has been found to be more reluctant to enter and retain treatment, despite experiencing significant distress. 8 A systematic review by Weyandt et al. 10 found that misuse of prescription opioids among students varied according to motives, co-occurring substance use, gender, and ethnicity. For instance, 31.9% of students misused opioids to get high, while 26.8% did so out of curiosity. 10 Males and White students reported higher rates of misuse and were more likely to combine opioids with other substances such as alcohol, marijuana, and cocaine. 10 In contrast, other studies suggest that Black individuals may be more likely to obtain and use opioids illicitly, often as a consequence of systematic barriers to healthcare services and treatment, compared to White populations. 1 The role of international student status is mixed, while some students report lower rates of use due to cultural norms and stricter legal consequences, 14 others suggest that increased misuse due to reduced supervision and cultural adjustments. 15
Despite growing concerns, Canada continues to face a significant opioid crisis, with over 40,000 apparent opioid toxicity deaths recorded between 2016 and 2023. 16 Canadian evidence also shows a substantial mortality burden among young adults aged 20 to 39 years. 17 While this mortality data does not directly measure prescription painkiller misuse among students, they highlight the importance of studying opioid- and painkiller-related risk in young adult populations. Yet, Canadian data on painkiller misuse among students remain limited. Existing studies often include small samples,5,18–20 focus narrowly on either descriptive variables or specific psychological or physical factors.18,20,21 Furthermore, most of the existing literature on student opioid misuse is based on American university and college students, which may not directly translate to the Canadian context due to significant differences in the healthcare systems, drug policies, demographic patterns,22–24 and campus culture. 25 The need for Canadian-specific data is further emphasized by Canada's high level of prescription opioid consumption. 26
Herein, we extend existing literature, identifying the correlates of students’ illicit prescription painkiller use through multivariable analysis. We examined the specific predictors associated with the illicit use of prescription painkillers, including demographic factors, health factors, academics, and alcohol/drug use. Investigating painkiller misuse by incorporating a broader set of risk factors, particularly mental health, offers a more comprehensive assessment of vulnerabilities among university students in Canada. Given the increasing burden of mental health challenges in Canada, 27 understanding prescription painkiller misuse risks among students has become increasingly important. Approximately 5 million Canadians met the diagnostic criteria for mood and anxiety disorders in 2022, including depression, bipolar disorder, generalized anxiety disorder, and social phobias. 28 Our study provides a more recent reflection of user patterns for painkiller misuse within the distinct cultural, societal, and policy context of Canada. Specifically, this study aims to identify the demographic, physical health, mental health, academic, and substance use predictors of illicit prescription painkiller use among Canadian university students using a large, national dataset.
Materials and Methods
Survey Design and Participants
This study is a secondary analysis of data obtained from a cross-sectional, self-report survey collected by the American College Health Association (ACHA). The survey collects self-reported information on students’ general health, disease and injury prevention, academic impacts, tobacco/alcohol/drug use, sexual behaviour, and mental health. In the ACHA-NCHA II Spring 2019 Canadian Survey, the dependent variable was assessed using an item asking whether students had used “prescription painkillers,” such as OxyContin, Vicodin, Codeine, without a prescription from a healthcare provider in the past 12 months. These examples are opioid-type prescription analgesics; however, the survey did not ask respondents to identify the specific medication used. Therefore, this study uses the term “illicit prescription painkiller use” to remain consistent with the survey wording, while acknowledging that the item primarily reflects non-prescribed use of opioid-type prescription painkillers and cannot be interpreted as confirmed opioid-specific use. Research ethics approval was granted by the University of Waterloo Research Ethics Board in accordance with the Tri-Council Policy Statement for the Ethical Conduct for Research Involving Humans. All participants in this study provided voluntary, and informed consent to data collection. The study protocol adheres to the ethical principles outlined in the Declaration of Helsinki. Participant data were treated with strict confidentiality and anonymized to protect privacy. The research poses minimal risk to participants, and all procedures were approved by the institutional ethics committee.
Variables of Interest
Outcome
The primary outcome was past-year illicit prescription painkiller use, defined as self-reported use of prescription painkillers without a prescription from a healthcare provider in the previous 12 months. Responses were categorized as yes or no.
Predictors of interest
Predictors of interest included race, international student status, academic performance, general health, chronic illness, mental health indicators, and alcohol, tobacco, e-cigarette, marijuana, and cocaine use.
Covariates
The multivariable model adjusted for demographic, academic, physical health, mental health, and co-substance use variables selected based on prior literature and theoretical relevance. Categories with sparse counts were collapsed where appropriate to improve model stability and interpretability.
