
Abstract
This article examines change in the composition of the Texas nursing home population between 1990 and 2009 in relation to the changing prevalence of diabetes. Data from the federal Minimum Data Set for Texas for 1999 and 2009 were analyzed for change in proportion of age groups by the Two-Sample Proportion Test. Change by gender within age groups while controlling for race/ethnicity was analyzed by the Cochran–Mantel–Haenszel test. The percentage of nursing home residents aged 50 to 64 years increased from 8% in 1999 to 12% in 2009, and the change was statistically significant for each race/ethnic group and both genders. The percentage reporting diabetes increased among all groups with more pronounced change for minorities. These results point to a need for closer examination of the impacts of changing diabetes prevalence on nursing homes.
Introduction
The changing prevalence of diabetes for the general population has become a focus of policy attention for the United States and other nations in recent years. Relatively little of this attention, however, has been directed toward the impact of this trend on the older population and those residing in nursing homes. The increased prevalence of diabetes in the general population and among children is frequently attributed at least partially to the increased prevalence of obesity, and these trends have also affected the patterns of disability in the larger society (Bhattacharya, Choudhry, & Lakdawalla, 2008). Planning to provide quality care that meets the needs of the afflicted at a bearable cost would be facilitated by a clear picture of how the nursing home population has changed in response to increased diabetes prevalence in the larger society. Demographics offer a major impetus for concern regarding long-term care as the U.S. population aged 65 and older is projected to increase from 12% in 2000 to 20% by 2030 and accounts for roughly a third of health care expenditures (Arterburn, Crane, & Sullivan, 2004). Examining the possibility that increased diabetes prevalence has affected the composition of the nursing home population in terms of proportions by gender, ethnicity, and age groups can offer insights into meeting the needs of the long-term population at an acceptable cost.
Nursing homes include residents of all backgrounds; but in past decades, the population has consisted predominantly of very old (85+) disabled White women (Kane, Kane, & Ladd, 1998). The existing literature suggests an influx of working-age residents into nursing homes for reasons related to diabetes; so this points to the possibility of a more diverse nursing home population by gender, ethnicity, and age group (N. A. Miller, Pinet-Peralta, & Elder, 2012). These developments imply that the case-mix of diseases and disorders among nursing home residents may have changed, particularly in regard to the co-morbidities for diabetes. If such change has materialized, the requirements for serving this population in terms of staffing skills and equipment may have also changed.
Analyzing data for the State of Texas offers insights into the impact of increased diabetes prevalence on nursing home populations for several reasons. One is that Texas ranked as the second most populous state with a diverse population that was 37.6 % Hispanic (Ennis, Ríos-Vargas, & Albert, 2011) and 12.6% non-Hispanic Black in 2010 (Rastogi, Johnson, Hoeffel, & Drewery, 2011). The percentage of adults overweight or obese for Texas increased from 49.4% in 1990 to 64.1% in 2005 (Combs, 2011). For 2009, the percentage of obese White adults was 25.7% while the figure for Blacks was 35.7% and 36.4% for Hispanics (Combs, 2011). These increases in the levels of obesity have been greater than many other states and indicate a high risk of diabetes for much of the population (Combs, 2011).
The rapidly increasing Hispanic population is another reason for interest in developments for Texas. The Hispanic population for the United States grew from 35,305,818 (12.5%) in 2000 to 50,477,594 (16.3%) in 2010. For Texas, the Hispanic population increased from 6,669,666 (32.0%) to 9,460,921 (37.6%) during this time (Ennis et al., 2011). The percentage of Hispanics below the poverty level for Texas (22.5%) was noticeably higher than the overall figure for the United States for 2007-2011, that is, 14.3% (Macartney, Bishaw, & Fontenot, 2013). Examination of diabetes among Hispanic nursing home residents in Texas may offer insights into long-term care policy that can apply in other places with substantial Hispanic populations. The state has a relatively high percentage of citizens with income below the poverty level, pointing to the risk that nursing home residents may qualify for public assistance in meeting the costs of long-term care (Bishaw, 2012).
This article will examine change in the Texas nursing home population by gender, within age groups, and by race/ethnicity by analyzing data from the federal Minimum Data Set (MDS) for Texas from the years 1999 and 2009. The change in overall demographic composition of the population along with the prevalence of diagnosed diabetes among various groups will be examined.
Diabetes and Public Policy
Changing diabetes prevalence for nursing home residents is an important matter for public policy for a variety of reasons. One is that nursing home residents are by definition a vulnerable population, so the impacts of increased diabetes prevalence can have consequences that adversely affect the well-being of this population. Another is that nursing home care accounts for a sizable portion of federal and state budgets, and effective policy formulation is enhanced by a clear understanding of the needs and requirements for the population being served. An additional reason is that the trend toward increased diabetes prevalence appears to have varying impacts on different demographic groups, so efficient and equitable allocation of resources may be enhanced by examination of change among these groups.
Regarding the cost of medical care due to increased diabetes prevalence, Herman (2013) pointed out that the number of diagnosed cases in the United States reached 12.1 million in 2002, rose to 17.5 million in 2007, and increased to approximately 22.3 million in 2012. The direct costs for treating these patients accounted for US$176 billion, approximately 12.5% of the total U.S. medical expenses for the year. Herman implied the importance of these developments for long-term care policy as the population aged 65 and older accounts for nearly 59% of diabetes-related expenditures.
The cost of treating diabetes for public sector medical assistance programs has also received attention. A Congressional Budget Office report (2013) found that 49% of those eligible for assistance from Medicare and Medicaid (“dual-eligibles”) were diagnosed with diabetes. Stewart, Grabowski, and Lakdawalla, (2009) observed that the price of service for nursing home residents covered by Medicaid increased faster than overall medical costs from 1977 to 2004.
The relationship among obesity, diabetes, and disability in the general population has been examined. Cheung et al. (2009) found that the prevalence of diagnosed diabetes increased from 6.5% for 1999-2002 to 7.8% for 2003-2006 with significant increases observed for women, non-Hispanic Whites, and the obese. The proportion of increase that was due to greater Body Mass Index (BMI) ranged from approximately 20% to 80%. Bhattacharya et al. (2008) found that increased obesity accounted for 40% of the increase in disability due to chronic illnesses such as diabetes.
Diabetes and Nursing Home Residents
Reviewing the substantial body of literature that applies to changing diabetes prevalence in nursing homes is facilitated by a conceptual framework to call attention to important variables. Andersen (1995) expanded his earlier model of health care utilization (Andersen & Newman, 1973) to focus on the environment (health care system and the external environment), population characteristics (predisposing characteristics, enabling resources, and need), health behavior (personal health practices and use of health services), and outcomes (perceived health status, evaluated health status, and consumer satisfaction). Andersen’s model was directly applied to the risk of nursing home placement for older people by E. A. Miller and Weissert (2000). This work focused on the population characteristics and identified the predisposing characteristics such as age, gender, and race or ethnicity. Age was found to have a strong, consistent relationship with the risk of nursing home placement while the role of gender was unclear. Non-Whites were found at greater risk of nursing home placement than Whites. For the enabling characteristics, income, level of education, and insurance status were not significantly related to the risk of nursing home placement. The risk of institutionalization was increased by living alone and by enrollment in Medicaid. Need factors that related to a greater risk of nursing home placement were identified by poor ratings on self-reported health surveys, deficiencies in performing the activities of daily living (ADLs), and dementia. Heart conditions, hypertension, and depression did not contribute to a greater risk of institutionalization.
