
Abstract
Older adults with vision loss and a friend or family member were interviewed over a 2-year period. We examined the effects of driving cessation on life satisfaction among older adults and a social contact. Drivers’ use of public transportation was examined as a moderator. Driving cessation was associated with a decline in life satisfaction among social partners but not for the drivers. Drivers’ use of public transportation at baseline moderated the effects of cessation on changes in well-being among social partners, but had little effect on the life satisfaction of the drivers. Life satisfaction was greater among the social partners of ex-drivers who used public transportation more frequently. The association between driving cessation and well-being should be studied in the context of older drivers’ social networks. Infrastructure (e.g., subways and buses) that supports transportation needs plays an important role in mitigating the effects of cessation on older adults’ social networks.
Keywords
Driving is the primary means of mobility for most adults in the United States (King et al., 2011; Rosenbloom, 1993), and represents a vital source of meaning, identity, and autonomy (King et al., 2011; Liddle & McKenna, 2003; Yassuda, Wilson, & Mering, 1997). However, as people age, an increasing proportion of the population is faced with the difficult prospect of giving up their keys, with vision loss being one of the most commonly cited reasons for driving cessation (Campbell, Bush, & Hale, 1993; Dellinger, Sehgal, Sleet, & Barrett-Connor, 2001). For older adults, driving cessation has been linked to greater isolation, reduced out-of-home activities, declines in life space, increased symptoms of depression, and poorer health (Curl, Stowe, Cooney, & Proulx, 2014; Fonda, Wallace, & Herzog, 2001; Huisingh et al., 2017; Marotolli et al., 2000; Mezuk & Rebok, 2008; Ragland, Satariano, & MacLeod, 2005). It is unclear, however, how driving cessation may impact the well-being of drivers’ family members and friends.
According to interdependence theory, people’s outcomes are shaped in part by the broader context of their social interactions with close others (Kelley & Thibaut, 1978; Rusbult & Buunk, 1993). For example, the provision of care for individuals with disabilities or illnesses that require support often occurs in the context of a broader social network (Dilworth-Anderson, Williams, & Cooper, 1999; Tennstedt, McKinlay, & Sullivan, 1989). The primary caregiver, frequently a spouse or adult child, is often supported by a network of friends and family members who function as secondary caregivers and provide different types of instrumental and emotional support (Dilworth-Anderson et al., 1999). The provision of care is associated with a variety of outcomes among both primary and secondary caregivers, including fatigue, depression, poorer health, and lower life satisfaction (Gaugler, Mendiondo, Smith, & Schmitt, 2003; Perlesz, Kinsella, & Crowe, 2000; Staight & Harvey, 1990). The process of driving cessation and provision of transportation support may similarly be interpreted within an interdependent context. The decision to stop driving has the potential to impact the lives of not only the older adult driver but also the driver’s family members and friends (Liddle, Gustafsson, Mitchell, & Pachana, 2017). When an individual is no longer able to drive, social partners may be asked to provide rides more frequently (King et al., 2011; Kostyniuk & Shope, 2003; Rudman, Friedland, Chipman, & Sciortino, 2006), and others who relied on the former driver may find their own mobility more limited (Johnson, 2008).
Research on caregiving also suggests that the availability of community infrastructure, resources, and social programs moderate some of the effects of the burden of care on caregiver well-being (Schryer et al., 2016; Sörensen, Pinquart, & Duberstein, 2002). In the context of driving cessation, the availability and use of driving infrastructure, such as public buses, trains, and paratransit, may function to support the mobility and independence of older adults and reduce dependence on the social network (Bailey, 2004; Mezuk & Rebok, 2008). Infrastructure supporting the transportation independence of older adults may mitigate the effects of driving cessation on the well-being of both older ex-drivers and their social partners.
In this study, we use an interdependent framework to examine the effect of driving cessation on changes in life satisfaction for both older adults with age-related vision loss and a nominated family member or friend. This study also examines the use of public transportation as a moderating factor on the effects of cessation on life satisfaction for both older drivers and their social partners.
Vision Loss and Driving Cessation
A variety of studies have found that factors, such as older age, female gender, and lower socioeconomic status (SES), are associated with restrictions in driving behavior and ultimately driving cessation (Anstey, Windsor, Luszcz, & Andrews, 2006; Chipman, Payne, & McDonough, 1998; Edwards et al., 2008; Horowitz, Boerner, & Reinhardt, 2002; Meng & Siren, 2015). In addition, age-related vision loss, including decreased visual acuity, contrast sensitivity, and reduced field of vision caused by age-related impairments, such as cataract, glaucoma, and macular degeneration, has been found to be associated with greater difficulties with driving, more driving restrictions, increased accident rates, and greater likelihood of cessation (Agramunt et al., 2016; Blane, 2016; Campbell et al., 1993; Dellinger et al., 2001; Diniz-Filho et al., 2016; McGwin, Chapman, & Owsley, 2000; Owsley et al., 1998; Sengupta et al., 2014). Vision loss is also one of the primary justifications given by older drivers for why they might eventually change their driving behavior and a common reason provided by former drivers for why they stopped driving (Campbell et al., 1993; Dellinger et al., 2001). According to the Alliance for Eye and Vision Research (2012), nearly 25% of older adults in the United States above the age of 80 are legally blind or experience some degree of visual impairment. In a representative sample of Americans aged 45 and older, Horowitz, Brennan, and Reinhardt (2005) found self-reported rates of visual impairment of 17% among adults aged 45 and older and 26.5% among respondents above 75.
Social Context of Driving Cessation
To our knowledge, only one study to date has examined the long-term effects of driving cessation on the social partners of older adult drivers. Curl, Proulx, Stowe, and Cooney (2015) used multilevel modeling to examine data from seven waves of the Health and Retirement Study (1998-2010). The researchers examined the effect of driving cessation on changes in husbands’ and wives’ engagement in productive (e.g., work, volunteering) activities. When one spouse stopped driving, there was a decline in the other spouse’s likelihood of engaging in paid employment, regardless of the spouse’s gender. Wives’ engagement in volunteer activities also declined following their husbands’ driving cessation. This study focused entirely on the social outcomes of cessation for spouses. It is unclear to what extent cessation may affect the well-being of other members of the former driver’s social network, including friends, other family members, and adult children who may also be affected by cessation.
