
Abstract
Previous research has established a link between sleep quality and psychological well-being in older adults. However, no research to date has investigated this relationship in the context of other factors known to influence both sleep and psychological well-being. Among a sample of 489 independently living older adults (ages 60 to 98), the current study examined the association between sleep quality and psychological well-being (positive emotions, negative emotions, depression) while controlling for individual differences in factors known to affect sleep: physical health, stress, physical activity, functional ability, and demographics. Multiple linear regression models showed that both better current sleep quality and better comparative sleep quality (from middle to older adulthood) predicted better psychological well-being. Implications include interventions to improve sleep quality in older adults.
The numerous benefits of good quality sleep are well known. Unfortunately, sleep quality often declines with age and sleep complaints become more common in later life, with 26% to 34% of older adults suffering from insomnia (Foley et al., 1995; Schubert et al., 2002). Such findings point to the conclusion that reduced sleep quality is simply a natural part of aging. However, sleep complaints are generally attributed to poor health rather than to the aging process itself. For example, Vitiello, Moe, and Prinz (2002) found that, after excluding individuals with existing health problems, few (1% to 3%) healthy older adults complained of sleep problems or had disturbed sleep. Foley, Ancoli-Israel, Britz, and Walsh (2004) came to the same conclusion using data from the National Sleep Foundation’s survey of older adults. Results from their study showed that self-reported sleep quality was associated with number of medical conditions; few (10%) older adults without medical conditions rated their sleep as fair or poor, whereas up to 40% of older adults with one or more medical conditions rated their sleep as fair or poor.
Sleep Quality and Psychological Well-Being
Aside from its ties to physical health, sleep quality plays an important role in psychological well-being in later life. Research has repeatedly shown a positive relationship between good quality sleep and psychological well-being (e.g., Foley et al., 2004; Morin & Gramling, 1989). In particular, Manocchia, Keller, and Ware (2001) studied sleep in chronically ill adults and found that individuals who lacked sleep problems reported a better overall quality of life compared with those who had trouble sleeping or suffered from a sleep disorder. Likewise, Schubert et al. (2002) concluded that, among older adults who were 53 years of age or older, poorer quality sleep was associated with diminished quality of life. Even after controlling for potentially confounding variables such as chronic health conditions, smoking, and education, an increase in number of insomnia traits was associated with a significant decrease in every quality of life domain, including emotional and mental health.
Similarly, research investigating the link between sleep and mood revealed a bidirectional relationship in which both positive and negative moods impacted subsequent sleep quality, which in turn affected later mood (Berry & Webb, 1983). Other research supports the finding that sleep is related to both prior and subsequent states of psychological well-being, including mood and social interaction (Totterdell, Reynolds, Parkinson, & Briner, 1994). Most recently, McCrae et al. (2008) found significant relationships between subjective sleep quality and affect in a sample of older adults who were 60 years of age or older. Over the course of 2 weeks, better quality sleep was associated with more positive affect, and likewise, poorer quality sleep was associated with more negative affect. These linkages of sleep with both positive and negative affect were found when assessing variance within subjects by comparing across days as well as between subjects in comparing “good sleepers” with “poor sleepers.”
Examination of the impact of sleep quality on psychological well-being cannot be complete without consideration of sleep quantity. Without at least a minimum amount of sleep, restfulness and other indicators of good sleep quality would not be possible (Åkerstedt, Hume, Minors, & Waterhouse, 1994a). Sleep quantity is also associated with psychological well-being. In one of the first studies examining the relationship between sleep and affect, Berry and Webb (1983) found that, in their sample of middle-aged women, more total hours of sleep was associated with more positive affect.
Correlates of Sleep Quality and Psychological Well-Being
Taken together, previous research has identified a solid link between sleep quality and psychological well-being. In older adults specifically, good sleep quality has been associated with improved quality of life and more positive mood. However, despite considerable empirical evidence that sleep quality and psychological well-being are positively associated, this relationship may be more complex than initially presumed. That is, several factors, including sleep quantity, physical and functional health, stress, and physical activity, have been found to predict psychological well-being, and these factors are also correlated with sleep quality.
As previously discussed, many sleep problems experienced in later life occur with medical conditions. Physical health problems are also associated with psychological disturbances, with poor physical health frequently comorbid with depressive symptomatology in older adults (Beekman et al., 1997; Djernes, 2006; Geerlings, Beekman, Deeg, & van Tilburg, 2000). Additional research has focused on elucidating the specific aspects of health problems that increase the risk of diminished psychological well-being. Multiple cross-sectional (Zeiss, Lewinsohn, Rohde, & Seeley, 1996) and longitudinal (Roberts, Kaplan, Shema, & Strawbridge, 1997; Turvey, Schultz, Beglinger, & Klein, 2008) studies have concluded that functional limitation, as well as poor physical health, predicts depression.