The literature regarding diabetes among older people has frequently examined the variables incorporated in the Andersen model. Subsequent inquiry suggests change regarding the predisposing characteristics in response to increasing diabetes prevalence. Meneilly and Tessier (2001) observed a relatively high prevalence of diabetes in the older population, as approximately 20% of those aged 75 and older are afflicted by the condition. These writers pointed out that while diabetes is ranked as the sixth highest cause of death for older people, its impact may be understated as it complicates the treatment of conditions more likely to be listed as the primary cause of death such as cardiovascular disease. Similar findings for diabetes prevalence among Americans aged 60 and older were observed by Jack, Boseman, and Vinicor (2004), again finding nearly 20% of this group diagnosed with the condition.
There has been some examination of the impacts of diabetes on older people of different groups in the general population. Chiu and Wray (2010) found higher prevalence of disability among diabetics for women, minorities, and the less educated and emphasized the detrimental effects that diabetes can have on the quality of life for older people. The complications related to diabetes can contribute to blindness and limb amputation, thus seriously impairing the person’s capacity to carry out ADLs and instrumental activities of daily living (IADLs). Dunlop, Song, Manheim, Daviglus, and Chang (2007) found that deficiencies in capacity to perform ADLs for older people varied by ethnicity and race as Hispanics interviewed in Spanish reported the highest prevalence of disability (23.4%) followed by African Americans (18.01%). Little difference was found between Whites (10.65%) and Hispanics interviewed in English (10.78%).
The variables of gender and race/ethnicity have also been examined in relation to age and diabetes prevalence. Zhang et al. (2010) found that the prevalence of diabetes mellitus for male nursing home residents increased from 16.9% in 1995 to 26.4% in 2004 while the prevalence for female residents increased from 16.1% to 22.2% and the prevalence of co-morbidities did not increase significantly. Resnick, Heineman, Stone, and Shorr (2008) analyzed data from the 2004 National Nursing Home Survey (NNHS) and found that diabetes was a primary or current diagnosis for 24.6% of nursing home residents with substantial disparity between White (22.5%) and non-White (at least 35.2%) residents. Residents diagnosed with diabetes tended to be younger with a mean age of 81.7 years compared with non-diabetic residents with a mean age of 84.9, and the prevalence of diabetes decreased at very advanced ages. Minority residents were more likely to be diagnosed with diabetes than Whites. Nursing home residents diagnosed with diabetes also tended to have a shorter overall length of stay than non-diabetic residents and were more likely to have a stay not exceeding 100 days. Diabetic residents were more likely to have been admitted from an acute care hospital (42.5% compared with 35.3% for non-diabetics) and tended to have more prescriptions for medication than non-diabetic residents.
N. A. Miller et al. (2012) compared nursing home residents for all states aged 31 to 64 years with those 65 years and older using data from the 2000 and 2008 federal MDS. The working-age residents were more likely to be Black or Hispanic and male compared with those 65 and older. The diseases and disorders that appeared most frequently in these working-aged nursing home residents included diabetes, renal failure, chronic obstructive pulmonary disease, asthma, and cardiovascular disorders. These residents were also more likely to have depressive symptoms and diagnosed bipolar disorder and were more likely to have had a previous stay at a psychiatric facility. Diabetes prevalence was also higher for working-age adults compared with those 65 and older.
There has been some direct examination of how the changing prevalence of diabetes has affected nursing home residents along with expressions of concern for how well nursing homes are prepared for an influx of residents with diabetes. Inconsistent results have been found regarding the risk of falling for diabetic nursing home residents. Schwartz et al. (2002) and Maurer, Burcham, and Cheng (2005) found that nursing home residents diagnosed with diabetes were at a greater risk of falls than residents not diagnosed with diabetes, but the findings of Resnick et al. (2008) did not support this conclusion. Resnick et al. also found that nursing home residents diagnosed with diabetes were more likely to have pressure ulcers than those not diagnosed with diabetes. Travis, Buchanan, Wang, and Kim (2004) used the MDS to profile diabetic nursing home residents at admission and found a high prevalence of co-morbidities regarding the cardiovascular and circulatory systems as well as depression and called for greater attention to advanced care planning for diabetic residents. The co-morbidities for diabetes include hypertension, stroke, heart disease, several forms of cancer, depression (Flegal, Carroll, Ogden, & Curtin, 2010; National Institutes of Health [NIH], 2008), and a greater risk of disability (Alley & Chang, 2007); so an increase in diabetes prevalence implies a likelihood that the prevalence of these co-morbidities has also increased.
In summary, the research findings regarding the changing prevalence of diabetes for the older population seem to parallel those for the general population. Variation has been found by gender, ethnicity, and age for the prevalence of diabetes. Research for the long-term care population has indicated similar patterns for nursing home residents and suggests a possibility that some may be entering nursing homes at earlier ages due to diabetes-related disability. The more equal ratios of men to women in earlier age groups points to possible change by gender among age groups in the composition of the nursing home population.
The discussion above suggests several possible impacts of increased prevalence of diabetes on the population of nursing home residents. The first is how much the demographic composition of the nursing home population has changed. The traditional model of nursing home residents as predominantly very old (85+) non-Hispanic White women may be outdated. The increased prevalence of diabetes has tended to have a greater impact on minorities than non-Hispanic Whites, suggesting the possibility that minorities have become a greater portion of the nursing home population due to diabetes-related disability. Another question is whether diabetes prevalence varies by gender among nursing home residents. The increasing prevalence of diabetes among working-age populations suggests that non-elderly diabetes-related disability may be contributing to increased admissions of working-age residents.
Data From the MDS
The MDS is a very detailed instrument that includes a vast array of data on individual nursing home residents including date of birth, gender, race or ethnicity, diagnosed medical conditions, indicators of physical functioning in terms of ADLs, indicators of cognitive functioning, and treatment procedures. The MDS has been revised and updated several times, but the same data form was used from 1999 to 2009, creating opportunities to compare the data for change over time (www.cms.gov, 2013). For the purpose of this research, the MDS for Texas was acquired for the years 1999 and 2009 to analyze changes related to the increased prevalence of diabetes. The MDS can include as many as six reports per year on an individual resident, so the uncorrected initial intake was selected for the purpose of having one record per resident. Many of the records were incomplete, so only those that included a full response regarding date of birth, race/ethnicity, gender, and diagnoses of diabetes were selected.
Patient age was calculated in relation to December 31 of the year for the MDS data, 1999 or 2009. This calculation was then used to sort residents into age groups of 17 or less, 18 to 34, 35 to 49, 50 to 64, 65 to 74, 75 to 84, and 85 and older. The categories for gender were male and female, and the diagnoses for diabetes were coded as Yes or No. Race and ethnicity are related but distinct concepts, but the MDS offers only one variable for this factor: Race/Ethnicity, variable AA4. The response categories offered for this variable are Native American/Alaskan Native, Asian/Pacific Islands, Black (not Hispanic), Hispanic, and White (not Hispanic). Native Americans, Asian/Pacific Islanders, and residents younger than 18 years were omitted from the analysis due to a very small number of cases. This left 79,144 cases from the 1999 data and 100,682 cases from 2009 that were suitable for analysis.
Change in Nursing Home Population Proportions
The existing literature suggests a number of ways in which the changing prevalence of diabetes may have affected the population of nursing homes. One is that some may be entering nursing homes at earlier ages due to diabetes-related disability, a possibility that can be explored by the data in Table 1.
Texas Nursing Home Residents Aged 18+, 1999 and 2009, Numerically and as a Percentage of Nursing Home Population.

Table 1 shows that for nursing home residents with records suitable for analysis, the proportion aged 50 to 64 years increased from less than 8% to almost 12% from 1999 to 2009. There were corresponding reductions in the 75 to 84 and 85+ age groups as a percentage of nursing home population. The disproportionate growth of residents aged 50 to 64 points to a possibility of changing proportions of men and women in nursing homes. The tendency of women to live longer than men contributes to female residents greatly outnumbering males at advanced ages, so an influx of middle-aged residents would be likely to increase the proportion of males in the nursing home population. Table 2 offers a breakdown of the Texas nursing home population by age and gender.
