
Abstract
In this paper, we apply an intersectional perspective and test whether resource substitution, which predicts that education will be more strongly related to the health of women than men, is operating among adults included in the 2014 Study of Health and Migration in Mexico (SHMM). Findings revealed modest and somewhat contradictory evidence regarding the potential role of resource substitution. For Mexican women, rates of elevated waist circumference are very high regardless of education level, but for hypertension, there is a strong, negative association with education even after adjustment for controls. Different patterns emerge for Mexican men as regression models show that the probability of both elevated waist circumference and hypertension is higher among the more educated. Overall, results suggest that education is only health protective for women’s risk of hypertension. In sum, this work highlights gender specificity in the relationship between education and health in Mexico, and that this relationship varies by health outcome.
Introduction
Low- and middle-income countries increasingly bear the global burden of chronic disease (Abegunde et al. 2007; Yusuf et al. 2001). As a large, middle-income country, Mexico has seen rising rates of obesity, diabetes, metabolic syndrome, and cardiovascular disease (Aguilar-Salinas et al. 2004; Kuri-Morales et al. 2009; Rivera et al. 2002; Rojas et al. 2010), often accompanying processes of globalization, epidemiological and nutrition transitions, and changes in physical activity. Contemporaneously, disparities in chronic disease may be widening with increasing economic development in Mexico (Smith and Goldman 2007), disproportionately impacting some sociodemographic groups.
In this paper, we examine how gender and education relate to two physical health conditions among Mexican adults that are costly, associated with numerous medical conditions, and predictive of mortality: elevated waist circumference (i.e., a primary indicator of abdominal obesity) and hypertension. Gender disparities across chronic medical conditions are well documented (Read and Gorman 2010), and research has established that socioeconomic status (SES), including education, operates as a fundamental cause of health (Link and Phelan 1995; Phelan and Link 2005). At the same time, scholars increasingly recognize that social identities intersect to shape health disparities (Bowleg 2012) and that assessments of health must consider how specific intersectional positions, including those reflecting the intersections of gender and education (e.g., highly educated women, lower educated men), relate to well-being. A small but growing number of studies have shown that the negative relationship between education and health conditions tends to be stronger among women (Ross, Masters, and Hummer 2012), including for waist circumference (Hermann et al. 2011) and hypertension (Gorman and Porter 2011). But to date, most research on this topic has been conducted in the United States and other developed nations, with few studies examining whether health status operates similarly by gender and education in Mexico (see works by Smith and Goldman 2007; Wong 2003). Patterns in Mexico may differ from the United States, as socioeconomic health gradients have been shown to be flatter in emerging countries and more complex depending on the health outcome (Buttenheim et al. 2010).
We explore these issues among adults in the 2014 Study of Health and Migration in Mexico (SHMM) and ask whether gender moderates relationships between education and physical health conditions among Mexican adults. We focus on two health outcomes, elevated waist circumference and hypertension, that were measured during the interview by trained medical personnel. We examine prevalence rates for each health condition and consider the intersection of gender and education. We also utilize logistic regression models to adjust for potential confounders and mediators of these relationships, including demographic characteristics, U.S. exposure, noneducation aspects of SES, health behaviors, and stress and support. Overall, our findings build upon existing scholarship exploring whether and how education differentially relates to health outcomes among men and women, including assessment of the role of potential mediating factors contributing to gendered health patterns among Mexican adults, while also highlighting the importance of replication in social science studies of health outcomes (Freese 2007; Freese and Peterson 2017).
Education as a Fundamental Cause of Disease
In their seminal work, Link and Phelan (1995) theorize that social position, determined by SES, is a fundamental cause of health because of its persistent link to health across time, contexts, and diseases. As a result, individuals with more resources or higher levels of SES are better situated to access knowledge and take advantage of treatment/prevention options to benefit their health (Phelan and Link 2005). Scholars have examined education as a fundamental cause of disease and highlight how it differs from other forms of SES, such as income (Herd, Goesling, and House 2007; Mirowsky and Ross 2017). As a key factor shaping positionality in the stratification system, education increases the odds of (good) employment and higher incomes (Mirowsky and Ross 2003). Education has other qualities that also make it particularly relevant for health: it encompasses learning, problem solving, critical thinking, and productive habits and skills (Ross and Mirowsky 2010b), which facilitate “learned effectiveness that enables self-direction toward health” (Mirowsky and Ross 2003:6).
Higher educational attainment has a strong and consistent association with favorable health, morbidity, and mortality and influences health status through a variety of mechanisms (e.g., improved health lifestyle; see Cutler and Lleras-Muney 2006). In this paper, we examine how education relates to elevated waist circumference and hypertension for several reasons. Noncommunicable disease risks, including hypertension and elevated weight, are significant contributors to the global burden of disease. Worldwide, hypertension followed by high body mass index are leading risk factors for mortality and years of healthy life lost (Lim et al. 2012). In Mexico, high body mass index is the primary contributor to years of healthy life lost among women (Forouzanfar et al. 2016). Indeed, Rtveladze and colleagues (2014) found that in 2010, two-thirds of men and three-quarters of adult women in Mexico were either overweight or obese, and Acosta-Cázares and Escobedo-de la Peña (2010) showed that among insured women aged 20 years and above in Mexico, obesity is the most prevalent risk factor for cardiovascular disease. Their analysis also indicated that Mexican men and women had a similarly high age-adjusted prevalence of hypertension (at 29 percent). Two recent studies have reported a similar prevalence rate for hypertension among Mexican adults, at 31 percent (Basu and Millett 2013; Campos-Nonato et al. 2013), with a substantial proportion unaware of their condition prior to blood pressure testing at interview. As preventable causes of substantial disease burden and premature mortality, our focus on how these health conditions associate with education among Mexican adults is timely.
