
Abstract
This current study investigated the construct validity and reliability of the Geriatric Fear of Falling Measure (GFFM) among community-dwelling older adults in the United States. Eighty-eight participants were assessed on the GFFM together with demographics, falls, and fear of falling and falls-efficacy measures at baseline and an 8-week follow-up visit. Cronbach’s alpha, regression analyses, and correlation analyses were used to examine the psychometric properties of the GFFM. The results showed that the GFFM demonstrated good construct validity and reliability among community-dwelling older adults in the United States. Our findings provide evidence for the validity and reliability of the GFFM. Further study with a larger and diverse sample is needed to determine whether the GFFM has potential as a quick screening tool of fear of falling in clinical settings.
Introduction
Fear of falling is defined as a lasting concern about falling that can cause an individual to avoid activities the individual remains capable of performing (Tinetti & Powell, 1993). Such fear is common among older adults (Greenberg, 2012; Moore & Ellis, 2008) and is as serious as falling (Cumming, Salkeld, Thomas, & Szonyi, 2000; Friedman, Munoz, West, Rubin, & Fried, 2002). Although falls are often an antecedent for such fear, older adults who have not fallen also express fears about falling (Tinetti, Mendes De Leon, Doucette, & Baker, 1994; Tinetti, Richman, & Powell, 1990). Fear of falling can result in activity restriction and curtailment (Howland et al., 1998; Lachman et al., 1998; Tinetti et al., 1994), functional limitations (Curcio, Gomez, & Reyes-Ortiz, 2009; Howland et al., 1998), gait and balance problems (Brouwer, Walker, Rydahl, & Culham, 2003; Li, Fisher, Harmer, McAuley, & Wilson, 2003), reduced physical abilities (Delbaere, Crombez, Vanderstraeten, Willems, & Cambier, 2004; Li et al., 2003), social isolation (Lachman et al., 1998; Suzuki, Ohyama, Yamada, & Kanamori, 2002; Tinetti et al., 1994), depression (Arfken, Lach, Birge, & Miller, 1994; Burker et al., 1995), decreased quality of life (Arfken et al., 1994), and subsequent falls (Delbaere et al., 2004). Although fear of falling is suggested as a critical end point for fall prevention interventions among older adults (Jørstad, Hauer, Becker, & Lamb, 2005), this fear is usually not discussed or brought up by older adults (Walker & Howland, 1992), which makes it difficult for practitioners to treat fear of falling. Therefore, it is imperative to identify reliable and valid measures to detect such fear among older adults.
Despite the significance of fear of falling, the best method of assessing fear of falling remains uncertain (Greenberg, 2012; Jørstad et al., 2005; Moore & Ellis, 2008). Using a single item to assess fear of falling has been a common method (e.g., are you afraid of falling?; Tinetti et al., 1990). Although single items are useful in screening for fear of falling, this method is limited in detecting the variability of fear. The Survey of Activity and Fear of Falling in the Elderly (SAFFE; Lachman et al., 1998) is another measure developed to assess fear of falling. It has been reported that this scale is complicated to administer and not easy to score (Jung, 2008). Although a modified version of this scale was developed (Yardley & Smith, 2002), it has not been widely used (Moore & Ellis, 2008).
As noted by Moore and Ellis (2008), researchers have also operationalized fear of falling by measuring falls efficacy (i.e., the confidence in doing activities without falling). To this end, fear of falling is conceptualized as low falls efficacy (Tinetti et al., 1994). Although falls efficacy has a strong theoretical foundation (i.e., Bandura’s theory of self-efficacy; Bandura, 1982) and less psychiatric connotation compared with fear (Tinetti et al., 1994), recent research indicates that falls efficacy and fear of falling are highly correlated, but two unique constructs (Hadjistavropoulos, Delbaere, & Fitzgerald, 2011; Li et al., 2002; Moore & Ellis, 2008; Valentine, Simpson, Worsfold, & Fisher, 2011). Hence, falls efficacy and fear of falling should not be used interchangeably.
A fear of falling measure that has received less attention is the Geriatric Fear of Falling Measure (GFFM; Huang, 2006). The GFFM was developed based on a conceptual model (Huang, 2005) to measure perceptions about falls and the circumstances when fear about falling develops among community-dwelling older adults in Taiwan (n = 25, Mage = 71.08 years, SD = 7.36, range = 65-82). Thus, the GFFM may be able to assess fear of falling among older adults more accurately.