Texas Nursing Home Residents for 1999 and 2009 by Gender and Age.
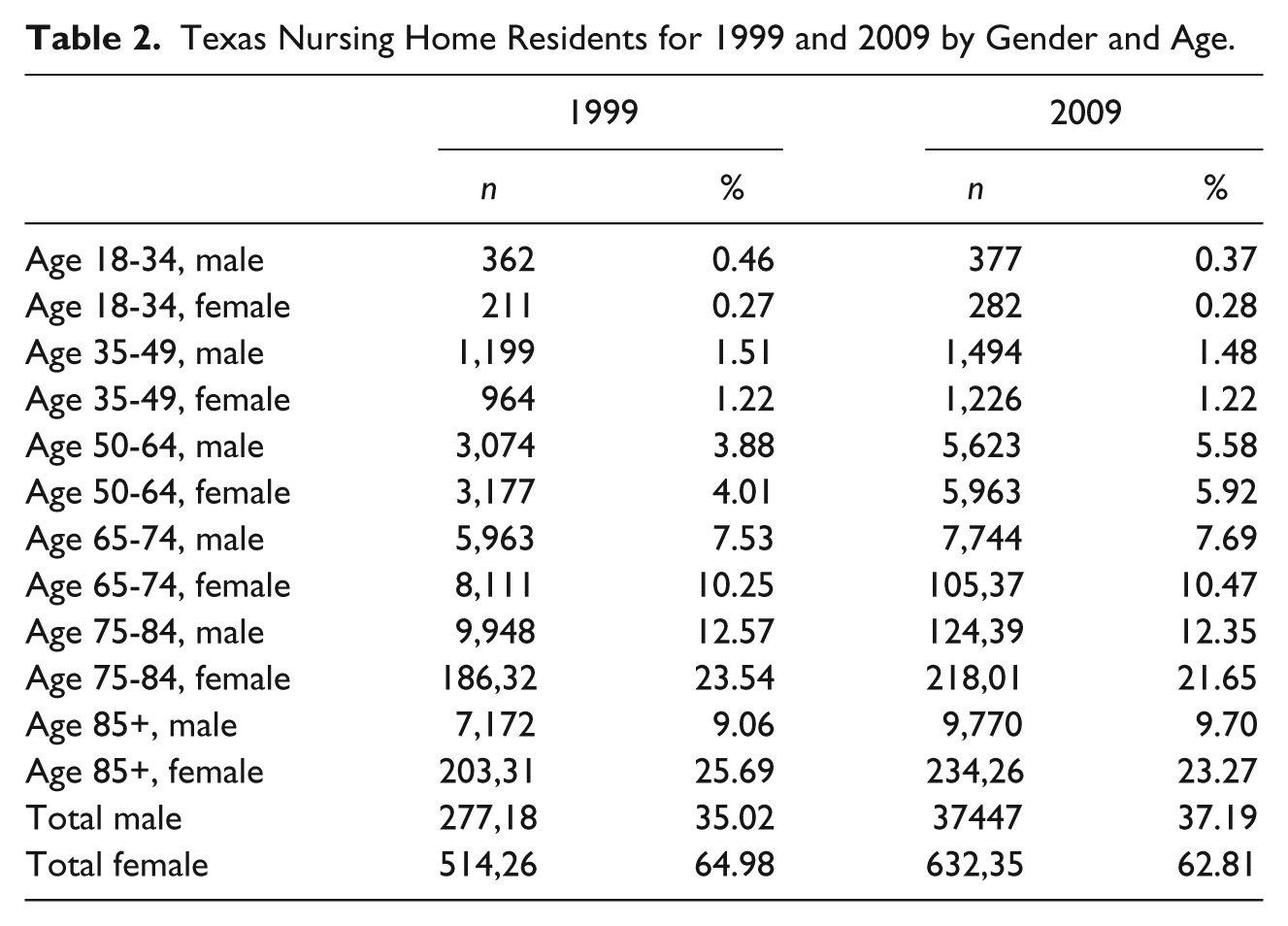
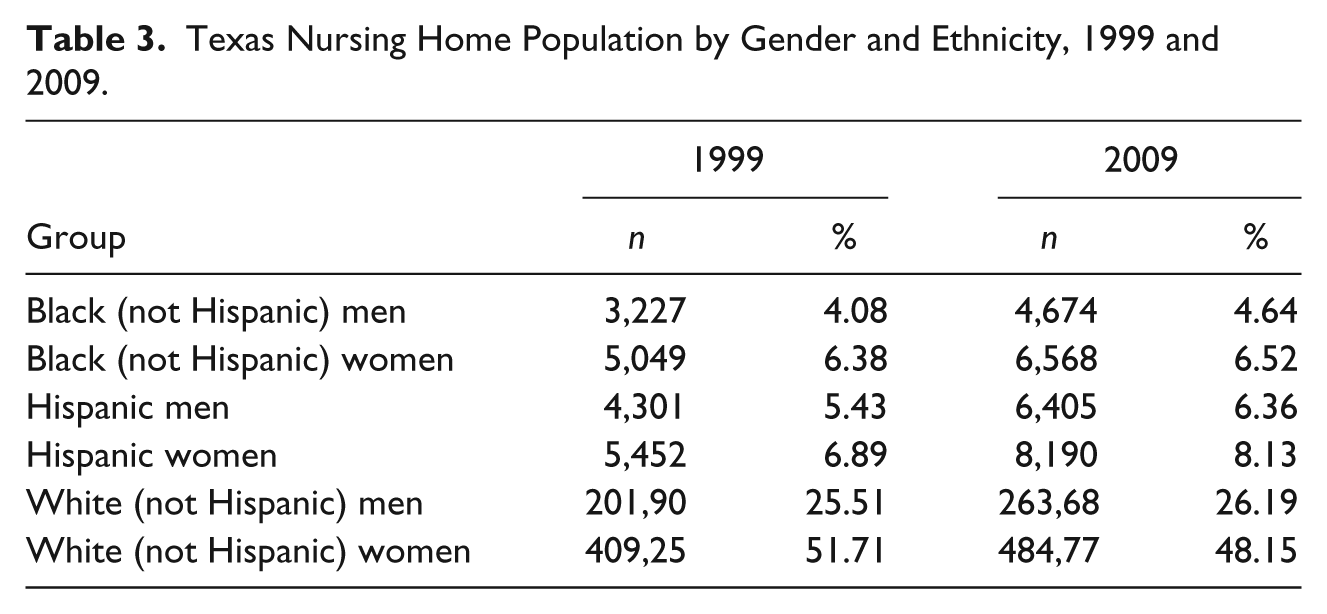
Particularly noticeable are the increases in men and women aged 50 to 64 and the declines in women aged 75 to 84 and 85+ as part of the nursing home population. The question remains of whether the composition of the nursing home population has changed by race or ethnicity. Table 3 indicates that non-Hispanic Blacks have remained stable as a portion of the nursing home population while the shares of Hispanics have increased and those of non-Hispanic White women have decreased.
Texas Nursing Home Population by Gender and Ethnicity, 1999 and 2009.
The raw figures indicate that the nursing home population has changed noticeably, raising the question of whether the extent of change is enough to merit serious consideration. This possibility was examined by comparing the makeup of the nursing home populations for 1999 and 2009 by the Two-Sample Proportion Test. The results are depicted in Tables 4, 5, and 6.
Non-Hispanic Black Nursing Home Residents, 1999 and 2009.