Despite the robustness of the education and health relationship (Herd et al. 2007; Link and Phelan 1995; Mirowsky and Ross 2017; Ross and Mirowsky 2010a; Ross and Wu 1995), intersectionality theory challenges the notion that the health benefits of education apply equally across social groups. Social identities are interconnected, and individual experiences and outcomes (including health status) are shaped by the specific intersectional position that a person holds (Bowleg 2012; McCall 2005). As discussed by Olena Hankivsky (2012), differences among men and among women are often as prominent as differences between men and women. If systems of inequality relating to gender (sexism) and education (classism) are intertwined and transformed at their intersection, this implies our understanding of how education relates to health status will vary among men and women due to the multiplicative nature of how social characteristics relating to status and well-being operate. Although there are methodological challenges associated with conducting intersectional research (Bowleg 2008), systematically comparing how health outcomes differ across the intersections of gender and education allows us to not only examine whether health status is poorest among those who simultaneously hold multiple disadvantaged statuses (i.e., low-educated women), it also permits an assessment of health outcomes among persons who concurrently hold social positions that are both marginalized and privileged (i.e., low-educated men) (Bowleg 2012; McCall 2005).
Overall, previous studies have documented a stronger negative association between education and physical health conditions and impairment among women (Cutler and Lleras-Muney 2006; Ostrove and Adler 1998; Ross et al. 2012; Ross and Mirowsky 2010b; Thurston et al. 2005). In seeking to explain this pattern, the resource substitution model argues that the resources constituting SES can substitute for one another. In other words, when one resource is absent, the presence of other resources reduces the negative impact of the absence and also increases the importance of present resources (Ross and Mirowsky 2010b). This is likely the case for education because it is not dependent on participation in the labor force, it reflects an individual’s status rather than household income and is relatively stable over the adult life course (Thurston et al. 2005). As women generally have fewer socioeconomic resources that can be substituted than men, the implication of resource substitution is that the education and health relationship is stronger and more positive among women. Studies using U.S. data support the resource substitution model for outcomes including physical impairment, self-rated health, and heart disease (Ross et al. 2012; Thurston et al. 2005). For example, physical impairment declines more steeply with educational attainment for women, such that gender gap in disability is nonexistent among college-educated adults (Ross and Mirowsky 2010b).
An alternate model, reinforcement of advantage, maintains that advantaged groups are positioned to see the greatest returns from their resources. This allows higher status groups to utilize their resources to reinforce and extend their advantage (Ross and Mirowsky 2010b). In terms of the education and health association, the result is that men would see greater benefits/gains from education than women. Although studies of mortality have found support for this model (the education and mortality association is stronger for men; see Ross et al. 2012 for an example), studies of physical health tend to find more support for resource substitution.
Although educational achievement in Mexico is quite similar between men and women (Population Reference Bureau 2016), other aspects of socioeconomic hierarchies in Mexico remain organized around gender (Fernández-Kelly 2008). A Mexican narrative of patriarchal ideology reinforces structural inequalities that women experience (Hondagneu-Sotelo 1994). Although there are signs of change, Andrews and Shahrokni (2014:150) discuss how changes in Mexican women’s access to education, employment, and consumption are “patriarchal accommodations” that reflect continuing investment in gender differences among men, women, and the state. Masculine gender norms in Mexico necessitate that men provide economically for their family, which shapes power dynamics and resource and labor distribution within a household. Although many Mexican households rely on the wages of women working in the informal or formal economy, women are paid lower wages relative to men and opportunities intended to increase women’s involvement in the labor force, such as maquiladoras, are structured to buttress the existing gender hierarchy (Fernández-Kelly 2008; Salzinger 2003). According to resource substitution, educational attainment may be more tightly associated with health for Mexican women because of their otherwise disadvantaged socioeconomic position and lack of other resources that can operate as SES substitutes for education.
Education, Health, and Gender Associations
Previous research exploring relationships between education and the health conditions examined in this study (hypertension and elevated waist circumference) provide some evidence of gender moderation. Using a cross-national European data set, Hermann and colleagues (2011) observed a steeper negative association between elevated waist circumference and education for women than men. Gorman and Porter (2011) found a similar pattern for hypertension among older adults in two U.S. data sources, as does Veenstra (2013) who found a strong, negative association between education and hypertension among Canadian women, but not men.
A limited number of studies examine the gender-SES gradient in health in Mexico (Wong 2003). In one study, Barquera and colleagues (2010) descriptively found a higher prevalence of hypertension among Mexican women than men. They also showed that rates of hypertension varied by education, but they did not examine whether these patterns differed by gender. In a more recent paper examining data from the 2006 Mexican National Health and Nutrition Survey, Beltrán-Sánchez, Palloni, Riosmena, and Wong (2016) found somewhat elevated predicted prevalence ratios for high blood pressure and elevated waist circumference among low versus highly educated adults. Supplementary results presented in an online appendix revealed significant moderation by gender, with steeper education gradients found among women than men. Descriptively analyzing the same data, Barquera and colleagues (2009) found that while highly educated Mexican women had lower mean waist circumferences than women with less education, highly educated Mexican males had higher mean waist circumferences than men with less education, suggesting a lack of consensus to date. Importantly, these two studies use different thresholds to define elevated waist circumference, with Barquera and colleagues using lower values. Moreover, these studies do not account for confounding variables. Given the findings from both Beltrán-Sánchez and colleagues (2016) and Barquera and colleagues (2009), our paper offers an important replication to this small but growing literature. We explore how gender shapes the education and health relationship utilizing a more recent sample of Mexican adults to confirm a stronger relationship between education and hypertension among Mexican women, and that the relationship between education and elevated waist circumference operates in different directions for women (negative) and men (positive).
Altogether, previous research suggests that gender will moderate relationships between education and hypertension and elevated waist circumference among Mexican adults. Thus, our analysis will test the following:
As some scholarship has found support for an alternative explanation, we also test the following hypothesis:
Mechanisms Linking Education and Health Outcomes
Education influences health status through a variety of pathways, including more favorable economic conditions, additional social psychological resources, and improved lifestyle (Ross and Wu 1995); we evaluate the mediating role of each. First, aspects of SES beyond education, such as income, have strong negative relationships with hypertension and waist circumference (Keenan and Rosendorf 2011; Salsberry, Corwin, and Reagan 2007), and men in Mexico are socioeconomically advantaged relative to women (Fernández-Kelly 2008). As such, these noneducation aspects of SES may account for some of the gender difference in how education relates to physical health conditions.
Second, social psychological resources are highly relevant for health, including the negative health consequences of the physiological response to chronic stressors (Thoits 1995). Various stressors are associated with this physiological response (e.g., neighborhood context, violence exposure), which low-SES groups experience more frequently (Adler and Snibbe 2003; Everson et al. 2002; Roux, Jacobs, and Kiefe 2002). Members of lower status groups (e.g., women) are also more vulnerable/reactive to selected forms of stress (Seeman 2000; Thoits 1995).
