
Abstract
Impulsive behavior is a characteristic of children with specific learning disabilities (SLD), and is related to learning ability. The present study aims to identify impulsivity behavior in children with SLD who attend inclusion schools, from their resource room teachers’ perspectives. A 31-item questionnaire that addressed four subscales was designed, and the study sample consisted of 103 resource room teachers of children with SLD from various inclusion schools in Al-Zarqa city in Jordan. The results revealed that the main problem was related to lack of premeditation, followed by lack of perseverance and urgency. The results also indicated that there were statistically significant differences only for the Lack of Perseverance subscale, with regard to level of disability, whereas there were no differences attributed to teacher gender, child gender, and age. Based on these findings, implications and recommendations are discussed.
Introduction
Children with specific learning disabilities (SLD) are considered to be a diverse group, exhibiting potential difficulties in many different areas. For example, one child with SLD may have significant reading problems, while another child may have difficulties in writing, and learning disabilities can be mild, moderate, or severe (National Association of Special Education Teachers, 2006). Over the years, a variety of characteristics associated with learning disabilities, which not all children with SLD exhibit, have been identified, including hyperactivity, impulsivity, perceptual-motor impairments, disorders of memory and thinking, emotional labiality, coordination problems, language deficits, attention disorders, equivocal neurological signs, academic difficulties, and deficits in social skills (Pierangelo & Giuliani, 2008).
Attention-deficit hyperactivity disorder (ADHD) is a specific developmental disorder that includes deficits in behavioral inhibition, sustained attention and resistance to distraction, and the regulation of one’s activity level to the demands of a situation (hyperactivity or restlessness) (Barkley, 1997). According to the Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR; American Psychiatric Association [APA], 2000), ADHD disorder is a common childhood disorder that is currently defined as having three primary symptoms: inattention (poor sustained attention to tasks or persistence of effort), hyperactivity (excessive task-irrelevant activity or activity that is poorly regulated to the demands of a situation), and impulsivity (impaired response inhibition, impulse-control, or capacity to delay gratification, usually as inability of the individual to stop or think before acting) (D. Miller, Derefinko, Lynam, Milich, & Fillmore, 2010). Swanson, Nolan, and Pelham developed a rating scale (SNAP) with items taken from the exact wording of the symptoms specified in the three domains (five for inattention, six for impulsivity, and five for hyperactivity) provided within the DSM-IV (Bussing, Fernandes, & Harwood, 2008; Swanson, Wigal, & Lakes, 2009).
Research has suggested that individuals with these three common difficulties associated with ADHD, and particularly impulsive behavior, also have difficulties with other psychological functions. For example, they may have problems with remembering to do things, or with their working memory, which refers to the capacity to hold information in mind that will be used to guide one’s actions, either soon or at a later time (Barkley, 1998; Stevens, 2005). They are often described as acting without hindsight or forethought, being less able than others to anticipate and prepare for future events, being less able to pursue long-term goals, and having more problems with time management compared with others (Barkley, 1997). Children with ADHD usually have difficulties in performing a set task and following rules (Barkley & Murphy, 2006). They may have delayed development of internal language (the mind voice) which is considered an important part of the normal development of contemplation, reflection, and self-control, also referred to as “self-regulation” (Barkley, 2006; Neef, Bicard, & Endo, 2001). When combined with their difficulties with working memory, this problem with self-talk or private speech often results in significant interference with reading comprehension, especially of complex, uninteresting, or extended reading assignments (Barkley, 1997). It is worth mentioning that the symptoms of ADHD associated with hyperactive and impulsive behavior appear to arise between 3 and 6 years old, while those who have the inattentive type of ADHD that is not associated with impulsiveness appear to develop this in middle or later childhood (Barkley, 2006).
SLD commonly occur with ADHD, and the most likely cause of impulsive behavior is ADHD. Therefore, some children with SLD may manifest inattention, hyperactivity, and/or impulsivity (APA, 2013). Literature on the early years has reported that children with SLD have more impulsive behaviors (Donfrancesco, Mugnaini, & Dell’Uomo, 2005). Impulsive behavior is seen as a wide concept and can have different meanings, such as acting before thinking, giving into cravings, the inability to plan (Kirby & Finch, 2010), the inability to appreciate consequences, a lack of patience (Pentz & Willis, 2012), a lack of impulse-control, and inability to delay gratification (Vollmer, Borrero, Lalli, & Daniel, 1999). Such children make decisions and select solutions quickly, without thinking about the consequences (Nagle & Thwaite, 1979). Many researchers have related impulsivity to risk-taking, a lack of planning, and quickly making decisions (Barahmand, Piri, & Khazaee, 2015; Eysenck & Eysenck, 1978).
Impulsivity can be seen as a dimension of normal personality, but a high level of impulsivity is associated with different childhood behavior problems such as aggression, disruptive behavior, and peer relationship problems, or as an essential characteristic of psychiatric disorder such as ADHD (Barahmand et al., 2015). Research has suggested that impulsivity is not a unitary construct (Evenden, 1999) and that increases in different aspects of impulsivity represent different subtypes of ADHD (Winstanley, Eagle, & Robbins, 2006).
In studies concerned with identifying impulsivity behavior among children with SLD, this is more strictly viewed as social timing-rule infraction, lack of motor control, distraction inhibition (Donfrancesco et al., 2005), and poor self-regulation (Barahmand et al., 2015; Weed, Keogh, Borkowski, Whitman, & Noria, 2011; Winstanley et al., 2006). In this field, Kavale and Forness (1996) have suggested that children with SLD interact with more distractibility, hyperactivity, and lack of self-control. According to Kindlon, Mezzacappa, and Earls (1995), there is cognitive impulsivity in addition to behavioral impulsivity, which represents cognitive inhibitory control and insensitivity among children.