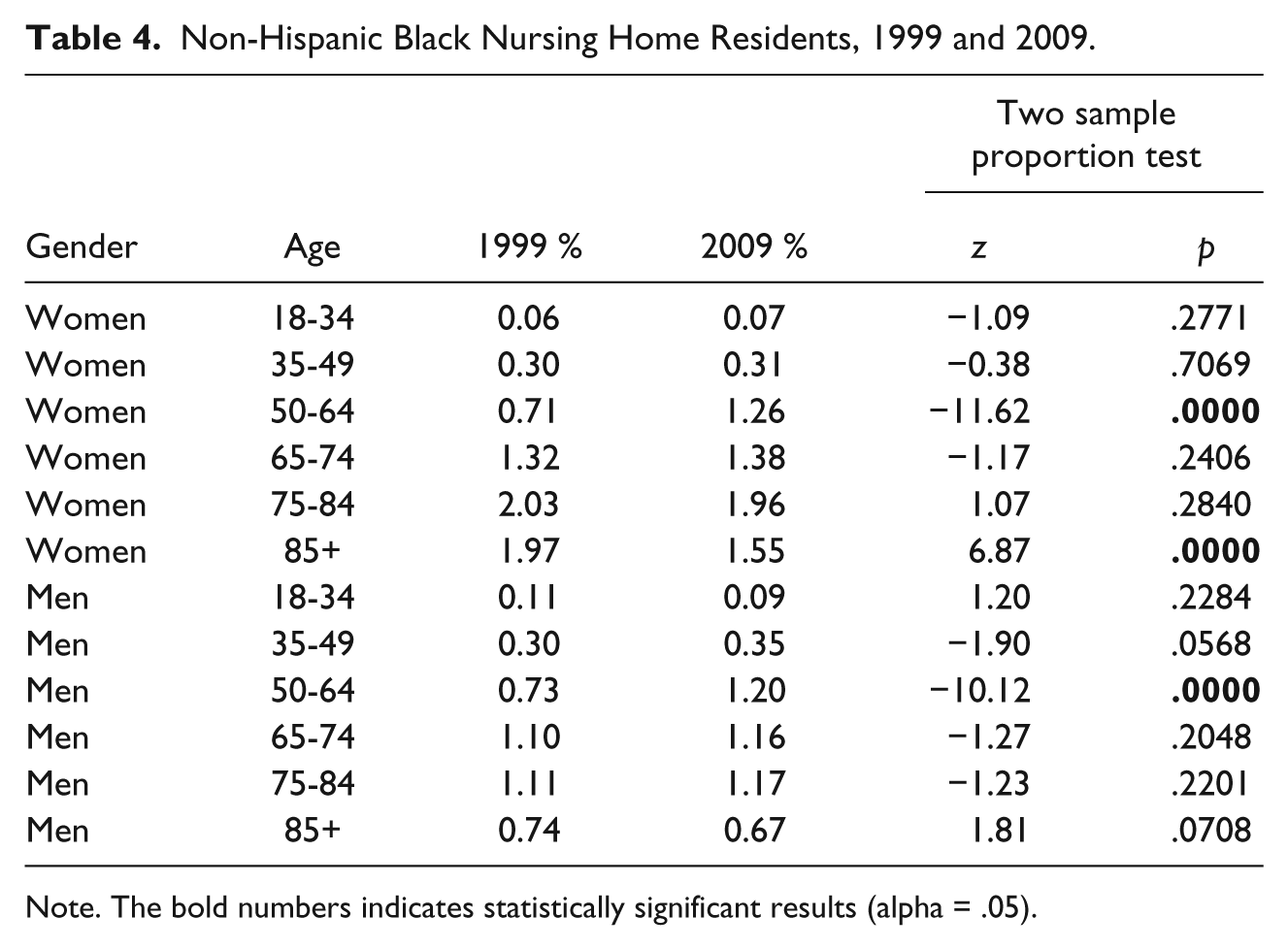
Note. The bold numbers indicates statistically significant results (alpha = .05).
Hispanic Nursing Home Residents, 1999 and 2009.
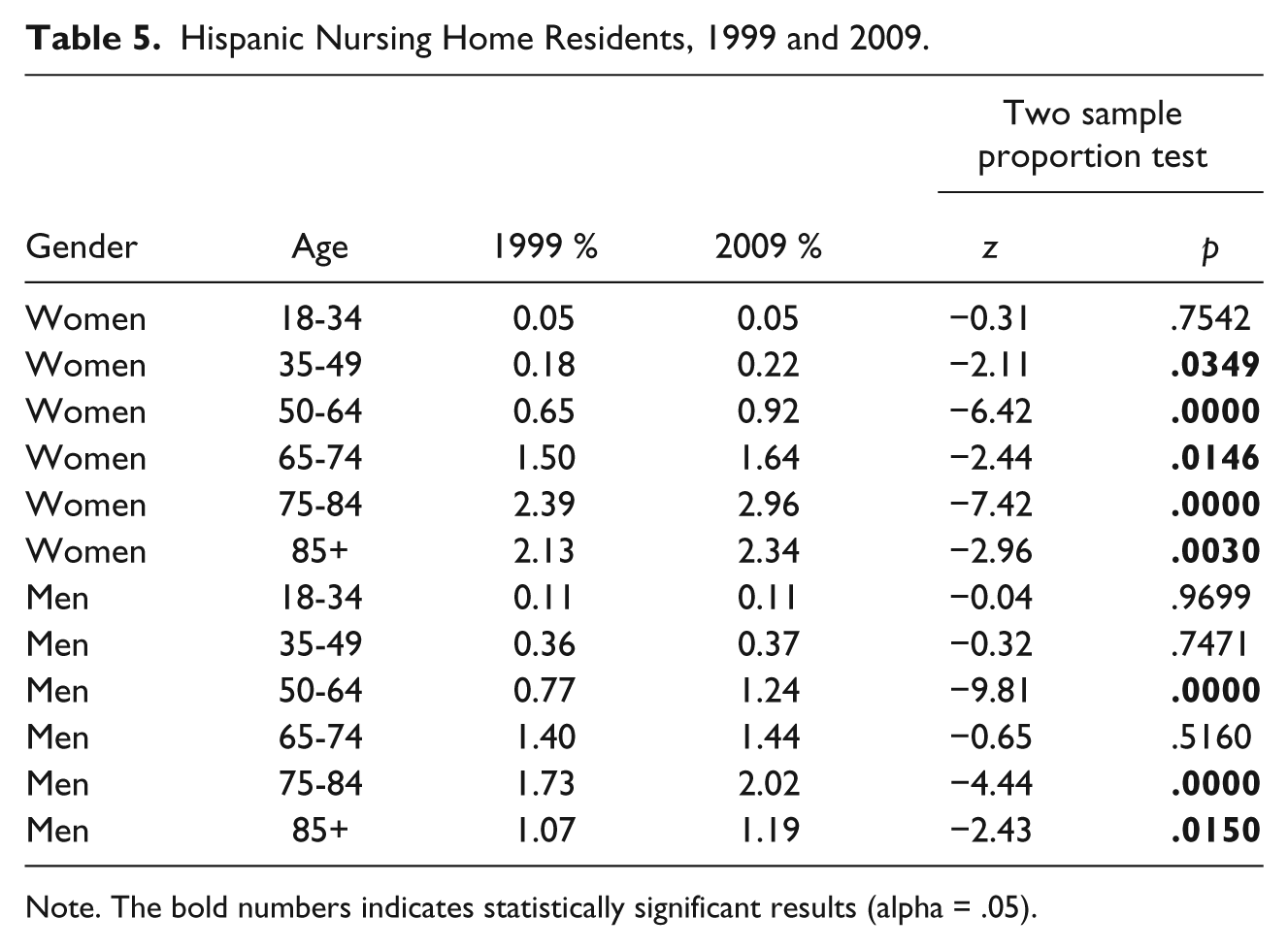
Note. The bold numbers indicates statistically significant results (alpha = .05).