A handful of studies have interviewed family members and friends directly about their experiences and emotions related to older adults’ driving cessation. Much of this literature has focused on the emotions and burden of care expected or experienced by informal family caregivers of older adult drivers with dementia (Byszewski, Molnar, & Aminzadeh, 2010; Perkinson et al., 2005; Taylor & Tripodes, 2001). Caregivers and other social partners are typically interviewed prior to or immediately following cessation and asked to report their concerns about the consequences of cessation for themselves and the former driver. Informal caregivers report experiencing a mixture of emotions about driving cessation. Taylor and Tripodes (2001) found that caregivers were concerned that license revocation would be associated with greater reliance on them and other family members for transportation. Following cessation, caregivers did indeed report more strain and greater likelihood of missing days of work. It is unclear in this study, however, whether the missed days of work were associated with the transportation needs of the (former) drivers or with some other factor. In contrast, Byszewski et al. (2010) found that caregivers of older adults with dementia generally expressed support for revoking the driver’s license, and, at a follow-up meeting, some caregivers expressed relief that the driver was no longer on the road.
In one of the few studies to focus on a cognitively intact sample of older adults and their family members, Connell, Harmon, Janevic, and Kostyniuk (2013) interviewed a sample of adult children who indicated that their parents’ driving was a source of concern for them. Those with parents who stopped driving indicated that they had mixed feelings after cessation. Similar to caregivers, some adult children reported feelings of relief that their parent was no longer on the road. Others expressed concern that their parent might become socially isolated. Rosenbloom (2010) found that adult children of current older adult drivers were concerned about the potential impact of their parents’ cessation on their (the adult children’s) time, and worried that they might become responsible for providing more of their parents’ transportation need.
When an older adult stops driving, some friends and family members may be called upon to provide additional transportation support and others who used to depend on the older driver for transportation may lose a source of mobility. Declines in well-being after cessation may also have a trickle-down effect on members of ex-drivers’ social network. Older adults who experience declines in health and increases in depression following cessation may require more social support and care from family members and friends (Greenglass, Fiksenbaum, & Eaton, 2006; Horowitz, Reinhardt, Boerner, & Travis, 2003). In sum, past research suggests that driving cessation has an effect on the spouses, family members, and friends of older adult drivers but the exact nature of that effect is not clear. Driving cessation may alternatively be a source of strain or a source of relief for members of a driver’s social network (Connell et al., 2013).
Public Transportation
Older ex-drivers often report becoming more dependent on the members of their social network for rides following cessation (Hanson & Hildebrand, 2011; Kostyniuk & Shope, 2003). Many older adults are uncomfortable relying on these social partners for rides, reporting that they do not wish to be a burden, and expressing concern about maintaining their independence (Adler & Rottunda, 2006). Public transit (e.g., buses, subways, trains, paratransit, etc.) would seem to be a natural alternative to support the transportation needs of older adults whose driving has been restricted, allowing them to maintain greater independence, and reducing reliance on the social network. However, availability of public transportation is limited in many regions, particularly in rural and suburban areas (Johnson, 2008). According to the 2001 National Household Travel Survey, only about half (49%) of all Americans have access to public transportation service at all (Bailey, 2004). Even in areas with better public transit, some researchers have found that older adults report barriers in the form of lack of accessibility (e.g., buses that are difficult to get in and out of), lack of knowledge about the transportation system, inconvenient stops, long travel times, and questions of safety (King et al., 2011; Kostyniuk & Shope, 2003; Patterson, 1985). However, in areas with more developed public transit systems, older adults make much greater use of the system. According to Bailey (2004), older non-drivers make an estimated 310 million trips using public transit per year, and in areas with the highest neighborhood density, 58% of non-drivers, aged 65+, report at least occasional use of public transit.
The role of public transportation in moderating the effects of cessation on well-being among older drivers and ex-drivers is largely unknown. Using several waves of data from the Baltimore Epidemiologic Catchment Area study, Mezuk and Rebok (2008) found that the inability to use public transit was associated with a smaller size of social network and lower frequency of contact with family members among older adult drivers over time. It was unclear, however, whether participants’ inability to use public transit was a result of the lack of availability of public transit or an inability to use public transportation because of health constraints. Mezuk and Rebok’s (2008) study does, however, suggest that public transit, where it is available, may be associated with better social network integration among those individuals who are willing and able to use it.
This Study
Few studies to date have examined the broader consequences of driving cessation in a social context. To smooth the transition from driver to ex-driver, it is important to understand the effects of that change not only on the drivers themselves but also on the friends and family members who may be supporting the ex-driver through that change. Harrison and Ragland (2003) concluded from a literature review that there is evidence for a negative association between driving cessation and life satisfaction among older drivers. However, they cautioned that in much of the research, it is unclear to what extent cessation is causally related to life satisfaction.
Studies have found that older drivers and their family and friends express concern about the potential impact of cessation on members of the social network as well as the older driver (Byszewski et al., 2010; Connell et al., 2013; Perkinson et al., 2005; Taylor & Tripodes, 2001). Research by Curl et al. (2015) further suggests that the social integration of both older adult drivers and their spouses may be affected by the driving cessation of at least one of the partners. However, the literature provides only indirect evidence that cessation has an impact on social contacts’ overall sense of well-being. The current research expands on past studies by examining the effects of cessation on changes in life satisfaction over time among drivers and a nominated friend and family member. We also explore the role of public transportation use as a potential moderator of the effects of cessation on the well-being of older adult drivers and their social partners. If the interaction between driver status (continuing vs. ex-driver) and the use of public transit is significant, it would suggest that the effect of cessation on changes in life satisfaction among older adults and their social partners over time may depend in part on drivers’ use of public transportation alternatives prior to cessation.
Thus, our research questions are as follows. Controlling for covariates, including demographic variables (age, gender, and SES), changes in driver’s health, availability of rides from the social contact, driver’s visual functioning, and frequency of driving at baseline,
Method
Participants
Eligible participants were recruited through a vision rehabilitation agency (79%) or through service provider programs and community outreach efforts (e.g., newspaper ads) in the greater New York City area. Older drivers were invited to participate in a 2-year longitudinal study on driving behavior among older adults with vision loss. Eligibility requirements included English-speaking, community-dwelling, current drivers, and age 55 and older with self-reported vision loss that could not be corrected with lenses. Eligible participants were also required to have sufficient cognitive functioning and hearing to be able to participate in face-to-face and telephone interviews. Participants were interviewed at five time points (baseline, 6 months, 12 months, 18 months, and 24 months) by trained interviewers with a master’s degree in clinical or developmental psychology, social work, or a related field. Three of the interviews (baseline, 12 months, and 24 months) were conducted in person and the remaining two were administered over the phone. At the baseline interview, participants were asked to nominate a friend or family member with whom they would be the most likely to discuss issues related to driving. Telephone interviews were conducted with social contacts at baseline, 12 months, and 24 months.