Data Analysis
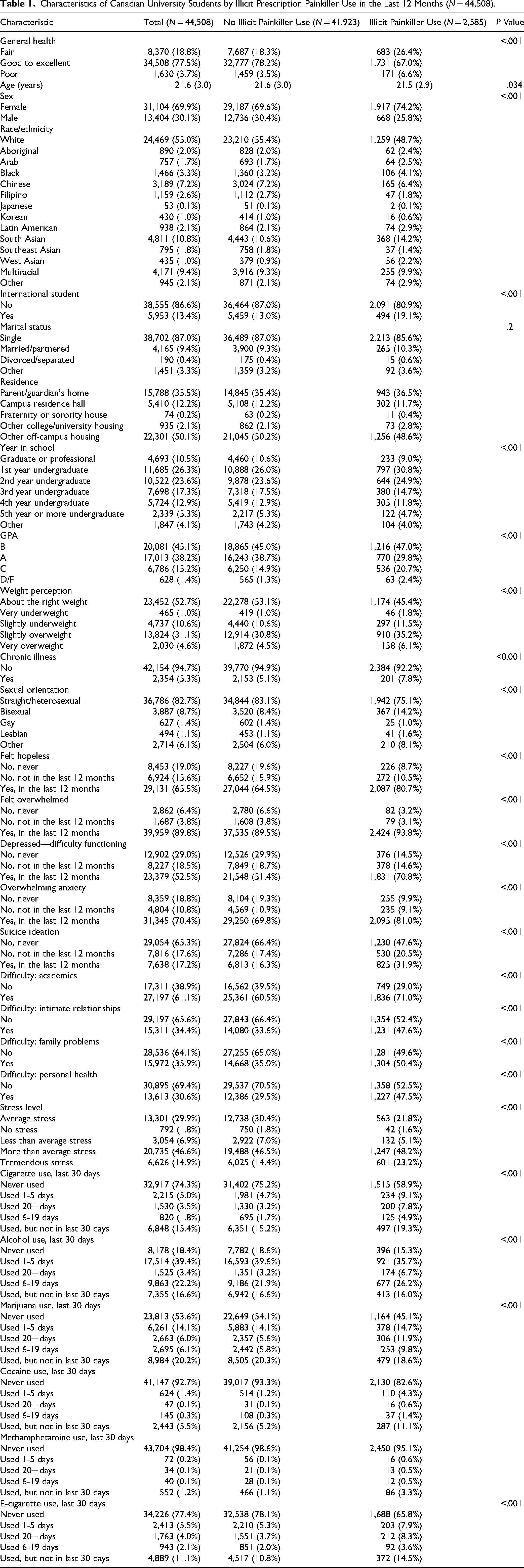
All statistical analyses were conducted in RStudio.29,30 To reflect the university student population, the analytic regression sample was restricted to participants aged 18 to 30. This age range was selected to include traditional undergraduate students as well as older undergraduate, graduate, and professional students who remain relevant to university-based prevention and intervention efforts. Descriptive statistics for the overall sample and for students reporting past-year illicit prescription painkiller use were calculated and are presented in Table 1. Percentages were calculated using the available responses for each variable unless otherwise specified; therefore, percentages may not sum to 100% because of missing, skipped, or invalid responses. Difference between students who did and did not report past-year illicit prescription use were assessed using Pearson's chi-squared tests for categorical variables and Wilcoxon rank-sum tests for continuous variables, with corresponding P-values reported in Table 1. A multivariable binary logistic regression analysis was used to examine the association between risk factors of interest and illicit prescription painkiller use.
Characteristics of Canadian University Students by Illicit Prescription Painkiller Use in the Last 12 Months (N = 44,508).
Results
Descriptive Results
Of the 55,284 respondents who completed the survey, 54,895 responded to the question on illicit painkiller use. After restricting the sample to participants aged 18 to 30 with complete data on all model covariates, the final analytic sample included 44,508 students, of whom 2,585 (5.8%) reported use in the last 12 months. The analytic sample had a mean age of 21.6 years (SD = 3.0) and was 69.9% female (Table 1). Among students who reported use, the majority were female (74.2%), White (48.7%), and reported good to excellent health (67.0%). In this group, 30.8% were in their first year of undergraduate studies and 19.1% were international students. Nearly half reported a B average (47.0%), while 29.8% reported an A average and 2.4% reported a D or F average (Table 1).