It is worth noting that children with impulsivity sometimes display normal behaviors, and may respond to stress by fidgeting, restlessness, and distracted behavior (Nkrumah, Olawuyi, & Torto-Seid, 2015). Teachers usually consider children to be exhibiting impulsivity when they are faced with difficulties in stopping to think before understanding directions, in organizing their possessions (Ziporli, 2008), and their assignments are usually incomplete or full of errors (Nwamuo, 2010). Usually, impulsive behavior leads to problems in performing school tasks due to impulsive children tending to respond hastily when faced with cognitive tasks, where they would rather be fast than accurate, and give the first answer that comes to their mind. Such children make decisions after only briefly looking at a problem without considering the consequences, and they are known as having poor problem-solving skills (Nkrumah et al., 2015; Olasehinde, 1991), as they prefer the quickest way to solve a problem because they dislike delay (Ying-he & Jia-Jia, 2011).
Reflective individuals take time and think deeply before responding and consider the alternatives before making a decision and choosing a solution (Michalska & Zajac-Lamparska, 2015; Nkrumah et al., 2015; Olasehinde, 1991). Reflective children perform better than impulsive children in cognitive tasks, who usually encounter difficulties in responding accurately and produce academic errors as they cannot wait and consider alternative options and consequences (Nkrumah et al., 2015; Zentall, 1993).
Causes Associated With Impulsivity
Many researchers have tried to explain the causes of impulsivity among children by using a biological versus environmental approach. One explanation which utilizes the biological approach is that fetal brain development is critical and undergoes complex and delicate changes; consequently, mothers who use drugs or smoke during pregnancy may have an effect on her fetus’s brain chemistry and cause her child’s future impulsivity (Nkrumah et al., 2015). It has even been proposed that a specific gene for the serotonin receptor (5HT2A102) may play an important role in the regulation of impulses. This gene is involved in serotonin regulation, which is implicated in ADHD. Individuals with two of these genes on paired chromosomes score higher on personality tests for impulsivity than those with one or no copies of the gene (Kreisman & Straus, 2004). The serotonin receptor gene is associated with both hyperlocomotion and ADHD, as well as impulsivity. Children with a polymorphism made more commission errors during a punishment reward condition in a go-on-go task (Nomura et al., 2015). Meanwhile, a lack of some vitamins, such as niacin, pantothenic acid, thiamine, and vitamins B and C, has been reported as being associated with impulsivity among children (Werbach, 1995). Electroencephalograph (EEG) and position emission tomography (PET) scans have shown that impulsive children have decreased blood flow, altered glucose utilization, and EEG activation (Woods & Ploof, 1997). Moreover, watching television for long periods of time, eating excess sugar, and poor discipline can also increase impulsivity (Nkrumah et al., 2015). Finally, inadequate mental stimulation and a lack of attention contribute to an increase and intensifying of signs of impulsivity (Nkrumah et al., 2015).
Dysfunction of the dopamine (neurochemical) system is responsible for some symptoms including impulsivity (Winstanley et al., 2006). Moreover, Weed et al. (2011) and Barahmand et al. (2015) confirmed that children with SLD, as well as children with impulsivity, have impaired frontal/prefrontal function, which Crews and Boettiger (2009) confirmed as overseeing behavioral control through executive functions, which include abstract thinking, motivation, planning, attention to tasks, and the inhibition of impulsive responses. Thus, it can be suggested that the achievement of children with SLD is at stake because of their executive function deficits, as well as because of their impulsive temperament. Frontal/prefrontal lobe function is associated with a child’s ability to solve problems; therefore, children with SLD who have average or above average intelligence may be unable to use their frontal lobe effectively, and any damage to the frontal lobe may affect a child’s ability to project future consequences resulting from current actions, make decision making problematic (Brain Injury Institute, 2011; Centre for Neuro Skills, 2016). Thus, children with SLD and children with impulsivity may experience problems in determining similarities and differences between things and events, performance, social skills, the ability to read, and language and numeracy skills. Frontal lobe damage may also impair attention span, motivation, judgment, organization capacity, control of motor skills such as hand and eye coordination, conscious thought and emotion, and even personality (Brain Injury Institute, 2011). The prefrontal lobe has been implicated in planning, personality expression, and moderating social behavior, and is involved in the orchestration of thoughts and actions in accordance with internal goals (E. Miller, Freedman, & Wallis, 2002). Therefore, impulsivity in children with SLD may explain or be associated with some of the inappropriate behaviors exhibited by children with SLD, including when faced with problems in social skills and communication, and social cognition, where they fail to interpret the feelings of others, do not know how to read social cues, and do not realize when their behavior is disturbing others (Bers, 2002; S. Miller & Mercer, 2001; Moor & Lagoni, 2003). There is also an impact on the frequency and occurrence of mistakes, both at the level of social interactions and academic performance. Such impulsive behavior is related to a lack of communication skills, as children do not respond to the requirements of social situations in appropriate ways, and may then fail to build healthy social relationships (Pavri & Luftig, 2000). This can in turn lead to future problems, including addiction, as some impulsivity behaviors, such as deficits in attention, lack of reflection, and/or insensitivity to consequences, are demonstrated in those addicted to drug (de Wit, 2009). Consequently, it is important to understand impulsive behavior in children with SLD and to build a treatment program for impulsive behavior which positively enhances the behavior of children with SLD and their academic performance, and also prevent them from displaying behavior problems in the future.
Cognitive and Behavioral Aspects of Impulsivity
Since 1970, many studies have been interested in investigating the cognitive and behavioral aspects of impulsivity in children with SLD, and have reported that children with SLD have higher levels of impulsivity (Barahmand et al., 2015), especially in severe cases (Donfrancesco et al., 2005). Previous results (Purvis & Tannock, 2000) have reported a prevalence of impulsivity, especially among students with dyslexia, and have shown that children with ADHD and a reading disorder performed worse than children with ADHD without reading disorder in an inhibitory control task, which suggests an additional impulsivity effect of dyslexia. Weed et al. (2011) found that children with dyslexia tend to be faster in their responses and show higher cognitive impulsivity than other groups of children. However, Nagle and Thwaite (1979) found that children with SLD are not more impulsive compared with children without disabilities, rather they use poor strategic behaviors when processing information.