Of the 610 individuals who were contacted and met the eligibility requirements, 381 agreed to participate in the baseline interview, for a response rate of 62.5%. Among the baseline participants, 215 individuals nominated a social contact who was willing to take part in the study, and 108 driver/contact pairs completed both the baseline and Year 2 interviews. A minimum of two data points were needed to examine changes in life satisfaction over time. Because the proportion of participants who stopped driving over the 2-year time span was relatively modest, and those who stopped did so at different times over the 2 years of the study, analyses in this paper include only data from the baseline and 24-month (end of Year 2) interviews. Sample sizes did not allow analyses of data from any of the interim sessions. Some data from both the drivers and their contact were used in each set of analyses. For example, both the drivers’ visual acuity and the contact’s provision of rides to the driver were included in the analyses of changes in life satisfaction for both the driver and the social contact. Therefore, a complete set of data was needed for each driver/contact pair. In addition, data points for specific variables of interest (e.g., health ratings, use of public transit, etc.) were unavailable for an additional 17 drivers and contacts. The sample size in the final hierarchical regression analyses included 91 driver/contact pairs. Contacts included spouses (48%), family members (25%; for example, adult children, siblings, nieces, and nephews), and friends (27%). The majority of participants (76.4%) lived in residences that were characterized as suburban or rural. At the end of Year 2, the driving status of older adults with vision loss was assessed with 21% of the sample reporting that they were no longer driving.
The goal of the current research was to examine the role of cessation in predicting changes in life satisfaction in both drivers and their social contact and to explore to what extent drivers’ use of public transit pre-cessation moderated those effects. For that reason, most of the variables except for life satisfaction, health and driving status described in the analyses below were taken from the baseline interviews only. The sociodemographic (i.e., age, gender, and SES) and health variables were selected as covariates in the model on the basis of past research which found each of these variables to be associated with the effect of cessation on well-being (e.g., Marottoli et al., 2000). Variables measuring visual functioning, driving frequency, and relationship between the contact and the driver were included in the model to rule them out as potential confounds in the analyses.
Measures
Demographic, relationship, and health variables
At baseline, older drivers and their social contacts were asked to report their age in years, gender (female = 1), income adequacy (1 = can’t make ends meet to 4 = money is not a problem), and years of education (1 = less than seventh grade to 7 = graduate school). Income adequacy and level of education were transformed into z-scores and combined to form a proxy measure of SES. Drivers and their social contacts were also each asked to rate the quality of the driver’s health (1 = very poor to 5 = excellent) at both the baseline and the Year 2 interview. Ratings of the driver’s health from both the baseline and Year 2 interviews were included as covariates in the analyses as an index of change in drivers’ self-reported health over time and contacts’ perceptions of the drivers’ health over time. Social contacts were additionally asked to identify the nature of their relationship with the driver, whether or not they lived in the same household with the driver (1 = yes, 0 = no) and whether they ever provided rides to the driver (1 = yes, 0 = no).
Measures of visual functioning
Objective measures of visual acuity and field of view were used to assess drivers’ level of visual functioning at baseline. Impairment of these types of visual functioning has been identified by previous research as associated with a greater likelihood of adverse driving events (e.g., accidents or near accidents; Johnson & Keltner, 1983; Marottoli et al., 1998; McGwin et al., 2000). Freeman, Munoz, Turano, and West (2005) also found measures of these types of visual impairment to be associated with driving cessation among older adults. The goal of this research was to examine gross functional impairment that may affect driving ability, and not necessarily to measure absolute visual capacity. Participants were therefore asked to wear their corrective lenses during testing. Results of both tests were log-transformed for the analyses reported below.
Binocular visual acuity was measured using the Goodlite Eye Chart. The Goodlite Eye Chart is small, lightweight, portable, and includes its own source of standardized light. Drivers’ binocular acuity was measured with a backlit LD-10 translucent acuity chart, using the Sloan letter set (National Academy of Sciences, 1980). The chart was administered at 1.5 m or 0.75 m (if participants were unable to read the letters at 1.5 m), or 0.375 m (if participants were unable to read the chart at 0.75 m). Participants were asked to read each string of letters with testing being discontinued if participants read three or more letters incorrectly. Acuity was calculated in logmar scores after adjusting for the testing distance. Higher scores indicate poorer visual acuity.
Visual field was measured using a Bernel Hand-Held Disc Perimeter. Participants were asked to fixate on a particular point along a hemispherical black background. A white target fixed to a long (23 cm) wand was then moved along the perimeter of the arc. The target was then moved from the extreme edges toward the fixation point in the center. Participants were instructed to report when they were able to see the target. This test was repeated 3 times. This test allowed us to test the outer horizontal limits of participants’ field of vision.
Public transportation
At baseline, older adult drivers were asked to report the frequency with which they used public buses, subways, and paratransit on a 4-point scale with response options that included never (1), less than once per month (2), at least once a month (3), and at least once a week (4). For the analyses below, drivers’ use of public transportation at baseline was averaged across the three types of public transportation.
Driving behaviors
All of the participants self-identified themselves at baseline as being drivers. Participants were asked to report how frequently they drove on a scale from 1 (once a month or less) to 5 (daily). At the end of Year 2, participants were asked to identify whether they were currently a driver or an ex-driver.
Life satisfaction
Social contacts and drivers were asked to rate their life satisfaction on the five item Satisfaction With Life Scale (SWLS; Diener, Emmons, Larsen, & Griffin, 1985) at both the baseline and at the end of Year 2. The SWLS is a measure of global life satisfaction that has been found to have good internal consistency and construct validity (Diener et al., 1985; Pavot & Diener, 1993). Researchers using the SWLS in clinical settings have found that the measure is sufficiently sensitive to identify changes in well-being over the course of treatment (Pavot & Diener, 1993). In this study, Cronbach’s alpha indicated high reliability for the SWLS for both the drivers and the contacts at each of the measurement points (alphas ranged between .81 and .84).