Aside from physical health and functional ability, psychological well-being is associated with stress, even as stress is measured in a variety of ways. Variation in mood correlates with daily stressors (Bolger, DeLongis, Kessler, & Schilling, 1989), with older adults experiencing more negative affect with daily stressors than younger adults (Mroczek & Almeida, 2004), and global stress has been found to predict depression in older adults (Norris & Murrell, 1984). Similarly, Tyler and Hoyt (2000) concluded that, for older adults 55 to 69 years of age, the experience of an acute stressor was a significant predictor of depressive symptoms. A 10-year longitudinal study of older adults found a cyclical relationship, such that stressors were associated with later increases in depressive symptoms which were then associated with increased number of stressors (Moos, Schutte, Brennan, & Moos, 2005).
Along with physical health and perceived stress, physical activity is a third factor that predicts psychological well-being. In a longitudinal study of older adults, Strawbridge, Deleger, Roberts, and Kaplan (2002) found that participants who reported high levels of physical activity were less likely to be depressed than those who reported less physical activity. Physical activity also served as a protective factor against subsequent depression 4 years later. In older adults, physical activity has been associated with improved quality of life in general (for a review, see Rejeski & Mihalko, 2001), improved life satisfaction (Mihalko & McAuley, 1996), and better health-related quality of life (Brawley, Rejeski, & Lutes, 2000).
In addition to serving as predictors of psychological well-being, functional ability, stress, and physical activity are correlated with sleep quality. Like physical health, more generally, functional ability is linked to sleep quality. Adults with insomnia display a diminished ability to complete daily tasks compared with adults without insomnia (Roth & Ancoli-Israel, 1999). In older adults specifically, sleep complaints have been associated with greater limitations in daily living activities (Foley et al., 1995).
Stress is also related to poorer sleep. Although good and poor sleepers do not tend to differ in objective counts of life stressors, the level of perceived stress associated with those life events is greater for insomniacs and poor sleepers than for good sleepers (Friedman, Brooks, Bliwise, Yesavage, & Wicks, 1995; Morin, Rodrigue, & Ivers, 2003). Finally, in older adults, physical activity is associated with sleep quality, with those individuals adhering to an exercise regimen reporting better sleep quality and fewer sleep problems than those individuals who did not exercise regularly (Foley et al., 2004; King, Oman, Brassington, Bliwise, & Haskell, 1997).
Collectively, past research indicates that the positive relationship between sleep quality and psychological well-being may be influenced by factors such as physical health, functional ability, perceived stress, and physical activity. However, no research to date has investigated the relationship between sleep quality and psychological well-being while controlling for these other factors. Determining whether sleep, in the context of these other factors, is an independent predictor of psychological well-being has important implications for the development of interventions to improve psychological well-being in older adults. Whereas physical health and functional ability, for example, are difficult to change, sleep quality may be more malleable. Simple changes in daily routine have proven effective in enhancing sleep quality for individuals without clinical sleep disorders. One easily accessible intervention is music-assisted relaxation, which meta-analysis has found to promote good quality sleep in adults of all ages (de Niet, Tiemens, Lendemeijer, & Hutschemaekers, 2009). Cognitive-behavioral interventions, such as sleep hygiene education and stimulus control, have also been found to be efficacious over time in improving sleep quality of older adults (McCurry, Logsdon, Vitiello, & Teri, 1998). Given the established link between good sleep quality and physical health (Colten & Altevogt, 2006; Reid et al., 2006), if good sleep quality is found to also uniquely predict psychological well-being, attempts to enhance sleep quality could be promoted as a means to improve both physical and mental health outcomes.
The Current Study
Our study extends existing sleep quality literature in three important ways. First, it investigates the unique relationship between sleep quality and multiple measures of psychological well-being (recent positive emotions, recent negative emotions, and depressive symptomatology) while accounting for the potential effects of sleep quantity, physical health, functional ability, stress, and physical activity in a nonclinical sample of community-dwelling older adults. Examining this unique association will allow for understanding whether sleep quality is an independent predictor of psychological well-being in older adults and, if so, will inform interventions for older adults’ sleep. As noted above, sleep quality may be more easily modified than other predictors of psychological well-being, such as physical health and functional ability.
This study also examines the unique relationship between comparative sleep quality from middle to older adulthood and psychological well-being. Investigating the association of both current sleep quality and comparative sleep quality with psychological well-being will produce a more complete understanding of the influence of sleep during the aging process. For instance, a person’s current sleep quality may only be “fair,” but if that determination is an improvement over previous sleep quality, the person may not express a sleep complaint. Conversely, someone who had “excellent” previous sleep quality might view a decline to “good” quality sleep as problematic. Interventions to promote sleep quality depend on this understanding. Meta-analysis has shown behavioral interventions for sleep problems to be effective in older adults (Irwin, Cole, & Nicassio, 2006), and if current sleep quality predicts psychological well-being outcomes differently than comparative sleep quality, additional techniques to improve sleep for the benefit of psychological well-being may be targeted toward a specific age-oriented sleep. For example, methods for the maintenance of sleep quality from middle adulthood through older adulthood may differ from methods for promoting current sleep quality in later life.
