
Abstract
Keywords
The Canadian Network for Mood and Anxiety Treatments’ (CANMAT) 2023 Update on Clinical Guidelines for the Management of Major Depressive in Adults 1 (“Guidelines”) was a much-anticipated update to the 2016 Guidelines. 2 The Guidelines’ consideration of conventional and non-conventional treatments within the context of patient-centred care makes it a critical document for guiding practice and policy.
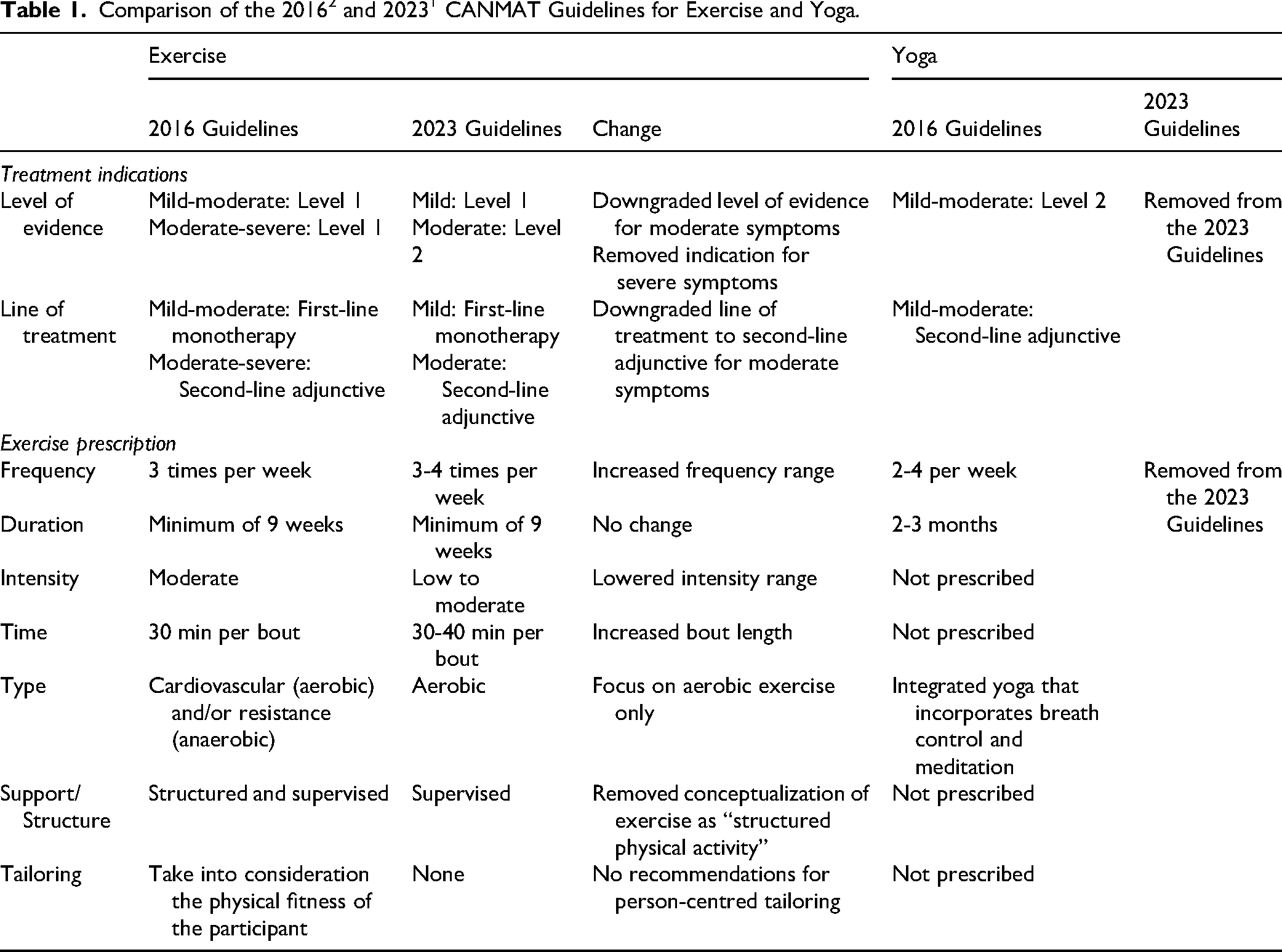
We were pleased to see continued recognition of exercise-based treatment for depression in the Guidelines. Exercise remains an under-utilized treatment modality,3,4 and the Guidelines play a vital role in raising awareness and informing evidence-based exercise prescription. However, the Guidelines feature several significant changes to the previous recommendations (Table 1). Critical changes include the downgrading of evidence and the demotion of exercise to a second-line adjunctive treatment for moderate depression, while retaining it as a first-line option for mild cases. Alongside these, misleading statements regarding safety and efficacy were introduced. These changes were not explicitly communicated to readers and it is not apparent how these decisions were made, calling the review process into question.