Binary Logistic Regression Analysis
Demographic factors
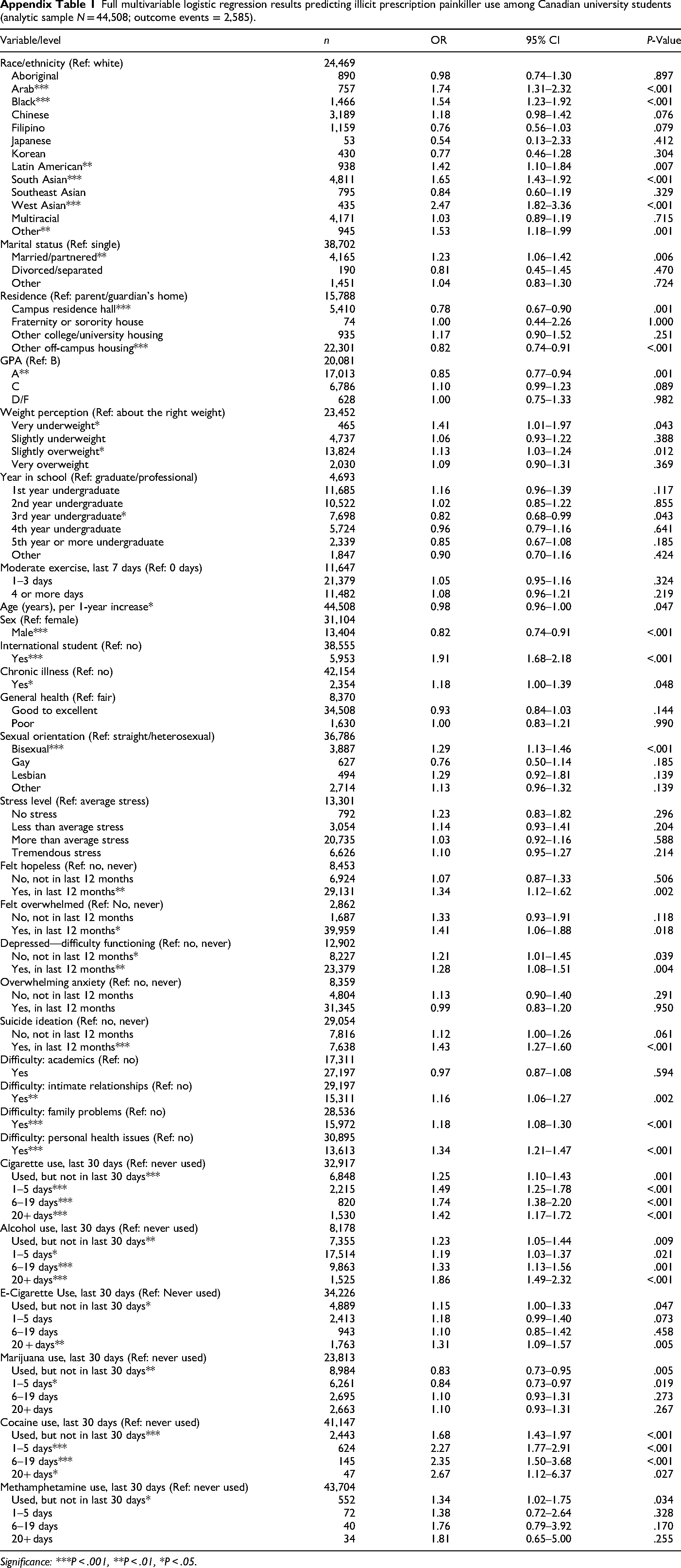
Figure 1 presents the multivariable logistic regression results, highlighting significant predictors of illicit painkiller use among Canadian university students. Findings of all covariates can be found in Appendix Table 1. Compared to White students, several racial minorities had higher odds of illicitly using painkillers, including West Asian (OR = 2.47, 95% CI, 1.82 to 3.36, P < .001), Arab (OR = 1.74, 95% CI, 1.31 to 2.32, P < .001), and Black students (OR = 1.54, 95% CI, 1.23 to 1.92, P < .001). Male students had lower odds of illicit prescription painkiller use than female students (OR = 0.82, 95% CI, 0.74 to 0.91, P < .001), as did older students (OR = 0.98, 95% CI, 0.96 to 1.00, P < .05). Students identifying as bisexual had higher odds of illicit use (OR = 1.29, 95% CI, 1.13 to 1.46, P < .001), compared to straight students.