Impulsivity and Academic Success
Numerous studies have suggested that impulsivity behavior has a negative effect on schoolwork. Kagan (1965) reported that scoring as impulsive on the Matching Familiar Figures Test (MFFT; Kagan, Rosman, Day, Albert, & Phillips, 1964) was associated with more reading mistakes compared with reflective children. Previous studies have also found that children who are impulsive frequently have deficits in reading and mathematics demonstrated reduced attention and cognition, compared with reflective children (Kagan, 1965; Lesiak, 1978; Rezaei, Boroghani, & Rahimi, 2013; Umaru, 2013). Impulsive children are more likely to offer incorrect solutions during examinations due to their only considering their first solution, and such children may fail during school tasks due to their inability to assess the validity of responses before choosing the appropriate option (Nkrumah et al., 2015; Olasehinde, 1991; Zentall, 1993).
Nkrumah et al. (2015) and Zentall (1993) stated that although poor achievement is usually explained as a result of a lack of intellectual abilities, impulsivity among children may partially explain low achievement among impulsive children, including those who have disabilities, as their impulsivity causes them to make guesses rather than to think (Olasehinde, 1991). Impulsivity may be related to future behavioral problems, for example, due to premature, unduly risky, or poorly conceived actions, deficits in attention, a lack of reflection and/or insensitivity to consequences, all of which occur during addiction (Crews & Boettiger, 2009; de Wit, 2009; Evenden, 1999).
Purpose of the Study
Although there are documented incidents of impulsivity among children with SLD, and previous studies have led researchers to emphasize the importance of detecting impulsivity in children with SLD and to provide them with appropriate remedial programs, little attention has been given to identifying impulsivity (Donfrancesco et al., 2005; Nagle & Thwaite, 1979). It is worth noting that several studies have emphasized that impulsivity behavior can be modified through training programs, and researchers have demonstrated the efficacy of modeling to modify the impulsivity behavior among children with SLD, by placing them in situations which allow them to pay more attention to the reflective model (Nagle & Thwaite, 1979; Nwamuo, 2010; Olasehinde, 1991). Mckinny, Montague, and Hocutt (1993) reported the effect of a cognitive and problem-solving program on reducing impulsive behavior among children with SLD, and who became more reflective children.
Testing impulsivity should be considered as part of the diagnostic process for children with SLD. Harrison and Romanczyk (1991) and Walker (1985) noted such relevance, as although many research studies have identified impulsivity in children with SLD, the relationship between SLD and impulsivity has not been clearly established. No study has been conducted in Jordan to identify impulsivity among children with SLD who attend inclusion schools. Thus, the present study was designed to improve understanding and to identify impulsivity behavior which children with SLD may display, by asking their teachers to assess impulsivity among some children with SLD whom they assist in the resource room within inclusion schools. Thus, this study was designed to elicit answers to the following research questions:
Jordanian Context
Jordan is a small a country at the heart of the Middle East, with limited resources. Like other countries including the United States, the United Kingdom, Australia, and Canada, Jordan is jointly developing programs and following people with disabilities, paving the way for the integration and inclusion of children with disabilities into general education classrooms (Avramidis, Bayliss, & Burden, 2000; United Nations Educational, Scientific and Cultural Organization, 2009), where children with an SLD are supported by resource rooms. At the present time, there are 900 part-time resource rooms within regular schools across Jordan, which offer remedial and special education services to 12,160 children from the second to sixth grades with SLD (Al-Natour, AlKhamra, & Al-Smadi, 2008). The Ministry of Education (MoE) suggests that 20 to 25 students with SLD are served in these settings (Al Jabery, AlKhateeb & Zumberg, 2012; Al Jabery, AlKhateeb & Zumberg, 2012). As integrating efforts continue, resource room teachers have been assigned the sole responsibility for supporting students with disabilities, while regular classroom teachers are not yet involved effectively in addressing the needs of included children (Abu-Hamour & Al-Hmouz, 2013). In 1994, the Remedial Education Department was founded by the MoE and this is accountable for the training of special educational needs teachers.
Method
Participants
The study sample was randomly recruited from among the special education teachers in 100 regular schools in Al-Zarqa city in Jordan. One hundred three special education teachers who taught children with SLD in the schools’ resource room (resource room teachers) were asked to complete a study questionnaire assessing impulsivity behavior in children with SLD. The demographics of the sample are shown in Table 1.
Sample Distribution.
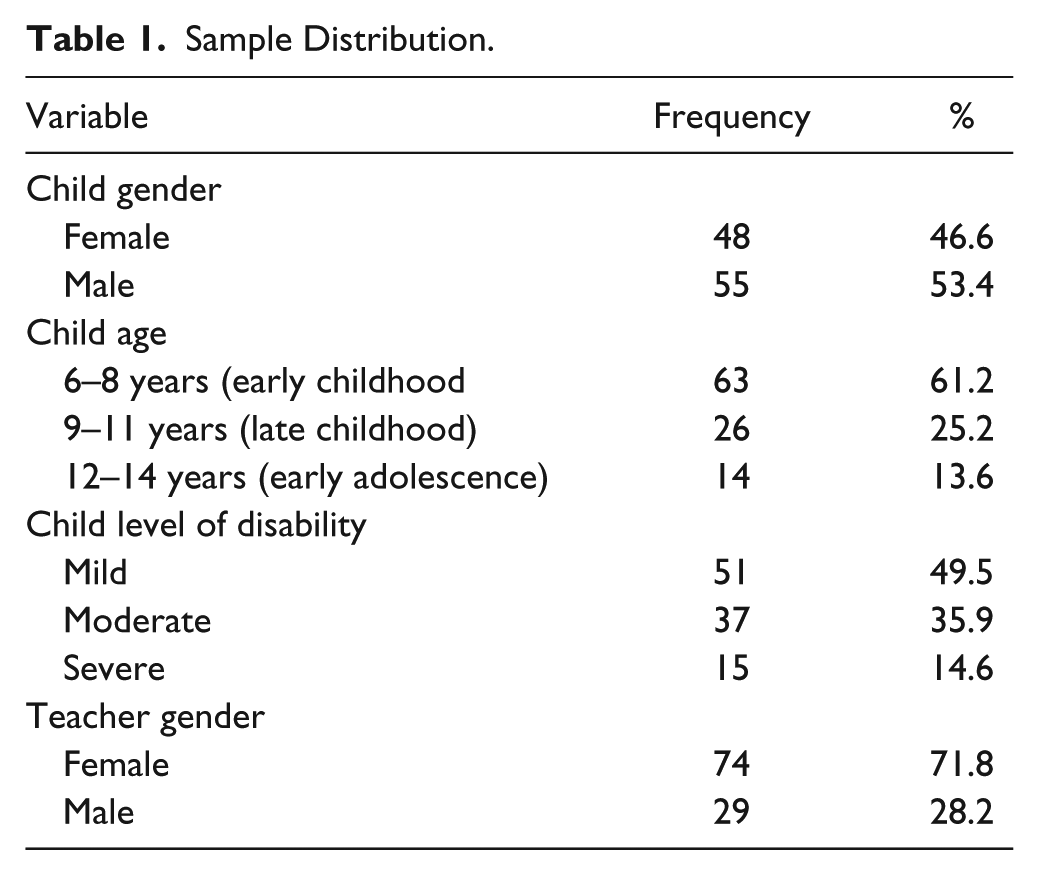
The teachers were asked to consider one child, chosen at random from their children with SLD, and to assess the child’s behavior using the scales provided. The subjects of the teachers’ observations consisted of 103 children with SLD, aged from 6 to 14 years, who attended inclusion settings within regular schools.