Finally, including multiple psychological well-being measures of discrete recent emotions and depressive symptomatology improves upon past research that only investigated the relationship between sleep quality and general affect. Although it is expected that sleep quality will be similarly related to negative affect and depressive symptomatology, an empirical investigation of these individual relationships will allow for well-rounded conclusions regarding the link between sleep and psychological well-being. That is, understanding whether the impact of sleep quality on day-to-day emotions is similar to its impact on depressive symptomatology is key to designing interventions to assist both individuals with moderate negative emotions and subsyndromal depression and those with more severe symptoms of depression.
Method
Participants and Procedure
Individuals who met the following criteria were eligible to participate in the current study: at least 60 years of age, living independently within the community (vs. a personal care facility), and able to complete the survey without the assistance of a proxy. Of the 1,106 potential participants who were contacted by telephone, 489 met all eligibility criteria and agreed to participate, resulting in a response rate of 44.21%. The final sample was composed of 213 men and 276 women whose ages ranged from 60 to 98 years. The sample was well educated, with 82.6% of the participants reporting a bachelor’s or higher degree, and racially homogenous, with 99% of the participants identifying as White.
For the majority of participants (82%), an individual in-person interview was conducted either in a private room on the university campus (n = 370, 76%) or in the participant’s home (n = 30, 6%). During these interviews, trained interviewers read each question aloud and recorded the participant’s responses. For the remaining participants (n = 89, 18%), surveys that were identical to the in-person interviews were mailed with written instructions that allowed participants to complete the survey independently. Both the in-person interviews and mailed surveys took approximately 1 h to complete and included a variety of topics related to physical and psychological health. Participants received monetary compensation for their time.
Measures
Income
Via a 1-8 scale (1 = <US$5,000; 2 = US$5,000-US$9,999; 3 = US$10,000-US$14,999; . . . 8 = ≥US$40,000), participants were asked to indicate their total household income for the past year. The majority (69.9%) reported an annual income of ≥US$40,000. Few participants (3.2%) reported an annual income of <US$15,000.
Sleep quality and quantity
Objective and subjective indices of sleep time, onset latency, and general quality are generally poorly correlated (McCrae et al., 2005; Means, Edinger, Glenn, & Fins, 2003). However, recent research shows that the subjective report of sleep quality and quantity is what matters in the association between sleep and affect (McCrae et al., 2008). Therefore, the current study uses self-report for all sleep measures.
Participants provided a rating of their overall sleep quality for the past year, with possible response options of 1 (fair or poor), 2 (good), 3 (very good), 4 (excellent). Then, using the same response options, they rated their overall sleep quality when they were younger. To ascertain sleep quality from a younger age, participants were instructed to think back to “around age 40.” Comparative sleep quality was calculated by subtracting prior sleep quality from current sleep quality, resulting in a range of −3 to +3, with negative scores reflecting a perception of diminished sleep quality, positive scores reflecting a perceived improvement in sleep quality, and zero scores reflecting a perception of maintained sleep quality.
An average of the number of hours dedicated for sleep each day was obtained as a quantitative measure of sleep. Using an open response format, participants indicated the time they usually go to bed and the time they usually wake up. From these numbers, time in hours was calculated.
Self-rated health
As a measure of self-rated health, participants were asked to, given their age, rate their health in general. Response options ranged from 1 (bad) through 5 (excellent). Previous research on older adults’ health has established this single-item measure as a valid and reliable indicator of self-rated health (e.g., Ruthig & Chipperfield, 2007; Spiers, Jagger, & Clarke, 1996).
Functional ability
A 10-item Instrumental Activities of Daily Living (IADL) Scale was used to assess functional ability. This scale consists of tasks necessary for independent living, such as light housework, laundry, and preparing a hot meal, and participants were asked if they were capable of completing each task without assistance (1 = Yes, 0 = No). Responses were summed to create a count of the number of tasks able to be completed independently, with higher scores indicating greater functioning.
Stress
Perceived stress was assessed by using seven items from Cohen, Kamarck, and Mermelstein’s (1983) global measure. Participants were asked how often during the past month they had experienced stressful circumstances (e.g. “could not cope with all the things you had to do”). Responses for each item ranged from 1 (never) to 5 (very often) and were summed with higher scores representing more stress (α = .79).
Physical activity
Consistent with past health and aging research (e.g., Ruthig, Chipperfield, Newall, Perry, & Hall, 2007), participants’ physical activity level was assessed using two items. They were asked to compare their activity, in general, with others their age on a scale from 1 (much less) to 7 (much more), and they were asked to rate their level of physical activity over the past few months (1 = extremely inactive; 7 = extremely active). Responses to these two questions were summed, and participants’ scores reflected the entire possible range from 2 to 14 (r = .66).
Emotions
Using a scale from 0 (never) to 6 (almost always), participants were asked how often they had felt each of 22 emotions during the past 2 days. As in past research (e.g., Chipperfield, Perry, & Weiner, 2003), responses to the 10 positive emotions (e.g., proud, grateful, excited) were summed (α = .86) separately from responses to the 12 negative emotions (e.g., bored, nervous, lonely; α = .86).