Initially, Huang (2006) developed 46 descriptions portraying situations that might trigger fear of falling and categorized them into four themes: psychosomatic symptoms (i.e., physical symptoms and emotional reactions resulting from a fear of falling), attitudes of risk prevention (i.e., individuals’ thoughts or behaviors used to prevent falls and readiness for emergency situations), attention to environmental safety (i.e., focusing on environmental modification and safety devices used to prevent falls), and modifying behavior (i.e., related to making conscious adjustments to avoid falling). Five items were removed from the GFFM scale after a panel of experts examined each item. The content validity index of this revised scale was 86% (with 41 items). Huang further conducted an item reduction procedure to create a short version of the instrument. The resulting version of the GFFM included only 15 items: four items in the psychosomatic symptoms subscale (e.g., my heart races when I think about falling after climbing to reach something high), five items in the adopting an attitude of risk prevention subscale (e.g., nowadays, I do less housework that requires more walking, such as sweeping and mopping), and six items in the modifying behavior subscale (e.g., I will ask others for help when I need something that is too high to reach). No items from the theme “attention to environmental safety” were retained in this revised version.
The 15-item GFFM was designed to be administered by health care providers as a screening tool. It takes approximately five minutes to complete. Individuals are asked to rate how often they experience each statement on a 1 (never) to 5 (always) scale. The total score can range from 15 to 75. A higher score indicates a greater fear of falling. Huang (2006) provided evidence for the construct validity (i.e., overall model fit: χ2(1, N = 384) = 266.14, p < .001, df = 87, χ2/df = 3.06, goodness of fit index = .92, adjusted goodness of fit index = .89, comparative fit index = .90, root mean square error of approximation = .07; and the relationship with the Falls Efficacy Scale [FES]: r = .29, p = .002) and reliability (i.e., internal consistency: Cronbach’s α = .86; and 2-week test–retest reliability: r = .88, p < .001) of the 15-item version of the GFFM using a sample of community-dwelling older adults aged 65 years and older in Taiwan.
A limitation of existing fear of falling measures is they often require older adults to rate their fear of falling on a hypothetical activity if they do not currently engage in the activity (e.g., the FES; Tinetti et al., 1990). However, using hypothetical questions may not be appropriate with older adults because of age-related cognitive decline (Holbrook, Cho, & Johnson, 2006; van der Zouwen & Dijkstra, 2002). Furthermore, older adults tend to perform poorly on unfamiliar tasks (Charness, 1987) and this can be exacerbated by low self-efficacy (Artistico, Cervone, & Pezzuti, 2003). In contrast to other measures, the GFFM does not focus on preset daily activities. Furthermore, the descriptions of items in the GFFM incorporate full action (e.g., I will sit on a chair or hold some support when taking a bath) not just an activity (e.g., take a bath or shower in the Tinetti et al., 1990). Thus, another strength of the GFFM is that hypothetical ratings of items are minimized.
Despite these strengths, the GFFM has only been validated with older adults in Taiwan (Huang, 2006). It has been suggested that additional testing of this screening tool is required to determine if it is valid among older adults in other countries (Greenberg, 2012; Moore & Ellis, 2008). Thus, this study examined the validity and reliability of the GFFM among a sample of community-dwelling older adults in the United States. Specifically, construct validity was established by examining (a) associations between the GFFM and a measure of falls efficacy, (b) the ability of the GFFM to predict functional mobility, (c) the ability of the GFFM to predict self-reported falls, and (d) group differences on the GFFM between fallers and nonfallers. Reliability was established by examining (a) internal consistency and (b) 8-week test–retest reliability.
Method
Design
The current study was part of a larger study that used a quasi-experimental design (treatment group: intervention, comparison group: no intervention) to investigate the effects of a program to reduce fear of falling among community-dwelling older adults (Chen, Edwards, & Janke, 2015). All participants were interviewed by either the primary investigator or trained research assistants at baseline and at an 8-week follow-up visit. The University of South Florida Institutional Review Board approved the study protocol (Pro00007425), and informed consent was obtained from all participants.
