
Abstract
An aging population and wartime injuries has led to a growing population needing caregivers. This article evaluates a pilot study of an Internet-based, skills-enhancement workshop developed for the United States Department of Veteran Affairs. Sixty caregivers are enrolled. Either the caregivers or people being cared for are Veterans living in California, Southern Nevada, or Hawaii. Measures include health indicators, health behaviors, and health care utilization. Baseline measures are compared to the same measures at 3 months using paired t tests. Participation in the program is examined, including number of sessions and number of posts. Caregivers show significant reductions in caregiver burden, depression, pain, and stress. Caregiver self-efficacy and two exercise measures show improvement. The care partners’ overall health show improvement (p<.05). The program successfully reaches rural residents, and participation is high. The Building Better Caregivers program is acceptable to caregivers, whose health, emotional health, and health behaviors show improvement. Caregivers successfully participate in the program.
Introduction
The Department of Veterans Affairs National Caregiving Initiative asked the Stanford Patient Education Center to develop an online education and support program for family caregivers (U.S. Government Accountability Office, 2008). The program was built on software used for three previous self-management workshops (Lorig et al., 2008, 2010; Lorig, Ritter, Laurent, & Plant, 2006, 2008).
Content was determined after discussions with 15-20 caregivers, reviewing caregiving literature, and expert input from a geriatrician, social worker, and psychologist. A list of 30 themes was generated. The experts and Stanford staff ranked each theme independently. Items with highest rankings were selected as content for the program. Thompson-Gallagher’s work dealing with difficult behaviors provided a unifying theme (Thompson-Gallagher et al., 2003, 2007; Thompson-Gallagher, Gray, Dupart, Jimenez, & Thompson, 2008).
This article examines the feasibility and acceptability of the pilot online program for caregivers. In addition, we looked at 3-month outcomes in terms of health status, health behaviors, and medical utilization.
Method
Building Better Caregiver (BBC) is a 6-week, Internet-based workshop for 20 to 30 caregivers aimed at enhancing caregiving skills. It is offered on a dedicated website. The workshop does not require “real-time” attendance and uses discussion boards for social networking.
Each workshop is moderated by a pair of trained peer or professional facilitators with caregiving experience. Training included taking the BBC workshop, attending four Webinars, and following a detailed protocol. Facilitators remind participants to log on, model action planning and problem-solving, offer encouragement, and post to the bulletin boards. They also monitor the daily posts for safety and report problems.
Each week participants, using screen names, are asked to logon at least 3 times. Weekly activities include reading and interacting with the week’s lessons, posting action plans, problem solving on discussion boards, and participating in self-tests and homework.
There were six components to each workshop: the Learning Center (interactive, didactic material), the Discussion Center (4 bulletin boards: action planning, celebrations, difficult emotions and problem solving), My Tools (individualized tools, including problem behavior diaries and exercise logs), a Post Office (where participants communicate one on one), Resources (web links and documents), and Help (a tutorial and links to facilitators and project staff).
Each week, new content was available in the Learning Center, while previous content remained available. Links provided access to pages with information on specific optional topics, such as TBI, PTSD, and Alzheimer’s. The Learning Center also populated the Discussion Center with new discussion questions.
The Java-based software was designed to be used by almost anyone with access to the Internet. Video clips and extensive graphics were avoided. BBC is compatible with most web browsers and both Windows and Macintosh operating systems. The pilot study evaluating this program was approved by both VA Greater Los Angeles Healthcare System and Stanford University’s institutional review board.
Table 1 gives a session-by-session overview of workshop topics. Participants were recruited using online sites, press releases, and publicity throughout the Veterans Integrated Service Networks in the Desert Pacific Healthcare Network (VISN 22) and the Sierra Pacific Network (VISN 21). Eligible participants had to live in California, southern Nevada, or Hawaii; be a Veteran or caring for a Veteran; caregiving at least 10 hr a week; and have stress levels 4 or greater (out of 10). In addition, the care partner (person being cared for) must have impaired cognitive functioning (e.g. traumatic brain injury, PTSD, Alzheimer’s). Potential participants left contact information. Three weeks before a workshop, participants were given a link to a secure site where they read about the study and completed a consent form. They were then screened for eligibility and asked to complete a baseline questionnaire. After completing the questionnaire, they were assigned a workshop.
