
Abstract
Background
Self-neglect in older adults has gained considerable attention over the past decade as an important public health problem (Burnett et al., 2012). Characterized by the failure to adequately perform activities to promote safe and independent living, multiple studies have linked self-neglect in older adults with an increased risk of early mortality, increased rates of hospitalizations and emergency room visits, and, more recently, with decreased adherence to prescribed medication regimens compared with non-self-neglecting older adults (Dong et al., 2009; Dyer, Goodwin, Pickens-Pace, Burnett, & Kelly, 2007; Lachs, Williams, O’Brien, Pillemer, & Charlson, 1998; Turner, Hochschild, Burnett, Zulfiqar, & Dyer, 2012). Unfortunately, self-neglect in older adults is the most common report to Adult Protective Services (APS) nationwide, and the number of reports is expected to increase proportionally as the U.S. population ages (Pavlik, Hyman, Festa, & Dyer, 2001).
Unfortunately, self-neglecting older adults often present with varied and concomitant physical and social conditions that may impair their ability to properly adhere to their prescribed medication regimens. These conditions include impaired executive function, low social support, isolation, depression, and poor physical function (Dyer et al., 2007). Several studies have shown that these characteristics, among others, are associated with poor medication adherence in older adults (Yap, Thirumoorthy, & Kwan, 2016). Although not powered for subgroup analyses, Turner et al. (2012) provided preliminary results indicating that poor physical performance was associated with lower adherence. Likewise, they reported that a higher number of medications were also associated with lower adherence levels (Turner et al., 2012). Number of medications is only one component of many medication-related factors that may affect medication adherence in older adults. However, the finding by Turner et al. is an important first step toward understanding whether some self-neglect behaviors are simply related to complicated self-management tasks.
Potentially compounding the issues of medication adherence in a medically burdened, community-based population of older adults is the complexity adhering to complicated regimens. Maximizing the benefits of prescribed medications while avoiding adverse events related to inappropriate medication administration often requires following a comprehensive set of directions for taking the medications. The number of medications taken, dosing, and additional prescriber instructions all contribute to the complexity of an individual’s medication regimen (Paquin et al., 2013). Higher levels of medication regimen complexity have been associated with lower levels of medication adherence in the general population of older adults (Claxton, Cramer, & Pierce, 2001; Corsonello et al., 2009). The significance of medication regimen complexity as a risk factor for nonadherence in self-neglecting older adults, however, is unknown.
Medication adherence and contributing factors such as regimen complexity in community-dwelling older adults with APS-substantiated self-neglect are widely unstudied. This gap in the literature likely results from the lack of access to this population for primary data collection and the difficulty enrolling these individuals into research-driven studies. To the authors’ knowledge, no studies assessing the link between medication regimen complexity and medication regimen adherence have been conducted. This study aims to (a) characterize medication regimen complexity and medication adherence in a community-based sample of older adults with APS-substantiated self-neglect and (b) examine the relationship between medication regimen complexity and adherence, controlling for the influence of several known contributors to poor medication adherence in older adults. Based on the previous study by Turner et al. (2012), we hypothesize that higher medication regimen complexity will be associated with lower medication adherence levels. Understanding the relationship between complexity and adherence in self-neglecting older adults may provide an avenue for developing individual- and system-level interventions for promoting positive health outcomes in this vulnerable population.
Method
Sample and Recruitment
This study is a secondary analysis of 31 participants with baseline data collected as part of a primary intervention to increase medication adherence in community-dwelling older adults with APS-substantiated self-neglect. APS are the state agencies charged with investigating alleged cases of self-neglect in adults aged 18-64 years with substantial disabilities and for those 65 and older. The primary study was a 12-month feasibility trial targeting change in theory and evidence-based personal and environmental determinants of medication adherence in older adults who self-neglect. The study was designed with a 6-month intervention of educational sessions, environmental cues, and social calls to promote adherence followed by a 6-month withdrawal of the intervention components. All participants included in the primary intervention met the following criteria: Participants (a) were at least 65 years of age, (b) spoke English or Spanish, (c) were community-dwelling, (d) had APS-substantiated self-neglect, (e) were taking medications for a chronic disease, (f) demonstrated capacity to give informed consent, and (g) were within a 1-h driving distance of Houston, Texas. A three-step recruitment process, successfully used previously to enroll over 300 older adults with APS-substantiated self-neglect in interventional studies, was used for the primary study and has been described elsewhere (Hansen, Flores, Coverdale, & Burnett, 2016). Written informed consent was obtained in the homes of all participants using a process reviewed and approved by the Committee for the Protection of Human Subjects at the University of Texas Health Science Center at Houston and the Texas Department of Family and Protective Services, Division of Adult Protective Services (Approval Number HSC-MS-12-0758).