Third, health behaviors and lifestyle factors have strong associations with health conditions. Hypertension is more prevalent among smokers and heavy drinkers (Briasoulis, Agarwal, and Messerli 2012; The National High Blood Pressure Education Program 2003) and mean waist circumference is highest among heavy drinkers and former smokers (Ford, Mokdad, and Giles 2003; Koloverou et al. 2015). Studies highlight the role physical activity plays in reducing hypertension and central adiposity risk (Börjesson et al. 2016; Hegde and Solomon 2015; Pedersen and Saltin 2015), and poor self-rated health is positively correlated with numerous chronic conditions (Singh-Manoux et al. 2006).
As we examine data on adults from a region in Mexico that sends a large number of migrants to the United States, we also adjust for the influence of U.S. exposure with measures of migration experience and English ability. Gender differences in health for migrants from Mexico to the United States are greater among adults with the least education, since Mexican women are more positively selected into U.S. migration based on health status than men (Hamilton 2015). Furthermore, adults in Mexico have a higher prevalence of high blood pressure/medication use and elevated waist circumference than Mexicans living in the United States (Barquera et al. 2010; Ford et al. 2003; Rojas et al. 2010), and some evidence suggests that acculturation is positively associated with blood pressure and waist circumference among Mexican American women (Vella et al. 2011).
Finally, our models include demographic controls. Although evidence is limited, married adults on average have better health and lower blood pressure. Marital relationships provide a variety of supports (e.g., financial, emotional) and encourage healthy behaviors (Holt-Lunstad, Birmingham, and Jones 2008; Kiecolt-Glaser and Newton 2001; Troxel et al. 2005), though the relationship with body weight appears dependent upon gender and ethnicity (Sobal, Hanson, and Frongillo 2009). These health conditions are also age graded, as the risk of hypertension and elevated waist circumference increases with age (Ford et al. 2003; Vasan et al. 2002). For women, having biological children is associated with metabolic changes likely associated with increased risk of hypertension and central adiposity related to waist circumference (Mosca et al. 2011). For men, these associations are less clear and likely attributable to health behaviors (Hardy et al. 2007), but childless men may face increased health risk (Eisenberg et al. 2011).
Overall, we apply these findings from previous scholarship on the mediating factors linking education to health, as well as evidence that education has a stronger relationship to health status among women (i.e., moderation), and posit our final hypothesis:
Data and Method
We draw on data from the 2014 SHMM. This project randomly surveyed Mexican adults (aged 18+ years) living in a medium sized town in the state of Guanajuato, located in central Mexico. The sample was designed to capture an equal number of men and women as well as adults with and without U.S. migration experience. Using the 2010 Instituto Nacional de Estadistica y Geografia (INEGI) data, census blocks for the municipal area were divided into two groups based on size (large and small blocks). All small blocks were sampled while large blocks were chosen by simple random sampling. In each block, systematic random sampling was used to select a predetermined number of households per block (De Vaus 2002). Following, an adult from each household was randomly chosen to interview. In total, 480 adults (aged 18+ years) participated in the study (response rate: 58 percent).
Participants completed a sociodemographic questionnaire that included questions on migration histories, self-reported medical conditions, SES, stress, and violence and a noninvasive physical assessment administered by a health professional. All surveys and physical assessments were conducted in the respondent’s home and in Spanish. Of the 480 respondents, our analytic sample excluded seven women who were pregnant or breastfeeding and an additional 30 cases were excluded because they declined to participate in the physical health assessment. The final analytical sample included 426 adults with complete data (out of a possible 443; a loss of 3.8 percent of cases). All respondents were born in Mexico, and 95 percent of respondents included in the analytic sample were born in the state of Guanajuato.
Measures
We examine two physical health outcomes. First, during the physical assessment, waist circumference was measured using a flexible tape measure positioned horizontally at the narrowest part of the respondent’s abdomen. Following established guidelines (Alberti et al. 2009), women were categorized with abdominal obesity, or elevated waist circumference, at a circumference at or above 88 cm, and men at or above 102 cm. Second, following established guidelines (Alberti et al. 2009), respondents are hypertensive if they had a measurement of 140 or greater systolic blood pressure or 90 or greater diastolic blood pressure, based on the average score across two blood pressure measurements. 1 Alternatively, respondents are also classified as hypertensive if they reported taking any antihypertensive medications at interview. Correlations of these health outcomes were minimal by gender and gender-by-educational attainment (available from authors upon request). We intentionally focus on elevated waist circumference rather than obesity because of the metabolic risks of excess abdominal fat even at a normal body weight and its association with a range of comorbidities such as cancer, heart disease, and diabetes (Pischon et al. 2008; Wei et al. 1997). It is also considered by medical professionals and health researchers to be a critical component of Metabolic Syndrome. Among our sample, elevated waist circumference and BMI are correlated, as expected (r = .56). In addition, the study of elevated waist circumference extends the empirical examination of the gender gradient in health in Mexico.
Our independent measures of interest include gender (1 = male, 0 = female) and educational attainment (highest level of completed schooling, where 1 = secondary, high school, or college, and 0 = less than secondary). 2 In regression models, we adjust for the confounding influence of factors shown to be related to gendered health disparities in past research. Demographic characteristics include age of the respondent (range = 18–86 years of age), marital status (1 = married or cohabitating, 0 = other), and whether the respondent has children (1 = yes, 0 = no). We also adjust for measures of U.S. exposure/acculturation: respondent ever lived in the United States for three months or more (1 = yes, 0 = no), and whether they have any English language ability, contrasting very good, good, or not good English language ability (=1) against no English ability (=0). 3
Beyond education, two additional measures of SES are included. Respondents assessed their socioeconomic standing on a nine-rung ladder, relative to others in Mexico (1 = poorest; 9 = richest). We also include a measure of whether the respondent reports feeling as if they have enough money to meet their needs (1 = just enough or more; 0 = not enough). Sensitivity analyses (not shown) included additional SES measures such as income and five-year economic outlook, but they were not included since they did not change the substantive conclusions and resulted in a loss of cases due to missing data.
