
Abstract
The Zarit Burden Interview (ZBI) is commonly used to measure dementia caregiver burden, but its factor structure is unclear. A two-factor structure for the 12-item ZBI, “personal strain” and “role strain,” has been shown, but recent data suggest that an additional factor of “guilt” is embedded in the “role strain” items. The 12-item ZBI administered to 194 informal rural and urban caregivers of persons diagnosed with dementia was analyzed using exploratory factor analysis. A two-factor structure, with item loadings consistent with previously conceptualized constructs of “personal strain” and “role strain,” was found. Moreover, this factor structure was invariant to caregiver subgroups. When the predictive value of these factors was explored, only “personal strain” was important in predicting caregiver psychological distress, measured with the Brief Symptom Inventory. However, “role strain,” which included the hypothesized “guilt” items, did not appear to be an important predictor of caregiver distress.
Canada, like other industrialized nations, will observe an unprecedented increase in its aging population. In 2011, the first of the baby boomer generation entered senior age (65+), and the aging of this demographically sizable generation is expected to increase strain on limited health care services (Smetanin et al., 2010). Advanced age increases the risk of dementia, and as Canada’s population ages, the incidence of dementia in Canada is projected to increase 250% between 2008 and 2038 (Smetanin et al., 2010). As a consequence, informal caregiving, which is unpaid care provided by a close friend or a family member (hereafter referred to as caregiving), is expected to increase exponentially in the next 30 years. Although select data suggest caregiving is associated with some positive and beneficial aspects (Beach, Schulz, Yee, & Jackson, 2000; Cohen, Colantonio, & Vernich, 2002), the vast majority of the data suggest caregiving is associated with negative consequences for physical, emotional, mental, and social health (e.g., Biegel & Schulz, 1999; Brodaty, 2007; Coon, Thompson, Steffen, Sorocco, & Gallegher-Thompson, 2003; George & Gwyther, 1986; Pinquart & Sorensen, 2003). Caregiver’s self-perceived burden is hypothesized to emerge from the belief that one lacks the ability to contend with the role demands associated with caregiving (George & Gwyther, 1986; O’Rourke & Tuokko, 2000), and higher levels of burden are hypothesized to be causally related to negative physical and psychological outcomes for caregivers (O’Rourke & Tuokko, 2000). Caregiver burden is particularly exacerbated when caring for persons with dementia (Pinquart & Sorensen, 2003), in part, because of the additional challenges associated with specific behaviors, functional and cognitive impairments, but also because the progressive nature of dementia demands an ever-increasing level of care (Vitaliano, Young, & Russo, 1991).
The purpose of the current study is to detail the measurement of dementia caregiver burden, which may be an important factor in caregivers’ health outcomes. While there exist a number of burden measures (e.g., Caregiver Strain Index, Caregiver Appraisal Measure, and Caregiver Hassles Scales; Vitaliano et al., 1991), not all measures are appropriate for every caregiver. Some measures are found valid for caregivers of persons emerging from acute hospital care (e.g., post-hip replacement or heart attack), while others are more appropriate for assessing burden in caregivers of persons with dementia (Vitaliano et al., 1991). The Zarit Burden Interview (ZBI) is a self-report measure that quantifies burden experienced by caregivers of persons with dementia. The original ZBI is composed of 22 items, 21 of which are based on a 5-point Likert-type scale. Abridged forms such as the 12-item ZBI, engendered by Bedard and colleagues (2001), have been created to provide brief and accurate assessment of caregiver burden (Bedard et al., 2001). Despite its popularity as an assessment tool, the ZBI’s factor structure remains unclear.
The 12-item ZBI administered to caregivers of persons with dementia revealed a two-factor structure comprising “personal strain” and “role strain” (O’Rourke & Tuokko, 2003). Similarly, the longer 22-item ZBI revealed the same two factors in a sample of caregivers of persons with acquired brain injury (Siegert, Jackson, Tennant, & Turner-Stokes, 2010). In contrast, other data support a three-factor structure for longer and shorter versions of the ZBI administered to dementia caregivers. For example, three factors were found for the 22-item ZBI in caregivers of persons with dementia due to Alzheimer’s disease (AD) or other pathologies, which were labeled “social consequences,” “psychological burden,” and “guilt” (Ankri, Andrieu, Beaufills, Grand, & Henrard, 2005). Similarly, a three-factor structure was found for the 22-item ZBI administered to family caregivers of persons with dementia, but these factors were labeled “embarrassment/anger” (consistent with “personal strain” factor loadings), “patient dependency” (consistent with “role strain” factor loadings), and “self-criticism” (consistent with “guilt” factor loadings; Knight, Fox, & Chou, 2000). More recently, a three-factor structure was supported in the 14-item ZBI administered to White and Black caregivers of persons with dementia (Flynn Longmire & Knight, 2011). The three factors, “embarrassment/anger,” “patient dependency,” and “self-criticism,” were identified through confirmatory factor analysis (CFA), and this factor structure was found to be invariant across the two racial groups. These few studies appear consistent in the factor loadings, but appear to only differ in the descriptions of these factors. The same ZBI items that loaded high on the factor labeled “self-criticism” (Flynn Longmire & Knight, 2011; Knight et al., 2000) were those that loaded on the factor labeled “guilt” by Ankri and colleagues (2005). Table 1 includes a summary of the previous research and findings from factor analyses.
Summary of Factor Analysis Studies of the Zarit Burden Interview.