Data Collection
All data were collected through in-person, home-based evaluations carried out by a registered nurse and a trained research associate. Demographic variables included age, race/ethnicity, gender, living situation, marital status, years of education, and monthly income. A comprehensive medical assessment was conducted with each participant. This assessment included a social and medical history, vital signs, medication review, and an assessment of physical function, cognitive function, memory, and mood. Additional assessments related to medication adherence included a self-reported adherence measure, pill counts, knowledge, skills, and perceived benefits and perceived outcomes associated with taking medications. All standardized assessment tools used in this study have been validated for use in the United States (Folstein, Folstein, & McHugh, 1975; Hirsch, Metz, Hosokawa, & Libby, 2014; McGivney, Mulvihill, & Taylor, 1994; Morisky, Ang, & Krousel-Wood, 2008; Reitan, 1958; Royall, Cordes, & Polk, 1998).
Medication Adherence Assessment
Medication adherence served as the primary outcome for this study. Adherence to prescription medications was measured using the Morisky Medication Adherence Scale (MMAS-8)™ (Morisky et al., 2008; Krousel-Wood, Islam, Webber, Re, Morisky & Muntner, 2009; Morisky & DiMatteo, 2011). The MMAS-8 is an eight-item self-report questionnaire that asks subjects about their general adherence behaviors and adherence in various situations, such as during travel or in the face of side effects (Morisky et al., 2008). The MMAS-8 has been shown to have high internal consistency reliability (α = .83) as well as good concurrent (r = .64, p < .05) and predictive validity. In addition, the sensitivity (93%) and specificity (53%) of the scale are adequately high (Morisky et al., 2008). The scale may be treated as either continuous or categorical. When treated categorically, scores of less than 6 indicate low adherence, scores of 6-7 indicate medium adherence, and scores of 8 indicate high adherence (Morisky et al., 2008).
Similarly to the previous study by Turner et al. (2012), pill counts were attempted as an alternative method for assessing medication adherence. However, in the current sample, pill counts proved unreliable and difficult to standardize due to ways in which the participants stored and took their medications. Therefore, pill counts are not reported here.
Medication Regimen Complexity Index (MRCI)
Medication regimen complexity was calculated using a 65-item tool known as the Medication Regimen Complexity Index (MRCI). The MRCI was originally developed and validated by George et al. in 2004 as an improvement on the previously-used Medication Complexity Index and has since been used in numerous studies (Advinha, De Oliveira-Martins, Mateus, Pajote, & Lopes, 2014; Elliott, O’Callaghan, Paul, & George, 2013; George, Phun, Bailey, Kong, & Stewart, 2004; Hirsch et al., 2014; Libby et al., 2013; Oosthuizen et al., 2011). There are three main sections of the MRCI: (A) medication form (tablet/capsule, paste, injectable, etc.), (B) dosage frequency (once daily, twice daily, PRN, etc.), and (C) special instructions (take with food, crush/break tablet, alternating dosage, etc.). An individual’s overall MRCI score may be calculated by summing the scores of A, B, and C. As originally intended by George et al. in 2004, calculations of regimen complexity only included prescription medications in this study (George et al., 2004). Over-the-counter medications were also excluded from MRCI calculations because adherence assessment referred only to prescription medications; to study the association between these two variables, the specific medications involved in our calculations had to be kept consistent.
The MRCI is an open-ended scale, meaning that there is no determined maximum or ceiling score (George et al., 2004). To the authors’ knowledge, no distinct levels of complexity have been defined for the community-dwelling older adult population in the United States. Previous research has demonstrated that individuals with certain medical conditions (geriatric depression and diabetes mellitus) have higher MRCI scores on average compared with individuals with other medical conditions (hypertension and HIV). However, the majority of the MRCI points tallied across all disease-specific cohorts came from medications for treating conditions other than those defining each cohort; therefore, the presence of multimorbidity appears to play the greatest role in determining an individual’s MRCI score, rather than the presence or absence of individual medical conditions (Libby et al., 2013).