Participants
Participants were recruited from a study participant registry or through flyers posted in community centers and independent living apartments. The eligibility criteria included community-dwelling adults aged 65 years or older, who understood English, and did not use a wheelchair. The final sample included 88 participants with a mean age of 77.89 years (SD = 8.08) and a mean education of 14 years (SD = 2.86). The majority were White (82%) and female 73% (see Table 1).
Characteristics of All Participants at Baseline and Characteristics of Individuals in the Comparison Group at Baseline and the 8-Week Follow-Up.
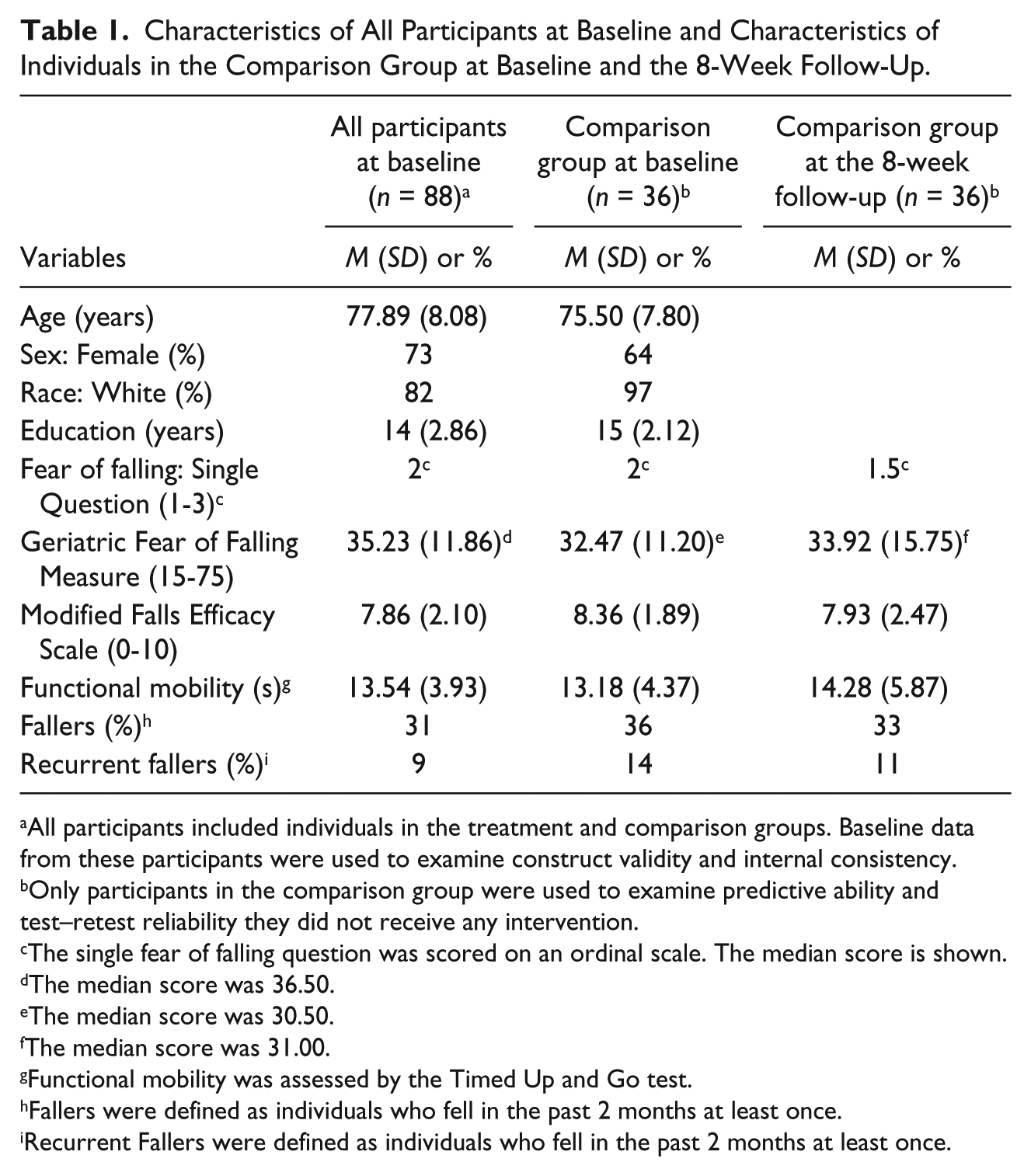
All participants included individuals in the treatment and comparison groups. Baseline data from these participants were used to examine construct validity and internal consistency.