Instrument
To achieve the study objective, and within clinical psychology to identify different aspects of behavior (Winstanley et al., 2006), a self-report questionnaire was designed by the researchers to report teachers’ observations of impulsivity behavior in children with SLD. A comprehensive review of the literature concerning impulsivity behavior and children with SLD characteristics was used as the basis for the study and as a source for designing the questionnaire (e.g., Pentz & Willis, 2012; Whiteside & Lynam, 2001). A number of questionnaires designed to measure impulsive behavior were also reviewed, such as the Barratt Impulsiveness Scale (Patton, Stanford, & Barratt, 1995); the Behavior Rating Inventory of Executive Function (BRIEF; Gioia, Isquith, Guy, & Kenworthy, 2000), which measures executive functioning; the Conners Teacher Rating Scale (CTRS; Conners, 1997), which measures ADHD based on dimensional adjuncts to the DSM-IV diagnoses for ADHD; the ADHD Rating Scale IV—Home Version (APA, 2000; DuPaul, Power, Anastopoulos, & Reid, 1998; Purpura & Lonigan, 2009); and the UPPS Impulsive Behavior Scale (Whiteside & Lynam, 2001).
To the researcher’s knowledge, there was no scale designed to identify impulsivity behavior in children in general, and children with SLD in particular, that was specifically developed for the Jordanian environment. The DSM-IV is usually used for diagnostic purposes, but, in contrast, the current study aimed simply to conduct a quick survey to identify the prevalence of impulsivity behavior among children with SLD in the Jordanian context. So the questionnaire was developed to identify the level of impulsivity behavior in children with SLD as reported by their teachers in the Jordanian schools (Miller et al., 2010; Swanson et al., 2009).
The questionnaire consisted of 31 items that addressed three subscales: (a) Urgency, which consisted of 12 items and referred to the tendency to experience strong impulses under negative conditions; (b) Lack of Premeditation, which consisted of 11 items and referred to the tendency to fail to think and reflect on the consequences of an act before engaging in that act; and (c) Lack of Perseverance, which consisted of eight items and referred to difficulties in remaining focused on a task that may be long, boring, or difficult. The modified UPPS Impulsive Behavior Scale (Whiteside & Lynam, 2001) was used to identify the means of the subscales used in the current study. The questionnaire employed a 4-point Likert-type scale of responses, with 4 indicating always, 3 often, 2 occasionally, and 1 never. Each teacher was asked to read the item carefully and to express his or her opinion concerning to what degree this item represented the target child. To determine the values of the levels of impulsivity behavior (low impulsivity behavior, moderate impulsivity behavior, high impulsivity behavior) and to assist in the interpretation of the results, the following ranges were derived: A score of 1 or above but less than 2 indicated a low level of impulsivity behavior; 2 or above but less than 3 indicated a moderate level of impulsivity behavior; from 3 through 4 indicated a high level of impulsivity behavior.
Validity and reliability of the instrument
The initial draft of the study scale was developed in English, and due to the background of the respondents, the questionnaire was translated into the Arabic language which is the respondents’ mother tongue. Then, a language specialist proofread both the Arabic and English copies. To ensure the validity and reliability of the questionnaire, only the Arabic version was tested.
The content validity of the instrument draft scale was evaluated by a panel of 10 experts, consisting of university faculty staff members with a specialization in the special education field, to ensure that the items represented the correct subscales of impulsivity and that the content of the instrument was accurate and adequate regarding language clarity, and to provide any additional comments. For instance, the panel suggested adding one item examining children’s ability to make decisions, and they advised shortening a number of items which they felt were too long. Items that were kept in the instrument were judged by the majority of the experts to be coherent, relevant, and representative of all subscales of impulsivity. So, the changes indicated by the validation panel were incorporated in developing the instrument development, omitting, adding, or rephrasing items, and reducing the number of items from 33 to 31.
Next, the validity of the instrument was further examined by initially administering the proposed scale of the study to an exploratory sample of 15 resource room teachers. The pilot study was designed to enable the researchers to examine the transparency of the items and their fitness to the scale, to enhance the scale to ensure the respondents’ acceptance of it, and to determine the time of application of the scale. This process provided in-depth understanding of how each item was understood and the way the participants used it in formulating their responses. After each respondent had received the proposed scale, he or she was asked to examine the scale items for clarity, suggest additions or deletions, and to correct any error in words or procedures. Most of the respondents’ suggestions related to items consisting of unfamiliar concepts, or that were considered irrelevant to the classroom environment. The field-testing also showed that respondents did not understand a number of technical terms used in the first draft of the questionnaire, such as “doesn’t control his actions”; thus, the pilot study was helpful in giving the researchers an opportunity to change the wording of these terms. All the suggestions from the pilot study were considered, and necessary changes were integrated into the scale. Most of the changes focused on reformulating or rewording some of the scale items; no item was deleted or added at this stage. Finally, the pilot study gave the researchers a good opportunity to test the time needed to complete the instrument: It took the teachers around 10 to 15 min to complete the questionnaire.