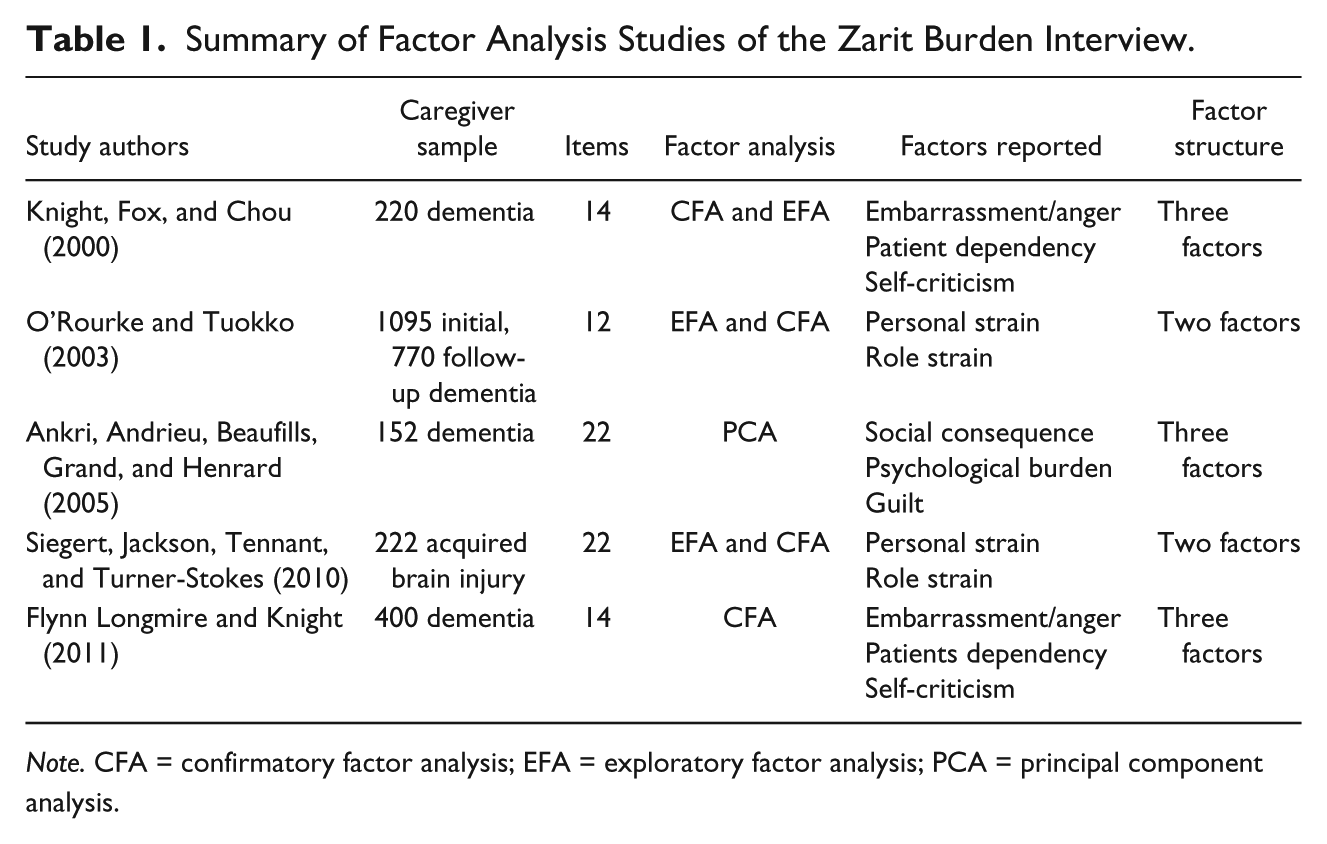
Note. CFA = confirmatory factor analysis; EFA = exploratory factor analysis; PCA = principal component analysis.
Data suggesting that the ZBI may measure guilt are important and are consistent with the research that suggests guilt is the primary emotion for caregivers, intensifying the experience of burden (Brodaty, 2007). Others suggest guilt may serve as a source of psychological and emotional strain, acting as a harbinger for depression and distress (Ghatavi, Nicolson, MacDonald, Osher, & Levitt, 2002). Similarly, experience of shame in dementia caregivers has been found to relate to depression (Martin, Gilbert, McEwan, & Irons, 2006). Because feelings of shame and guilt are believed to arise if an individual feels he or she has failed to fulfill some obligation (Andershed & Werkander Harstade, 2007), it is reasonable to assume that a caregiver’s experience of these emotions may be more frequent or unique, relative to non-caregivers.
The concepts of shame and guilt both reflect negative feelings associated with “not being sufficient” (Werkander Harstade, Roxberg, Andershed, & Brunt, 2012); however, evidence supports a distinction between shame and guilt (e.g., Blavier & Glenn, 1995; Martin et al., 2006; Werkander Harstade et al., 2012). Shame is believed to be self-focused, affecting one’s own sense of self and identity (Andershed & Werkander Harstade, 2007). Connected to emotions such as dishonor and disgrace, shame is believed to play an integral role in forming one’s moral standing and moral behavior (Andershed & Werkander Harstade, 2007; Werkander Harstade et al., 2012). Conversely, guilt is conceptualized as pertaining to one’s behavior and actions; thus, guilt has an external focus and is associated with a perceived breach of current rules, norms, and moral obligations (Andershed & Werkander Harstade, 2007). Feelings of guilt are aimed at what has been done and move the individual to compensate for, or diminish the effect of, a perceived wrong or inadequate action on the person associated with the “guilt action” (Werkander Harstade et al., 2012).