Depression
The Center for Epidemiological Studies Short Depression Scale (CES-D 10; Andresen, Malmgren, Carter, & Patrick, 1994) was used to assess depressive symptomatology. Participants noted how frequently during the past week they had experienced depressive symptoms. The 10 items include statements such as “I could not get going” and “I felt lonely,” and, for each, responses ranged from 0 (rarely or none of the time) to 3 (most or all of the time). Responses to positively worded items (i.e., “I felt hopeful about the future” and “I was happy”) were reversed before all responses were summed. Higher total scores indicated more depressive symptoms (α = .79).
Results
See Table 1 for descriptive statistics and bivariate correlations of all study variables.
Descriptive Statistics
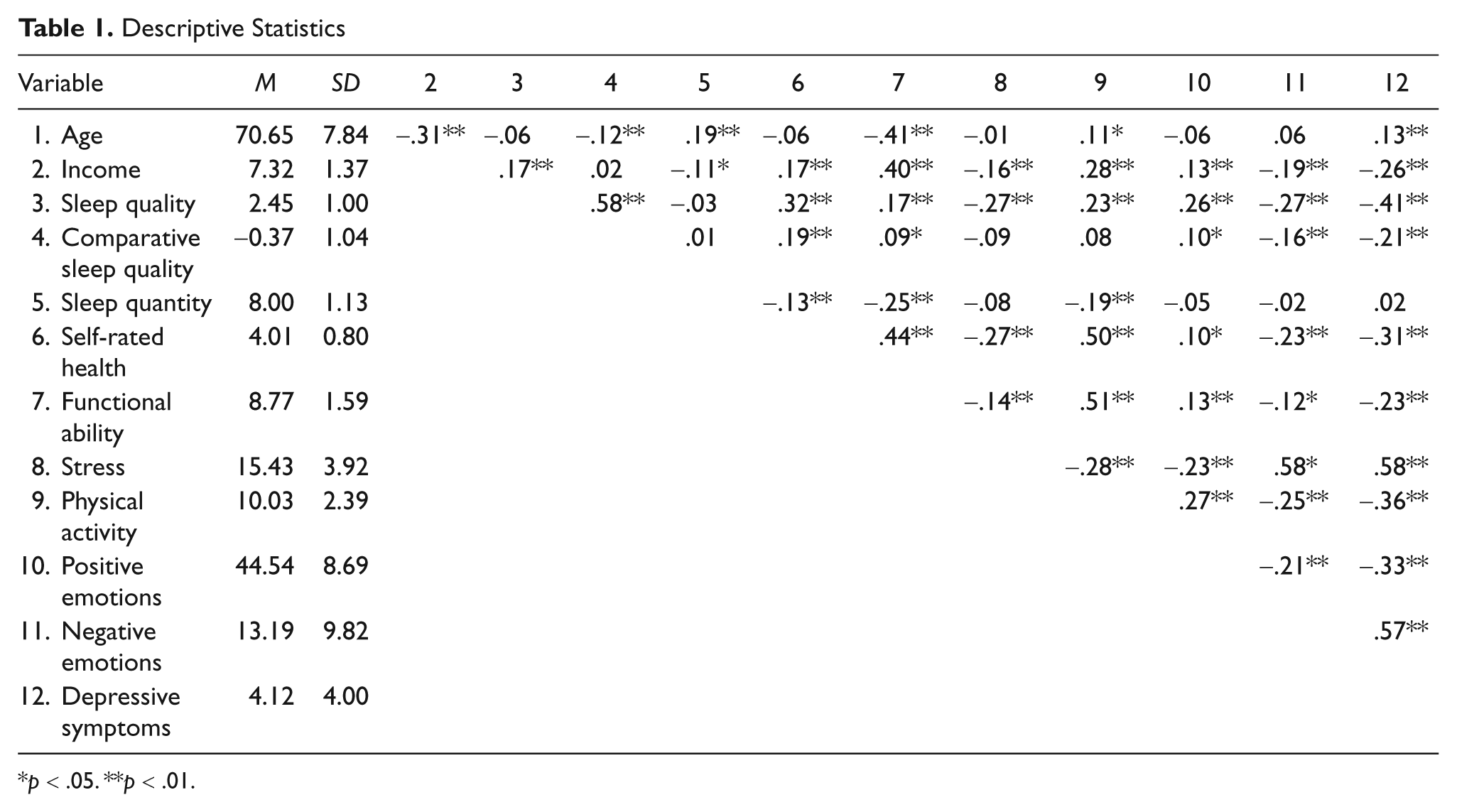
p < .05. **p < .01.
Current Sleep Quality
Three separate OLS regression models were computed using the enter method to identify whether current sleep quality independently predicts frequency of recent positive emotions, frequency of recent negative emotions, and depression after controlling for sleep quantity as well as other physical (physical health, functional ability), psychosocial (perceived stress), and sociodemographic (age, gender, income) variables known to be associated with sleep quality and to influence psychological well-being. In addition to sleep quality and sleep quantity, each regression model included age, gender, income, self-rated health, functional ability, stress, and physical activity as predictors of positive emotions, negative emotions, or depression.