Plan of Analysis
Changes in life satisfaction at Year 2 were assessed using hierarchical regression for the driver and the social contact separately. Step 1 of the analysis included demographic characteristics, such as the age, gender, and SES of the respondent. Step 1 also included respondents’ life satisfaction at baseline, and health at both baseline and end of Year 2. In Step 2, contact-specific information was added, including whether or not the contact lived with the participant driver and whether they ever provided the participant driver with rides. Driver-specific variables, including measures of the driver’s degree of visual field, level of visual acuity, driving frequency, and public transportation use, were added in Step 3. Driver status at the end of Year 2 (driver or ex-driver) was also included in Step 3. Finally, in Step 4, an interaction term for driver status by use of public transportation was included in the model.
Controlling for life satisfaction at baseline allowed us to examine changes in the criterion variable associated with changes in driver status (Cronbach & Furby, 1970; Holahan & Moos, 1981). A significant result for driving status at the end of Year 2 would suggest that a change in driving status over the 2-year time span (from a driver at baseline to a nondriver at Year 2) was associated with a change over time in life satisfaction. A significant interaction between driver status and use of public transit would suggest that the effect of driver status on changes in life satisfaction over time was moderated by participant drivers’ use of public transit at baseline.
Hayes’ PROCESS macro for SPSS (Hayes, 2013) was used to probe all significant interactions. PROCESS allows the simple slopes for the association of driving status with each criterion variable (life satisfaction of drivers and social contact) to be examined at low (M − 1 SD) and high (M + 1 SD) levels of use of public transportation.
Results
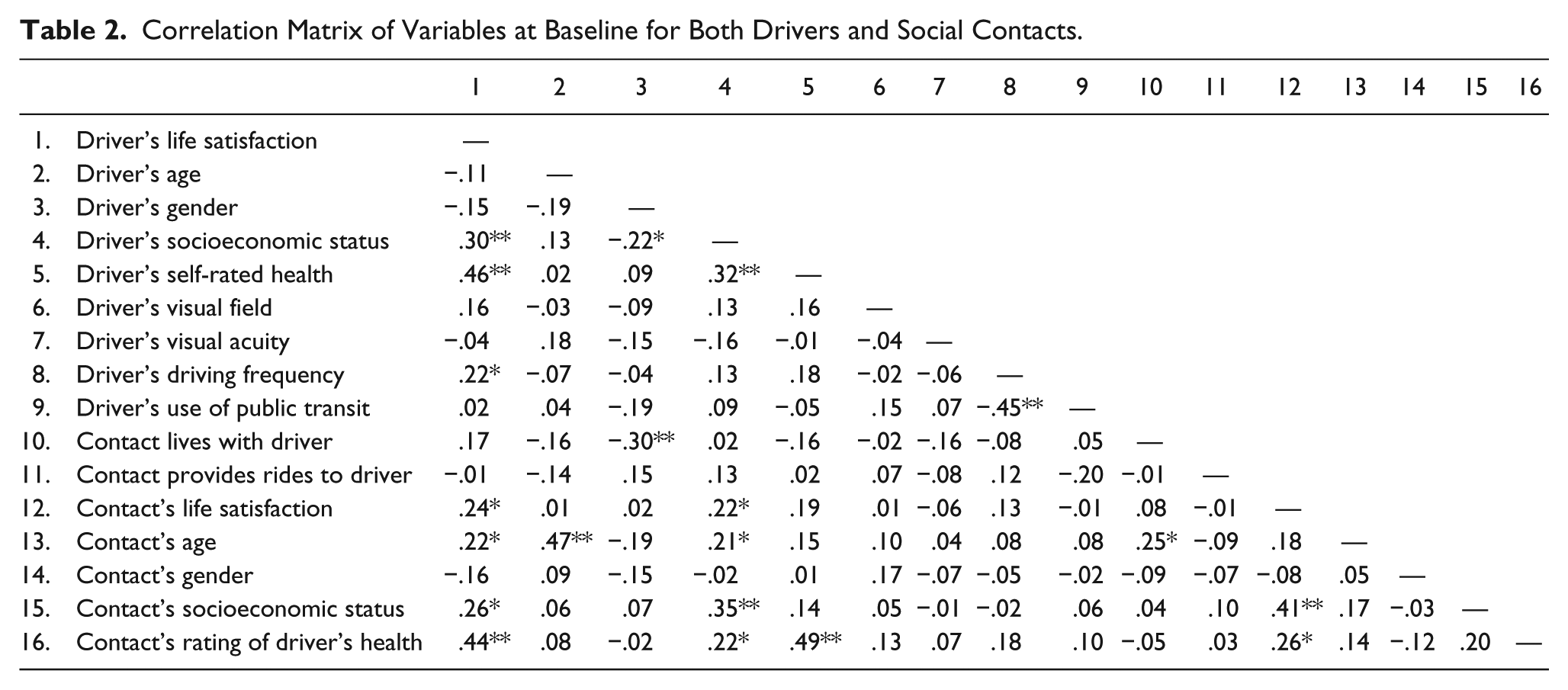
Descriptive data are reported for both participants and social contacts for all of the variables in the study (see Table 1). t-tests and chi-square analyses were used to examine whether the 91 participants and social contacts for whom we had complete data differed on any variable from the 290 participants who were omitted because of incomplete data. The sample of participants included in the current analyses (M = 137.23, SD = 21.00) scored marginally higher on the measure of visual field than did those who were omitted (M = 131.36, SD = 27.19), t(373) = −1.89, p = .06. No other differences approached significance. Correlations were also computed between all driver and social contact variables at baseline (see Table 2).
Descriptive Statistics for Driver and Contact Variables (N = 91).