Comparison of the 20162 and 20231 CANMAT Guidelines for Exercise and Yoga.
Literature Review
To better understand the CANMAT exercise prescription, our laboratory group conducted a review of the Guidelines’ 964 references. We identified 29 manuscripts related to exercise, of which 9 were eligible for this review (Supplemental References A-I). Please see Table 2 for a summary of major findings, and the Supplemental Files for an overview of the review process and references.
Summary of Major Outcomes for Meta-Analyses of Exercise-Based Treatment for Depression.
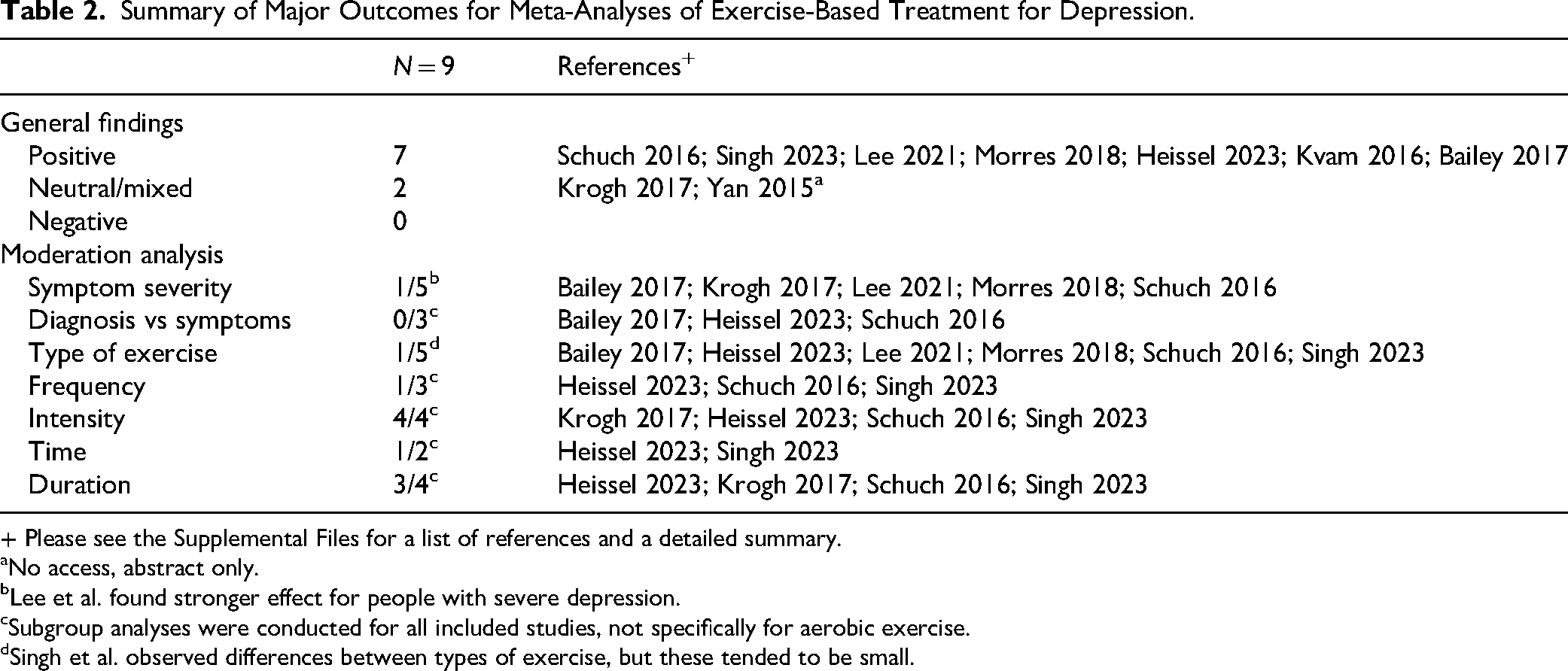
+ Please see the Supplemental Files for a list of references and a detailed summary.