Measures of health behavior and status are each constructed as a dichotomy contrasting healthy versus less healthy behavior, including the following: never smoked tobacco, does not currently drink (defined as never having a single drink within the last 12 months), and engages in a high level of physical activity (defined as participating, during an average week, in vigorous physical activity/exercise for 30 minutes or more at least three times per week). We also adjust for self-rated health, based on respondents rating of their overall health status (1 = fair or poor, 0 = good, very good, or excellent health). In addition, please note that in regression models predicting hypertension status, we also adjust for elevated waist circumference (Huxley et al. 2010).
We also adjust for measures reflective of stress and social support. First, we include an indicator of how safe respondents felt in their community. This measure, perceptions of community insecurity, ranges from 1 to 3, where higher values indicated stronger feeling of being unsafe (1 = very safe/safe, 2 = somewhat unsafe, and 3 = unsafe). Second, respondents rated how frequently they receive their needed amount of emotional support (contrasting those who report always receiving necessary support against those who responded usually or sometimes, and rarely or never).
Analysis Plan
In Tables 1 and 2, we present characteristics of our analytic sample and prevalence rates for both health conditions stratified by gender and education. Next, we estimate logistic regression models predicting both health outcomes in Table 3. All descriptive statistics and models are unweighted. For both outcomes, we present two models: (1) a baseline model that only includes the interaction between gender and education, and (2) a model that includes the Gender × Education interaction and adjusts for all controls. We used the method developed by Karlson, Holm, and Breen (2012) to formally test for mediation in a logistic regression model using the KHB command in Stata 14 (Kohler, Karlson, and Holm 2011). For ease of interpretation, baseline and adjusted interaction models were graphed using the Margins command in Stata 14 (see Figures 1 and 2).
Sample Characteristics: Mexican Men and Women, by Education Level.
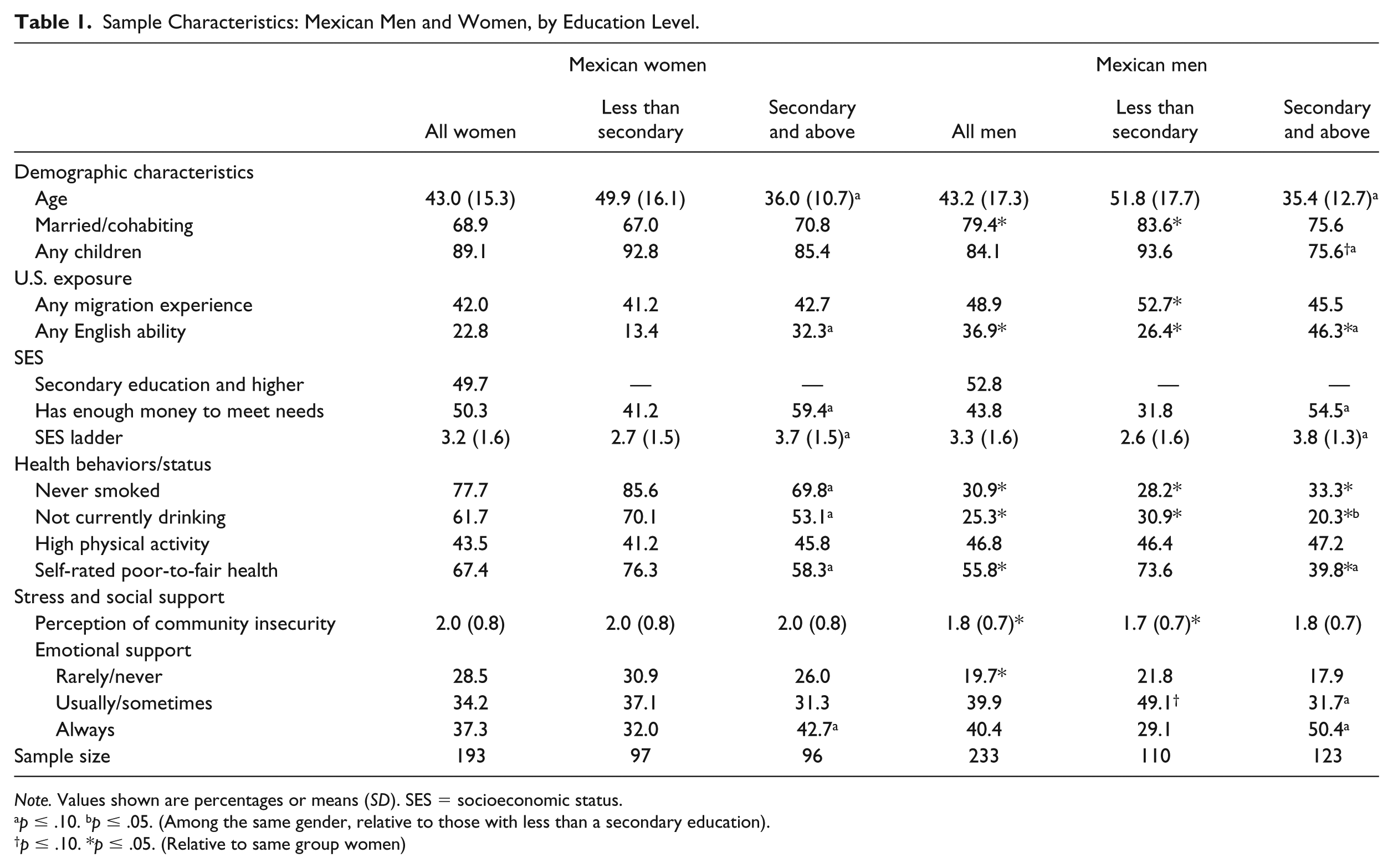
Note. Values shown are percentages or means (SD). SES = socioeconomic status.
p ≤ .10. bp ≤ .05. (Among the same gender, relative to those with less than a secondary education).