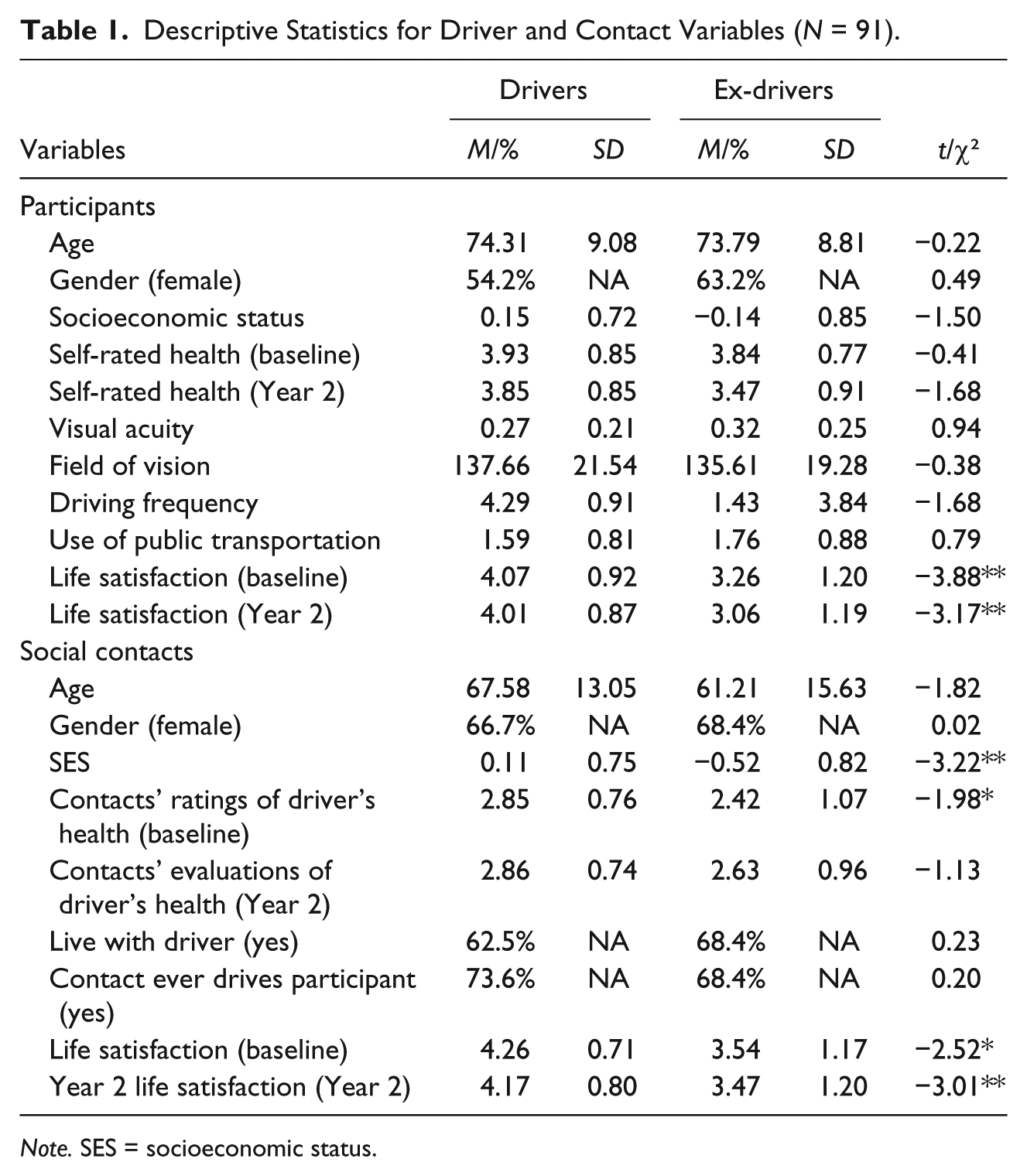
Note. SES = socioeconomic status.
Correlation Matrix of Variables at Baseline for Both Drivers and Social Contacts.
Drivers’ own driving status (driver vs. ex-driver) did not predict changes in their life satisfaction across time (Table 3). Only baseline life satisfaction, whether the contact ever gave rides to the participant, and degree of visual field predicted life satisfaction at Year 2. Drivers with higher life satisfaction at baseline reported higher life satisfaction at Year 2. Drivers who demonstrated a better field of vision reported more satisfaction over time. Drivers who received rides from their social contact at baseline reported lower life satisfaction at the second time point. The interaction between the use of public transportation and driving status was nonsignificant.
Unstandardized Coefficients for Regression Models Showing the Interaction Between Driving Status and the Use of Public Transportation on Life Satisfaction for Participants/Drivers (N = 91).
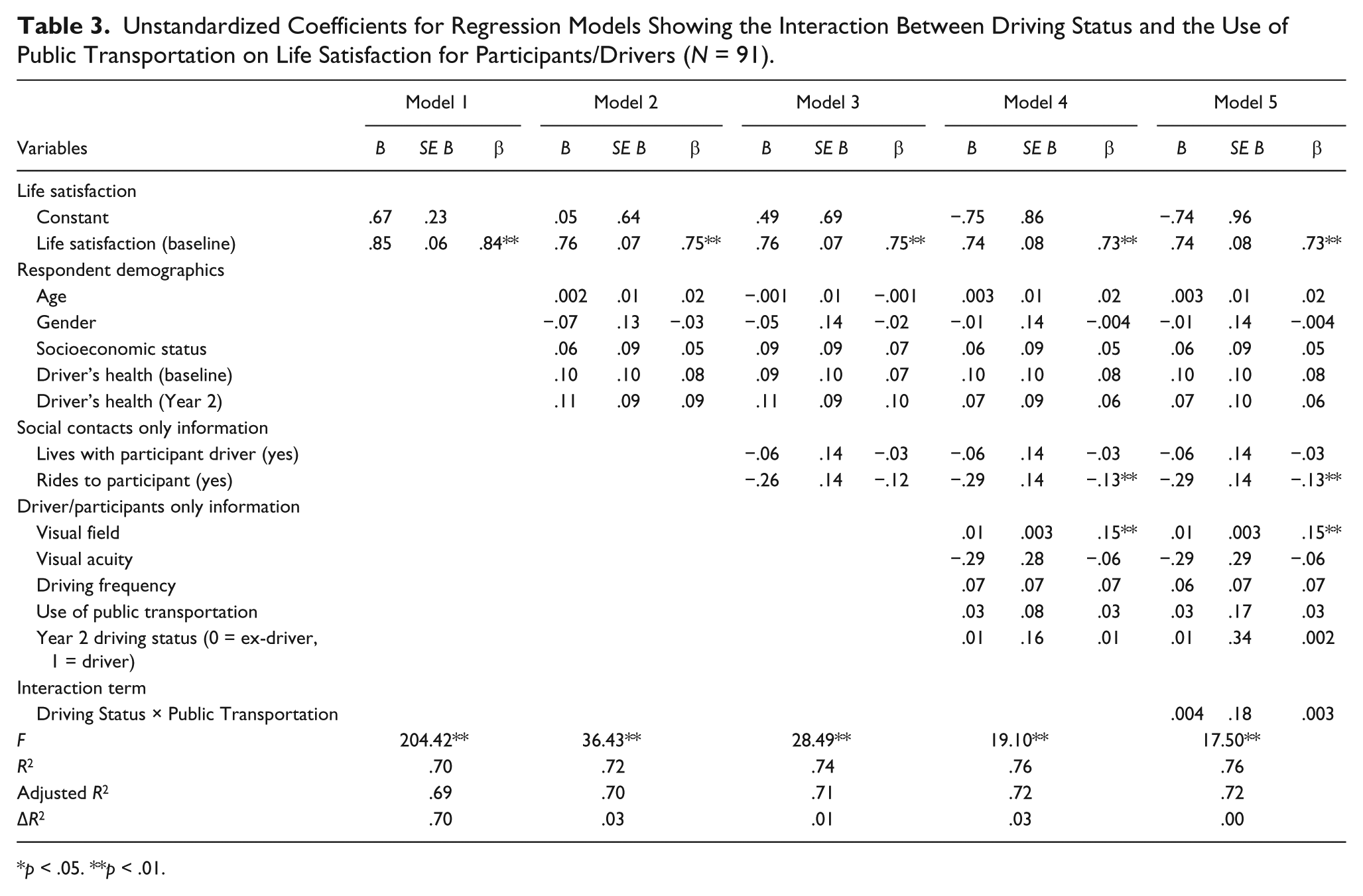
p < .05. **p < .01.