The MRCI is both valid and reliable. The construct validity of the MRCI was confirmed using Spearman’s Rho by George et al. in 2004 (p < .0001 for convergent and p = .1 for discriminant) and by Hirsch et al. in 2014 (p < .05 for convergent and p > .05 for discriminant; George et al., 2004; Hirsch et al., 2014). Content validity was judged to be good by expert panels in both studies. In addition, criterion validity was found to be moderate to good (weighted κ = 0.48-0.63; Hirsch et al., 2014). In the study by George et al., all measures of interrater reliability were >.97 and all measures of test–retest reliability were >.98 (George et al., 2004).
Mini-Mental State Examination (MMSE)
Memory was assessed using the MMSE. The MMSE is scored from 0 to 30 with lower scores indicating greater cognitive impairment. A score of < 24 is sometimes used as a cutoff point for a positive screen of dementia (Simard, 1998; Tombaugh & McIntyre, 1992). The MMSE includes questions regarding orientation to time and place, registration, repetition and recall of words, attention, visuospatial function, and simple calculations (Simard, 1998). Evidence supports that lower MMSE scores are associated with lower medication adherence (Gray, Mahoney, & Blough, 2001; Insel, Morrow, Brewer, & Figueredo, 2006).
The MMSE is considered to have acceptable validity and reliability. Most studies report sufficient sensitivity (20%-100%), specificity (46%-100%), positive predictive value (31%-100%), and negative predictive value (43%-100%). Ranges of these values across studies are broad due to variation in populations from which participants were drawn, but most studies report all of these values to be >50%. Internal consistency of the MMSE has been found to be acceptable (α = .54-.96) and test–retest reliability has been found to be high (α = .80-.95 in most studies; Tombaugh & McIntyre, 1992).
Trail Making Test (TMT, Part B)
Executive function, the ability to put tasks in sequential order resulting in goal-oriented behavior, was assessed with the TMT and the Executive Clock Drawing Task (CLOX I) test (Royall et al., 1998). The TMT consists of two tests and is widely used neuropsychological assessment. Part A requires the individual to follow a sequential order by drawing draw lines connecting circles with ascending numbers (i.e., 1, 2, 3, . . .). Part B of the TMT includes drawing lines connecting both letters and numbers sequentially (i.e., 1 to A, 2 to B, 3 to C, . . .). These tests measure attention, visual search and scanning, flexibility, and the ability to maintain two simultaneous thought processes. Scoring of the TMT is a count of seconds to completion of the task (Reitan, 1958). The TMT-B has proven to be a valid measure of executive function (Sánchez-Cubillo et al., 2009). A time >273 s to completion was used to indicate impaired executive function. Evidence in the literature suggests that greater TMT-B times are associated with lower medication adherence (Hinkin et al., 2002).
CLOX I
The CLOX I is a clock-drawing task used to examine executive function (Royall et al., 1998). For the test, the subject is instructed to draw a clock showing a time of 1:45 p.m., and points are awarded based on the clock’s shape, numbers, and hand placement. Possible point totals range from 0 to 15, with a lower number of points indicating lower executive function. The CLOX I has shown high internal consistency (Cronbach’s α = .82) and interrater reliability (r = .94), as well as good construct validity shown by high correlation with MMSE scores (Royall et al., 1998).
Geriatric Depression Scale
Depression was assessed using the short form of the Geriatric Depression Scale (GDS), a 15-item questionnaire in which subjects answer questions about various depressive symptoms (Burke, Roccaforte, & Wengel, 1991). For a cutoff score of >4 indicating depression, sensitivity has been found to be between 84% and 93% and specificity between 65% and 85.7%, indicating high validity (Almeida & Almeida, 1999; Paradela, Lourenço, & Veras, 2005). Internal consistency reliability (α = 0.81) for the GDS is also sufficient (Almeida & Almeida, 1999).