Content of Workshops
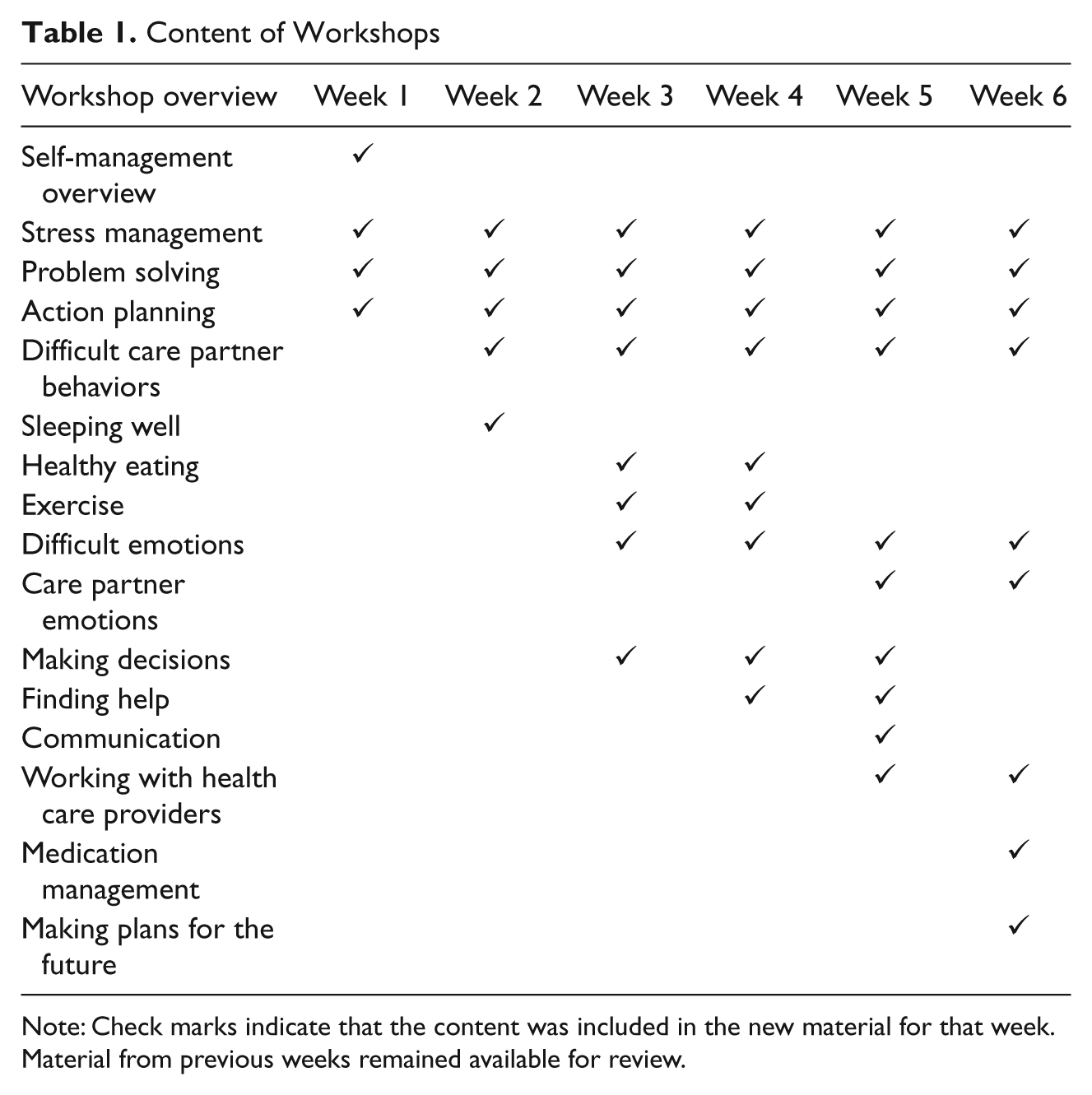
Note: Check marks indicate that the content was included in the new material for that week. Material from previous weeks remained available for review.