The concept of “guilt” is preferred in the current study, as the ZBI items that potentially reflect guilt pertain to action rather than internal conflict (i.e., “feel I am not doing enough,” “feel I could be doing a better job”). In line with the conceptualization of guilt, past research supports the notion of guilt arising out of a perceived inadequacy to fulfill the caregiver’s role. For example, elevated behavioral problems in the care recipient increase role demands on the caregiver, and behavioral problems have been found to positively correlate with caregiver guilt (Ankri et al., 2005). In addition, relative to spousal caregivers, feelings of guilt are found to be high in adult child caregivers, it is suspected this is due to the younger caregiver having multiple roles to fulfill (e.g., caregiver, spouse, parent, and career roles) leading to a perceived inability to adequately meet all role demands (Ankri et al., 2005; Gonyea, Paris, & de Saxe Zerben, 2008). Although such findings suggest guilt plays an important role in the caregiving experience, it remains that “guilt” may not always be captured by the commonly used measure of caregiver burden, such as the 12-item ZBI.
Some studies have found support for the ZBI measuring a third latent construct of guilt (Ankri et al., 2005; Flynn Longmire & Knight, 2011; Knight et al., 2000), whereas others have only found two latent factors measured by the ZBI (O’Rourke & Tuokko, 2003; Siegert et al., 2010). The conflicting results from factor analyses may be due to the use of various versions of the ZBI and differences in sample characteristics (Siegert et al., 2010) as opposed to variations in the latent structure of the ZBI. Although O’Rourke and Tuokko (2003) found a two-factor structure of the 12-item ZBI, the specific items that have been found to identify a third factor of “guilt” in longer versions are common to this abridged version. Thus, given the potential of guilt in exacerbating the experience of burden, and the inconsistent results of the existing literature, it is reasonable to re-evaluate the factor structure of the 12-item ZBI in the context of the more recent data on guilt in a shortened ZBI version (Flynn Longmire & Knight, 2011). It is possible that items within the 12-item version reflect the construct of caregiver guilt.
The purpose of the current study was to identify the factor structure of the 12-item ZBI in a sample of 197 predominantly rural caregivers of persons with dementia. Moreover, we sought to explore whether the measurement of guilt was similar for two groups of caregivers—adult children versus spouses—as some data suggest adult children caregivers are more likely to experience feelings of guilt (Ankri et al., 2005; Gonyea et al., 2008). Rural caregivers have access to fewer resources (Morgan, Semchuk, Stewart, & D’Arcy, 2002; Sullivan, Weinert, & Fulton, 1993) and are vastly understudied (Goins, Spencer, & Byrd, 2009). Data are contradictory on whether rural and urban caregivers differ in burden, with some suggesting rural caregivers of persons with dementia report higher burden than urban caregivers (Bien, Wojszel, & Sikorska-Simmons, 2007), and others suggesting a small or trivial association between burden and rurality (Byrd, Spencer, & Goins, 2011; O’Connell, Germaine, Burton, Stewart, & Morgan, 2013). Although we have no a priori hypotheses for how rurality might impact measurement of burden on the ZBI, patients’ geographic location could impact the experience of caregiving due to less access to specialty services for rural patients, which could impact caregivers’ experience of guilt. We, therefore, sought to explore whether the measurement of burden was similar for caregivers based on the degree of patients’ rurality.
Based on previous research, we hypothesized that we would find a three-factor structure in the ZBI, which would include measurement of guilt. Moreover, we were able to explore factorial invariance to variables such as relationship to patient with dementia and degree of rurality, factors that might be important for guilt or for burden. Finally, we tested whether the resulting factors predicted caregiver’s report of psychological distress or quality of life.
Method
Participants
This study analyzed archival data from 197 caregivers of persons diagnosed with dementia after an interdisciplinary assessment at the Rural and Remote Memory Clinic (RRMC) in Saskatoon, Saskatchewan. The patient population of the RRMC includes persons living in rural areas (defined as 100 km outside the two main urban centers of the province) who have been referred to the clinic for memory or other cognitive or behavioral concerns (Morgan et al., 2009). The assessment procedures are interdisciplinary, and the family participates in an interview conducted together by the neurologist, (neuro)psychologist, and physical therapist (clinic described in Morgan et al., 2009). Potential diagnoses are discussed by the interdisciplinary team, and made according to up-to-date diagnostic guidelines (detailed assessment procedures described in Morgan et al., 2009). Severity of difficulties in function and cognition are rated in the six domains of the Clinical Dementia Rating scale (CDR; Hughes, Berg, Danzinger, Coben, & Martin, 1982) by the psychologist. In addition to the patient’s psychological assessment, the caregivers complete the ZBI, a measure of psychological distress (Brief Symptom Inventory [BSI]) and quality of life (Short-Form Health Status Survey [SF-12], each discussed in the “Measures” section).
Measures
The 12-item ZBI has been discussed in detail regarding its hypothesized factor structure. There is evidence to suggest that the reliability of the ZBI is strong, with high internal consistency (Bachner & O’Rourke, 2007; Vitaliano et al., 1991). The ZBI has been found to have sufficient evidence for construct validity and criterion-related validity (Vitaliano et al., 1991). The ZBI has also been found to be a good predictor of depression (Schreiner, Morimoto, Arai, & Zarit, 2006) and has been found to correlate highly with measures from the BSI (Vitaliano et al., 1991).
The BSI is a self-report symptom scale of psychological state (Derogatis & Melisaratos, 1983). It is believed to address elements of psychological strain such as, depression, anxiety, and personal feelings of self-worth (Derogatis & Melisaratos, 1983). This measure has been found to have adequate evidence for reliability, showing high internal consistency, and has strong evidence for both criterion-related validity and construct-related validity (as compared with Symptom Check List 90–Revised and Minnesota Multiphasic Personality Inventory, respectively; Derogatis & Melisaratos, 1983). The 53-item BSI was used in this study and scores range from 0 to 212 with higher scores suggesting greater distress.