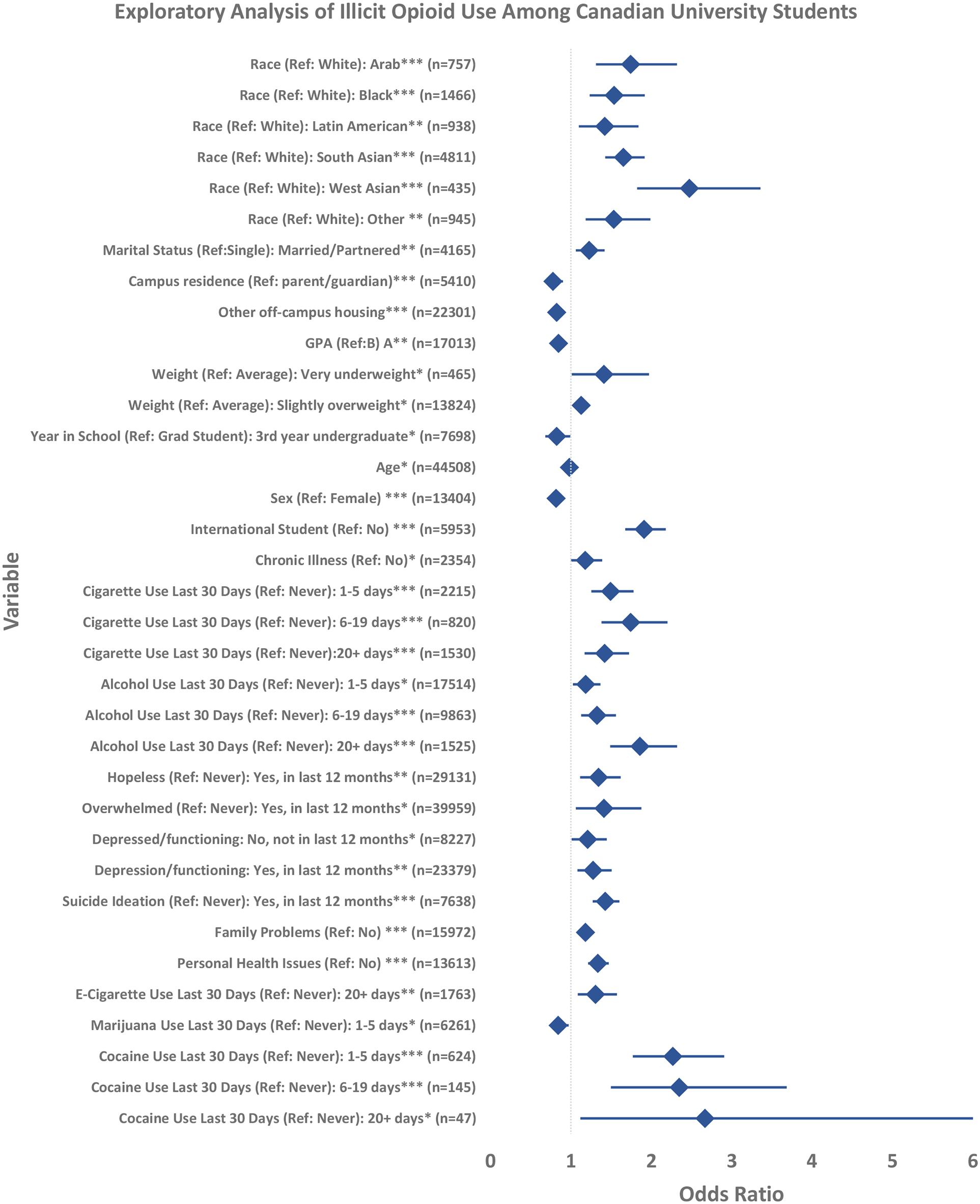
Significant predictors of illicit prescription painkiller use among Canadian university students, multivariable logistic regression (analytic sample N = 44,508; outcome events = 2,585). Odds ratios with 95% confidence intervals shown. Statistical significance is indicated as: p < .05 (*), p < .01 (**), and p < .001 (***).
Physical and mental health-related factors
The results indicate that covariates related to participants’ mental health play an important role in illicit painkiller use. Students who reported seriously considering suicide in the last 12-months had higher odds of illicit painkiller use (OR = 1.43, 95% CI, 1.27 to 1.60, P < .001), compared to those who reported never having such thoughts. Similarly, individuals who reported feeling hopeless (OR = 1.34, 95% CI, 1.12 to 1.62, P < .01), overwhelmed (OR = 1.41, 95% CI, 1.06 to 1.88, P < .05), or depressed to the point of impaired function (OR = 1.28, 95% CI, 1.08 to 1.51, P < .01) had higher odds of use. Compared with students who did not report traumatic events, those reporting trauma related to family (OR = 1.18, 95% CI, 1.08 to 1.30, P < .001) and personal health (OR = 1.34, 95% CI, 1.21 to 1.47, P < .001) also had higher odds of use. Students with chronic illnesses had higher odds of illicit painkiller use than students reporting no chronic illness (OR = 1.18, 95% CI, 1.00 to 1.39, P < .05).
Academic factors
Compared with graduate and professional students, third-year students had lower odds of nonmedical prescription painkiller use (OR = 0.82, 95% CI, 0.68 to 0.99, P < .05). Students with an average A GPA also had lower odds of use than students with a B average (OR = 0.85, 95% CI, 0.77 to 0.94, P < .01). International students had nearly twice the odds of illicit prescription painkiller use compared with domestic students (OR = 1.91, 95% CI, 1.68 to 2.18, P < .001).
Co-substance use
Co-substance use variables were strongly associated with illicit prescription painkiller use. Compared with non-smokers, students who smoked 1 to 5 days (OR = 1.49, 95% CI, 1.25 to 1.78, P < .001), 6 to 19 days (OR = 1.74, 95% CI, 1.38 to 2.20, P < .001), and more than 20 days (OR = 1.42, 95% CI, 1.17 to 1.72, P < .001) all had increased odds of use. Alcohol use and e-cigarettes also depicted a dose–response relationship, with individuals who drank more than 20 days (OR = 1.86, 95% CI, 1.49 to 2.32, P < .001) and used e-cigarettes for more than 20 days (OR = 1.31, 95% CI, 1.09 to 1.57, P < .001) also had increased odds, compared to non-users. Cocaine use was also associated with higher odds, with the highest estimate among students reporting cocaine use on more than 20 days (OR = 2.67, 95% CI, 1.12 to 6.37, P < .05). In contrast, students reporting marijuana 1 to 5 days (OR = 0.84, 95% CI, 0.73 to 0.97, P < .05) or previous marijuana use but not in the last 30 days (OR = 0.83, 95% CI, 0.73 to 0.95, P < .01) had lower odds of illicit prescription painkiller use than non-users.