No access, abstract only.
Lee et al. found stronger effect for people with severe depression.
Subgroup analyses were conducted for all included studies, not specifically for aerobic exercise.
Singh et al. observed differences between types of exercise, but these tended to be small.
Level of Evidence
The Guidelines define Level 1 i evidence as “meta-analysis with narrow confidence interval”; and Level 2 evidence as “meta-analysis with wide confidence intervals.” However, the terms “narrow” and “wide” are not quantitatively defined by CANMAT, leaving its interpretation subjective. This subjectivity becomes problematic in the recommendations for exercise: It is not clear why Level 1 evidence is assigned to the consideration of exercise as a treatment for mild depression, but then Level 2 evidence is assigned to justify the use of exercise for moderate depression—especially when both conclusions draw from the same body of meta-analytic evidence.
Symptom Severity
The Guidelines recommend exercise as a first-line ii monotherapy for mild depression and a second-line adjunctive treatment for moderate depression. This distinction suggests that the effectiveness of exercise is believed to reduce as depressive symptoms become more severe. However, the evidence does not support this assumption. Five systematic reviewsA,C,E,F,G conducted analyses on whether the severity of depressive symptoms moderated the effect of exercise. FourA,C,F,G found no effect of symptom severity, while oneE reported larger effects for greater symptom severity. While it is noteworthy that comparatively less research has examined exercise for people with severe depressive symptoms, there is a growing body of trials with this population. In short, exercise appears to be effective across a range of symptom severities (see also Noetel et al. 5 ). The evidence does not support the recommendation that exercise can only be used as a second-line adjunctive treatment for moderate symptoms, and not used at all for severe symptoms.
Comparison With Conventional Treatments
The Guidelines state, “There is stronger evidence for the efficacy and safety of pharmacotherapy and psychotherapy compared to exercise” (p. 654). While exercise-based treatment for depression is a comparatively young field, there is increasing evidence of exercise's impact. Meta-analyses cited by the Guidelines suggest that exercise is comparableD,H to pharmacotherapy and psychotherapy in treating depression; that its number needed to treatB is equivalent or superior to conventional treatments; and that it has relatively low attrition rates.A,F Indeed, publication bias estimates suggest an under-estimate of exercise's effect.B,G These results align with more recent publications, including a 2026 Cochrane review 6 which found exercise to produce meaningful albeit modest effects (SMD ≈ −0.46) in methodologically robust trials. Crucially, this effect is comparable to those often seen for conventional treatments for depression.
The Guidelines do not provide any references to indicate increased safety risk. With important exceptions (e.g., active eating disorder), mental illness does not present an absolute contraindication7,8 to exercise. When compared to pharmacotherapy, 9 individuals receiving exercise-based treatment report fewer adverse events like dizziness, drowsiness, and agitation. Exercise tends to be associated with minor adverse events,B,C such as muscle pain and fatigue; however, these transitory unpleasant experiences are common in exercise initiates, tend to reduce with time and physical conditioning, and can be mitigated with a tailored and supervised exercise program. While no health intervention is risk-free, the health benefits of exercise—such as improved cardiometabolic health and brain health—tend to outweigh potential risks.