Positive emotions
As shown in Table 2, Model 1, the overall regression model predicting frequency of positive emotions was significant (R2 = .16, p = .000). After accounting for sleep quantity and the physical, psychosocial, and sociodemographic variables, better sleep quality predicted more frequent positive emotions (β = .22, p = .000). In this model, less stress (β = –.15, p < .01) and greater physical activity (β = .24, p = .000) were also significant predictors of more positive emotions. Surprisingly, greater self-rated health (β = –.15, p < .01) predicted fewer positive emotions. Neither sleep quantity, functional ability, nor any of the demographic variables predicted positive emotions.
Current Sleep Quality as a Predictor of Emotions and Depression in Older Adults
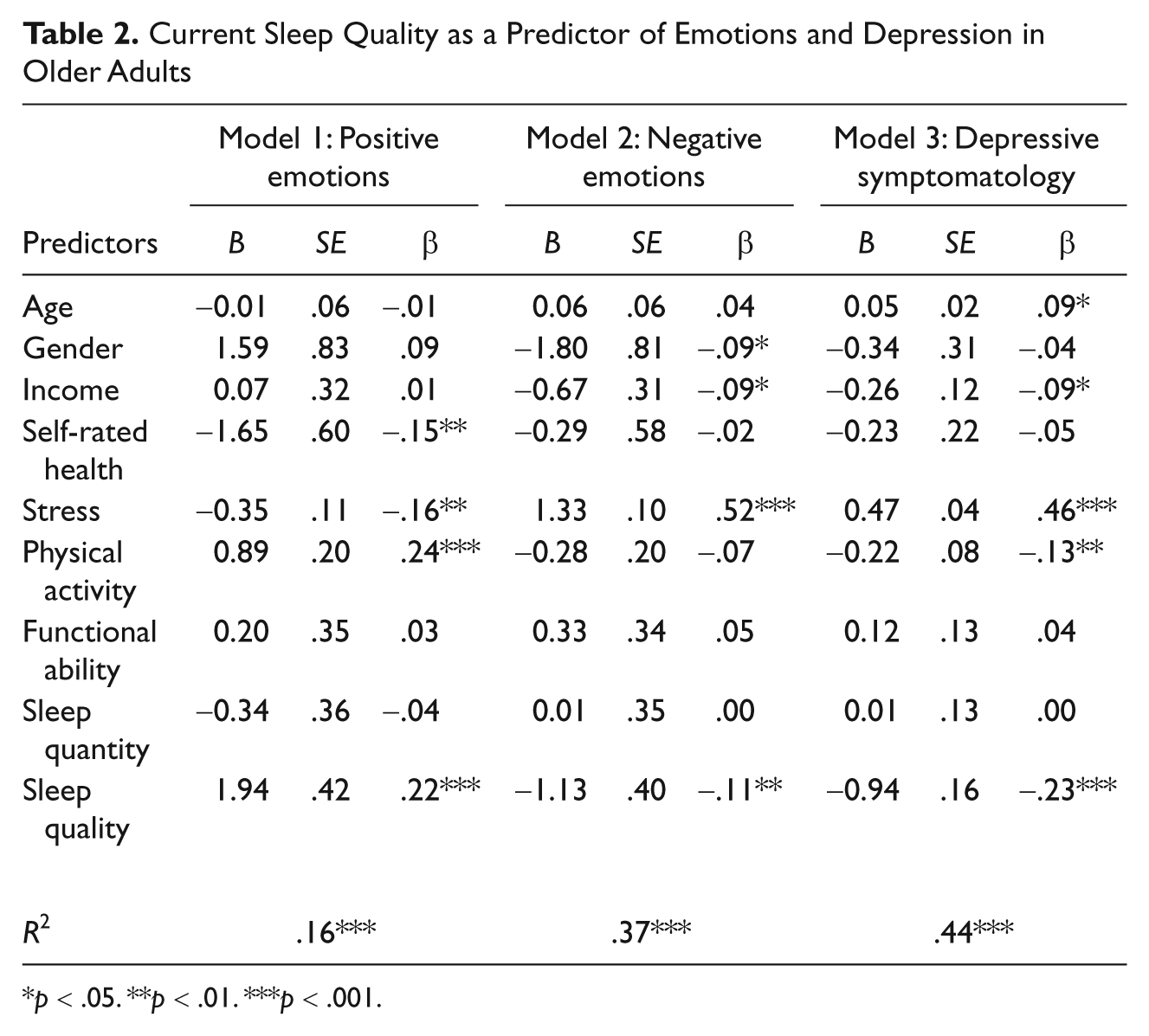
p < .05. **p < .01. ***p < .001.
Negative emotions
The overall regression model predicting frequency of negative emotions was also significant (R2 = .37, p = .000; see Table 2, Model 2). As anticipated, poorer sleep quality predicted more frequent negative emotions (β = –.11, p < .01), as did greater stress (β = .52, p = .000). Gender was also a significant predictor (β = –.09, p < .05), with men reporting more frequent negative emotions. Finally, lower income predicted more negative emotions (β = –.09, p < .05).
Depression
As depicted in Table 2, Model 3 and consistent with the model for negative emotions, the regression model predicting depression was significant (R2 = .44, p = .000) and poorer sleep quality predicted more depressive symptoms (β = –.23, p = .000). However, compared with the model for negative emotions, this model has different additional significant predictors. Increased stress predicted greater depression (β = .46, p = .000), as did less physical activity (β = –.13, p < .01). Of the demographic variables, age (β = .09, p < .05), as well as lower income (β = –.09, p < .05), predicted greater depression.