Information was collected from caregivers at baseline and 3 months using self-administered online questionnaires. These included basic demographics, health indicators, health behaviors, and heath care utilization measures. Specifically, self-rated health was measured with a scale from the National Health Interview Survey (U.S. Department of Commerce, 1985). The Illness Intrusiveness Index measured the impact of disease on daily life (Devins et al, 1990). Visual numeric scales (VNS) were used to measure pain, shortness of breath, stress, problems sleeping, and fatigue over the past 2 weeks. Visual numeric scales have been shown to correlate well (r = .72) with same-worded visual analogue scales (VAS) and had a 94% completion rate compared to a 76% rate for the VAS(Ritter, González, Laurent, & Lorig, 2006). The stress VNS and problem-sleeping VNS were new for this study and will require further psychometric testing with a larger sample. The Zarit Burden Inventory (ZBI) measures caregiver burden (Parks & Novielli, 2000). The Caregiver Strain Index (CSI) measured caregiver strain (Thornton & Travis, 2003). It is commonly administered to caregivers of older adults in community-based settings and is shown to have high internal reliability (alpha = .90). Depression was measured by the PHQ-8 scale, a modified version of the PHQ-9 (Kroenke & Spitzer, 2002). Self-report data were also collected on caregiver and care partner sick days, effects of caregiving on work, residence/living arrangements, and the relationship between caregiver and care partner.
Three health-related behaviors were obtained: stretching and strengthening exercise, aerobic exercise, and use of cognitive symptom management techniques (Lorig et al., 1996). Three self-reported health care utilization measures were assessed for caregiver and care partner: visits to physicians, visits to hospital emergency rooms, and number of nights spent in a hospital. In a previous study, we found that self-report of outpatient visits correlated at r = .70 with chart audit data, while days in the hospital correlated at r = .83 (Ritter et al, 2001). An 18-item Caregiving Self-Efficacy Scale was adapted from a scale developed and validated by Steffen, McKibbin, Zeiss, Thompson-Gallagher, and Bandura (2002), based on Bandura’s theory (Bandura, 1997; Rabinowitz, Mausbach, & Thompson-Gallagher, 2009; Rabinowitz et al., 2006).