Exercise Dose
The exercise prescription presented by the Guidelines is inconsistent with 7 comprehensive reviews.A,B,C,E,F,G,H For instance, the Guidelines’ narrow focus on aerobic exercise disregards evidence showing that different types of exercise—including strength and balance/flexibility—are effective. Similarly, the recommendation for “light-moderate” intensity is puzzling, as the literature consistently finds that moderate-to-vigorous intensities are associated with greater benefits. 5 Lastly, while a minimum duration of 30 min is supported, there is no clear evidence favouring the specific 30 to 40 min per bout prescribed by the Guidelines.
In short, there is limited basis for the current recommendations in terms of type (aerobic), intensity (light-moderate), or bout (30-40 min). By presenting a rigid prescription that lacks a transparent evidence base, the Guidelines create a significant disconnect between its recommendation and the scientific literature. The critical issue is not to define an alternative dose, but rather to question the opaque process that resulted in such a specific and seemingly arbitrary conclusion.
Structure and Supervision
The Guidelines omit the term “structured” while retaining the concept of “supervision” in their recommendations. Exercise programs are said to be “structured” if they follow a plan, and “supervised” if they involve oversight from an exercise professional (e.g., kinesiologist, clinical exercise physiologist). Four meta-analysesA,B,E,G identified supervised exercise as being more beneficial than unsupervised exercise. However, in the evidence base, supervision is almost always applied to a structured program, with participants asked to follow a specific exercise program (e.g., 3 × 30-min brisk walks/week). By selectively removing the qualifier of “structured,” the Guidelines have fundamentally misinterpreted the evidence. This omission of “structured” reframed exercise as a general lifestyle suggestion rather than an intentional, prescribed, evidence-based treatment, which may further undermine its clinical adoption.
Conclusions
We acknowledge that it is not standard practice to prescribe exercise for depressive disorders, and that existing health systems tend not to facilitate a referral process. However, efforts should be made to enhance knowledge translation, for instance, increasing awareness of existing evidence and supporting the implementation in clinical practice, rather than downgrading this option to a second-line treatment. Our lab has been working to remedy these gaps, including developing an Exercise and Depression Toolkit (https://exerciseanddepression.ca/) for health care providers and launching a professional training program in collaboration with the Canadian Society for Exercise Physiology (csep.ca/csep-certification/csep-exercise-and-depression-specialization/). We have also piloted models for patient referral systems in partnership with local community-based fitness facilities. These programs have been marked by success, with high rates of recruitment and good adherence (e.g., 14 participants recruited within 2 weeks, 11 participants completed 10 ). In short, it is feasible to deliver tailored physical activity interventions to people living with depression.
In conclusion, we are perplexed regarding the CANMAT's Guidelines for exercise-based interventions for depression. The available evidence speaks to the benefits of exercise across symptom severities, with all types of exercise associated with benefit, and generally greater benefit with more vigorous forms of exercise. Not only is exercise comparable to antidepressant medications and psychotherapy in terms of its impact; but it has a proven safety profile with notable positive side-effects; and demonstrates feasibility within community settings—including the option of group-based programming. It may be particularly appealing to individuals not interested in conventional mental health treatments, or those traditionally difficult to reach (e.g., men, racialized communities). We hope that future Guidelines will better reflect the state of the field and position exercise-based interventions as another evidence-based treatment option for people living with depression.
Supplemental Material
sj-docx-1-cpa-10.1177_07067437261464744 - Supplemental material for Revisiting the Exercise Recommendations in the 2023 CANMAT Guidelines for Major Depressive Disorder
Supplemental material, sj-docx-1-cpa-10.1177_07067437261464744 for Revisiting the Exercise Recommendations in the 2023 CANMAT Guidelines for Major Depressive Disorder by Madelaine Gierc, Yiling Tang, Victoria Whiteford, Daria Sosna, Yawei Wei and Guy Faulkner in The Canadian Journal of Psychiatry
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicts of Interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Gierc received Michael Smith Health Research BC Research Trainee funding for her work on exercise-based treatments for depression, and has received speaker honorariums for presentations on the topic. Dr Faulkner has received a Canadian Institutes of Health Research Foundation Award for his work on exercise-based treatments for depression. Dr Faulkner contributed to the 2016 Guidelines. 2 The Population Physical Activity Lab received funds from the Canadian Society for Exercise Physiology to develop the Exercise and Depression Specialization.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.