To estimate the reliability of the questionnaire, its internal consistency coefficient was calculated using Cronbach’s alpha. A reliability coefficient of 0.89 was obtained for the whole instrument, 0.74 for the Lack of Premeditation, 0.70 for the Lack of Perseverance, and 0.81 for the Urgency subscales. These results indicate that the reliability coefficients were satisfactory for the purpose of this study.
Ethical Considerations
Participants were informed before the study commenced about the aims of the research, and were assured that their responses would be treated with confidentiality and anonymity. The study protocol was reviewed and approved by the Institutional Review Board at Hashemite University.
Data Collection
A list of all schools implementing an inclusion setting through use of a resource room for children with SLD within Al-Zarqa city was provided to the researchers by the MoE and was used to identify potential study participants. The researchers conducted personal visits to the schools and met with the resource room teachers and acquainted them with the purpose of the study. The researchers and the resource room teachers in each school randomly selected three children with SLD from the children who attended the resource room. The researchers hand-delivered the questionnaire to resource room teachers during the second semester of the academic year 2015/2016. Teachers were encouraged to read the items carefully before selecting the appropriate choices represent the target child’s characteristics. It should be noted that each of the resource room teachers in each school completed an individual questionnaire for one child with SLD. The researchers made appointments to collect the completed questionnaires 1 week later.
Data Analysis
The survey questionnaire was quantitatively analyzed using the Statistical Package for the Social Sciences (SPSS). The collected data were analyzed and expressed using means and standard deviations (SDs) for the first question, and t tests and analysis of variance (ANOVA) were performed to examine the second question. To control for the inflation of Type I error rate in univariate ANOVAs, a Bonferroni-adjusted Type I error rate of .05/3 (i.e., 0.017, where the number of subscales = 3) was employed, as suggested by Nolan and Heinzen (2014).
Results
The data collected from the sample were coded, entered into SPSS, and analyzed using the SPSS software package (edition 22). Descriptive statistics for all the variables identified in this study were examined using SPSS frequencies. Missing subjects were not detected, and the results of the study are addressed in response to each individual research question.
Impulsivity Behavior Among Children With SLD
Research Question 1 examined the impulsivity behavior of children with SLD according to their teachers’ perception. Descriptive statistics, including mean and SD, were used to analyze the data.
To determine whether the three subscales correlated, correlation analysis was used. As shown in Table 2, results revealed a statistically significant correlation between the three subscales, which range between 0.49 and 0.69 at the level 0.017, so the total mean of the impulsivity scale was considered due to the existing correlation between the three subscales.
Results of Correlation Analysis Between the Subscales.
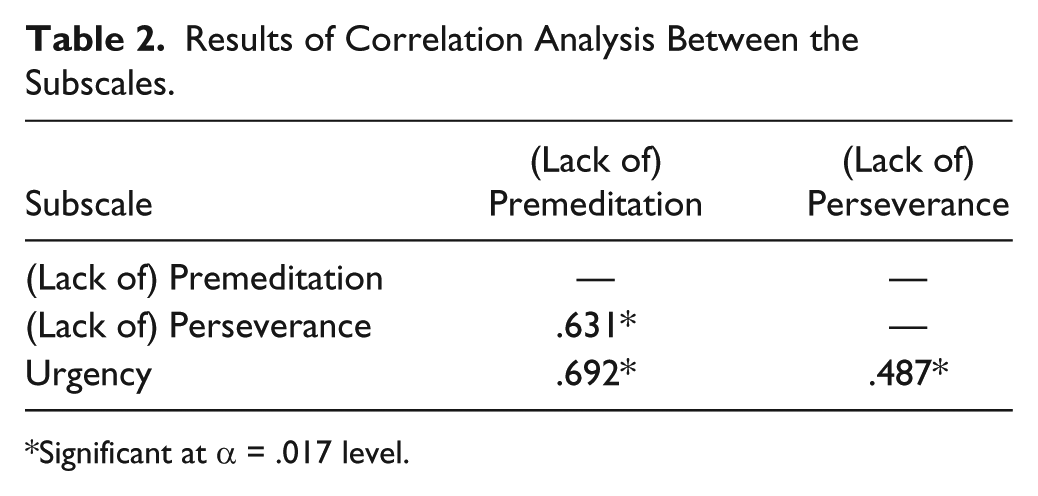
Significant at α = .017 level.
As shown in Table 3, the overall mean score for teachers’ perception of impulsivity behavior among children with SLD was 2.5847 (SD = 0.43), indicating that teachers perceived that children with SLD had moderate levels of impulsivity behavior.
The Distribution of Impulsivity Behavior Among Children With SLD Attending Inclusive School.
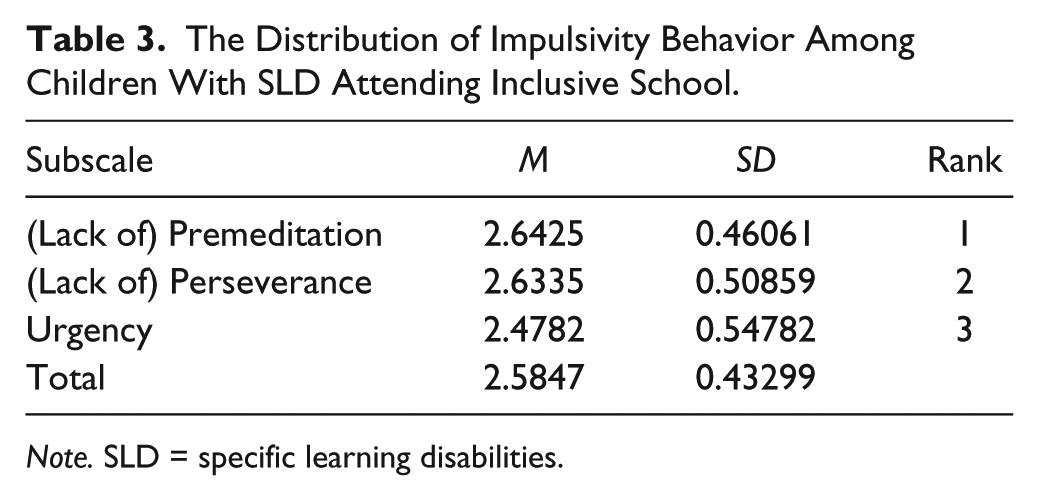
Note. SLD = specific learning disabilities.