Discussion
Race and Other Demographics
This study reveals critical insights into the prevalence and risk factors of painkiller use without a prescription among Canadian university students. Notably, the results underscore the association between race and prescription painkiller misuse. West Asian students demonstrated higher odds of painkiller misuse compared with White students. This finding should be interpreted cautiously, as the ACHA-NCHA II did not measure medication source, pain severity, cultural norms, and other important confounders. While the specific drivers of this disparity cannot be determined from cross-sectional data, the findings may reflect unmeasured structural or contextual factors, including barriers to healthcare access, differences in pain management experiences, stigma, or differential access to formal medical care. Future qualitative and longitudinal quantitative research is needed to better understand the mechanisms underlying this association.
Similarly, Black students were also more likely to use prescription painkillers without a prescription, in comparison to White students. This finding should be interpreted in the context of broader evidence on racial inequities in pain assessment, prescribing, and healthcare access. Data from 1993 to 2009 indicates large disparities between the rate of prescription painkillers, such as opiates, between White Americans (approximately 16/100,000) and Black Americans (5/100,000), 31 highlighting disparities in access. Overall, White students were less likely to use prescription painkillers without a prescription in comparison to Black, Arab, Latin American, and West Asian students. These findings are inconsistent with existing American literature that has reported higher rates of opioid misuse among White individuals. 32 This discrepancy may reflect important contextual differences between Canada and the United States, including disparities in healthcare access, drug policy,33,34 and the racial composition of the university population, 35 which may alter who is more likely to seek illicit alternatives to prescribed medications.
Given the limited access to prescription medications often reported by minority groups, White students may have greater access to prescription painkillers through healthcare providers, making them less likely to obtain these drugs without a prescription. Moreover, doctors may be more willing to prescribe painkillers to White than to Black and minority students, as the latter groups are often incorrectly stereotyped as more likely to abuse or sell prescription painkillers. 1 However, because the present study did not measure pain severity, prescription access, medication source, or experiences of discrimination, these mechanisms cannot be directly measured. Nonetheless, these findings highlight the importance of equity-focused prevention strategies and improved access to culturally responsive health and counselling services for racialized students.
Findings indicate that bisexual students were at a higher risk of painkiller use, consistent with previous research. This may be explained by the cognitive dissonance theory, where conflicting beliefs cause psychological distress, that may contribute to opioid misuse. 36 Additionally, men had significantly lower odds of illicit painkiller use compared to women, aligning with studies citing differences in pain experiences, cultural norms, and likelihood of experiencing dependency. 37 These findings suggest the need for targeted support addressing the diverse social and psychological factors influencing prescription drug misuse, particularly among bisexual students and women.
Physical and psychological factors
Psychological well-being was associated with illicit prescription painkiller use. Students who reported feeling hopeless, overwhelmed, having personal health issues, and those who seriously considered suicide were more likely to use prescription painkillers without a prescription compared to those who reported never having such feelings. These findings align with previous literature linking opioid misuse to suicidal ideation, depression, and psychological distress.38–40 However, given that our study uses cross-sectional data, we cannot determine whether mental health concerns preceded, followed, or co-occurred with illicit prescription painkiller use.
Similarly, emotional stressors such as family problems were associated with increased odds of misuse, consistent with prior research. 41 These findings are relevant in Canadian universities given the increased prevalence of student mental health struggles and lack of university mental wellness initiatives. 42 Canadian university students face long wait times, limited access to culturally competent care, and inadequate mental health infrastructures both on campus and within the broader healthcare system, where many even lack a family doctor.43,44 These disparities severely limit struggling students’ access to early preventative intervention and may contribute to their self-medication with illicitly obtained painkillers. Our findings further highlight the need for improved care to limit the risk of painkiller misuse among undergraduates.
Students with chronic illness had higher odds of illicit prescription painkiller use than those without chronic illness. Chronic pain and illness can affect academic functioning through missed class, reduced concentration, and reliance on others 45 ; however, this study did not measure pain severity, prescribed medication access, or reasons for use. Students with bodyweight extremes also had higher odds of use. This association may reflect unmeasured physical discomfort, chronic health conditions, or psychological distress, but these mechanisms were not directly assessed. Additional research is needed to clarify the relationship between physical health, pain, bodyweight, and illicit prescription painkiller use among university students.