Comparative Sleep Quality
Participants reported better sleep when they were younger (M = 2.82, SD = .94) compared with the past year (M = 2.45, SD = 1.00), t(484) = −7.81, p < .001. Because of this significant difference in sleep quality, three additional OLS regression models were computed to investigate whether the comparison between sleep quality in younger and older age would predict the dependent variables of positive emotions, negative emotions, and depression. The same quantitative sleep and physical, psychosocial, and sociodemographic variables that were used in the previous models were also included in these models.
Positive emotions
As shown in Table 3, Model 1, the significant overall model predicting positive emotions (R2 = .13, p = .000) mirrored the model that used current sleep quality as a predictor, such that comparatively better sleep quality predicted a greater frequency of positive emotions (β = .10, p < .05), as did less stress (β = –.19, p = .000) and greater physical activity (β = .25, p = .000). Greater self-rated health (β = –.12, p < .05) again predicted less frequent positive emotions.
Comparative Sleep Quality as a Predictor of Emotions and Depression in Older Adults
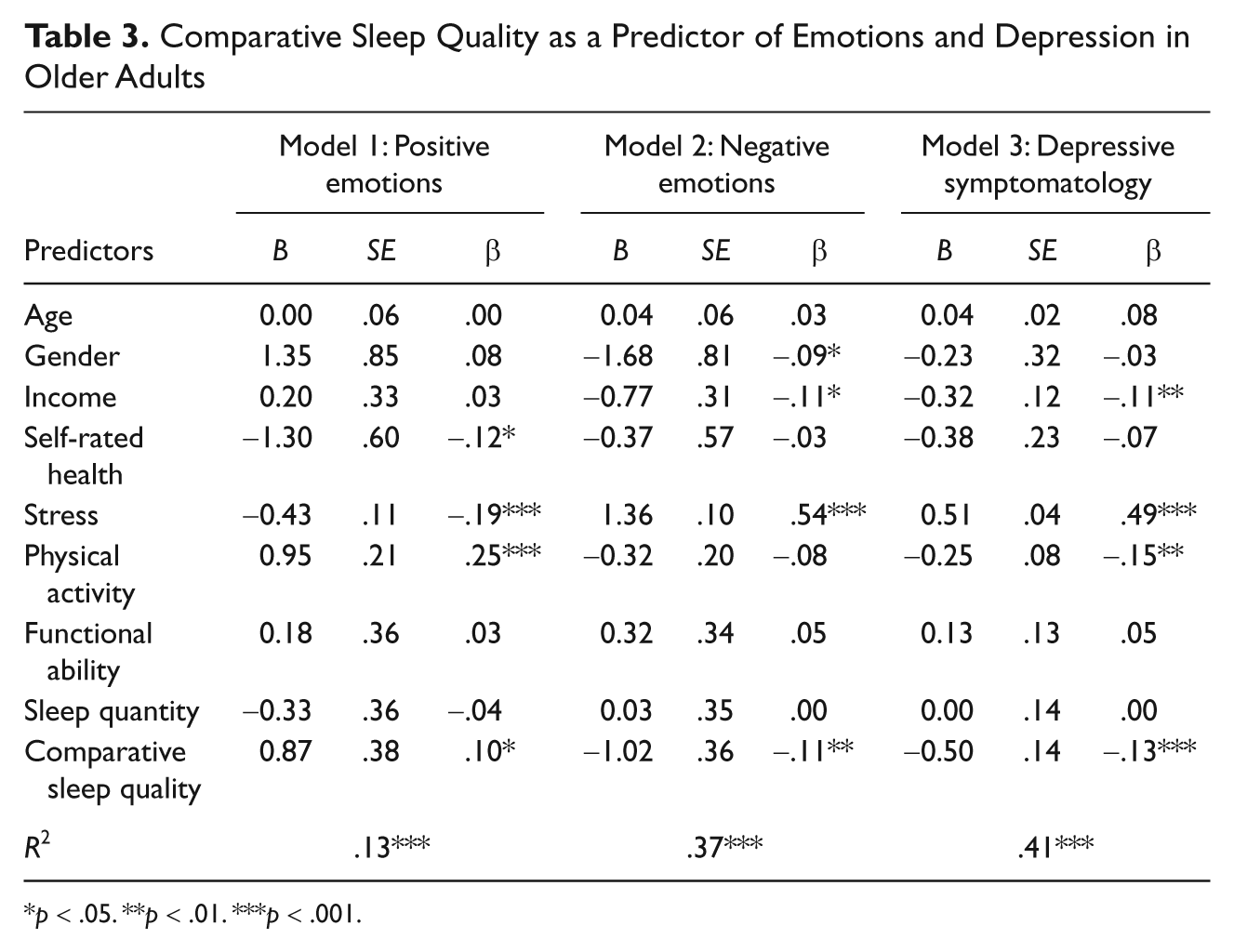
p < .05. **p < .01. ***p < .001.