The SF-12 is a health-related quality-of-life instrument, which incorporates two measures: a Physical Component Summary (PCS) and a Mental Component Summary (MCS; Amir, Lewin-Epstein, Becker, & Buskila, 2002). It comprises 12 items: 6 related to physical health (e.g., bodily pain, general health, physical functioning, etc.) and 6 items pertaining to mental health (e.g., social functioning, vitality, mental health, etc.; Amir et al., 2002). The SF-12 is reliable, with good evidence for criterion-related validity in a sample of persons with severe mental illness (Salyers, Bosworth, Swanson, Lamb-Pagone, & Osher, 2000) and concurrent validity with World Health Organization Quality of Life (WHOQoL) measure, Center for Epidemiological Studies–Depression Scale, Quality of Life Depression Scale, the 90-item Hopkins Symptom Scale, and WHOQoL (Amir et al., 2002). The SF-12 was used as a measure of quality of life for this sample of caregivers of persons with dementia, and higher scores suggest better quality of life.
The Clinical Dementia Rating Scale Sum of Boxes (CDR-SOB) is a variant form of the original CDR. The CDR-SOB adds up the ratings of impairment (each from 0, no impairment, to 3, profound impairment) in the domains of memory, orientation, judgment and problem solving, community affairs, home and hobbies, and personal care (O’Bryant et al., 2008). The CDR, however, uses information from these box scores, but its scoring rules emphasize the role of memory, which is very specific to AD. Due to the equal weighting of all six domains in the CDR-SOB, we argue it is more consistent with staging severity of dementia due to pathologies other than AD. Likely due, in part, to the expanded range in possible scores (0-18), the CDR-SOB has been found to be a sensitive measure, accurately staging a range of dementia severities and discriminates early stages of AD from mild cognitive impairment (O’Bryant et al., 2008).
Metropolitan influenced zone (MIZ) is a standardized measure from Statistics Canada categorizing workforce commutes from a place of residence to an urban center, defined as a population of 10,000 or more. Despite being characterized as urban, the cities of patients included in the sample are relatively small, with population sizes of 43,000; 33,000; 15,500; 15,000; and 14,000. It is notable that “urban” defined with the MIZ overlaps with what was considered rural in other studies (e.g., Bedard, Koivuranta, & Stuckey, 2004). The MIZ has an advantage over merely categorizing degree of rurality based on population size alone; rather, the MIZ measures the influence of an urban center on the surrounding region. MIZ is rated from no urban influence considered rural/remote with no access to an urban center to urban. In a moderate to strong MIZ place of residence, 5% to 49% of the workforce would commute for work to an urban center. In contrast, a place of residence coded as weak to no MIZ, less than 5% of the workforce would commute to an urban center for work. MIZ groups included no MIZ, weak MIZ, moderate MIZ, strong MIZ, or urban. For these analyses, MIZ was grouped as rural (no or weak MIZ) versus moderate-urban (moderate, strong, and urban).
Statistical Procedure
SPSS was used for all analyses. For descriptive statistics of group-based differences in ZBI scores, a factorial ANOVA, independent samples t test, and correlations were used where appropriate. Exploratory factor analysis (EFA) using oblique rotation was performed to identify the factor structure of the 12-item ZBI in a sample of caregivers of persons with dementia. Oblique rotation was chosen because of the interrelation between factors. SPSS Amos was used to explore factorial invariance for subgroups of caregivers. This method of multiple-group CFA is a form of structural equation modeling. Factorial invariance tests the original model with models that increasingly constrain variables to be equal for spouses and adult children. Model fit improvement is explored by constraining each progressive variable, first factor loadings (regression weights), then intercepts for each item, residuals, factors, and then covariance between the two factors, reveals whether the original model is substantially improved by forcing equivalence for the two groups. If the original model is improved by forcing equivalence, this suggests that the original model does not capture differential latent structures for the subgroups being compared.
Finally, multiple regression was used to determine whether the resulting ZBI factors were associated with differential predictors. Stepwise multiple regression (i.e., where all predictors are entered simultaneously, order is not important; rather, predictors that account for most variance are retained) was chosen as the method as the primary purpose was data driven prediction as opposed to theoretical modeling (Keith, 2006). Predictors entered simultaneously were CDR-SOB, BSI, and the SF-12 measures of PCS, physical, and MCS, mental health quality of life (no multicollinearity evident).
Results
Description of Sample
Of the initial sample of 197, 3 were missing ZBI scores, and so the sample for all analyses was 194. The mean age of the current caregiver sample was 61.93 (SD = 14.81; note that age was missing from six cases). The vast majority of the sample was of European ancestry, and there appeared to be a bimodal distribution in the degree of rurality of the patient’s home measured with the MIZ. Consistent with the previous research, the sample was predominantly female, comprised 58 male (29.9%) and 132 female caregivers (68.8%; gender was missing for four cases). As can be seen in Table 2, 103 (54.5%) caregivers were spouses of the care recipient, 78 were adult children of the recipient (41.3%), and 8 (4.2%) were classified as other (i.e., sibling, extended family of recipient, neighbor, friend, etc.; 5 cases had missing data for relationship). As can be seen in Table 3, most commonly caregivers reported in-person contact with care recipient everyday (72.1%). Not surprisingly, spousal caregivers reporting daily in-person contact with the care recipient, but one spouse reported seeing their spouse a few times a week. In contrast, 28 adult child caregivers reported daily in-person contact, 18 reported contact a few times a week, 7 once a week, 8 a few times a month, 5 once a month, and 12 reported in-person contact several times a year. Importantly, we do not have data on frequency of contact that was not in-person, such as via the telephone (frequently reported by caregivers, in our clinical experience) or other remote methods.
Descriptive Statistics of Sample, Presented as Number and Percent Contribution to Total Sample Along and associated ZBI Scores for Caregiver Subgroups.