p ≤ .10. *p ≤ .05. (Relative to same group women)
Prevalence of Health Conditions by Gender and Education among Mexican Adults (Mean or %)
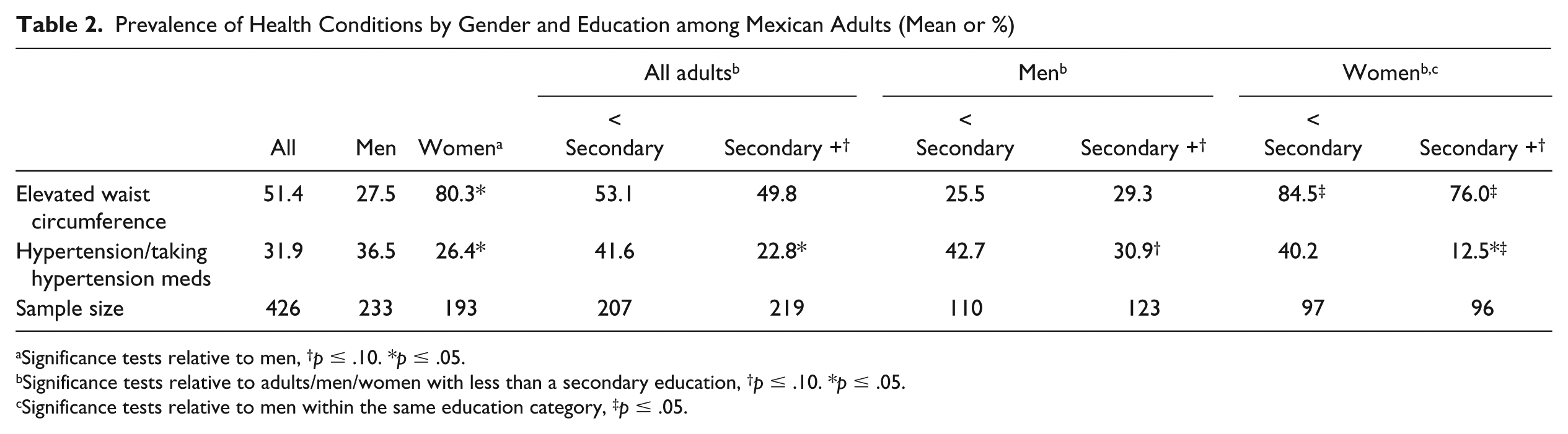
Significance tests relative to men, †p ≤ .10. *p ≤ .05.
Significance tests relative to adults/men/women with less than a secondary education, †p ≤ .10. *p ≤ .05.
Significance tests relative to men within the same education category, ‡p ≤ .05.
Coefficients and Standard Errors from Logistic Regression Models Predicting Elevated Waist Circumference and Hypertension (N = 426).
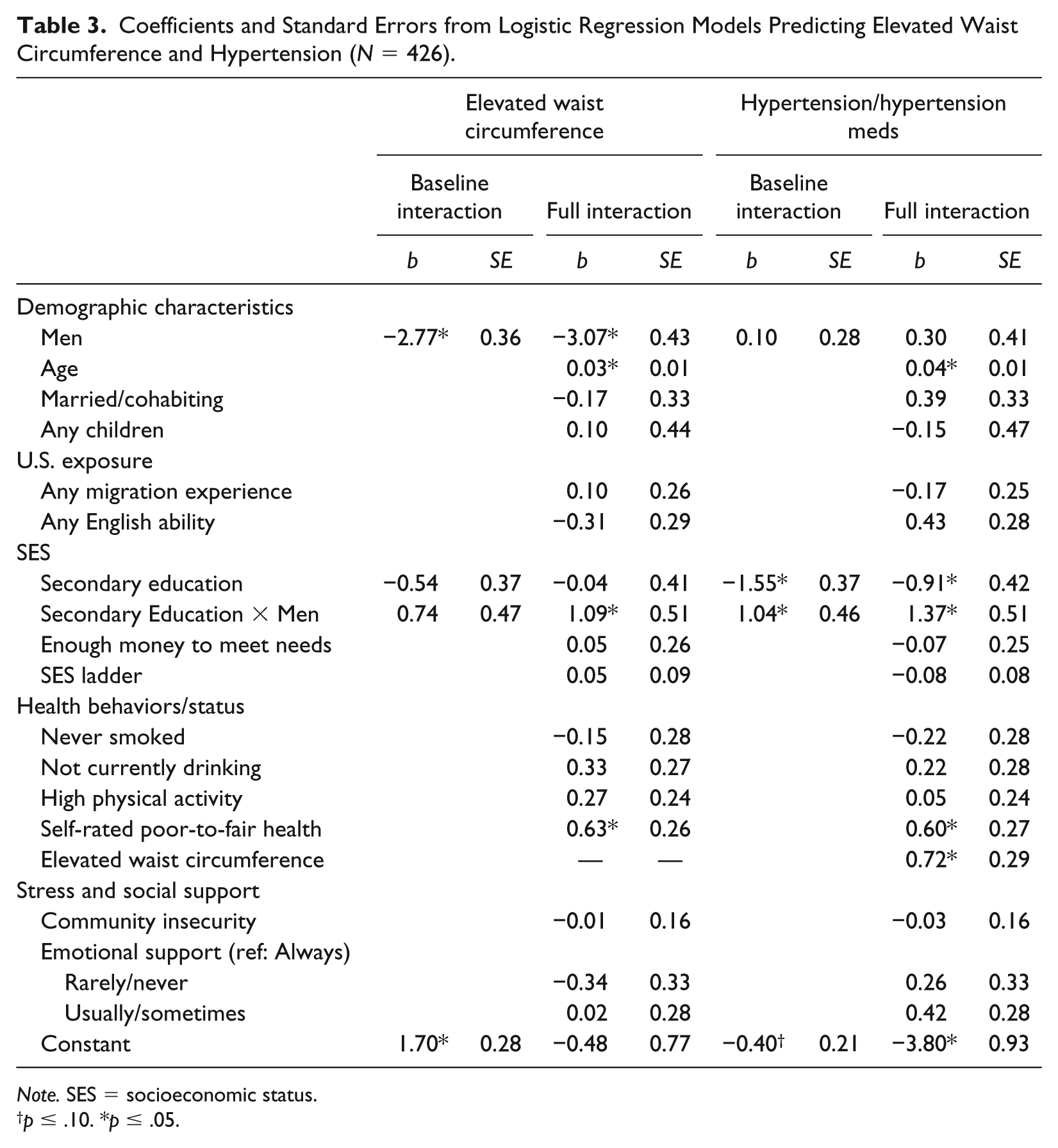
Note. SES = socioeconomic status.
p ≤ .10. *p ≤ .05.