Negative emotions
The model predicting negative emotions (Table 3, Model 2) was also significant (R2 = .37, p = .000) and mirrored the previous model that included current sleep quality (see Table 2). Comparatively worse sleep quality predicted more frequent negative emotions (β = –.11, p < .01), as did greater stress (β = .54, p = .000). Lower income predicted more frequent negative emotions (β = –.11, p < .05), and gender was again a significant predictor (β = –.09, p < .05), with men reporting more frequent negative emotions.
Depression
The last regression model significantly predicted depressive symptoms (R2 = .41, p = .000; see Table 3, Model 3). As shown in this model, comparatively worse sleep quality also predicted greater depression (β = –.13, p = .000). Unlike in the prior model for depression (Table 2), age was not a significant predictor. However, increased stress (β = .49, p = .000), less physical activity (β = –.15, p < .05), and lower income (β = –.11, p < .01) were again predictors of greater depression.
Taken together, these results reveal that, even after accounting for quantity of sleep and physical, psychosocial, and sociodemographic variables known to be associated with sleep quality and to influence psychological well-being, good current quality sleep and comparatively better sleep quality from middle to older adulthood predict better psychological well-being, as evidenced by more frequent positive emotions, less frequent negative emotions, and fewer depressive symptoms.
Discussion
Research has established a link between sleep quality and psychological well-being among older individuals, particularly as assessed by emotions (McCrae et al., 2008). However, investigations of this association thus far have not accounted for several important factors that influence this relationship. The current study examined the unique association of older adults’ sleep quality with their psychological well-being while accounting for individual differences in physical health, functional ability, perceived stress, physical activity, sleep quantity, and the sociodemographic variables of age, gender, and income.
Sleep Quality Predicts Psychological Well-Being
Even after accounting for age, gender, income, self-rated health, functional ability, stress, physical activity, and sleep quantity, sleep quality predicted multiple measures of psychological well-being. Specifically, both better current sleep quality and a perceived improvement in sleep quality predicted more frequent positive emotions, as well as less frequent negative emotions and fewer depressive symptoms. These results indicate that good quality sleep, as measured currently or in comparison with past sleep quality, is independently associated with psychological well-being benefits.
Research investigating the underlying processes that comprise the subjective assessment of sleep quality has focused on correlating sleep quality measures with other measures, including objective measures such as polysomnography. Riedel and Lichstein (1998) found that longer durations of deep sleep and shorter time needed to fall asleep were associated with higher ratings of sleep quality by older adults. Likewise, good quality sleep has been linked to sleep continuity in young women (Åkerstedt, Hume, Minors, & Waterhouse, 1994b) and both adults with insomnia and normal sleepers base their determinations of sleep quality on subjective feelings the next day, such as feeling well-rested (Harvey, Stinson, Whitaker, Moskovitz, & Virk, 2008).
Although informative, neither these research studies nor others have investigated the social cognitive processes that more broadly underlie the appraisal of sleep quality. Evaluative judgments are comparative against a standard (Kahneman & Miller, 1986; Schwarz, 1999). That is, individuals cannot determine whether their sleep is “good” or “poor” without comparing it with some standard or norm for what constitutes that level of sleep quality. These comparisons might take the form of social comparisons by comparing with reports by other people their age or individuals might compare their sleep to what they understand to be an objective standard (e.g., 8 h of uninterrupted sleep is good).
By measuring sleep quality in two ways, both currently and compared with earlier in life, the current study provides a more complete understanding of the way sleep quality is related to psychological well-being in older adults. A determination of subjective quality relies on some type of comparison. Regardless of whether individuals assess their sleep quality using a benchmark from earlier in life or a comparison with similar others, the relationship with psychological well-being is the same. Therefore, sleep-improvement interventions for older adults may be tailored using either or both methods as part of the determination of sleep quality.
Furthermore, the inclusion of a quantitative measure of sleep in addition to the measures of sleep quality allows for understanding of the predictive power of sleep quality separate from that of sleep quantity. Whereas sleep quality was a significant predictor in each of the six models, sleep quantity did not predict any of the psychological well-being outcomes. The link between sleep quality and psychological well-being, as well as the absence of a link between sleep quantity and psychological well-being, demonstrates the importance of considering older adults’ sleep complaints even in the absence of quantifiable sleep deficits. When considering implications for psychological well-being, perceived sleep quality may be just as important, if not more important, than simply the number of hours spent sleeping.
Other Predictors of Psychological Well-Being
More frequent positive emotions were also predicted by less stress and more physical activity in both the current sleep quality and comparative sleep quality models. These findings confirm previous research that established links between affect and stress (Mroczek & Almeida, 2004) as well as between emotions and physical activity (Strawbridge et al., 2002). Self-rated health was also a significant predictor of positive emotions in both models but not in the anticipated direction. Poorer self-rated health predicted more frequent positive emotions. As the sample in this study had predominantly high ratings of self-rated health with relatively little variability, a downward shift in self-rated health likely reflects a shift in ratings from excellent to very good versus from good to bad. That is, “poorer” self-rated health still represents moderate-to-good, rather than “poor,” health.