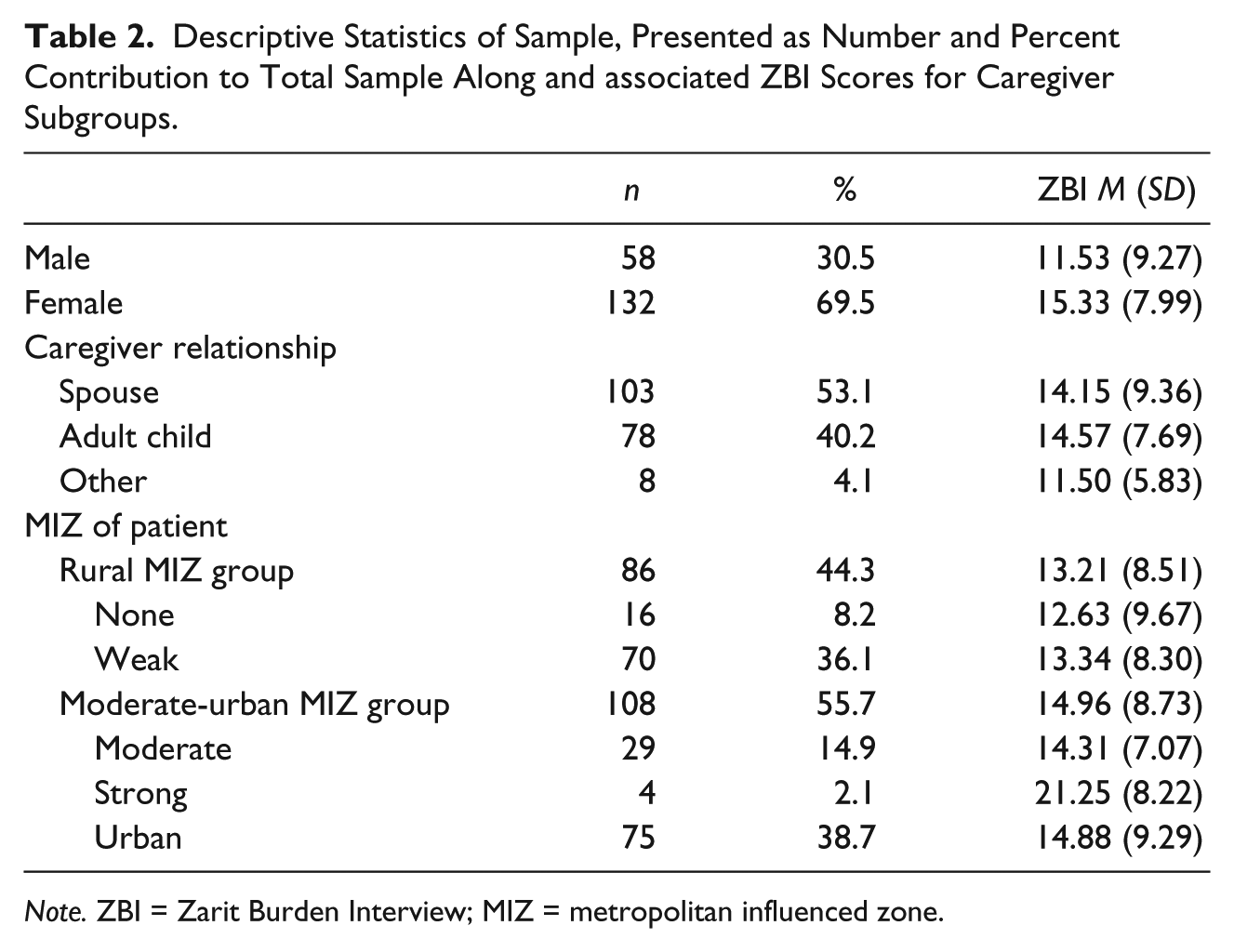
Note. ZBI = Zarit Burden Interview; MIZ = metropolitan influenced zone.
Frequency of Caregiver–Care Recipient In-Person Contact, Presented as Number and Percent Contribution to Total Sample.
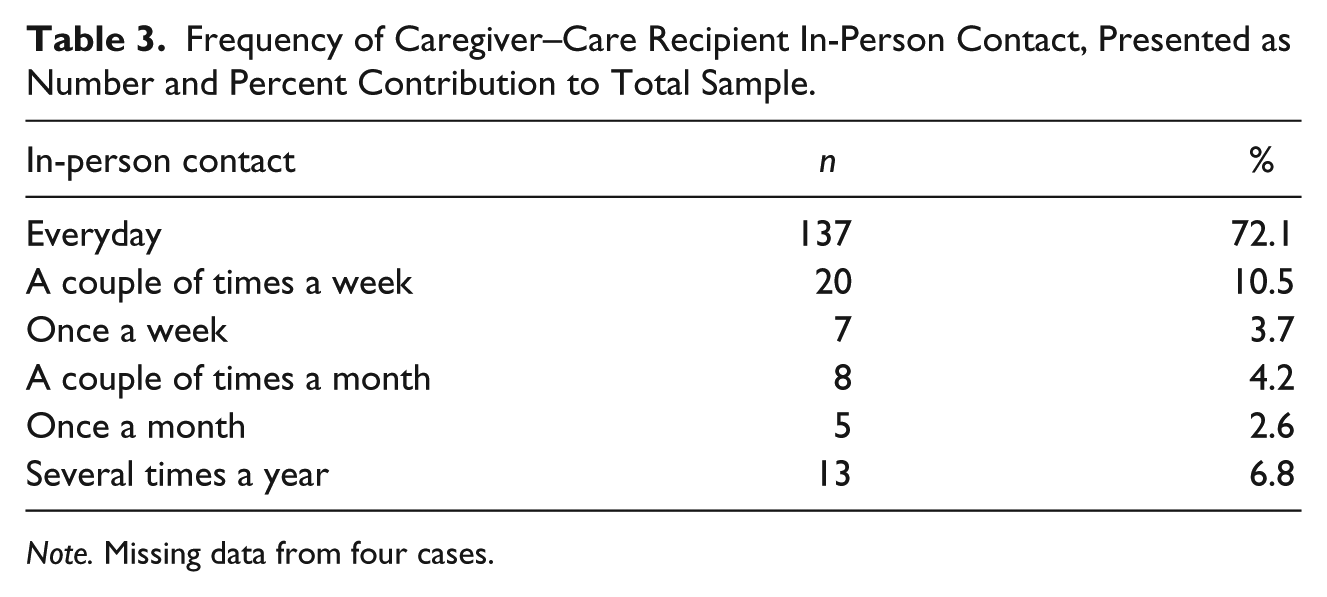
Note. Missing data from four cases.