Academic factors
Academic performance and health-related challenges were important factors in illicit prescription painkiller use among university students. Previous studies have linked illicit drug use with lower academic performance.5,8,10,46 In this study, students with an A average had lower odds of use than students with a B average, while lower GPA categories did not differ significantly. This may suggest that academically high-achieving students benefit from healthier coping mechanisms, consistent with research on stress-coping profiles. 47 Similarly, third-year students showed lower risk of misuse compared to other students. However, this finding should be interpreted cautiously as the year in school may reflect academic pressure, student responsibilities, or other unmeasured factors.
International student status was associated with higher odds of illicit prescription painkiller use. In comparison to other countries, such as America, Canadian universities have the second-highest proportion of international students, after Australia. 48 While some research suggests that international students are less likely to misuse substances,14,49 a systematic review by Aresi et al. 15 found that intercultural stressors may increase the risk of alcohol and drug use. Our findings support the latter, indicating higher odds of painkiller misuse among international students. In the Canadian context, barriers to healthcare access, communication challenges, unfamiliarity with health systems, and insurance differences may contribute to unmet health needs.50–52 In Canada, many international students are not covered by provincial healthcare (e.g., Ontario Health Insurance Plan), 53 and may seek alternative forms of pain management, increasing the risk of illicit painkiller use.
Co-substance use
Another influential predictor of prescription painkiller uses without a prescription found in this study was a student's use of tobacco, alcohol, and other drugs. Various studies suggest that those who misuse prescription painkillers are more likely to report recreational use of other prescriptions, as well as an increased odds for engaging in cigarette smoking, heavy drinking, and other illicit drugs.54–56 Generally, these findings align with the results of our study that indicate increased odds of prescription painkiller use for those who had higher frequencies of drug, alcohol, and tobacco use compared to nonusers. Interestingly, while some research has shown that marijuana use is associated with higher rates of prescription painkiller misuse, 57 other studies, including our own, have found an inverse relationship. 58 It may be possible that students use marijuana for pain relief,59,60 and therefore, may not need prescription painkillers.
Limitations and Implications of Findings
The ACHA data had a relatively low response rate (∼20%), introducing potential participation bias and limiting generalizability. Given that there are many variables of interest and there are no identifying variables (participant identifiers), no sample weights were conducted. The study utilized a narrow definition of prescription misuse as using medication without a prescription. A more inclusive definition that may include additional methods of misuse such as using another person's prescription or using one's medication for a different purpose or dose than intended. This definition of prescription misuse may limit the generalizability of our predictors. Although the ACHA-NCHA II item provided opioid-type examples of prescription painkillers, the survey did not capture the exact medication used; therefore, findings should be interpreted as illicit prescription painkiller use rather than confirmed opioid-specific misuse. Furthermore, as a cross-sectional study using data collected at a single point in time, causal relationships cannot be inferred or established. Therefore, the associations identified in this study are observational and should be interpreted accordingly. Residual confounding from unmeasured variables also cannot be ruled out, as the model may not have captured all relevant predictors of illicit painkiller use. Lastly, given that this study utilizes a self-report measure, the question requires individuals to admit to illicit drug use and may therefore be underreported, which may affect the precision of the prevalence estimates due to self-report bias.
Irrespective of these limitations, our study offers important Canada-specific insights into prescription painkiller misuse among university students, an area where national data has been limited. While Canada's publicly funded healthcare system reduces some barriers to prescription access, illicit use persists, 61 suggesting that broader cultural and systemic factors may also contribute. Our findings underscore academic, physical, and mental health factors as key predictors of painkiller misuse, emphasizing the importance of addressing psychological and healthcare access challenges unique to the Canadian context.
Amid growing concerns of student mental health and the opioid crisis in Canada, these findings provide meaningful guidance for campus policies and public health planning. They highlight the need for culturally competent prevention, targeted outreach, and improved counselling services for high-risk populations. Targeted educational campaigns, delivered through orientation events, seminars, university newsletters, and course modules, alongside mental health initiatives, may be especially effective for incoming and at-risk students. These strategies may help students recognize the risks of illicit prescription painkiller use, identify early warning signs, and connect with national support initiatives such as the Public Health Agency of Canada's Youth Substance Use Prevention Program.
Importantly, this study does not assume the motivations behind non-medical use of prescription painkillers or suggest that all use is recreational. Instead, it identifies students who may be more vulnerable due to physical health issues, psychological distress, or limited access to care. Future research may build on this work using longitudinal designs to explore the temporal trends and risk factors over time. Ultimately, we hope that these findings support early intervention efforts and guide universities and policymakers in expanding access to timely medical and mental health support.
Footnotes
Acknowledgments
We would like to thank Dr Kanwal Singh for editing the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer from the American College Health Association
The opinions, findings, and conclusions presented/reported in this article/presentation are those of the authors, and are in no way meant to represent the corporate opinions, views, or policies of the American College Health Association (ACHA). ACHA does not warrant nor assume any liability or responsibility for the accuracy, completeness, or usefulness of any information presented in this article/presentation.
Data Access
Data for this study was obtained from the American College Health Association, specifically, the Canadian subset of the National College Health Assessment.