Statistical Analysis
Univariate linear regression analyses were used to examine the crude association between the MRCI (continuous) and the MMAS-8™ (continuous) and other confounders, and multivariable linear regression models were used to examine the adjusted association between MRCI (continuous) and the MMAS-8™ (continuous) after controlling for potential confounding variables. The Shapiro-Wilk test was used to test normality of the outcome variable. Scatter plots were used to visually assess the linearity of the continuous measures. Purposeful selection of covariates using backward selection criteria was used for building a multivariable model. A p value of .25 for the Wald test in the univariate analyses was used to select potential confounding risk factors to be included in the preliminary multivariable model, and a p value of .05 was used to retain variables in the multivariable model (Hosmer, Lemeshow, & Sturdivant, 2004; Mickey & Greenland, 1989). Bursac, Gauss, Williams, and Hosmer (2008) showed that this method of variable selection has the capability of retaining important confounding variables and the potential to provide a slightly richer model when compared with other stepwise selection procedures (Bursac et al., 2008). We also assessed the importance of the potential confounding variables on the basis of a 10% change in the estimate of association between MRCI and MMAS-8™ (Hosmer et al., 2004). If the exclusion of a potential confounder caused a change of greater than 10% in the estimated association between MRCI and MMAS-8™, we did not remove that variable from the multivariable model despite its statistical significance. Measures of association was presented by the regression co-efficient (β), 95% confidence interval (CI), and a p value. A complete case analysis was done. Statistical analyses were performed using SAS statistical software (version 9.4; SAS Institute Inc, Cary, NC) and STATA statistical software (version 12; StataCorp LP, College Station, TX; Hamilton, 2012).
Results
The sample size of this study was 31. Sociodemographic characteristics of the sample, as well as results from cognitive assessments, can be seen in Table 1. The average age of the participants was 74.5 with a standard deviation of 6.3 years. Over half of the sample was female (64.5%) and African American (64.5%). Approximately half (51.6%) of the participants lived alone, whereas the other half lived with a spouse, relative, or in other living situations. The mean number of years of education was less than a high school education (11.2 years), with a standard deviation of 2.9 years. Average number of medications taken, including over-the-counter medications, was 9.4 with a standard deviation of 5.7. Average number of prescription medications used for MRCI calculations, not including over-the-counter medications, was 8.2 with a standard deviation of 5.4. The average number of doses per day listed on the prescription labels of these medications was 1.55. The most common medical conditions reported among study participants were hypertension (n = 25; 80.6%), coronary artery disease (n = 17; 54.8%), diabetes mellitus (n = 15; 48.4%), and heart failure (n = 11; 35.5%).
Summary Statistics and Univariate Linear Regression Analysis for Sociodemographic Measures, Medication Regimen Complexity, Depression, and Cognitive Assessments.
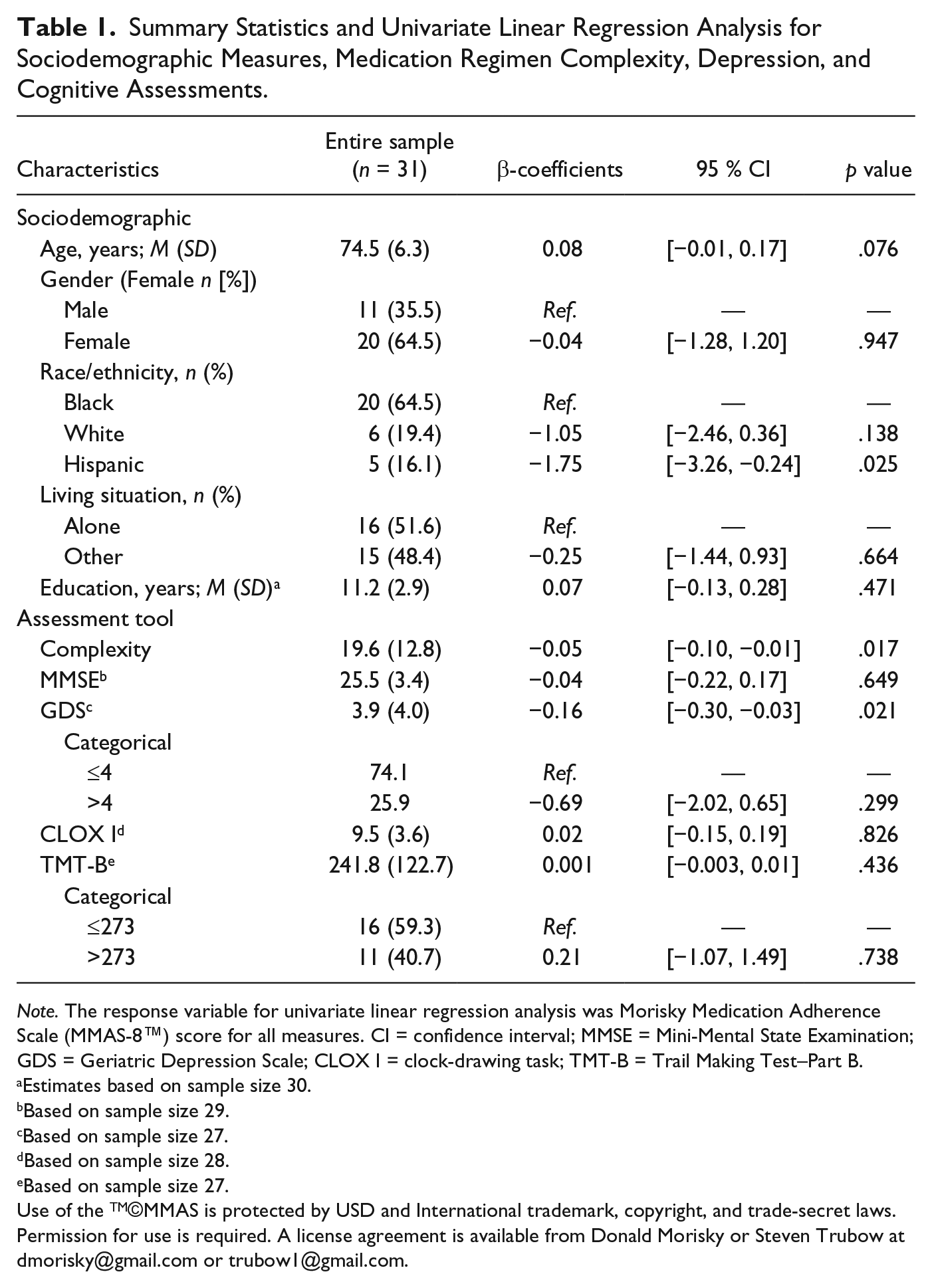
Note. The response variable for univariate linear regression analysis was Morisky Medication Adherence Scale (MMAS-8™) score for all measures. CI = confidence interval; MMSE = Mini-Mental State Examination; GDS = Geriatric Depression Scale; CLOX I = clock-drawing task; TMT-B = Trail Making Test–Part B.
Estimates based on sample size 30.
Based on sample size 29.
Based on sample size 27.
Based on sample size 28.
Based on sample size 27.
Use of the TM©MMAS is protected by USD and International trademark, copyright, and trade-secret laws. Permission for use is required. A license agreement is available from Donald Morisky or Steven Trubow at
Sample MMSE, GDS, CLOX I, and TMT-B scores can also be seen in Table 1. The mean MMSE score of the entire sample was 25.5 with a standard deviation of 3.9. The mean GDS score was 3.9, and 25.9% of the sample had scores greater than 4 (indicative of depression). The mean CLOX I score was 9.5 and the mean time to completion of the TMT-B was 241.8 s. Of the 27 subjects who completed the TMT-B task, 11 (40.7%) took more than 273 s to complete the test (indicative of low executive function).
The mean MRCI score for this sample was 19.6 with a standard deviation of 12.8. Dosing regimen contributed the most to complexity on average (MRCI Part B; M = 12.6, SD = 7.5), followed by medication form (MRCI Part A; M = 4.1, SD = 0.7) and special instructions (MRCI Part C; M = 2.8, SD = 0.4). MMAS-8™ scores ranged from 2 to 7 with a mean of 5.1 and a standard deviation of 1.6. Of the 31 subjects for whom adherence data was available, 17 had “low adherence” scores of 0-5, whereas 14 had “medium adherence” scores of 6-7. Notably, no participants scored an 8 (high adherence).