The predominant diagnosis for care recipients was dementia due to AD, but dementia etiologies varied (i.e., vascular dementia, dementia due to Lewy Body Disease, dementia due to frontotemporal lobar degeneration). The mean age of the care recipient was 74.67 (SD = 9.00), excluding three cases with missing information. The care recipients were predominantly female: 118 female (59.9%) and 76 male (38.6%). The mean CDR-SOB was 6.74 (SD = 3.43), suggesting that on average, patients were quite impaired (i.e., this score is equivalent to being impaired in each of the six cognitive and functional domains measured).
ZBI Analyses
Descriptive analysis of the 12-item ZBI data indicates a mean ZBI score of 14.19 (SD = 8.67; range = 0-48). To explore group differences in ZBI based on caregiver gender (male or female) and relationship (spouse, child, or other), a 2 × 3 ANOVA revealed a statistically non-significant but small main effect of relationship, F(2, 183) = 0.54, p > .05,
The results of the EFA on the ZBI are displayed in Table 4. These data do not support the emerging research suggesting a third factor measured in the ZBI with the 12-item version. Results indicated a two-factor structure with Factor 1 accounting for 49.5% of variance and Factor 2 accounting for 14.1% of the variance. Factor loadings were consistent with the previous research; items 1-9 loaded significantly on Factor 1, commonly referred to as “personal strain” (Bedard et al., 2001; O’Rourke & Tuokko, 2003; Siegert et al., 2010). Items 11 and 12 loaded higher on Factor 2, “role strain,” and appear to be driving the second factor. In the case of Item 10, “Do you feel uncertain about what to do about your relative/friend?” loading estimates were similar across factors, 0.553 on Factor 1 and 0.557 on Factor 2. For the purpose of further analysis, Item 10 must be designated to one of the two factors. The equal factor loading for Item 10 is a finding similar to O’Rourke and Tuokko (2003), whose EFA loading estimates for this item differed by only 0.1, and CFA indicated significant loading across factors for Item 10. With the exception of Item 10, the item loadings in O’Rourke and Tuokko’s (2003) study are consistent with Bedard et al.’s (2001) predictions. Bedard and colleagues (2001) produced the 12-item ZBI, creating this version from the 22-item ZBI based on factor analysis and total-item correlations. Bedard et al. (2001) proposed a factor structure of the new 12-item ZBI, placing Item 10 in Factor 2, “role strain.” Due to minimal existing data, the current researchers consider the factor loading of Item 10 in studies using the 22-item version of the ZBI where Item 10 consistently loaded on Factor 1, “personal strain” (Ankri et al., 2005; Knight et al., 2000; Siegert et al., 2010). While it is not ideal to rely on item loadings from versions other than the 12-item ZBI, the literature shows consistent item loadings across ZBI versions. Thus, for the purpose of further analysis, Item 10 was loaded on Factor 1, “personal strain.”
Factor Analysis Using Oblique Rotation, of the 12-Item ZBI in Sample of Caregivers of Persons With Dementia.
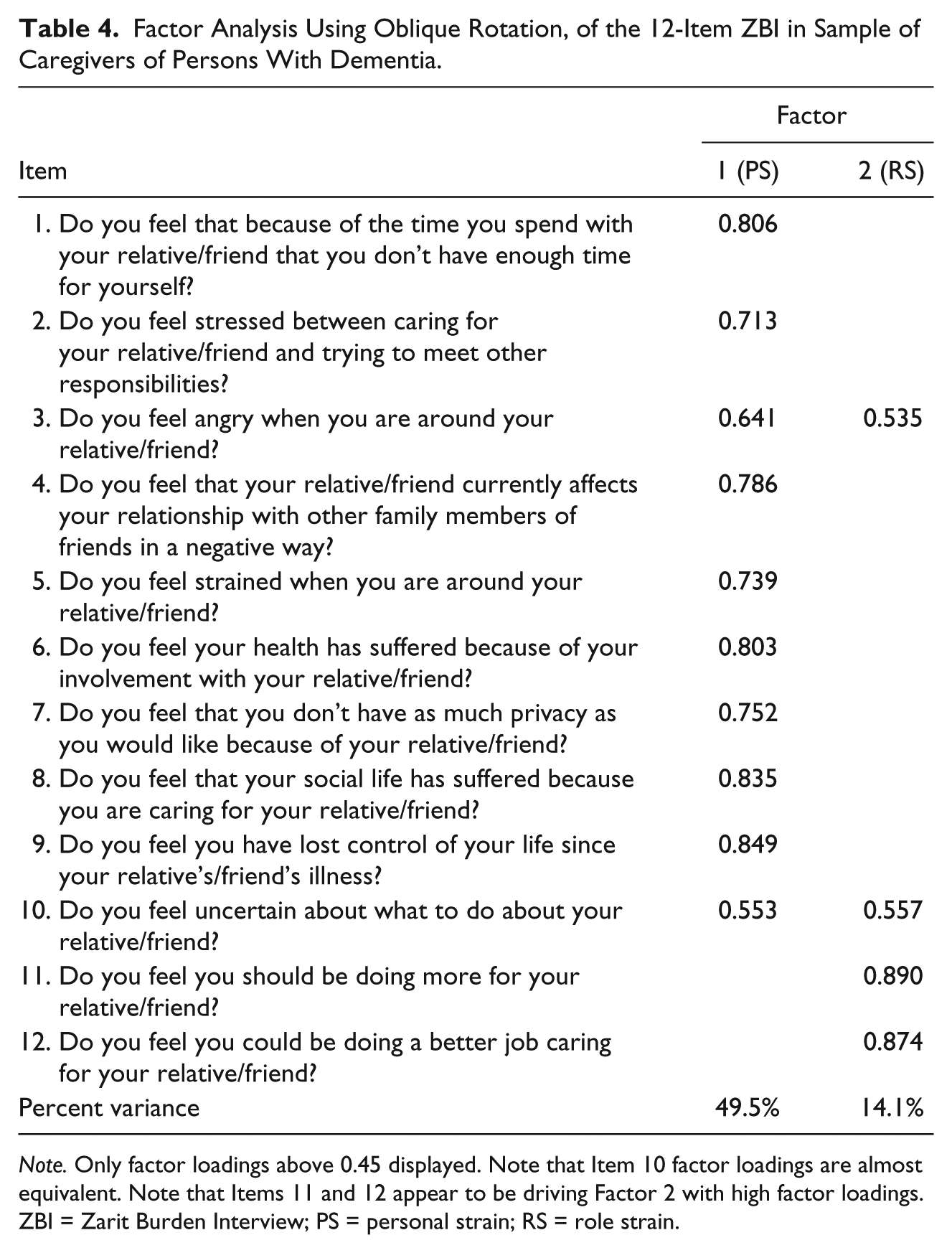
Note. Only factor loadings above 0.45 displayed. Note that Item 10 factor loadings are almost equivalent. Note that Items 11 and 12 appear to be driving Factor 2 with high factor loadings.
ZBI = Zarit Burden Interview; PS = personal strain; RS = role strain.
Exploration of factorial invariance was performed for two subgroups of caregivers: adult children versus spouses based on the postulation that these two groups may demonstrate differential expressions of guilt as caregivers (data from non-spouses or adult children were excluded from this analysis). For spouses and adult children, we found evidence for weak invariance; constraining the factor loadings to be equal for adult children and spouses did not improve the model above and beyond the unconstrained model (χ2 difference = 10.45, p = .402), suggesting that the loadings supporting the two-factor structure were equivalent for adult children and spouses. Although not all agree to which level measurement invariance must be demonstrated (Wu, Li, & Zumbo, 2007), it is notable that these data did not support strong (strict) invariance to measurement across spouses and adult children. For the purpose of the current study, where the focus is on the basic factor structure of the ZBI as a two-factor measure versus a three-factor measure, invariance to factor loadings is likely sufficient. A similar analysis was performed for two MIZ groups: those with no or weak MIZ versus caregivers of patients located in a residence of a moderate MIZ to urban center. Similarly, weak invariance was supported with the factor loadings demonstrating equivalence for the groups based on MIZ (χ2 difference = 11.15, p = .346).