Measures of participation in program included number of sessions completed, number of sessions participated in, number of logins, number of pages visited, and number of posts.
Outcomes at 3 months were compared to baseline data using paired t tests. All participants who returned questionnaires were included in the analyses regardless of degree of participation in the workshop.
Results
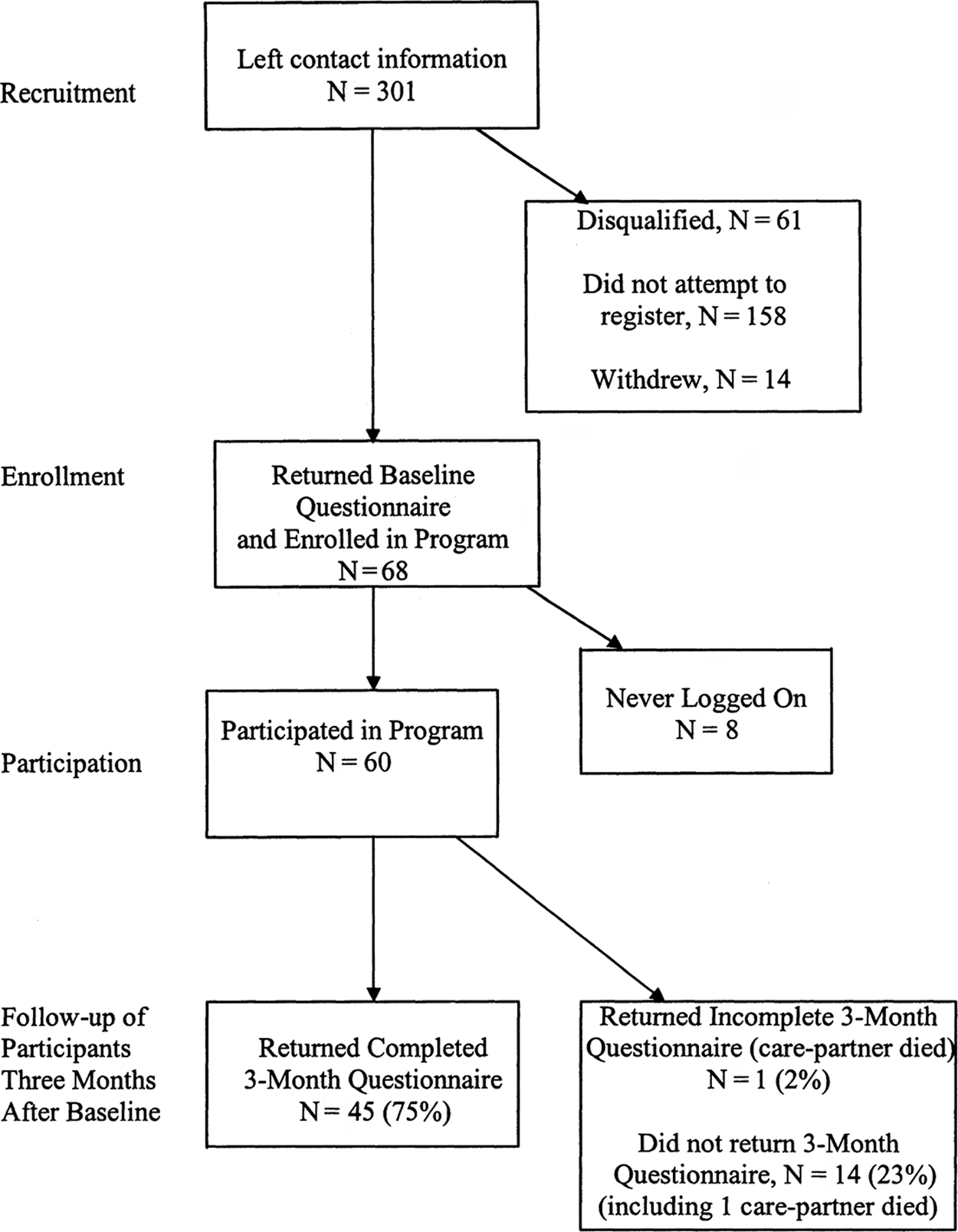
A total 301 respondents left contact information. The most popular referral source was the Veterans Affairs (29%), followed by e-mail or online sites (19%), and other support groups or health associations (16%). Of the 301 respondents, 149 read and signed the consent form and were screened for eligibility; 61 were found ineligible, mainly because they lived outside the target geographic area; 68 were assigned workshops, with 60 logging on at least once. Figure 1 provides the overall details of participant recruitment, enrollment, and follow-up.
Participants in Caregiver Program
Of the 60 participants, 20 (33%) lived in zip codes considered rural by the Department of Veterans Affairs and the U.S. Census.
The majority of caregivers were non-Hispanic-White women, mean age = 57, and mean education level = 15.3 years (Table 2). Thirty-seven percent of caregivers worked for pay. All of these reported that they made changes in their work situation because of caregiving (e.g., reduced hours, leave, etc.). Twenty percent of the caregivers were Veterans. Sixty-two percent of caregivers were the spouses of their care partner, and 20% were parents. Most lived with their care partner (74%).
Caregiver and Care Partner Baseline Means (N = 60)
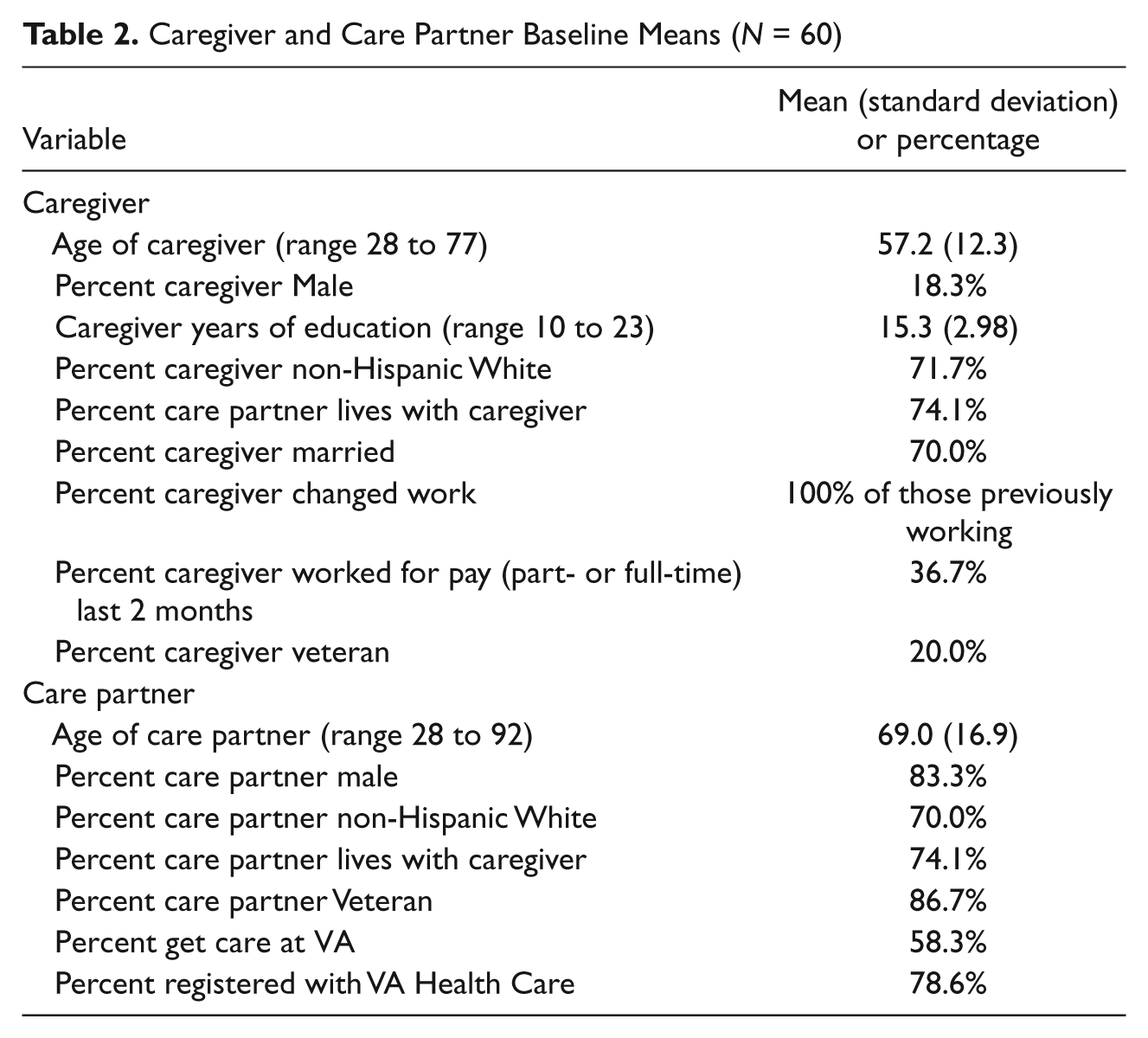
Care partners were older than caregivers (mean age = 69) and more likely male (83%). Approximately 70% were non-Hispanic Whites. The most common condition was dementia (68%), followed by PTSD (32%) and TBI (17%). Most care partners were Veterans (87%). Although 79% were registered with the VA Health Care System, only 58% received their health care through the VA.