Table 2 displays the results of a multivariable linear regression model used to analyze the relationship between medication regimen complexity and self-reported adherence. Age and race/ethnicity were included in the multivariable model based on our selection criteria; however, only race/ethnicity was retained in the final model. A significant negative association between MRCI scores and medication adherence (β = −0.04; 95% CI = [−0.09, 0.00]; p = 0.046) was observed after controlling for the potential confounder of race/ethnicity. Thus, increased medication regimen complexity was shown to be an independent predictor of lower adherence.
Multivariable Linear Regression Results for Analyzing the Relationship Between Medication Regimen Complexity (MRCI Score) and Adherence (MMAS-8 Score, the Response Variable)™.
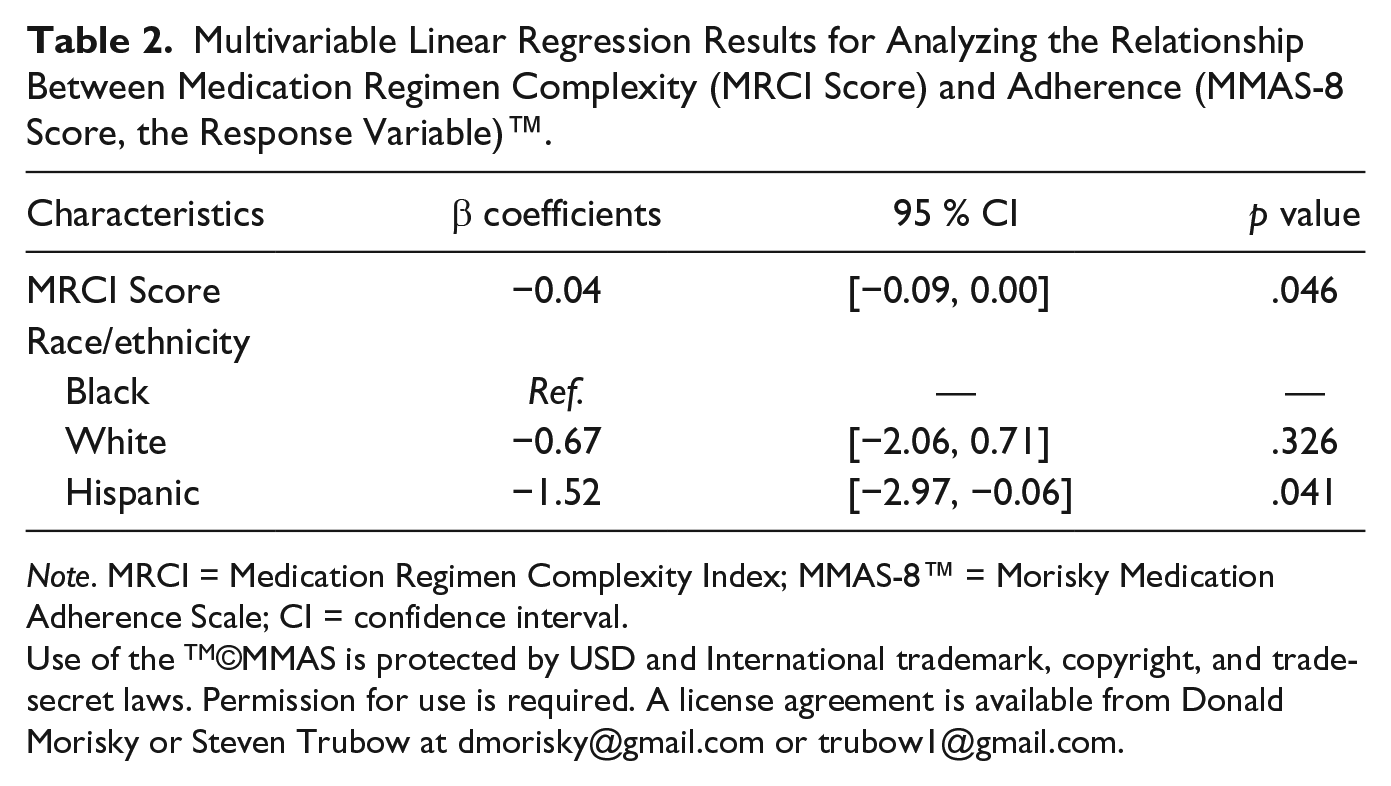
Note. MRCI = Medication Regimen Complexity Index; MMAS-8™ = Morisky Medication Adherence Scale; CI = confidence interval.