Social contacts’ baseline life satisfaction was similarly associated with Year 2 life satisfaction (Table 4). Social contacts’ life satisfaction was also predicted by SES and their ratings of their own health at Year 2. Social contacts with higher SES at baseline and better health at Year 2 reported higher levels of life satisfaction at Year 2. More importantly, among social contacts, changes in life satisfaction were predicted by driving cessation of the primary respondent. Social contacts of primary respondents who stopped driving over the 2-year study reported lower life satisfaction compared with those whose primary respondent continued to drive. The interaction between driving cessation and primary respondents’ use of public transportation at baseline was also significant. Among the social contacts of primary respondents who made little use of public transportation at baseline (approximately 1 SD below the mean), the friends and family members of ex-drivers reported lower levels of life satisfaction than did the social partners of continuing drivers (b = .57, SE = .21, p < .01). Among the social partners of primary respondents who made greater use of public transportation at baseline (1 SD above the mean), there was little difference 2 years later in the life satisfaction of the social contacts of ex-drivers and continuing drivers (b = –.23, SE = .30, p = ns; see Figure 1).
Unstandardized Coefficients for Regression Models Showing the Interaction Between Driving Status and the Use of Public Transportation on Life Satisfaction for Social Contacts (N = 91).
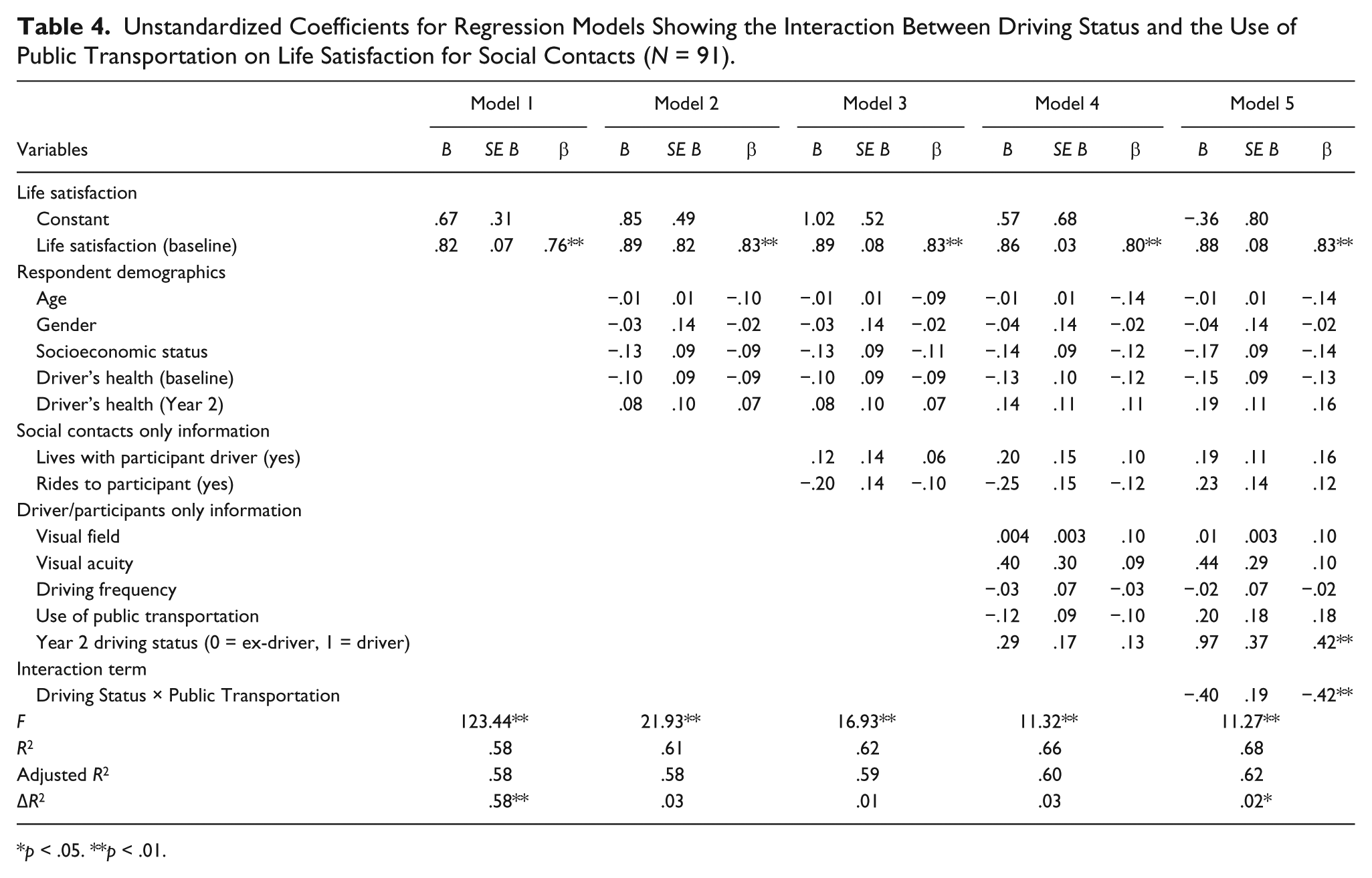
p < .05. **p < .01.