Non-Hispanic White Nursing Home Residents, 1999 and 2009.
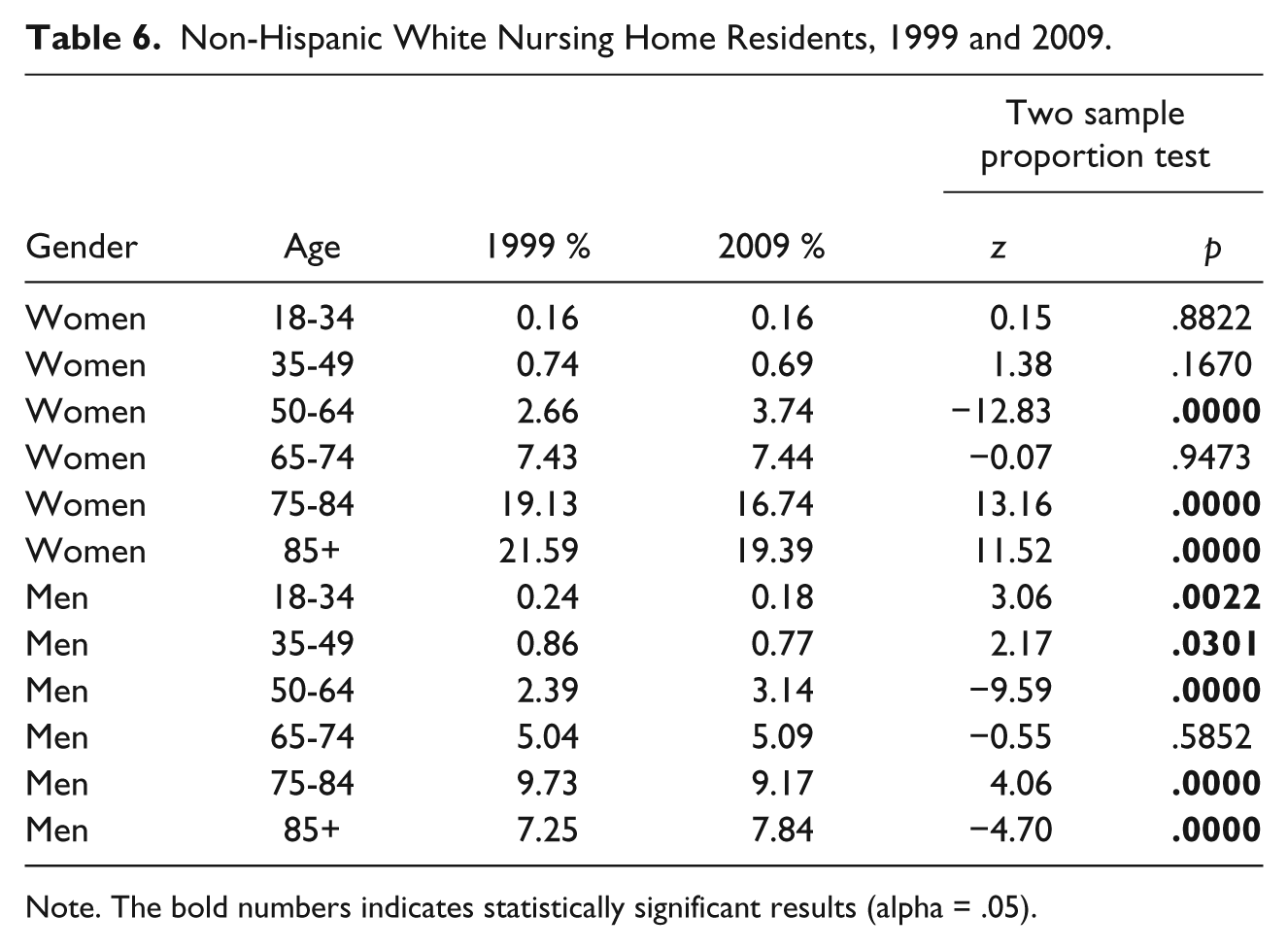
Note. The bold numbers indicates statistically significant results (alpha = .05).
Particularly noticeable is that those aged 50 to 64 showed a statistically significant increase for both genders and all race/ethnic groups. The stability of non-Hispanic Blacks as a portion of the nursing home population is highlighted in Table 4 as the change from 1999 to 2009 is not statistically significant for six of the nine age/gender groups tested. Other than those aged 50 to 64, the only statistically significant change was the decrease in non-Hispanic Black Women aged 85+. Table 5 shows that Hispanic women of all age groups except 18 to 34 increased as a portion of the nursing home population, and the change was statistically significant for all these groups. Hispanic men aged 50 to 64, 75 to 84, and 85+ also recorded statistically significant increases. A statistically significant increase was found for non-Hispanic White women aged 50 to 64 while the 75 to 84 and 85+ age groups reduced as a part of the nursing home population (Table 6). While the proportion of non-Hispanic White men decreased for those aged 18 to 34, 35 to 49, and 75 to 84, there were statistically significant increases for the shares aged 50 to 64 and 85+.
Change of Diabetes Prevalence Within Groups
The data regarding the change of various groups as a proportion of the nursing home population demonstrate that the nursing home population has changed and suggests that diabetes prevalence may have been a factor. This possibility was tested more directly by analyzing the change in the fraction with diagnosed diabetes among groups from 1999 to 2009, and the results are depicted in Tables 7, 8, and 9. Particularly noticeable is that nearly all groups showed statistically significant increases from 1999 to 2009. The only exceptions were Hispanic women aged 18 to 34 and non-Hispanic White men aged 18 to 34, the latter being the only group to actually show a decrease in the percentage reporting diabetes. Particularly noticeable is that the prevalence of diabetes for Hispanics of both genders and all age groups was consistently higher than the figures for non-Hispanic Blacks or non-Hispanic Whites of the same category for 1999 and 2009.
Non-Hispanic Blacks.