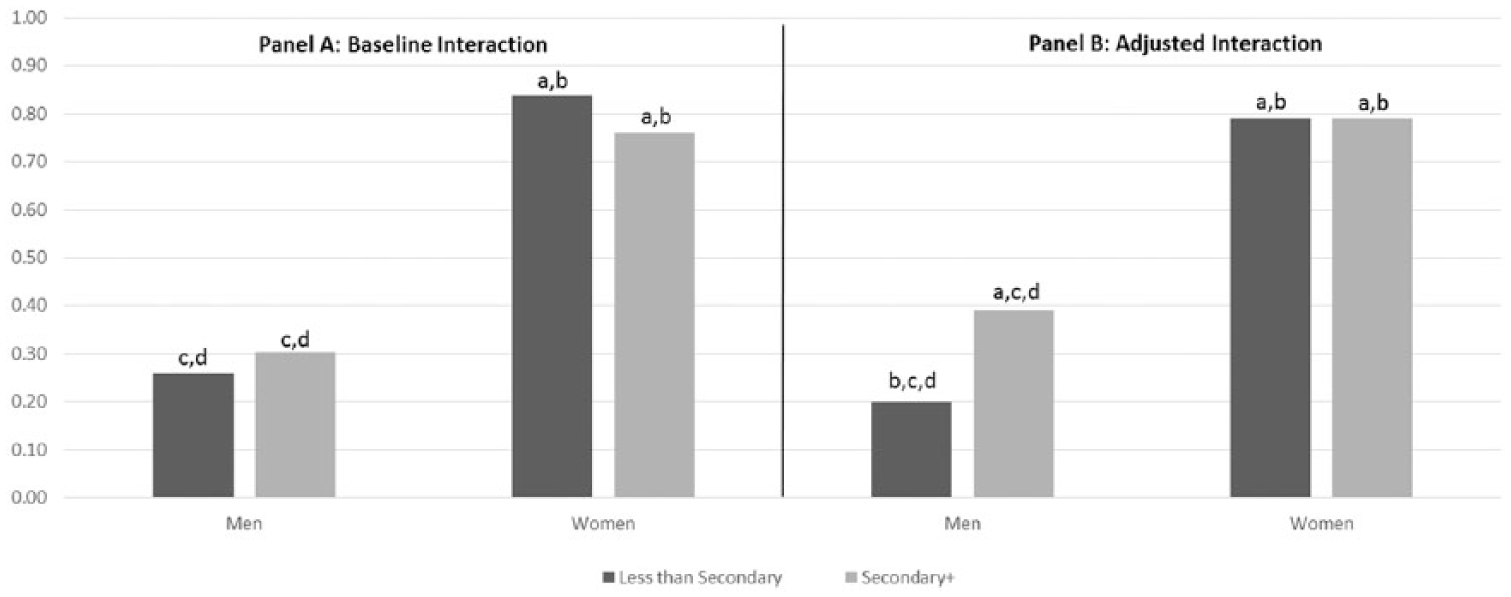
Baseline and adjusted predicted probabilities of elevated waist circumference, by gender and educational attainment.
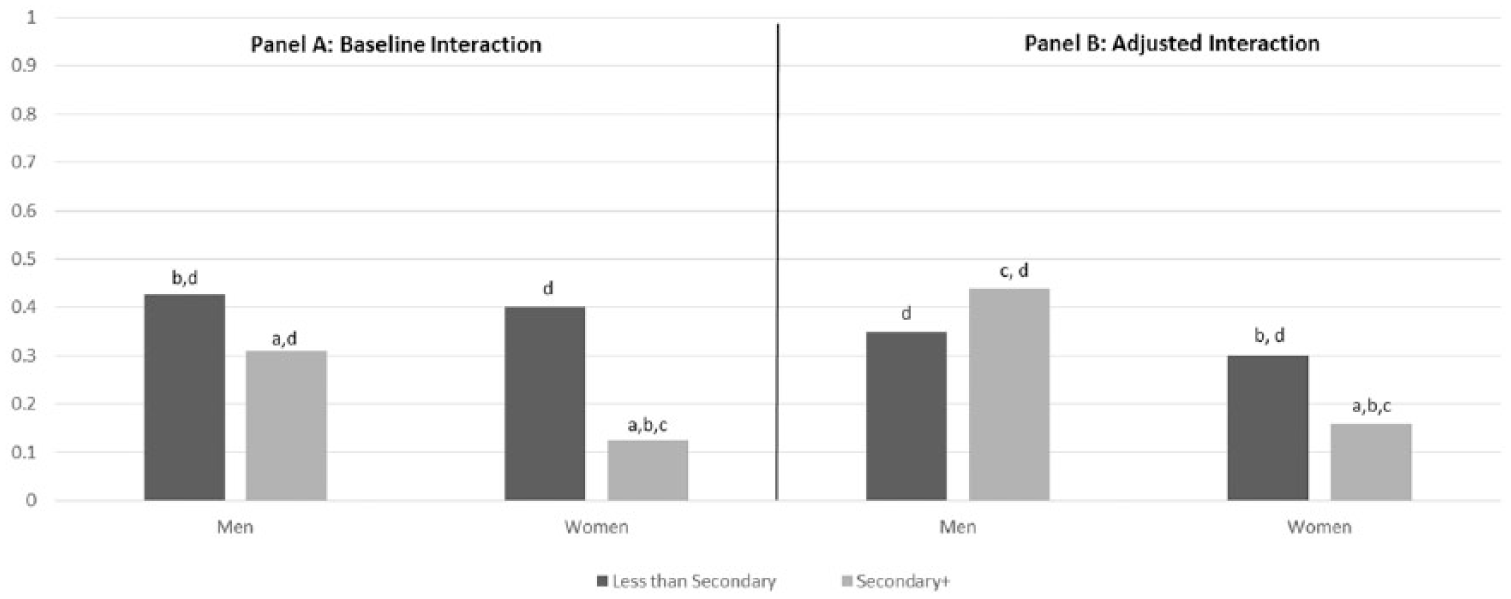
Baseline and adjusted predicted probabilities of hypertension, by gender and educational attainment.
Results
Table 1 shows substantial evidence that sample characteristics vary by both gender and level of completed schooling. Among men and women, those who did not complete secondary school are substantially older, on average, than adults with more education. We also see that a higher proportion of men are married or cohabiting at the time of interview, but this is only significantly different for men and women with less than a secondary education.