Only participants in the comparison group were used to examine predictive ability and test–retest reliability they did not receive any intervention.
The single fear of falling question was scored on an ordinal scale. The median score is shown.
The median score was 36.50.
The median score was 30.50.
The median score was 31.00.
Functional mobility was assessed by the Timed Up and Go test.
Fallers were defined as individuals who fell in the past 2 months at least once.
Recurrent Fallers were defined as individuals who fell in the past 2 months at least once.
Measures
Demographics
Participants’ age and education were measured in years. Sex and race were dichotomized with male and non-White as the reference group.
Fear of falling
Fear of falling was assessed by the GFFM. An English version of the GFFM was obtained from the original developer (Huang, 2006). The GFFM included 15 items and was rated on a scale of 1 to 5. A composite score was calculated for each individual, with higher scores indicating greater fear of falling.
Falls efficacy
The Modified Falls Efficacy Scale (mFES) was used to measure falls efficacy (Hill, Schwarz, Kalogeropoulos, & Gibson, 1996). The mFES includes 14 activities with a rating scale from 0 (not confident) to 10 (completely confident). Participants were asked to score activities hypothetically if they did not perform the activities. An average score ranging from 0 to 10 was computed for each participant. Higher scores indicated greater confidence in performing activities without falling. The mFES was previously found to have acceptable construct validity (examined by the difference between healthy older adults and individuals who attended a falls clinic: F(14, 159) = 5.25, p < .001), internal consistency (Cronbach’s α = .95), and 1-week test–retest reliability (intraclass correlation coefficient [ICC] = .95; Hill et al., 1996).
Functional mobility
Participants’ functional mobility was measured by the Timed Up and Go test (Shumway-Cook, Brauer, & Woollacott, 2000). This test was administered by asking participants to walk a 3-meter course starting from and ending in the same chair using normal pace. Time (in seconds) required to complete the test was used in analyses.
Falls
A fall was defined as an unexpected event in which the adult came to rest on the ground, floor, or lower level (Lamb, Jørstad-Stein, Hauer, & Becker, 2005). During the baseline and postintervention interviews, participants were asked, have you experienced any falls in the past 2 months? If participants answered yes, they were categorized as fallers (coded 1), otherwise they were coded as nonfallers (coded 0). Individuals who fell were further asked how many times they fell. Participants reporting two or more falls were defined as recurrent fallers (1 = recurrent fallers, 0 = not recurrent fallers).
Analyses
To examine construct validity, we investigated if the GFFM captured the concept of fear of falling. First, the relationship between the GFFM and the mFES was examined using a Pearson correlation. The GFFM was expected to have a negative relationship with the mFES. Because, older adults with a heightened fear of falling may have poorer functional mobility and be more likely to experience future falls (Arfken et al., 1994; Delbaere et al., 2004; Hotchkiss et al., 2004), the ability of the GFFM to predict functional mobility and falls history was examined. Specifically, logistic regressions were used to examine whether the GFFM scores at baseline predicted fallers and recurrent fallers at the 8-week follow-up. Linear regression was used to examine whether the GFFM scores at baseline predicted functional mobility at the 8-week follow-up. All regression models were adjusted for demographics and falls at baseline. Finally, older adults who fall are likely to have a heightened fear of falling compared with those who have not had a fall (Delbaere et al., 2004; Howland et al., 1998). Hence, the ability of the GFFM to discriminate fallers from nonfallers was investigated using independent t tests.
For reliability, internal consistency was assessed by calculating the Cronbach’s alpha of the GFFM. An acceptable Cronbach’s alpha was determined to range between .70 and .90 (Portney & Watkins, 2008). Test–retest reliability was examined with intraclass correlation (two-way mixed model, absolute agreement). An ICC above .75 was expected to demonstrate good test–retest reliability for the GFFM (Portney & Watkins, 2008).
Statistical analyses of the GFFM included data from all participants at baseline (N = 88), with the exception that the predictive ability of the GFFM and test–retest reliability were determined using data from only the participants in the comparison group who completed both baseline and follow-up interviews (n = 36; see Table 1).