Use of the TM©MMAS is protected by USD and International trademark, copyright, and trade-secret laws. Permission for use is required. A license agreement is available from Donald Morisky or Steven Trubow at
Discussion
This study explored the association between medication regimen complexity and medication adherence in a sample of 31 community-dwelling older adults with APS-substantiated self-neglect. Despite sharing similar morbidity and mortality outcomes, the association between medication regimen complexity, medication nonadherence, and self-neglect in older adults has been understudied. In fact, only one study (Turner et al., 2012), to the author’s knowledge, has investigated medication adherence and self-neglect (Turner et al., 2012). Our findings, consistent with that study, demonstrate poor medication-taking behaviors among self-neglecting older adults. More importantly, our study provides new evidence demonstrating that medication regimen complexity is significantly associated with adherence levels among older adults who self-neglect, despite adjusting for potential effect modifiers. These findings may have implications for understanding the etiology and poor health outcomes, including elevated mortality rates, for some cases of self-neglect as well as guiding future prevention and intervention studies. Moreover, these findings question whether medication nonadherence should be truly considered a behavior of self-neglecters, given its strong link to complexity.
It is well known that adhering to one’s chronic disease medications is critical for promoting positive outcomes, reducing adverse events, and helping older adults achieve therapeutic targets and quality-of-life goals in the presence of single or multimorbidity (Osterberg & Blaschke, 2005). Interestingly, our study found that no participants reported high adherence to their medication regimens despite the tendency for individuals to overestimate their adherence levels when asked to self-report. In fact, the majority (55%) reported low adherence, whereas 45% reported medium adherence. This finding is disparate from what has been reported in other community-dwelling samples of older adults with no known self-neglect. In a large study of 2,180 community-dwelling older adults with a mean age of 75 years that also used the MMAS-8™ to measure adherence, only 14.1% had low adherence whereas 34.2% and 51.7% had medium and high adherence, respectively. Such differences in adherence may account for higher hospitalization, emergency room visits and readmissions, and increased mortality associated with self-neglect (Dong et al., 2009; Lachs et al., 1998). Identifying the barriers to adherence in this population, whether common or unique, is important for developing tailored prevention and intervention programs to reduce adverse health outcomes.
Nonadherence to prescribed medications may play a significant role in the etiology of elder self-neglect. The most common chronic conditions among self-neglecters are hypertension, diabetes, and arthritis (Dyer et al., 2007). Without proper adherence to therapeutic treatments, older adults are at risk of stroke, executive dysfunction, falls, and reduced physical performance, all of which are conducive to the development of elder self-neglect (Berry et al., 2010; Maurer, Burcham, & Cheng, 2005; Vicario, Martinez, Baretto, Casale, & Nicolosi, 2005). Dyer et al.’s (2007) etiology model of elder self-neglect suggests that self-neglect results from a cascade of events beginning with complications from nutritional deficiencies, dementia, diabetes, and/or depression (Dyer et al., 2007). Multiple medical problems may lead to executive dysfunction and impair one’s ability to perform activities of daily living. Poor adherence to prescribed medications may lead to the worsening of chronic conditions that affect one’s ability to live safely and independently. Thus, nonadherence may initiate a chain of negative events resulting in elder self-neglect. Alternatively, elder self-neglect may be one of the many potential causal factors of medication nonadherence. Longitudinal studies are needed to establish the temporality between elder self-neglect and medication nonadherence, and to understand the circumstances by which each acts as a catalyst for the other.
Aside from supporting previous findings, one of the major contributions of the current study is the significant association between medication adherence and regimen complexity. We found that elder self-neglecters had high medication regimen complexity scores (mean MRCI ~ 20), relative to other groups of older adults described in the literature. Studies with community-dwelling elders have found mean MRCI scores of 9.0-9.9, whereas those with institutionalized and hospitalized elderly individuals have found mean MRCI scores of 18.2-30.3 (Advinha et al., 2014; Ferreira, Galato, & Melo, 2015; Mansur, Weiss, & Beloosesky, 2012; Wimmer, Bell, Fastbom, Wiese, & Johnell, 2016; Wimmer et al., 2014). Thus, older adults living in the community with self-neglect appear to follow medication regimens with complexities more similar to those of elderly nursing home residents and hospitalized elders than to those of other community-dwelling older adults. Community-dwelling elder self-neglecters often live alone and often do not have assistance with medication administration. Highly complex medication regimens in the self-neglect population may thus account for previous findings showing that APS cases of elder self-neglect have significantly higher odds of institutionalization compared with other forms of abuse and neglect (Lachs, Williams, O’Brien, & Pillemer, 2002).