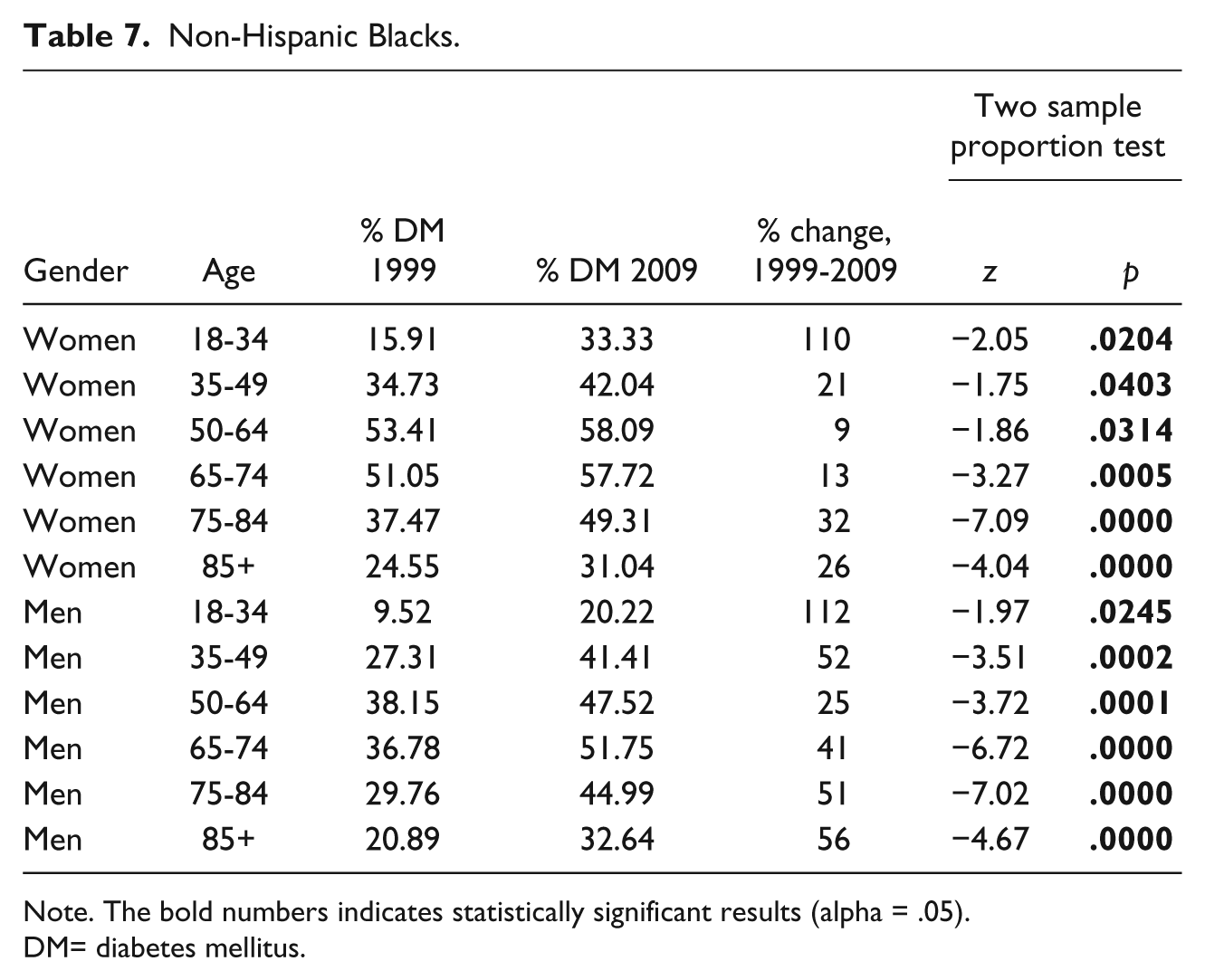
Note. The bold numbers indicates statistically significant results (alpha = .05).
DM= diabetes mellitus.
Hispanics.
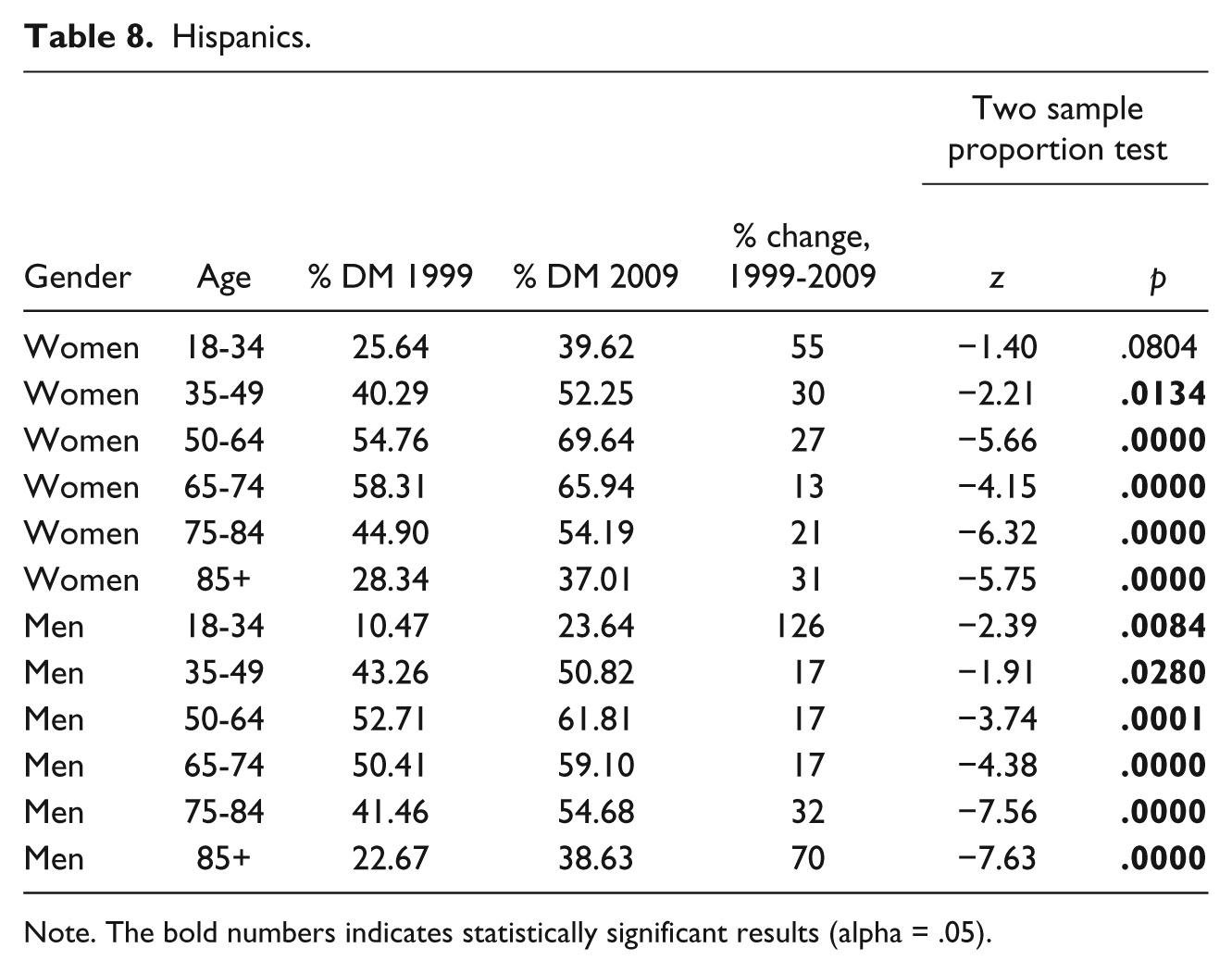
Note. The bold numbers indicates statistically significant results (alpha = .05).
Non-Hispanic Whites.