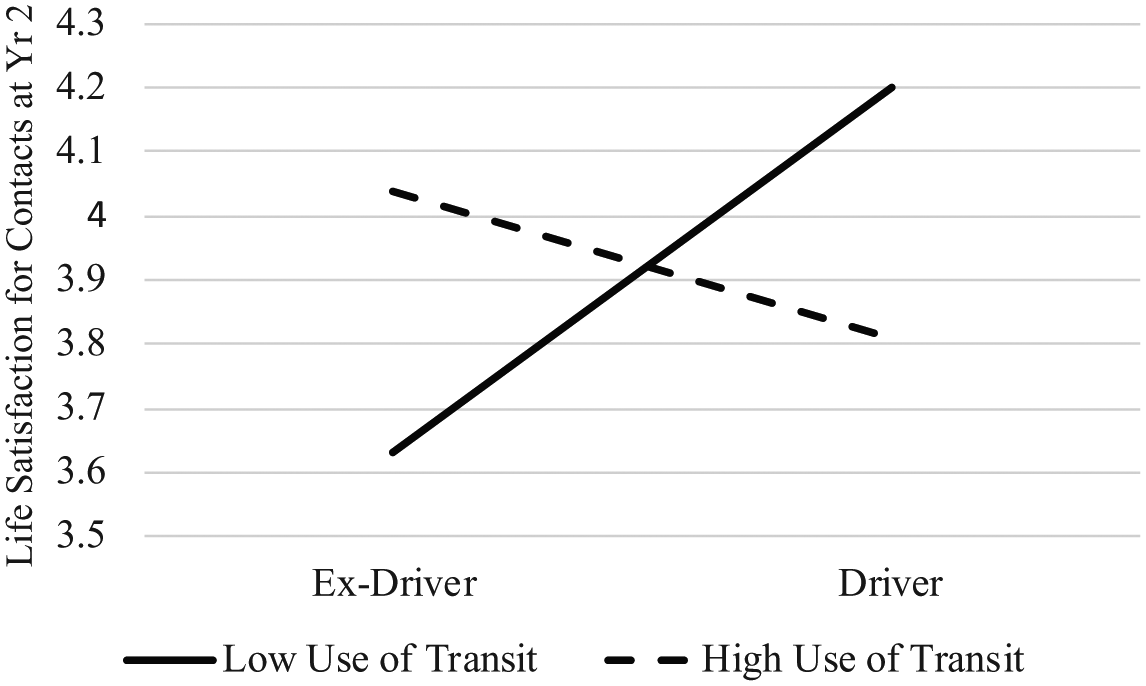
The effect of driving status by transportation use on social contacts’ life satisfaction at Year 2.
Discussion
Previous studies have examined intraindividual predictors of driving cessation, such as health, age, gender, and visual functioning (Chipman et al., 1998; Edwards et al., 2008; Freeman et al., 2005; Sims, Ahmed, Sawyer, & Allman, 2007). An extensive body of literature has already examined the consequences of driving cessation on the well-being of older adults (e.g., Curl et al., 2014; Marotolli et al., 2000; Mezuk & Rebok, 2008; Ragland et al., 2005). However, although it seems likely that when older adults stop driving their transition to being an ex-driver could also affect their family members and friends, only a handful of studies to date have examined what that effect might be. To our knowledge, our study is the first to examine the effects of driving cessation on changes in life satisfaction of both drivers and their social contacts over a 2-year period, including drivers’ use of public transit prior to driving cessation as a moderator.
Life Satisfaction Among Older Adult Drivers
Past research has found an association between driving cessation and increased symptoms of depression over time (Fonda et al., 2001; Marottoli et al., 1997; Ragland et al., 2005). However, cessation was not associated with changes in life satisfaction among older adult drivers in our study. Why did cessation have so little impact on changes in older adult drivers’ life satisfaction at Year 2?
One possibility is that life satisfaction is a relatively temporally stable indicator of well-being. Mood indicators such as depression may be more sensitive to fluctuations in emotions associated with life events such as driving cessation (Pavot & Diener, 1993). Assessments of life satisfaction, in contrast, may be less affected by shifts in a single domain of quality of life such as driving, particularly if the process of driving cessation occurred gradually or at an earlier point within the 2-year time span. Huisingh et al. (2017) found that the life space scores of older adults who stopped driving over the 6-year time span were more restricted compared to those who continued to drive. Life space scores did not, however, abruptly decline with the driving cessation event, but rather shifted gradually over time. Driving cessation is typically not an abrupt transition but one which occurs gradually over time, moving from contemplation to the adoption and maintenance of driving restrictions prior to cessation (Kowalski, Jeznach, & Tuokko, 2014; Tuokko et al., 2006). A gradual and voluntary shift from driver to nondriver may be associated with fewer perceived negative consequences (Kowalski et al., 2014) than an abrupt or nonvoluntary cessation. This gradual transition from driver to nondriver may be particularly characteristic of drivers with diseases that cause gradual declines in visual functioning over time (Spiegel, Rubin & Steverink, 2017).
Participants for this study were recruited based on the criterion that they had been experiencing some degree of vision loss. Analyses revealed that vision loss, specifically loss of degree of visual field, was associated with declines in life satisfaction over time. This raises the possibility that, for the participants in this study, the process of driving cessation was intrinsically linked to loss of vision. Cessation may have had little impact on life satisfaction because for the participants who were experiencing significant age-related changes in visual functioning, cessation represented just one more adjustment as part of a larger transition. It is possible that cessation may have a larger impact on the life satisfaction of older adults who stopped driving for reasons other than age-related visual functioning, such as cognitive decline, or declines in physical mobility that may either represent a sudden transition or limit the accessibility of other transportation options.
A third possibility is that lower life satisfaction may be a better predictor than an outcome of cessation among older adult drivers. As noted above, Harrison and Ragland (2003) cautioned not to interpret the negative association between driving cessation and life satisfaction found in some studies as reflecting a causal effect of cessation. This raises the specter of reverse causation. It is possible that older adults who are at a particularly low point in their lives in terms of their well-being, because of declines in visual functioning or general health, may be more likely to stop driving. The act of cessation, particularly over the long term, may not decrease their life satisfaction substantially more. This is a research question that warrants further investigation.