Regarding the subscales, the findings, as shown in Table 3, indicate that on average, children in this sample displayed higher levels of problems associated with premeditation, with a mean score of 2.64, followed by problems with perseverance, which had a mean score of 2.63, while problems related to urgency were ranked as the least serious with a mean score of 2.48.
Table 4 displays the items for the three subscales in which teachers were asked to report the extent to which a target child with SLD demonstrated impulsivity behavior. The table illustrates that the most serious problems were viewed as being those related to a lack of premeditation, and teachers regarded the ability of children with SLD to make decisions based on careful and deep reflection as their biggest problem, with a mean score of 3.17, followed by problems concerning caution regarding thoughts and action, which had a mean score of 2.94. Problems related to a lack of perseverance revealed a mean score of 2.95, and children with SLD were curious about puzzles and quizzes, although problems with completing homework on time received a mean score of 2.81. With regard to problems relating to urgency, the data indicated that the most serious problem that children with SLD display is related to their ability to self-control, with a mean score of 2.89, followed by making quick decisions, which had a mean score of 2.76.
The Distribution of Impulsivity Behavior Among Children With SLD According to Teachers’ Responses (Based on 4-Point Likert-Type Scale: 1 = never, 2 = occasionally, 3 = often, 4 = always).
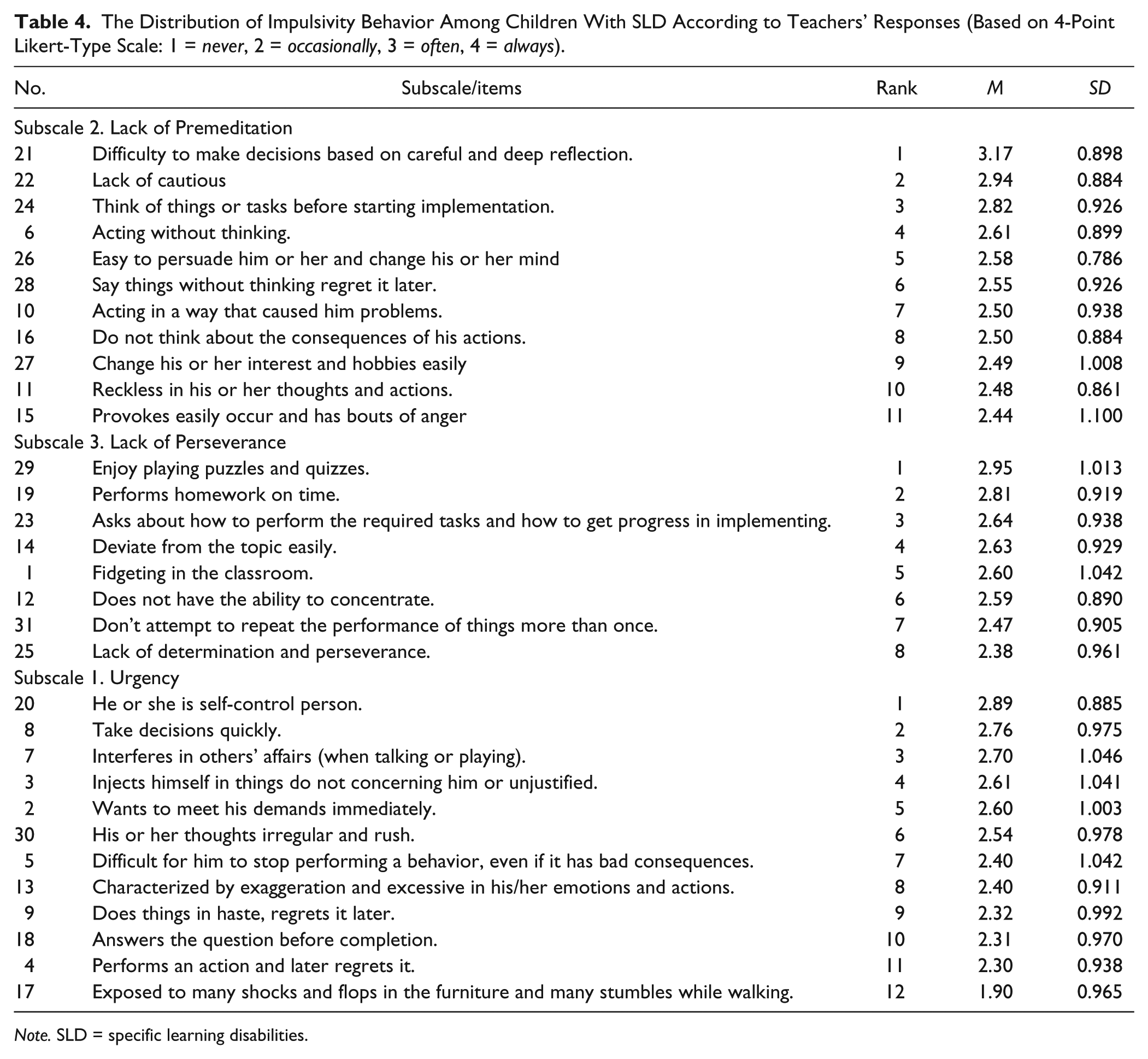
Note. SLD = specific learning disabilities.
Variables Associated With Impulsivity Behavior
The second research question examined the statistically significant differences among the impulsivity behavior children with SLD displayed according to their resource room teachers. The following variables were investigated: (a) child gender, (b) child age, (c) level of disability, and (d) teacher’s gender. To examine the differences among children with SLD due to gender, a t test was utilized (using Bonferroni-adjusted Type I error rate with α= 0.017). The results showed that there were no statistically significant differences in impulsivity behavior among children with SLD according to their teachers’ perception due to child gender.