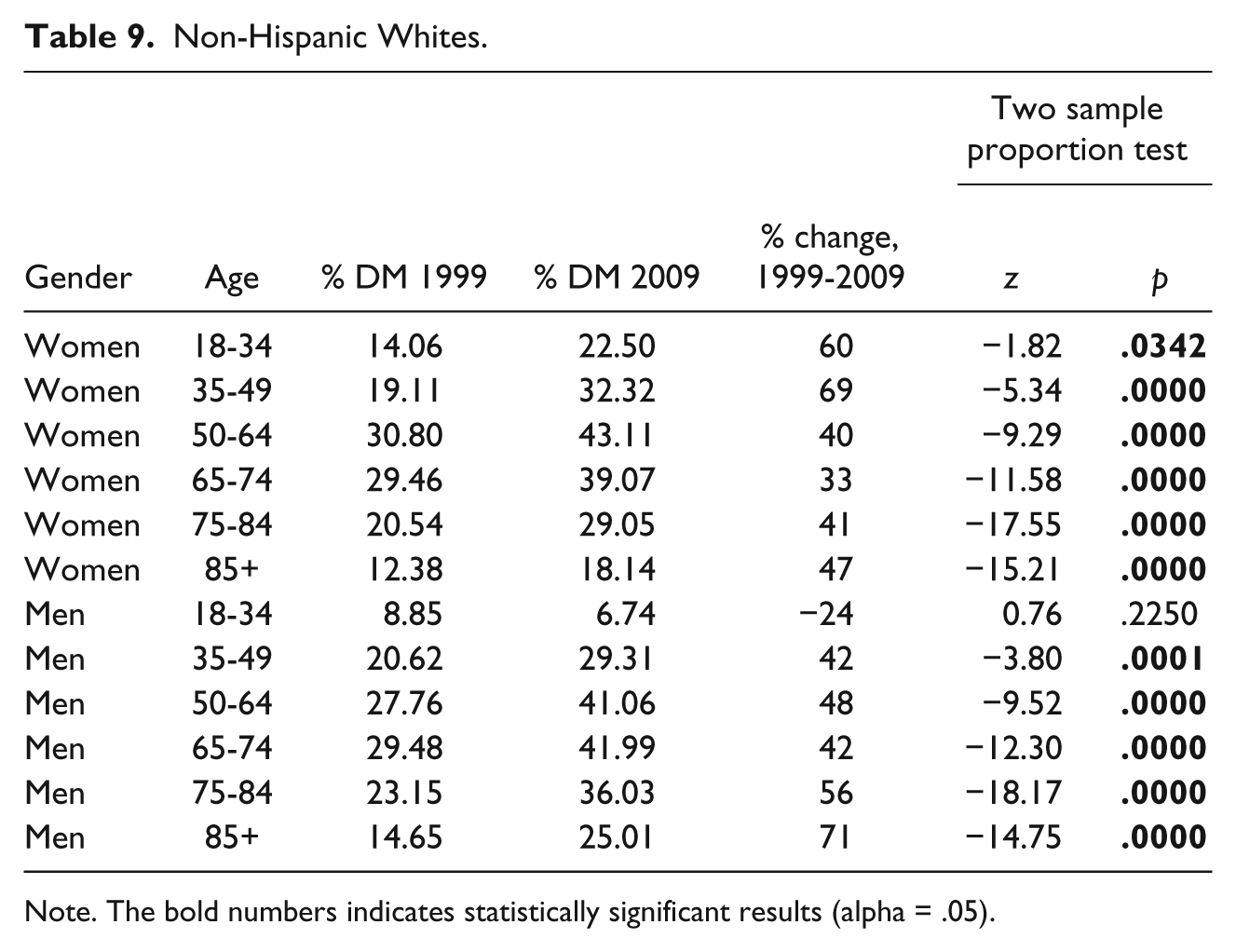
Note. The bold numbers indicates statistically significant results (alpha = .05).
Some interesting matters also appear among the groups aged 18 to 34. One is that the while the diabetes prevalence for non-Hispanic Black males in 1999 (9.52%) was comparable with non-Hispanic White males (8.5%), the figure for non-Hispanic Black residents more than doubled to 20.22% while that for non-Hispanic Whites reduced to 6.74% for 2009. The prevalence for Hispanic males aged 18 to 34 also more than doubled from 10.47% to 23.64%. Similarly, the figure for non-Hispanic Black women (15.91%) is comparable with that of non-Hispanic White women (14.06%) in 1999, but the two diverge in 2009 as non-Hispanic Black women double to 33.33% while non-Hispanic White women show a more modest increase up to 22.50%. Hispanic women show the highest prevalence for this age group in 1999 (25.64%) and 2009 (39.62%). The 50 to 64 age group shows the highest diabetes prevalence for non-Hispanic Blacks and Hispanics of both genders and non-Hispanic White women for 1999 and 2009, while the highest diabetes prevalence for non-Hispanic White men is found in the 65 to 74 age group.
Overall, the data from the Texas MDS appear consistent with the general patterns indicated in previous research for the larger society. Diabetes prevalence increased for nearly all age groups and both genders. All three categories for race/ethnicity showed increases in diabetes prevalence, but the increases were more pronounced in minorities than in non-Hispanic Whites. The noticeable increase in the 50 to 64 age group as a portion of the nursing home population, along with their dramatic increases in diabetes prevalence, points to possible variation by gender as this age group largely accounted for the increase in men as a proportion of the nursing home population. Previous literature has observed that non-Hispanic Whites tend to have a lower prevalence of diabetes than minorities in the general population and nursing homes (Resnick et al., 2008), but the question remains of whether there is a difference by gender within age groups.
The possibility that the risk of diabetes varies within age groups by gender was examined by the Cochran–Mantel–Haenszel test, a technique that allows for comparison of two binary nominal variables (gender and diabetes diagnosis) while controlling for a third variable (Race/Ethnicity) that does not have to be dichotomous (Conover, 1999). The Cochran–Mantel–Haenszel test was run for each age group comparing the proportion of nursing home residents diagnosed with diabetes by gender while controlling for race/ethnicity for 1999 and 2009. Table 10 presents the comparative risk of diabetes for male and female nursing home residents for 1999 while Table 11 shows the results for 2009.
Diabetes Risk, Men Versus Women by Age Group Controlling for Ethnicity, 1999.
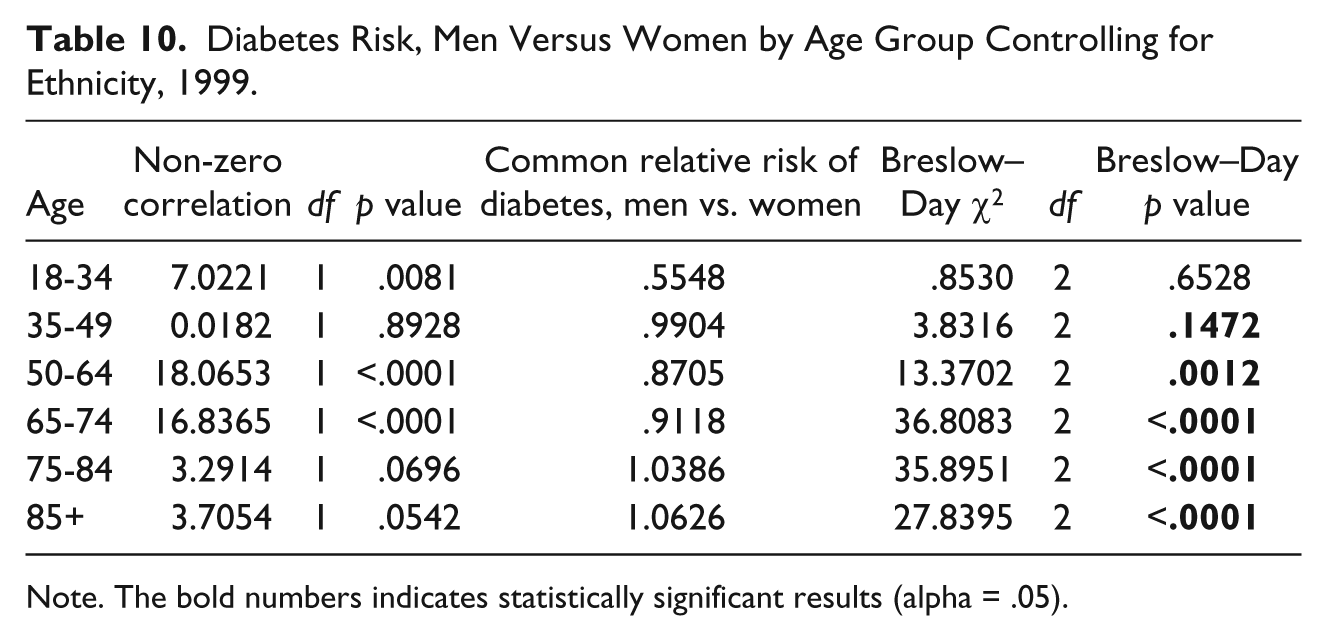
Note. The bold numbers indicates statistically significant results (alpha = .05).