Forty-five of the original 60 registered participants completed 3-month follow-up questionnaires. Two care partners had died; of the remaining 58 participants, 78% submitted follow-ups.
Table 3 shows 3-month outcomes. Among health indicators, participants showed significant reductions in the Zarit Burden Inventory, depression, pain, and stress. Caregiver perceived self-efficacy improved significantly, and aerobic and strength/flexibility exercise were significantly increased. Care partners overall health improved. There were no significant changes in health care utilization. The significant changes represent effect sizes (changes in terms of baseline standard deviations) ranging from .22 (Zarit Burden Inventory) to .70 (reduction in stress).
Baseline and 3-Month Change Scores, Caregivers (N = 45)

Note: The means for the two “days miss work” variables are based only on those who worked at baseline and 3-months (N = 15) or those who worked at baseline (N = 32) for the intent-to-treat probability. Probabilities are from paired t tests. Standard deviations are shown in parentheses after the mean values. Effect sizes are the change score divided by the baseline standard deviation. Statistically significant probabilities (.05 or less) are bolded. Baseline means are for the 60 cases who returned 3-month data. Intent-to-treat analyses assume no changes for those missing 3-month data.
There were also several questions in the 3-month questionnaire about changes in caregiving, living arrangements, and employment. Fourteen (33%) of the 45 participants reported having more help at 3 months. One respondent (2%) had less help because of funding cuts. Twelve of the 45 respondents reported needing more care due to the care partners’ worsening conditions (such as more memory impairment), 1 reported improvement (“more independent now”), 5 reported merely that they had more caregiving, and 8 mentioned a switch to more outside caregivers (including hospice). There were 5 care partner residence changes but only 2 (4%) reported a change from living at home to a care facility (one was for temporary rehabilitation after a fall). One other change was from a care facility to home and two were moves to different home residences.