The two models predicting negative emotions had the same significant predictors. In addition to poor sleep quality or perceived diminished sleep quality over time, greater perceived stress and a lower income predicted a greater frequency of negative emotions. Men also reported more frequent negative emotions than women. Although this result seems counterintuitive to findings that women are generally more emotionally aware and expressive than men (Feldman Barrett, Lane, Sechrest, & Schwartz, 2000; Fischer & Manstead, 2000), it is possible that the men in our sample were more comfortable expressing the specifically negative emotions than were the women (Fabes & Martin, 1991).
When considering depressive symptoms as a component of psychological well-being, both the current sleep quality and the comparative sleep quality models included more stress, less income, and less physical activity as predictors of depression. These results are consistent with previous research that found associations between depression and high levels of stress (Norris & Murrell, 1984) as well as low levels of physical activity (Strawbridge et al., 2002). In addition to improving sleep quality, older adults might pursue stress reduction techniques and physical activity as means for reducing symptoms of depression. Finally, in the current sleep quality model, age was also a significant predictor, such that older age was associated with more depressive symptoms.
Implications
The link between sleep quality and psychological well-being underscores the importance of good sleep quality in older adults. While many older adults experience sleep problems, evidence exists for the effectiveness of behavioral interventions to improve sleep quality (for a review, see Irwin et al., 2006). Unlike pharmacological interventions which are accompanied by concerns of dependence and undesirable side effects, behavioral interventions are ideal for long-term use and are readily available for older adults. Relaxation techniques, for example, have been shown to improve sleep quality in older adults and such improvements persist over time (Lichstein, Riedel, Wilson, Lester, & Aguillard, 2001).
Together, these findings reveal that psychological well-being is associated with many factors in addition to sleep quality. However, these factors might be less malleable in older adults than sleep quality. For example, older adults with physical limitations might have great difficulty increasing their physical activity in an effort to promote psychological well-being. In addition, simple interventions such as easily accessible health promotion programs have not been found to predict older adults’ exercise at 1-year follow-up (Sharp & Connell, 1992). Increasing income is also likely to be difficult for most people and especially for older adults. However, stress reduction could benefit older adults and is included in many of the behavioral treatments to improve sleep quality as well.
With the exception of age as a predictor of depressive symptoms only in the current sleep quality model, both the current sleep quality and sleep quality change models had the same significant predictors for all psychological well-being outcome variables. These parallel findings support the use of either the current or retrospective measurement technique as part of the appraisal of sleep quality in older adults.
Limitations and Conclusion
This study utilized a cross-sectional design, thereby preventing the associations between sleep quality and psychological well-being from being interpreted as causal relationships. Longitudinal studies have confirmed the effectiveness of sleep interventions in improving sleep quality over time (Pallesen et al., 2003), and future research should investigate the potential for improvement in psychological well-being along with better sleep quality. A longitudinal cross-lagged panel study could expand on this study to determine the direction of the relationship between sleep quality and psychological well-being.
Participants rated their sleep quality over the past year. It is possible that the retrospective nature of this assessment may have resulted in less accurate reporting than a more immediate measure, such as a daily sleep diary. However, this measure allows for a more general understanding of the participants’ sleep quality at the present time. Rather than assessing sleep quality within only the past week or month, during which time the participant might have experienced anomalous sleep due to a specific life experience (i.e., acute illness or stressful event), using the past year as a reference produces a more accurate description of sleep quality in general.
Likewise, previous sleep quality was also assessed using a retrospective measure with participants asked to reflect to “around” age 40. It is possible that this instruction may have elicited slightly different time periods for different participants and that certain life events might have occurred during that time which influenced sleep quality. Again, however, this measure captures sleep quality in general during younger age.
The sleep quantity variable was also somewhat limited. Although the variable captures the amount of time typically dedicated to sleep, it does not precisely measure time spent sleeping. The use of objective measures such as actigraphs in future research would allow for a more accurate reporting of time spent sleeping.
To explore the variables associated with psychological well-being and sleep quality, multiple time periods were employed. For example, stress was measured over the past month, whereas the depression scale asked participants to reflect over the past week, and sleep quality was assessed over the past year. Although all of the measures are psychometrically sound, future research might explore the relationships between the variables using the same time reference as well as daily sleep diaries for an immediate measure of sleep quality.
The sample for this study was relatively homogeneous, as the majority of participants were well educated, White older adults who rated their physical health as good. Future research should explore whether these findings extend to more diverse samples of older adults. Specifically, sleep quality may be differentially associated with psychological well-being in older adults in poor physical health or those with mental illness. In addition, as our sample consisted solely of independently living older adults, these findings might not extend to individuals who reside in nursing or personal care homes.
Despite the limitations, the results of this study contribute to the body of literature related to sleep quality and psychological well-being by demonstrating the unique link between the two while controlling for other factors known to influence the relationship. After controlling for self-rated health, stress, physical activity, functional ability, and demographics, both good current sleep quality and improved sleep quality over time predicted more frequent positive emotions, less frequent negative emotions, and less depression. These findings have implications for developing interventions aimed toward improving older adults’ sleep quality as a possible means to also influence psychological well-being.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support for the research and/or authorship of this article.