Results
The characteristics of the participants are displayed in Table 1. Approximately 31% (n = 88) of the entire sample reported a fall at baseline. Of the participants who completed the 8-week follow-up interview (n = 36), 32% reported a fall at baseline and 33% at follow-up. The percentage of recurrent fallers at baseline and the 8-week follow-up were 14% and 11%, respectively.
Construct Validity
The results showed that the GFFM was significantly correlated with the mFES (r = − .71, p < .01). The GFFM at baseline did not predict falls (odds ratio [OR] = .99, 95% confidence interval [CI] = [.91, 1.07]) or recurrent falls (OR = 1.08, 95% CI = [.93, 1.25]) at the 8-week follow-up (Table 3). However, it significantly predicted poorer functional mobility (β = .29, p < .001) at the 8-week follow-up. Fallers (M = 36.59, SD = 12.97) had a higher mean score on the GFFM than nonfallers (M = 34.62, SD = 11.40), but the difference was not statistically significant, t(86) = −.72, p = .48, d = .16).
Reliability
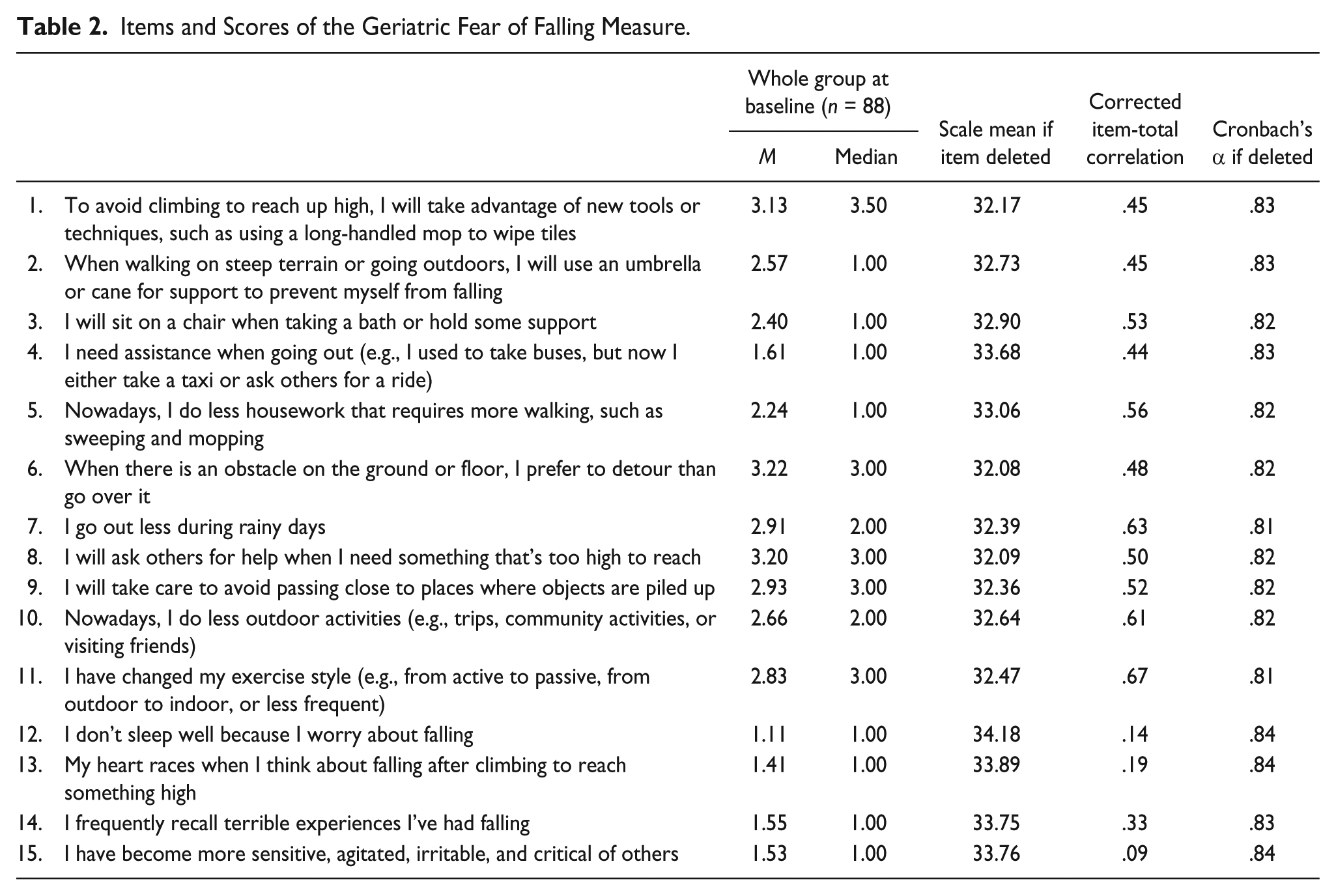
Cronbach’s alpha for the GFFM was .84 and reached the expected range, demonstrating internal consistency. Table 2 presents the mean and median scores for each item. Item 6 had the highest average score (median = 3) and Item 12 had the lowest score (median = 1). The results from the corrected item-total correlation showed that most of the items were moderately correlated with the full scale, with the exception of Items 12, 13, and 15. However, removing these items did not substantially improve the Cronbach’s alpha.