Diabetes Risk, Men Versus Women by Age Group Controlling for Ethnicity, 2009.
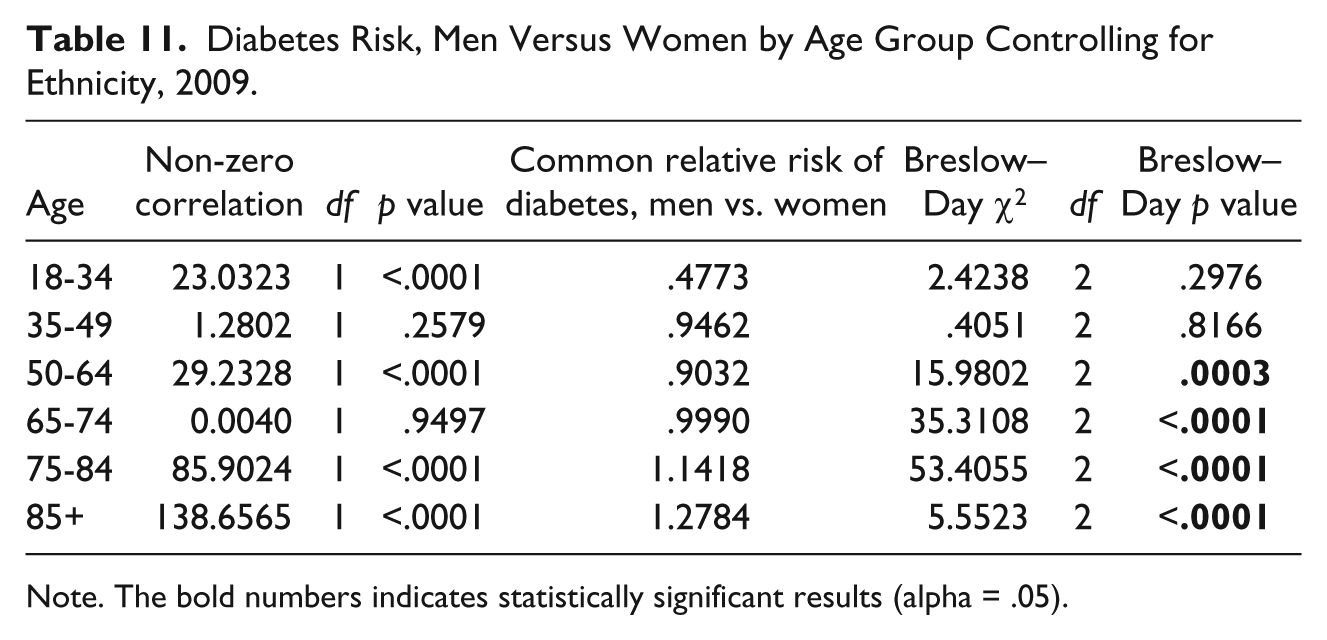
Note. The bold numbers indicates statistically significant results (alpha = .05).
The results show variation by gender as well as change between 1999 and 2009 when observing various age groups. Nursing home residents aged 18 to 34 showed a statistically significant difference between men and women, with males at a noticeably lower risk for diabetes for both years. For nursing home residents aged 35 to 49, the differences between men and women were not statistically significant and the relative risk of diagnosed diabetes was relatively equal for 1999 and 2009. The 50 to 64 age group showed a statistically significant difference with a higher risk for women for both years, although the gap did narrow over the time span. The 65 to 74 age group also showed change as the differences between men and women were statistically significant for 1999 but not for 2009, as men went from lower comparative risk for the former year to equal risk for the latter. An interesting change occurred for the 75 to 84 and 85+ age groups as the difference was not statistically significant for 1999, but the greater risk for men was statistically significant for 2009.
Discussion
The limitations of the MDS make it difficult to draw conclusions regarding the impacts of changing diabetes prevalence on the Texas nursing home population. It should also be pointed out that fewer than half the cases of nursing home residents included records sufficiently complete to include in the analysis for 1999 and 2009. It was not possible to include Native Americans, Asians, and those below 18 years old because their small numbers risked compromising the privacy of individuals. An expanded study covering a larger region or the entire United States would provide for inclusion of these groups. It should also be pointed out that the data were summarized for the entire State of Texas, and this may have masked regional variations as well as the interaction of income with ethnicity for the risk of nursing home admission. These are matters that are worthy of further examination.
These limitations notwithstanding, there are some matters that appear worthy of notice. One is that the changes observed in the nursing home population for the most part mirrored those of the larger society. The prevalence of diabetes increased for all groups, and minorities tended to report greater increases than non-Hispanic Whites. The noticeably higher prevalence of diabetes among Hispanics of all ages is a matter of concern for Texas policymakers. The very high rates of obesity among Hispanics in particular regions such as the Rio Grande Valley may point to an increased risk of nursing home admission in this region (Fisher-Hoch et al., 2010).
Another important observation is that the noticeable increase in the proportion of nursing home residents aged 50 to 64, along with the high diabetes prevalence for this age bracket, is consistent with an expectation that the increased diabetes prevalence may contribute to a population of non-elderly entering nursing homes with disabilities related to this condition. Further inquiry is recommended regarding the causal factors for an influx of middle-aged adults into nursing homes and how this affects the operation of long-term care facilities. In particular, the relationship between obesity and the admission of middle-aged residents to nursing homes is worthy of further inquiry. Lapane and Resnik (2005) noted that fewer than 15% of nursing home residents were obese in 1992, but this rose to 25% by 2002. If a large part of the middle-aged diabetic residents are obese, this may require acquisition of special equipment such as Hoyer lifts plus specialized training for nurses and nursing assistants in providing care for this population (Lapane & Resnik, 2006). Bennet (2008) pointed out that the treatment and quality of life issues for bariatric nursing home residents require specialized equipment, psychosocial resources, dietary counseling, and physical and occupational therapy resources that have not been required in the past by nursing home residents. Bariatric residents may also be considerably younger than the traditional nursing home population and may expect amenities such as access to the Internet and cell phones. The development of statistically significant difference in the prevalence of diabetes for males aged 75 and older in 2009 compared with women when such difference was not present in 1999 also calls for further examination.
Overall, this research indicates that the nursing home population is being affected by the change in diabetes prevalence in the general population and suggests that the increased prevalence of obesity is a major contributing factor. The impacts of these trends merit closer examination to prepare appropriate care for this population and to accurately project costs for long-term care policy.
Footnotes
Acknowledgements
The authors wish to express thanks and appreciation to those who provided needed assistance and advice that made the completion of this research possible: Daniel Heimmermann, PhD, Provost and Vice President of Academic Affairs, Mississippi University for Women; Dr Luis V. Colom, UTB Vice President for Research; Christopher Cohen, UTB Information Security Officer ; Bebe Crooks, UTB Special Assistant to the VPR, Research Integrity & Compliance (retired); Clair Goldsmith, PhD, UTB Vice President for Information Technology and Chief Information Officer; Dirce E. Hernandez, UTB Security Analyst; Paul Kavanaugh, PhD, Manager, Department of Institutional Grant Writers, Division of Research, UTB; Gregory Petroski, PhD, Research Assistant Professor and Statistician for Office of Medical Research, University of Missouri; Belinda M. Reininger, DrPH, University of Texas School of Public Health, Brownsville Regional Campus; Dr Anne Rentfro, UTB Professor of Nursing; Pablo Sanchez, Data Management Analyst, University of Texas School of Public Health, Brownsville Regional Campus.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.