Full multivariable logistic regression results predicting illicit prescription painkiller use among Canadian university students (analytic sample N = 44,508; outcome events = 2,585).
| Variable/level | n | OR | 95% CI | P-Value |
|---|---|---|---|---|
| Race/ethnicity (Ref: white) | 24,469 | |||
| Aboriginal | 890 | 0.98 | 0.74–1.30 | .897 |
| Arab*** | 757 | 1.74 | 1.31–2.32 | <.001 |
| Black*** | 1,466 | 1.54 | 1.23–1.92 | <.001 |
| Chinese | 3,189 | 1.18 | 0.98–1.42 | .076 |
| Filipino | 1,159 | 0.76 | 0.56–1.03 | .079 |
| Japanese | 53 | 0.54 | 0.13–2.33 | .412 |
| Korean | 430 | 0.77 | 0.46–1.28 | .304 |
| Latin American** | 938 | 1.42 | 1.10–1.84 | .007 |
| South Asian*** | 4,811 | 1.65 | 1.43–1.92 | <.001 |
| Southeast Asian | 795 | 0.84 | 0.60–1.19 | .329 |
| West Asian*** | 435 | 2.47 | 1.82–3.36 | <.001 |
| Multiracial | 4,171 | 1.03 | 0.89–1.19 | .715 |
| Other** | 945 | 1.53 | 1.18–1.99 | .001 |
| Marital status (Ref: single) | 38,702 | |||
| Married/partnered** | 4,165 | 1.23 | 1.06–1.42 | .006 |
| Divorced/separated | 190 | 0.81 | 0.45–1.45 | .470 |
| Other | 1,451 | 1.04 | 0.83–1.30 | .724 |
| Residence (Ref: parent/guardian's home) | 15,788 | |||
| Campus residence hall*** | 5,410 | 0.78 | 0.67–0.90 | .001 |
| Fraternity or sorority house | 74 | 1.00 | 0.44–2.26 | 1.000 |
| Other college/university housing | 935 | 1.17 | 0.90–1.52 | .251 |
| Other off-campus housing*** | 22,301 | 0.82 | 0.74–0.91 | <.001 |
| GPA (Ref: B) | 20,081 | |||
| A** | 17,013 | 0.85 | 0.77–0.94 | .001 |
| C | 6,786 | 1.10 | 0.99–1.23 | .089 |
| D/F | 628 | 1.00 | 0.75–1.33 | .982 |
| Weight perception (Ref: about the right weight) | 23,452 | |||
| Very underweight* | 465 | 1.41 | 1.01–1.97 | .043 |
| Slightly underweight | 4,737 | 1.06 | 0.93–1.22 | .388 |
| Slightly overweight* | 13,824 | 1.13 | 1.03–1.24 | .012 |
| Very overweight | 2,030 | 1.09 | 0.90–1.31 | .369 |
| Year in school (Ref: graduate/professional) | 4,693 | |||
| 1st year undergraduate | 11,685 | 1.16 | 0.96–1.39 | .117 |
| 2nd year undergraduate | 10,522 | 1.02 | 0.85–1.22 | .855 |
| 3rd year undergraduate* | 7,698 | 0.82 | 0.68–0.99 | .043 |
| 4th year undergraduate | 5,724 | 0.96 | 0.79–1.16 | .641 |
| 5th year or more undergraduate | 2,339 | 0.85 | 0.67–1.08 | .185 |
| Other | 1,847 | 0.90 | 0.70–1.16 | .424 |
| Moderate exercise, last 7 days (Ref: 0 days) | 11,647 | |||
| 1–3 days | 21,379 | 1.05 | 0.95–1.16 | .324 |
| 4 or more days | 11,482 | 1.08 | 0.96–1.21 | .219 |
| Age (years), per 1-year increase* | 44,508 | 0.98 | 0.96–1.00 | .047 |
| Sex (Ref: female) | 31,104 | |||
| Male*** | 13,404 | 0.82 | 0.74–0.91 | <.001 |
| International student (Ref: no) | 38,555 | |||
| Yes*** | 5,953 | 1.91 | 1.68–2.18 | <.001 |
| Chronic illness (Ref: no) | 42,154 | |||
| Yes* | 2,354 | 1.18 | 1.00–1.39 | .048 |
| General health (Ref: fair) | 8,370 | |||
| Good to excellent | 34,508 | 0.93 | 0.84–1.03 | .144 |
| Poor | 1,630 | 1.00 | 0.83–1.21 | .990 |
| Sexual orientation (Ref: straight/heterosexual) | 36,786 | |||
| Bisexual*** | 3,887 | 1.29 | 1.13–1.46 | <.001 |
| Gay | 627 | 0.76 | 0.50–1.14 | .185 |
| Lesbian | 494 | 1.29 | 0.92–1.81 | .139 |
| Other | 2,714 | 1.13 | 0.96–1.32 | .139 |
| Stress level (Ref: average stress) | 13,301 | |||