Items and Scores of the Geriatric Fear of Falling Measure.
Logistic and Linear Regression Analyses of Predictors of Falls, Recurrent Falls, and Functional Mobility.
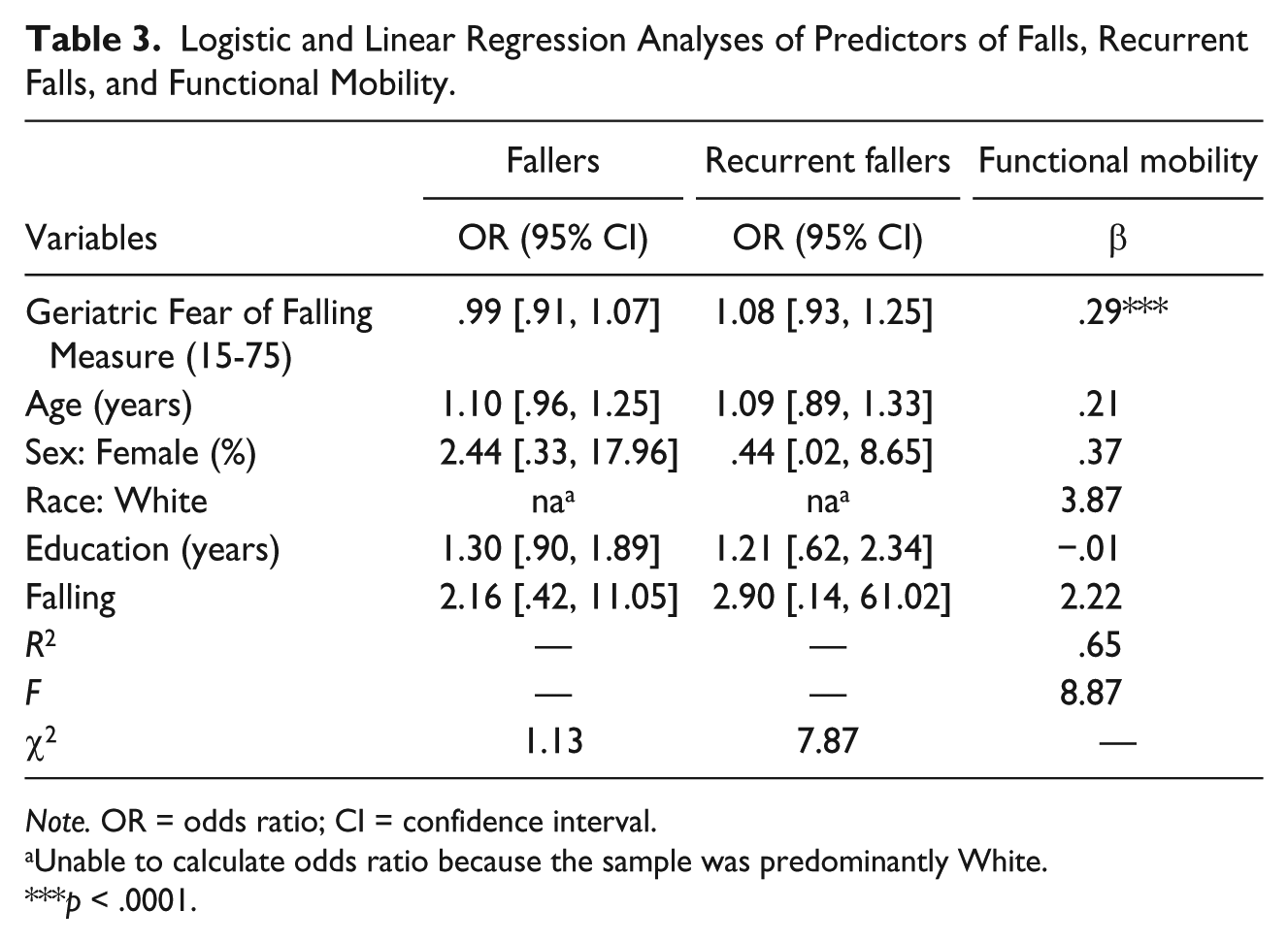
Note. OR = odds ratio; CI = confidence interval.