Stepwise multiple regression for the ZBI factor of “personal strain” suggested predictors of BSI (t = 3.62, p < .001), CDR-SOB (t = 3.86, p < .01), and MCS (t = 2.38, p = .018) were significant, with BSI alone accounting for 19.9% of the variance, which was improved by the addition of CDR-SOB (R2 = .282), and further improved by the addition of MCS (R2 = .305), but the addition of PCS did not improve prediction (t = .39, p > .05). Conversely, only MCS predicted “role strain” (t = 4.40, p < .001, R2 = .099), and the addition of BSI (t = 1.79, p > .05), CDR-SOB (t = 0.48, p > .05), and PCS (t = 0.86, p > .05) did not improve prediction.
Discussion
Although recent data suggest that the ZBI may measure a third latent variable of guilt, we found support for two factors in the 12-item ZBI in a sample of caregivers of persons with dementia. Moreover, we demonstrated measurement invariance across subgroups of caregivers: The ZBI reflects a two-factor structure when it is used in spouses and in adult children caregivers, despite some evidence that adult children caregivers are more likely to demonstrate guilt (Gonyea et al., 2008). In addition, two factors were found irrespective of degree of rurality despite a postulation that degree of rural residence might contribute to guilt through greater unmet needs in more rural locations. Finally, psychological distress, quality of life, and severity of patients’ dementia were explored as predictors for each factor and predictors differed for the two factors providing further support for the separability of these two factors. A two-factor structure is consistent with the previous studies regarding the factor structure of the 12-item ZBI in caregivers of persons with cognitive impairments (Bedard et al., 2001) and dementia (O’Rourke & Tuokko, 2003). Some studies refer to a factor as “personal strain” or “role strain” (Bedard et al., 2001, O’Rourke & Tuokko, 2003), but others have labeled them “embarrassment/anger” or “patient dependency,” respectively (Flynn Longmire & Knight, 2011; Knight et al., 2000). Irrespective of labels, there is consistency in general definitions for the two factors. “Personal strain” can be conceptualized as “how personally stressful the experience of caregiving is” (Kumamoto & Arai, 2004; Whitlatch, Zarit, & von Eye, 1991). Accordingly, the items commonly associated with “personal strain” surround the caregiver’s subjective and emotional responses to a range of aspects of caregiving. Examples include the time requirement associated with caregiving and how that may affect the caregivers’ personal time and time for other relationships, or how a caregiver’s sense of control over their life is affected by the diagnosis, and progression, of the recipients’ illness. Items which loaded highest (greater than 0.79) on “personal strain” in the current study were those pertaining to “time for self,” “health and social life,” “privacy,” and “lost control of life.” It is not surprising that the subjective and emotional nature of the items comprising “personal strain” translates into a factor predictive of psychological distress. While the specifics of the items in “personal strain” range notably, it would appear that an underlying theme pertains to time and a need for personal recognition, as an individual, but also within the context of other relationships (i.e., friend, sister, father, employee). “Role strain” appears more reflective of the pragmatics associated with caregiving, rather than a personal appraisal of the experience. In fact, it can be adequately described as “the stress due to role conflict or overload” (Kumamoto & Arai, 2004; Whitlatch et al., 1991).