| No stress | 792 | 1.23 | 0.83–1.82 | .296 |
| Less than average stress | 3,054 | 1.14 | 0.93–1.41 | .204 |
| More than average stress | 20,735 | 1.03 | 0.92–1.16 | .588 |
| Tremendous stress | 6,626 | 1.10 | 0.95–1.27 | .214 |
| Felt hopeless (Ref: no, never) | 8,453 | |||
| No, not in last 12 months | 6,924 | 1.07 | 0.87–1.33 | .506 |
| Yes, in last 12 months** | 29,131 | 1.34 | 1.12–1.62 | .002 |
| Felt overwhelmed (Ref: No, never) | 2,862 | |||
| No, not in last 12 months | 1,687 | 1.33 | 0.93–1.91 | .118 |
| Yes, in last 12 months* | 39,959 | 1.41 | 1.06–1.88 | .018 |
| Depressed—difficulty functioning (Ref: no, never) | 12,902 | |||
| No, not in last 12 months* | 8,227 | 1.21 | 1.01–1.45 | .039 |
| Yes, in last 12 months** | 23,379 | 1.28 | 1.08–1.51 | .004 |
| Overwhelming anxiety (Ref: no, never) | 8,359 | |||
| No, not in last 12 months | 4,804 | 1.13 | 0.90–1.40 | .291 |
| Yes, in last 12 months | 31,345 | 0.99 | 0.83–1.20 | .950 |
| Suicide ideation (Ref: no, never) | 29,054 | |||
| No, not in last 12 months | 7,816 | 1.12 | 1.00–1.26 | .061 |
| Yes, in last 12 months*** | 7,638 | 1.43 | 1.27–1.60 | <.001 |
| Difficulty: academics (Ref: no) | 17,311 | |||
| Yes | 27,197 | 0.97 | 0.87–1.08 | .594 |
| Difficulty: intimate relationships (Ref: no) | 29,197 | |||
| Yes** | 15,311 | 1.16 | 1.06–1.27 | .002 |
| Difficulty: family problems (Ref: no) | 28,536 | |||
| Yes*** | 15,972 | 1.18 | 1.08–1.30 | <.001 |
| Difficulty: personal health issues (Ref: no) | 30,895 | |||
| Yes*** | 13,613 | 1.34 | 1.21–1.47 | <.001 |
| Cigarette use, last 30 days (Ref: never used) | 32,917 | |||
| Used, but not in last 30 days*** | 6,848 | 1.25 | 1.10–1.43 | .001 |
| 1–5 days*** | 2,215 | 1.49 | 1.25–1.78 | <.001 |
| 6–19 days*** | 820 | 1.74 | 1.38–2.20 | <.001 |
| 20+ days*** | 1,530 | 1.42 | 1.17–1.72 | <.001 |
| Alcohol use, last 30 days (Ref: never used) | 8,178 | |||
| Used, but not in last 30 days** | 7,355 | 1.23 | 1.05–1.44 | .009 |
| 1–5 days* | 17,514 | 1.19 | 1.03–1.37 | .021 |
| 6–19 days*** | 9,863 | 1.33 | 1.13–1.56 | .001 |
| 20+ days*** | 1,525 | 1.86 | 1.49–2.32 | <.001 |
| E-Cigarette Use, last 30 days (Ref: Never used) | 34,226 | |||
| Used, but not in last 30 days* | 4,889 | 1.15 | 1.00–1.33 | .047 |
| 1–5 days | 2,413 | 1.18 | 0.99–1.40 | .073 |
| 6–19 days | 943 | 1.10 | 0.85–1.42 | .458 |
| 20 + days** | 1,763 | 1.31 | 1.09–1.57 | .005 |
| Marijuana use, last 30 days (Ref: never used) | 23,813 | |||
| Used, but not in last 30 days** | 8,984 | 0.83 | 0.73–0.95 | .005 |
| 1–5 days* | 6,261 | 0.84 | 0.73–0.97 | .019 |
| 6–19 days | 2,695 | 1.10 | 0.93–1.31 | .273 |
| 20+ days | 2,663 | 1.10 | 0.93–1.31 | .267 |
| Cocaine use, last 30 days (Ref: never used) | 41,147 | |||
| Used, but not in last 30 days*** | 2,443 | 1.68 | 1.43–1.97 | <.001 |
| 1–5 days*** | 624 | 2.27 | 1.77–2.91 | <.001 |
| 6–19 days*** | 145 | 2.35 | 1.50–3.68 | <.001 |
| 20+ days* | 47 | 2.67 | 1.12–6.37 | .027 |
| Methamphetamine use, last 30 days (Ref: never used) | 43,704 | |||
| Used, but not in last 30 days* | 552 | 1.34 | 1.02–1.75 | .034 |
| 1–5 days | 72 | 1.38 | 0.72–2.64 | .328 |
| 6–19 days | 40 | 1.76 | 0.79–3.92 | .170 |
| 20+ days | 34 | 1.81 | 0.65–5.00 | .255 |
Significance: ***P < .001, **P < .01, *P < .05.