Unable to calculate odds ratio because the sample was predominantly White.
p < .0001.
For test–retest reliability, intraclass correlation was performed. The results showed that the single measure ICC was .79 (95% CI = [.63, .89]), indicating that the GFFM remained stable over the 8-week period.
Discussion
The purpose of this current study was to evaluate the psychometric properties of the GFFM among community-dwelling older adults in the United States. The construct validity of the GFFM was supported by its significant association with the mFES and its ability to predict poorer functional mobility in older adults. The reliability of the GFFM was supported by the homogeneity of the items within this measure and its stability over an 8-week period. Overall, our initial validation suggests the GFFM is a valid and reliable tool to assess fear of falling.
Fear of falling is a significant predictor of future falls (Hotchkiss et al., 2004). However, the GFFM did not predict future falls or recurrent falls in this current study. It is possible that the 8-week duration of the study was too short to ascertain predictive ability for falls. Although falls are common among older adults, the participants in the current study might not have reported enough falls during the 8-week period. Thus, a larger sample and longer follow-up period are recommended for future research. Another possible explanation is that older adults can experience fear of falling regardless of their falls status (Tinetti et al., 1994; Tinetti et al., 1990).
Similar explanations might apply to the nonsignificant difference in the GFFM between fallers and nonfallers. Although fallers had a higher score on the GFFM than nonfallers, there was no significant difference because the effect size and sample size were small. Besides, it is likely that some of the nonfallers also experience fear of falling (Tinetti et al., 1994; Tinetti et al., 1990).
The Cronbach’s alpha of the GFFM was within the expected range. However, Items 12, 13, and 15 did not correlate well with the full scale. Cultural differences may explain these results. These three items all fell under the psychosomatic symptoms subscale. Although somatizing distress is ubiquitous, somatic symptoms may be manifested differently across cultures (Kirmayer, 2001). Therefore, it is possible the three items used to capture psychosomatic symptoms due to fear of falling among older adults in Taiwan do not strongly reflect symptoms among older adults in the United States. Further investigation is needed to examine the contribution of these items and whether they need to be modified or removed from the GFFM.
The findings regarding test–retest reliability of the GFFM in this current study were similar to the results presented in the study by Huang (2006). For test–retest reliability, the retest was completed during the 8th week at the end point of the larger study. Comparable to the findings in Huang’s study (2 weeks), these results showed that the GFFM remained stable over an 8-week period.
There were limitations to this study. First, falls data were collected retrospectively, which may lead to recall bias. Second, older adults may have remembered the same fall experience because the recall period of falls was short (i.e., 2 months). Previous research has shown that a 12-month recall period is more reliable than a 3-month recall period (Cummings, Nevitt, & Kidd, 1988). Future studies using the self-report method to collect falls information are recommended to use at least a 12-month recall period. Third, all participants were aware they were in the study, and this could have potentially affected their behavior (e.g., become more cautious when walking), thereby affecting the results of the study (e.g., fewer falls). Fourth, only participants who lived in Florida were included in this study and the sample was predominantly White and female. Therefore, the sample is not representative of the U.S. population. Future studies with a larger and more representative sample are needed to replicate the findings from this study.
The GFFM was developed based on a conceptual model for assessing perceptions about falling and the circumstances surrounding fear about falling among community-dwelling older adults. Overall, the findings suggest that the GFFM demonstrated acceptable psychometric properties among community-dwelling older adults in the United States. These preliminary findings support the need for a larger study with a more diverse sample to investigate whether the GFFM has the potential to be used as a quick screening tool of fear of falling in clinical settings in the future.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.