Our finding that complexity is independently associated with adherence levels suggests that complexity alone is an important barrier to adherence among self-neglecters. As such, medication regimen complexity qualifies as a relevant target for intervention and prevention programs for self-neglecters. Interventions such as medication reconciliation or assistive care technologies to support adherence in the presence of highly complex regimens could play critical roles in providing the necessary assistance for a person to maintain safe and independent living in their homes and to help reduce hospitalizations, emergency department admissions, nursing home placement, and early mortality.
Implications for Practice
The self-neglecters included in this study were all taking medications prescribed by licensed medical practitioners. Clinical visits, where such medications are prescribed, serve as opportunities to review medications, to assess medication regimen complexity and to make necessary changes to facilitate adherence. This will not only increase the comprehensiveness of the patient care but may also improve the health outcomes of the older adults. Social service agencies such as APS could implement more in-depth training on these topics and perhaps identify services for assisting their clients with medication administration. Such policies and procedures could be highly beneficial given that evidence-based models for reducing medication complexity and improving medication adherence in older community-dwelling older adults are available. This may also reduce the number of recidivistic cases that APS receives.
There are various ways to deal with high medication regimen complexity. First, medication regimens should be reviewed by a clinician for potential complexity reductions, such as removing unnecessary medications or simplifying dosing regimens. If safe reduction of complexity cannot be achieved because all prescribed medications are necessary, next steps to reduce the risks associated with high medication regimen complexity include referrals to home health agencies and/or discussing other options for medication management assistance.
Notably, from an operationalization perspective, our findings also allude to the idea that poor medication adherence perhaps should not simply be considered an indicator of self-neglecting behavior. Instead, intention may need to be established as the regimen may result in unintentional nonadherence. Future research should investigate intentional nonadherence from unintentional nonadherence.
Limitations
First, the parent study from which these data were obtained was a pilot study using a single group pretest–posttest design; no control group was recruited. As a result, comparison of medication regimen complexity and medication adherence between our sample and comparable community-dwelling elders without self-neglect could not be performed. Second, this study had a small sample size, limiting its statistical power and the number of covariates that could be used in analysis. Third, participants were not selected randomly; rather, they were referred to the study through APS and had to be able to provide written informed consent to participate. Therefore, results may not be fully generalizable to all older adults with self-neglect, specifically those with cognitive impairments. Finally, we used self-report for estimating medication adherence, which may have resulted in inaccuracies due to recall or depressed affect. However, we used a standardized scale to limit its threat to validity.
Conclusion
On the whole, our findings support previous evidence of poor medication-taking behaviors among older adults who self-neglect. They also provide new evidence linking low medication adherence with high levels of medication regimen complexity in this population. These findings are important as they corroborate the understanding that complex medication dosing regimens, even when necessary, may increase the risk for nonadherence and potentially harmful outcomes in this population. Although this study had a small sample size, it provides evidence to support the further study of medication regimen complexity and its relationship to medication adherence among community-dwelling older adults who neglect themselves. Given the high burdens of hospitalization and mortality in this vulnerable population, intervention and prevention programs addressing the concerns of complexity and adherence have the potential to benefit both suffering self-neglect individuals and society at large.
Footnotes
Acknowledgements
The authors would like to thank all of the participants who graciously provided their time and responses. In addition, the authors would like to thank Texas Adult Protective Services for collaborating on this study and assisting with recruitment. Without each, this and other important studies would not be possible.
Authors’ Note
Committee for the Protection of Human Subjects at the University of Texas Health Science Center at Houston and the Texas Department of Family and Protective Services, Division of Adult Protective Services (Approval Number HSC-MS-12-0758).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported in this manuscript was funded by the U.S. Administration on Community Living grant # 90EA0001/01.