The 12-item ZBI items of “should be doing more” and “could be doing a better job,” which in the current study loaded on “role strain,” are the same two items often embedded in the factor identified as “guilt” or “self-criticism” in studies supporting a three-factor structure (Ankri et al., 2005; Flynn Longmire & Knight, 2011; Knight et al., 2000). It remains possible that a three-factor structure is unique to the 22-item ZBI when completed by dementia caregivers (Ankri et al., 2005; Knight et al., 2000) or to the 14-item version (Flynn Longmire & Knight, 2011), which accounts for the lack of a third factor found with the 12-item version in this study and a previous study (O’Rourke & Tuokko, 2003). It is also possible that the differences in sample characteristics across these studies account for the differences in factor structure. Most notably, the one study to replicate this finding was also Canadian with a predominantly Caucasian sample. The two U.S.-based samples demonstrated a third factor each containing a large proportion of Black caregivers (13.3% in one subsample, 33.9% in another subsample, Knight et al., 2000; 21.3% in one subsample and 33.8% in another subsample, Flynn Longmire & Knight, 2011), and the final study to reveal a third factor was a French-based sample (Ankri et al., 2005) of caregivers. These discrepancies underscore the need to determine factor structure in a wide variety of caregiver samples. Future research on the factorial invariance of the ZBI in non-Canadian predominantly Caucasian caregivers is clearly needed.
Although a third factor of “guilt” was not identified in this study, these specific items were clearly the main contribution to “role strain.” Perhaps most surprising in our findings was the fact that “role strain” was not strongly associated with caregivers’ psychological distress. Irrespective of whether labeled “guilt” in one study or “role strain” in another, if the latent construct really did capture some aspect of caregiver guilt, we would have predicted, based on the previous data (e.g., Boye, Bentsen, & Malt, 2002; Gonyea et al., 2008; Spillers, Wellisch, Kim, Matthews, & Baker, 2008), that it would be related to psychological distress in caregivers. Using the 22-item ZBI, where a three-factor structure was revealed, the “guilt” factor identified by Ankri and colleagues (2005) demonstrated a high correlation with the Caregiver Guilt Questionnaire (Losada, Marques-Gonzalez, Penacoba, & Romerp-Moreno, 2010). Clearly, additional research is required on the measurement of the construct of guilt with the ZBI, but particularly with abridged versions of the ZBI.
Although these data are useful for providing information about the measurement properties of one abridged version of the ZBI, the generalizability of these data is restricted to the sample. The sample used for this study was drawn from a larger sample of “help-seeking” caregivers living in rural or remote locations. Convenience sampling from “help-seeking” caregivers may present a sample of particularly distressed caregivers or, potentially, particularly resourceful caregivers. It remains possible that highly resourceful caregivers are less likely to experience guilt, which could impact the measurement of the latent properties of the ZBI. An alternative suggestion could be that they are more likely to experience guilt, and this guilt underlies the help-seeking behavior. We are unable to compare the measurement invariance for help-seeking and non-help-seeking caregivers to address these speculations. Another important sample characteristic is the frequency of in-person contact, which varied from every day for all, but one spouse to less frequent, reported by adult children caregivers. Adult children of rural parents with dementia may live elsewhere due to economic necessity (and choice) and, therefore, see their parents in-person less frequently, but we do not have data on other forms of remote contact nor do we have data on how remote caregiving interacts with caregiver burden. Regardless, these data suggest that the 12-item ZBI is best captured by two factors, irrespective of whether the caregiver is a spouse, who has daily contact, or an adult child, who is more likely to report less frequent in-person contact. A further limitation pertains to the measurement of invariance due to degree of rurality. It is important to stress that we measured rurality of the patient and not the caregiver, which may have differed. The patient’s access to resources as an important factor in the development of caregiver guilt was the rationale for the analyses, but does limit these findings. Finally and perhaps most relevant to the current study are the limited data on guilt in the archival database. Additional measures of guilt administered to this caregiving sample would have allowed for more definitive conclusions regarding the importance of the predictive value of “role strain,” the factor clearly driven by items presumed to measure guilt in longer ZBI versions.
In conclusion, the current study adds to the literature regarding the factor structure of the ZBI. The results indicate a two-factor structure of the 12-item ZBI, incorporating factors of “personal strain” and “role strain.” This finding is consistent with the previous research and provides support for the psychometric properties of the 12-item ZBI proposed by Bedard and colleagues (2001). Moreover, we provide novel data supporting the factorial invariance to relationship (spousal versus child caregiver) and degree or patient’s rurality. These data suggest the 12-item ZBI provides a measure of burden that assesses both “personal strain” and “role strain” but fails to adequately capture “guilt” within the context of caregiver burden.
Footnotes
Acknowledgements
We thank Dr. Peter Grant for his comments on our structural equation modeling analyses.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: D. Morgan’s work was supported by an Applied Chair in Health Services and Policy Research from the Canadian Institutes of Health Research (CIHR) and the Saskatchewan Health Research Foundation (SHRF).