For differences attributed to the level of disability, a one-way ANOVA was utilized (using Bonferroni-adjusted Type I error rate with α = 0.017). The results show that there were no statistically significant differences among children with SLD due to a child’s age, although there were statistically significant differences among children with SLD due to their level of disability for the Lack of Premeditation subscale, as shown in Table 5.
Differences Among the Level of Disability in Impulsivity Behavior Among Children With SLD.
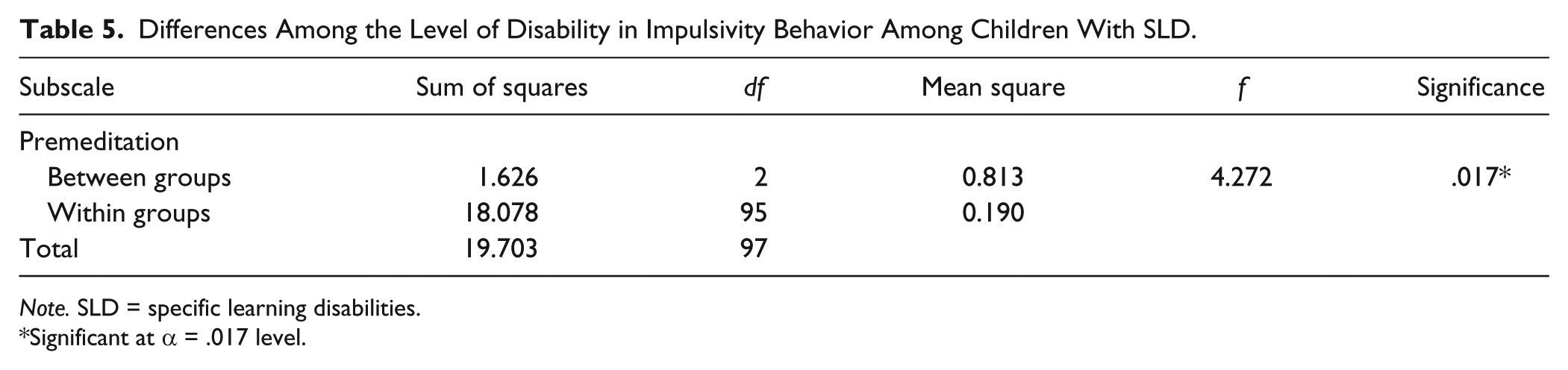
Note. SLD = specific learning disabilities.
Significant at α = .017 level.
The results for the Tukey test indicate that there were statistically significant differences between the mean scores of children with severe SLD and children with mild SLD, in favor of the children with severe SLD. Children with severe SLD display more problems with premeditation compared with children with mild SLD, as shown in Table 6.
Multicomparisons of Impulsivity Behavior Among Children With SLD on the Level of Disability Variable.

Note. SLD = specific learning disabilities.
Significant at α = 0.017 level.
Discussion
This study was conducted to understand impulsive behavior among children with SLD according to the perceptions of their resource room teachers, and to explore the statistically significant differences among children with SLD, related to child gender, child age, level of disability, and teacher’s gender. Results indicated that teachers’ perceptions about the level of impulsivity behavior among children with SLD were moderate on the overall scale and the three subscales. The results of this article confirm the work of Barahmand et al. (2015) who found that children with SLD showed moderate levels of impulsivity, especially in problems with premeditation and perseverance. In contrast, this result disagrees with the findings of other studies which reveal that children with SLD (dyslexia) were more impulsive compared with children without SLD (Donfrancesco et al., 2005), and suggest that learning disability and ADHD including impulsivity are on a continuum and interrelated (Mayes, Calhoun, & Crowell, 2000). This result could be due to the fact that about half of the children in the current study have with mild SLD. Moreover, the current study did not deal with the different types of learning disability, which according to other research results have demonstrated different levels of impulsivity behavior. For example, Donfrancesco et al. (2005) found that children with dyslexia showed a significantly higher cognitive impulsivity and less accuracy than children with spelling disability. Other research supports this explanation, finding that the performance of children with SLD in the MFFT showed higher impulsivity (Bolster, Marshall, Bow, & Chalmers, 1986; Nagle & Thwaite, 1979), especially in severe cases, as a more recent study has also shown (Donfrancesco et al., 2005).
The result showed also that impulsivity among children with SLD manifests most strongly as a lack of premeditation, followed by a lack of perseverance, while urgency was ranked as the least serious problem. These results are similar to previous research which has shown that impulsive behavior is usually associated with SLD (Barahmand et al., 2015; Pierangelo & Giuliani, 2008), especially for children with dyslexia (Donfrancesco et al., 2005; Purvis & Tannock, 2000), and such children perform with less accuracy and make more errors than children without disabilities. This may be attributable to the functioning of the frontal/prefrontal lobe, which is considered to be associated with SLD and impulsivity (Weed et al., 2011). Poor performance, SLD, and impulsivity are related to frontal/prefrontal impairment (Anderson, Damasio, & Damasio, 1990), leading to the conclusion that SLD and their underachievement are generally associated with their impulsivity.
The most serious problem identified was related to the Lack of Premeditation subscale, reflecting children experiencing difficulties in making decisions based upon careful and deep reflection, displaying a lack of caution, and acting without thinking. This result shows that children with SLD are at risk of displaying impulsive behavior, which is represented mainly by hasty behavior without thinking about the consequences, which is reflected in poor organization and planning when confronted with situations or educational problems. Such impulsive behavior deprives a child with an SLD of logical thinking for problem solving, which leads them to make a large number of errors. This can usually be explained by possible visuospatial difficulties, as orthographic representations are coded spatially, as noted by Hillis and Caramazza (1991). This result could be due to the fact that programs designed for children with SLD in inclusion schools in Jordan place little value on modifying impulsivity behavior; instead, the focus is on an academic program which considers impulsivity as a secondary problem that can be solved by enhancing a child’s academic performance. This result is similar to the findings of other research in this area, indicating that children with SLD display some difficulties related to impulsivity, such as acting before thinking and the inability to plan (Kirby & Finch, 2010). Such children make decisions and choose inappropriate solutions without thinking about the consequences (Eysenck & Eysenck, 1978; Nagle & Thwaite, 1979).