A somewhat surprising result of these analyses was the finding that the provision of rides by family members and friends at baseline was negatively associated with life satisfaction among drivers and ex-drivers at the end of Year 2. The availability of support from members of an individual’s social network is usually positively associated with well-being (Newsom & Schulz, 1996). One possible interpretation of this finding is that increased engagement of others in a driver’s social network may function as an indicator of declines in well-being. When an older driver is depending more on members of their social network for transportation even prior to cessation, it may signal that an individual is on the way to needing more help. More research is needed to understand the relationship between transportation support from social network members and well-being among older drivers.
Life Satisfaction Among Social Contacts
Although cessation was not directly related to changes in life satisfaction among the drivers, it was significantly associated with reduced life satisfaction among drivers’ family and friends. This finding is consistent with interdependence theory (Kelley & Thibaut, 1978; Rusbult & Buunk, 1993), which suggests that the outcomes of individuals and their social contacts are closely interconnected. When an individual stops driving, it has the potential to affect the outcomes of members of their social network. Spouses of older adults who stop driving may find their own social engagement activities curtailed (Curl et al., 2015). Spouses, adult children, and other family members and friends may find themselves providing more transportation and/or potentially having fewer opportunities to engage in social interactions with the former driver. This finding warrants further more in-depth exploration about the nature of the impact of cessation on different members of a driver’s social network. Measures of life satisfaction tell us only about individuals’ cognitive appraisal of their own well-being. They do not tell us the exact nature or mechanism of the effect. The effect of cessation on the life satisfaction of social contacts may also vary according to the nature of the relationship (spouse, adult child, or friend), whether the contact and the driver live in the same household, and the extent to which the social contact provides transportation support for the driver. We attempted to address these questions in this study by including items measuring living arrangements and provision of rides by the contact to the driver as covariates in the analyses, but more nuanced measures of relationship type, closeness, and social context may reveal more complex relationships between driving cessation and well-being among social contacts.
Public Transportation
There was little evidence in this study that older adult drivers’ use of public transit at baseline had any effect on their own life satisfaction regardless of whether they continued or gave up driving over the 2-year time span. Older drivers’ use of public transportation did, however, moderate the effects of cessation on the life satisfaction of their social contacts. The social contacts of ex-drivers who stated that they used buses, subways, and paratransit never or rarely reported lower levels of life satisfaction 2 years later. The friends and family members of ex-drivers who used public transportation on a more regular basis prior to cessation reported levels of life satisfaction that were similar to that of the social contacts of continuing drivers.
Infrastructure that supports independent transportation is likely to become an increasingly important aspect of urban planning, particularly with the shift in population age expected over the next few decades (Vincent & Velkoff, 2010). The utility of transportation infrastructure likely differs depending on the nature of the environment that older adults are living in (i.e., urban vs. rural, central vs. suburban). This study was conducted in and around New York City which has a well-developed transportation system. However, the majority of participants (76.4%) did not live in the heart of the city but rather lived in suburban areas. This study suggests that transportation infrastructure, where it exists and in what form it exists, has the potential to play an increasingly important role in supporting not only the transportation needs of older adults but also the well-being of their larger support networks. Further research is needed to better understand the types of transportation infrastructure that would be most effective in supporting the transportation needs of older adults who are faced with the prospect of driving cessation, as well as the members of their social networks.
In this study, older adults’ use of public transportation was measured at baseline, prior to cessation, while all participants were still driving. The finding that respondents’ use of public transportation prior to cessation affected the life satisfaction of social partners is important because it suggests that the social partners’ life satisfaction was influenced not merely by respondents’ use of trains and buses, but by their preparation for the transition from driver to nondriver. Recent research suggests that drivers’ readiness to engage in mobility transition may be an important determinant in the maintenance of well-being (Berg-Weger, Meuser, & Stowe, 2013). This study suggests that the same pattern may also be true for the well-being of older drivers’ social partners.
Limitations and Conclusion
Some limitations of our study deserve mention. Only a minority (N = 19) of older adults stopped driving over the course of the study. The percentage (21%) of participants who stopped driving in this study was similar to other studies that have examined cessation among older drivers with age-related visual impairments (e.g., 25% cessation in Sengupta et al., 2014). Nevertheless, the small number of participants who stopped driving does limit the generalizability of the findings and may be one reason for the lack of a significant effect of driving cessation and use of public transportation on the well-being of older drivers. These findings should be interpreted with some caution given the relative low power in the study.
The modest sample size also limited the kinds of analyses that could be done with the available data. For example, in the current analyses, we found it necessary to examine cessation across the entire 2-year time span. A larger sample size would allow more time-sensitive analyses of how cessation affects changes in patterns of life satisfaction over multiple time points. It would also be beneficial to include outcomes more sensitive to short time changes such as positive and negative affect and to examine changes in affect both closer and farther away in time from the point of driving cessation. The inclusion of more detailed measures of use of transportation options would provide a more detailed and nuanced picture of how transportation infrastructure availability, accessibility, and use in different environments supports the well-being of older drivers, their family members and friends.
Nevertheless, our study adds to the literature by providing evidence that cessation can affect the well-being of drivers’ social contacts, and that public transportation if and when it is available has the potential to moderate the impact of cessation on the well-being of older drivers’ family members and friends. Our findings support the key notion of interdependence theory that both the goals and outcomes of close social contacts are interconnected, and in doing so suggest that both research examining the correlates and outcomes of driving cessation, as well as health care professionals working with older drivers should closely consider the social context and environmental infrastructure in which the transition from driver to ex-driver might occur.
Footnotes
Institutional Review Board Approval
The Driving Transitions and Mental Health in Disabled Elders study (RO1AG020579) was granted Institutional Review Board (IRB) approval from Jewish Home Lifecare (now The New Jewish Home). No protocol number was associated with the file, but documentation is available upon request. IRB approval was also provided by CSULB to Emily Schryer for secondary data analyses (#891383-1).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Driving Transitions and Mental Health in Disabled Elders study upon which the current analyses are based was supported by a National Institute on Aging (NIA) grant awarded to Amy Horowitz (principal investigator), Kathrin Boerner and Joann Reinhardt (co-investigators). Emily Schryer’s work on this project was supported by a postdoctoral fellowship from the Social Sciences and Humanities Research Council of Canada (SSHRC).