One person who had been working full-time (out of only 7 working full-time) reported losing her job because of her care partner’s medical needs. Twenty-four people were not working at all at baseline (53%), and 29 people were not working at three months (64%).
Among those working at both times (N = 15), at baseline there was M = 9.5 days of work missed in the past 2 months due to caregiving and M = .5 days due to sickness. At 3 months, the participants reported M = 4.1 days missed due to caregiving and M = 1.5 due to sickness.
Of the 60 registered participants, 59 participated in at least one session. Sixty-three percent of respondents logged at least 4 weeks, and 45% logged on all 6 weeks. Mean sessions participated in was M = 4.2 (SD = 2). There were high participation rates in the workshops with M = 16.2 (SD = 16) logins over the 6 weeks, M = 670 (SD = 594) pages visited, and M = 36.9 (SD = 43) posts per participant. Within each workshop, there were 450 to 900 posts.
Discussion
In a review of support interventions for dementia caregivers, Thompson et al. (2007) included four technology-based interventions, but found no evidence such programs improved health outcomes. The current program differs from those earlier programs by including social networking with an emphasis on active problem solving. This allows peer modeling and feedback from moderators and other participants in a manner designed to improve self-efficacy.
Recruitment
Recruiting for this pilot was more difficult than anticipated. The inclusion criteria were narrow in terms of participant characteristics and geography. Twenty-eight percent of those expressing interest were from outside the study area. When possible, Internet-based studies should be opened to a national population. Second, the VA currently has no systematic means of directly reaching caregivers. This is partially due to HIPAA restrictions and partially to underdeveloped infrastructure for supporting family caregivers. There was a contact link on My Healthy Vets (the VA website), but it took five clicks to find it. There was no systematic way of reaching those who did not receive care from the VA—64% of all Veterans (National Center for Veterans Analysis and Statistics, 2009).
Three-Month Outcomes
Nearly all health indicators and behaviors improved. Even with only 45 cases, many improvements were statistically significant. Effect sizes improvements of .22 to .70 compare favorably to effect sizes found in meta-analyses (.14 to .41) of earlier interventions (Thompson-Gallagher & Coon, 2007), although randomized control comparisons would be required to confirm these results.
Workplace absence because of caregiving is a major concern. Although not statistically significant, a mean reduction of 4.5 missed working days could have implications for caregivers and their employers if confirmed with a larger sample. There was little indication that the program reduced medical utilization.
Limitations
This was a small pilot study, limited in the number of participants and length of follow-up. Because the study did not have a control group, it is possible that caregivers not in the workshop might have improved similarly. Of greatest concern is the possibility that “dropouts” who failed to return follow-up questionnaires were those who benefited least, leaving mainly those who benefited in the follow-up. The few baseline differences between “dropouts” and completers suggest this is not highly likely. In addition, the large number of measures increases Type 1 error likelihood, although the consistency of the results over a large number of measures argues in favor of the program being beneficial.
Program Acceptance
Caregivers often have a difficult time leaving their care partner to obtain support. We presented support program that allowed easy access. Based on the number of weeks of participation, the number of posts, and the number of logins, it would appear that that BBC was user-friendly. It was valued by the participants; we received numerous unsolicited emails expressing gratitude.
A problem for many programs is reaching people in rural areas. The rural participants in this program (33%) compares favorably to 20% of the U.S. population (United Nations Department of Economic and Social Affairs, 2008) and is close to the 38% of Veterans in rural areas (U.S. Department of Veterans Affairs, 2010). An Internet-based program such as BBC can successfully reach rural populations.
Policy Implications
Participants found BBC acceptable and useful. This pilot targeted Veterans, but the care partner mean age of 69 suggests the program might be useful for a broader population of caregivers. The positive indications suggest that future research is warranted and that a sufficiently powered, randomized trial should be undertaken.
Footnotes
Acknowledgements
We wish to thank Stephanie Ross, Audra Garder, and Christina Lum for assistance with implementing the workshops.
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
The pilot program was funded by the Department of Veterans Affairs National Caregiving Initiative.