A lack of perseverance was ranked as the second highest impulsive behavior displayed by children with SLD, especially concerning curiosity regarding puzzles and quizzes, completing homework on time, and easily being distracted from the activities they are engage in. This may be due to children with SLD who display ADHD experiencing memory and attention problems, where estimating the time, setting goals and working on self-stimulation to achieve goals is difficult. Some of these children display hyperactive behavior, which may have an effect on their ability to deal with complex tasks and to complete it on time as noted by many researchers (Alkhcrma, 2007; Donfrancesco et al., 2005). This result confirmed that the multidimensional nature of executive function, shown in self-regulatory behaviors, may affect the relationship between type of learning disability, and achievement for children, as shown by previous research (e.g., Barahmand et al., 2015; Weed et al., 2011).
The results also show that the problem related to urgency ranked as the least serious problem that children with SLD have. This is exhibited by children encountering difficulties in self-control, followed by making decisions quickly. This result is similar to previous research which indicated that children with SLD have a lack of self-control and are more distractible (Kavale & Forness, 1996), while frequently displaying a lack of patience (Pentz & Willis, 2012).
The results revealed that there were no statistically significant differences in impulsivity behavior among children with SLD, according to their teachers’ perceptions, due to child gender and age. This indicates that teachers have the same perception of impulsivity among children with SLD regardless of their age and gender. This result is consistent with the results of Mahone et al.’s (2002) study, which found that there were no significant differences in impulsivity behavior among children, including those with SLD, due to age and gender. Also this result is similar to other studies which found no significant age differences in impulsivity emerged (Pentz & Willis, 2012; Steinberg et al., 2008) and that there are few sex differences in impulsivity (Haghighi, Ghanavati, & Rahimi, 2015; Reynolds, Ortengren, Richards, & de Wit, 2006). This could be because impulsivity behavior is related to biocauses, especially to neurochemical secretions in the body (Winstanley et al., 2006). Another cause might be related to the environment of the child, especially as in Jordan there are no national specific programs focusing on remedial work with impulsivity, and also there are severe shortages of professionals specializing in impulsivity remedial work.
The results showed also that children with severe SLD have higher levels of impulsivity compared with children with mild SLD. This result is similar to that of Donfrancesco et al. (2005), who found that children with severe SLD have higher levels of impulsivity. This may due to these children having poor strategic behaviors when processing information, as noted by Nagle and Thwaite (1979). Consequently, children with severe disabilities may encounter more challenges in processing information compared with their peers with mild SLD.
It is worth noting that a strength of this study lies in the development of a scale to identify impulsivity among children with SLD, and in identifying the most serious problems related to impulsivity. In addition, this study highlights the importance of considering impulsivity when creating programs for children with SLD, as this behavior affects a child’s social and academic performance. Future studies of impulsivity in children with SLD should explore the relationship between impulsivity and academic performance, and social competencies and communication skills, which are considered the main problems for these children, so that appropriate interventions can be offered. Future study could also investigate impulsivity among children with various types of learning disabilities (e.g., dyslexia, spelling disorders, and dyscalculia).
Limitations of the Study
The findings should be considered within the limitations of the study. This study relied on information provided by teachers regarding the impulsivity of children with SLD. Observational methods or mothers’ reports of their children’s impulsive behavior could complement the information provided by teachers.
Despite these limitations, the results obtained have important implications. Impulsivity appears to be associated with children with SLD and may impact the behavior of these children and their ability to perform tasks effectively, due to a lack of premeditation and perseverance, in addition to the urgency behavior displayed by some children. In the clinical situation, intervention programs targeting detecting impulsivity in children with SLD and creating treatment program to modify impulsivity behavior among children with SLD may contribute to enhancing their quality of life should receive greater attention (Mckinny et al., 1993; Nagle & Thwaite, 1979).
A clinical implication of this study is concerned with rehabilitation. It is important to know whether children with SLD have marked impulsivity behavior or not, due to the role of treatment and therapeutic programs in reducing impulsive behavior. In fact, treatment programs for children with SLD provide evidence of the importance of developing meta-cognitive abilities to inhibit impulsivity (Donfrancesco et al., 2005; Nagle & Thwaite, 1979).
Conclusions and Recommendations
To summarize, the current study has shown that children with SLD suffer from a lack of premeditation and perseverance, which is why they are impulsive. This result has certain implications, and impulsivity assessments of children with SLD are recommended because of the high frequency of these symptoms in these children, with a focus on adopting a more specific rehabilitation program. It can be concluded that the moderate level of lack of premeditation and perseverance children with SLD shown according to the recently study result many effect these children’s reading, writing, and mathematical achievement. Consequently, children with SLD need treatment programs which use educational tools as models and audio-visual aids for affect, as these dramatically improve learning. In addition, reading stories and playing contributes to increased attention to scientific material, as visual and auditory memory training using educational games and computer programs is widely beneficial to these children. To solve the problem of not being able to estimate time, regulatory ways to follow time should be utilized, such as cards for hours of time, which can be used to remind a child of the time and to shorten the effort required to perform a task.
Although impulsivity is one the behavioral characteristics of children with SLD, demonstrated by a lack of planning and acting before thinking, the role of the environmental circumstances involved in the development of impulsive behavior should be considered. Because most inclusion schools in Jordan pay little attention to identifying and treating impulsive behavior among children, teachers need to undergo specific training in how to deal with and modify impulsive behaviors in children with SLD, and considered an appropriate setting to reduce impulsivity.
Finally, to conclude, both educational and clinical studies have made valuable contributions to our understanding of impulsivity and its involvement in SLD. Such studies have enriched and advanced our comprehension of the basis of impulsivity behavior among children with SLD. Because the exact relationship between SLD and impulsivity has not been clearly established, there is need for a deep investigation of the neurochemical aspects of impulsivity behavior, and for collaboration between educational, psychiatric, and neurological professionals to build a clear holistic vision about impulsivity and SLD.
Footnotes
Acknowledgements
The authors acknowledge support from the Hashemite University (HU), National Institute on Drug Abuse’s International Program (NIDA International Program), and Jordan Society for Scientific Research (JSSR) for funding the training workshop which helped developing and revising this manuscript and the support to the trainers from the University of California, San Francisco and Yale University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.