Turning to measures of U.S. exposure, regardless of education level, women report less English ability than men. At the same time, Table 1 shows for within gender comparisons, adults with at least a secondary education report significantly higher rates of any English ability. Among those with less than a secondary education, a significantly higher proportion of men (but not women) report any U.S. migration experience. Looking at completed schooling, and mimicking national patterns in Mexico (Population Reference Bureau 2016), men and women in our sample are very similar as about half completed at least secondary school. We see gender similarity for other aspects of SES as well.
In addition, on average, men engage in significantly worse health behaviors: they report more smoking and drinking than women. For drinking, rates of current use are significantly higher among men and women with more education. We see a similar pattern for smoking among women; but among men, rates of ever smoking are lower (but not significantly so) among the more highly educated. For self-rated health, there is no gender difference among adults with less than a secondary education; among those with more schooling, however, women report poor-to-fair health at a significantly higher rate than men. At the same time, reports of poor-to-fair self-rated health are significantly lower among men and women with more schooling.
Turning to measures of stress and support, Table 1 shows that among adults with less than a secondary education, women report more strongly than men that they feel insecure in their community. A significantly higher proportion of Mexican women also say that they rarely or never receive the amount of emotional support that they need. And among men and women, adults with more education report that they more regularly receive needed amounts of emotional support.
Overall, patterns in Table 1 illustrate that risk and protective factors related to health status vary by gender and education among this sample of adults in Mexico. Next, Table 2 presents prevalence rates for both health outcomes and shows that these conditions are prominent within this sample of adults. Just over half (51.4 percent) have an elevated waist circumference, and nearly one-third (31.9 percent) are either hypertensive at interview or are taking hypertension medication, mirroring national-level Mexican health survey data (see Barquera et al. 2009; Barquera et al. 2010; Beltrán-Sánchez et al. 2016).
Looking across Table 2, we see a mixed pattern by gender. Elevated waist circumference is extremely high among women (80.3 percent), compared with 27.5 percent of men. In contrast, a higher proportion of men are hypertensive. For education, rates of elevated waist circumference are similar between adults with and without a secondary education; however, hypertension is significantly elevated among adults who did not complete a secondary education.
Finally, Table 2 presents rates of each health condition stratified by both gender and education. Descriptively, it shows that education is a somewhat stronger stratifier of health conditions among Mexican women than men. We also see that within each education group, rates of elevated waist circumference are significantly higher among women than men, especially for women who did not complete secondary school; as a result, the gender gap in elevated waist circumference is larger among adults who did not complete secondary school (84.5 – 25.5 = 59.0) compared with those who did (76.0 – 29.3 = 46.7).
For hypertension, rates are higher among Mexican men and women with lower education—but the gap is much bigger for women (3.2 times higher for lower than higher educated women) than men (1.4 times higher for lower than higher educated men). Although the hypertension rate is very similar for men and women who did not finish secondary school, women with at least a secondary education experience much lower rates of hypertension than men of similar schooling.
Next, we turn to logistic regression models in Table 3. Looking first at models for elevated waist circumference, the baseline model mimics the descriptive results and shows that men are significantly less likely to have an elevated waist circumference than women. Although the interaction between Gender × Education is not significant in the baseline model, it emerges as significant after controls are added in the full model (with strong effects seen for age and self-rated health).
Figure 1 graphs the relationship between gender and education for elevated waist circumference. Panel A shows the interaction based on the baseline model, and Panel B shows the interaction after adjustment for controls. For Mexican women, Figure 1 shows that education does not differentiate their probability of elevated waist circumference. For both groups of women their predicted probability is very high, and adjusting for control measures had almost no influence on this relationship.
For Mexican men, however, Figure 1 shows that the probability of elevated waist circumference is significantly higher among those with more education—but only after adjustment for control measures. Adjusted probabilities of elevated waist circumference for men show a predicted probability of .20 for men without a secondary education and .39 for men who earned a secondary education or higher. Figure 1 also shows that within each education category, women experience a much higher probability of elevated waist circumference than men (.79 – .20 = .59 difference by gender among those with low education, compared with .79 – .39 = .40 difference by gender among those with high education); as a result, the gender gap in the adjusted probability of elevated waist circumference is larger among those with little formal schooling.
We also ran the KHB formal test for mediation (results available upon request), and results showed no statistically significant evidence of mediation between elevated waist circumference and gender, education, or Gender × Education.
Turning now to models for hypertension, Table 3 shows that the interaction between Gender × Education is significant in both models, but the relationship is strengthened with the addition of controls. Figure 2 graphs the interaction based on both models. For women, the probability of hypertension is significantly lower among those with at least a secondary education (see Panel A). Adjusting for controls reduces this gap somewhat, but it remains significant in Panel B (predicted probability for women with low education is .30, compared with .16 for women with higher levels of education). For men, the baseline graph in Panel A also shows that the probability of hypertension is significantly lower among those with at least a secondary education. In Panel B, however, adjusting for controls causes the probability of hypertension to decline for men with low education and to increase for men with more schooling. As a result, the relationship between education and hypertension reverses for Mexican men with adjustment for controls: those with low education have a lower probability (.35) of hypertension compared with men with more education (.44), but the gap is not significant.
Both panels of Figure 2 also show there is almost no gender difference in hypertension probability among those with low education; among those with at least a secondary education, however, men have a much higher probability of hypertension than women (.44 compared with .16 in the adjusted model). Finally, and similar to findings for elevated waist circumference, KHB tests showed no evidence of mediation for control measures between hypertension and gender, education, and Gender × Education.
Conclusion
In this paper, we built on previous research examining gender by education disparities in hypertension and elevated waist circumference. To date, the majority of research exploring whether and how the education-health relationship is gendered has been conducted in developed nations like the United States, with relatively little research conducted in Mexico and other locations. Previous research suggests that resource substitution may be operating, wherein education is more strongly related to the health of women than men; here we tested whether this was the case among a sample of adults living in Central Mexico.
In total, our findings revealed modest and somewhat contradictory evidence regarding the potential role of resource substitution. For elevated waist circumference, we found no evidence that education is protective for women. Rates of elevated waist circumference are very high, regardless of their education level. And while we found that the gender gap is larger among those with less schooling, we did not find evidence supporting resource substitution (see Hypothesis 1a). Instead, the smaller gender gap among the highly educated occurs because men’s probability of elevated waist circumference increases with education, especially after adjustment for controls (a finding that runs counter to the prediction of reinforcement of advantage and Hypothesis 1b). Interestingly, this finding for men does mimic patterns seen in Barquera and colleagues (2009), who analyzed data from the 2006 Mexican National Health and Nutrition Survey. Our research both replicates and extends prior research as their analysis only presented unadjusted associations while we conduct multivariate analyses. Given the amplification in men’s probability of elevated waist circumference in the SHMM following adjustment for controls in Figure 1, in supplemental analyses (not shown), we investigated which variables were responsible for this shift. Testing showed that adjusting for age was responsible for most of the shift. More specifically, due to the strong, positive relationship between age and elevated waist circumference, and the much older average age of men with lower versus higher education in our sample (see Table 1), adjusting for age removed this confounding influence on the predicted probabilities shown in Figure 1. Given the lack of additional mediation of the relationship between education and elevated waist circumference among men in our sample, future research could consider a wider array of explanatory mechanisms (e.g., diet, height, and other health behaviors) than are available in our data.
For hypertension, we found different gender patterns by education. Among women there is a significant, negative association between education and hypertension even after adjustment for controls. Among men, we found a more moderate negative association between education and hypertension in the baseline model. Yet after adjustment for controls, this relationship flipped: men with at least a secondary education had a higher (albeit nonsignificant) probability of hypertension than men without a secondary education. Supplemental tests (not shown) again revealed that age confounded the relationship and highlights the need for additional research of how education relates to health outcomes among men in Mexico, including why the education-hypertension relationship is positive among men and (as expected) negative among women. Altogether, findings for hypertension offer some support for the resource substitution hypothesis (Hypothesis 1a) but fail to support the reinforcement of advantage hypothesis (Hypothesis 1b) and are similar to Beltrán-Sánchez et al. (2016), who also found steeper education and hypertension gradients among women than men in Mexico.
Our research adds to mounting evidence of the prevalence of chronic medical conditions among Mexican adults and the gendered manner in which education can operate as a fundamental cause or prevention of disease. In recent years, Bowleg (2012) and others have argued that health research needs to examine how intersecting identities such as gender and SES shape health disparities. Therefore, our results using the SHMM bridge the literature by replicating prior research in Mexico and applying an intersectional framework to understand the education gradient in these important metabolic conditions among Mexican men and women. In discussing the challenges of incorporating an intersectional perspective into health research, Bauer (2014) emphasized the importance of comparing those who are multiply marginalized (e.g., low-educated women) with those who experience both privilege and marginalization (e.g., highly educated women and low-educated men) and those who are privileged (e.g., highly educated men) to make visible the health impacts associated with each intersectional position. Scholars have also discussed that the well-being of those who hold multiple marginalized positions (e.g., low-educated women) is not always the lowest, as they are often situated in positions of acute social invisibility. This “intersectional invisibility” is associated with both disadvantages and advantages, including the potential for lower exposure to active forms of oppression compared with low-educated men who are more “prototypical” members of marginal groups (Purdie-Vaughns and Eibach 2008; Veenstra 2013).
However, we find little evidence of this in our sample of Mexican adults. Low-educated men experience a similar probability of hypertension as low-educated women, even after adjusting for controls, and highly educated women have significantly lower odds of hypertension than men. At the same time, education failed to differentiate health risk among Mexican women with regard to elevated waist circumference. And once we adjusted-away the confounding effect of age, being a highly educated man in our sample was also not associated with a privileged position in terms of physical health. Overall, our results reveal a nuanced relationship between gender, education, and physical health for Mexican adults.
Following Ross and Wu (1995), we also evaluated the potential mediating connections between education and health but generally found little support for Hypothesis 2. As previously discussed, we saw an amplification of education and health relationships among men for both outcomes, and more generally, the formal KHB test did not yield evidence of significant mediation of gender, education, or the Gender × Education interaction in any model, confirming prior work finding that these commonly explored mediators are unable to fully explain these disparities (Cutler and Lleras-Muney 2006).
Although these findings have important implications for our understanding of the health risks faced by men and women of varying SES groups in Mexico, the work does have limitations. The SHMM was designed as a pilot study of one migrant-sending community in Mexico, resulting in a relatively small sample (480 surveys). Yet the results presented generally support findings of studies using larger and nationally representative surveys in Mexico (see Barquera et al. 2009; Barquera et al. 2010; Beltrán-Sánchez et al. 2016). Moreover, the fact that the study was conducted in one community is advantageous, in that we can treat the contextual impacts as fixed effects. Future research would benefit from expanded data collection in different types of communities (e.g., that vary by urbanicity or prevalence of emigration) and examine a broader array of physical and mental health outcomes.
The diverging gender and education patterns found in our analyses indicate that efforts to reduce the prevalence of these health problems will require gender- and education-specific interventions to maximize their potential effectiveness. That higher levels of educational attainment were not always found to be health protective is troubling and may signal important and impending public health implications. It may indicate that the SES-health gradient in Mexico is still shifting as their economy develops, or even that the SES-health gradient in Mexico is still shifting as their economy develops, or a flattening of the SES-health gradient such that a greater share of the population faces metabolic risks. More specifically, among women, rates of elevated waist circumference are very high, regardless of their level of completed schooling, suggesting the necessity of targeting policy initiatives to reach all women. This could include health promotion campaigns and interventions designed to improve diet and reduce weight among Mexican women in workplaces, schools, and religious institutions and interactions with health care providers. Men with higher levels of completed schooling face an elevated risk for both hypertension and elevated waist circumference and may lack awareness of their risks or inaccurately perceive their educational attainment to be health protective. This suggests that health promotion campaigns may need to specifically target highly educated men. Also of concern is that as educational attainment continues to increase in Mexico, more men and women will be at risk of hypertension and elevated waist circumference—a burden that may strain the health care system and economy. Furthermore, the confounding role of age for education and health patterns among Mexican men suggests that health policies and interventions to combat the rising prevalence of hypertension and elevated waist circumference will need to consider demographic shifts in educational attainment, increases in life expectancy, and the aging of the Mexican population (Andrade 2009; Angel, Vega, and López-Ortega 2017).
Footnotes
Authors’ Note
A previous version of this paper was presented at the 2017 annual meeting of the Population Association of America.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for research, authorship, and/or publication of this article: The data collection was supported by grants from the Social Science Research Institute (SSRI) and the Faculty Initiatives Fund (FIF) at Rice University. We are grateful for their support.