
Abstract
The more than 20 million U.S. veterans have a history of physical activity engagement but face increasing disability as they age. Falls are common among older adults, but there is little evidence on veterans’ fall risk. We conducted a retrospective cohort study using 48,643 observations from 14,831 older (≥65 years) Americans from the 2006–2014 waves of the Health and Retirement Study. Veterans reported more noninjurious falls (26.6% vs. 24.0%, p < .002), but fewer fall-related injuries (8.9% vs. 12.3%, p < .001) than nonveterans. In adjusted analyses, for each 5-year increase in age, the odds of a noninjurious fall were greater for veterans (odds ratio [OR] = 1.05, 95% confidence interval [CI] = [1.01, 1.10]) and, among those with regular physical activity, the odds were lower for veterans compared with nonveterans (OR = 0.89; 95% CI = [0.81, 0.99]). For veterans, physical activity engagement may prove a particularly effective mechanism for reducing the aging-related risks associated with falls and fall injuries.
Introduction
Numbering over 20 million, U.S. veterans of the armed services are older and in poorer health but more physically active than other Americans (Hoerster et al., 2012; Littman et al., 2009; Wu & Lewis, 2015). Nearly half of the veteran population are adults ages 65 years and older compared with 8% of the civilian population (Hoerster et al., 2012). Given strong links between aging-related disability and physical engagement with falls (Deandrea et al., 2010; Florence et al., 2018; Sherrington et al., 2017), veterans may have a unique profile for exposure to falls, a growing threat to older adults’ well-being and independence (Hartholt et al., 2019).
Although risk factors for falls are generally well understood, the interactions of such risks for the veterans’ population are poorly understood. On one hand, because of a high prevalence of disability, veterans may be more greatly exposed to falls than other individuals. Research on disablement suggests that weakened functional status is the strongest predictor of falls (Verbrugge & Jette, 1994), and veterans may therefore have greater function-related fall risk. On the other hand, due to their history of service that includes demanding physical activity and higher lifetime rates of activity (Littman et al., 2009; Sparling et al., 2015), veterans may be at lower risk for falls, after accounting for differences in functional status. The literature is generally indicative of a protective (Finnegan et al., 2019; Sherrington et al., 2017) effect of physical activity on falls (Orwoll et al., 2018), and veterans may be more active when they do engage in physical activity. Given that disability may increase while the safety of physical activity may decrease over time (Orwoll et al., 2018; Tinetti & Kumar, 2010), veterans’ fall risk profiles may also change as veterans age.
There is an extremely limited literature on veterans and falls (Luther et al., 2005; Soncrant et al., 2018, 2020; Zubkoff et al., 2016, 2018) that has primarily focused on service-connected veterans, an older group with more disabilities than the general veteran population (Quigley et al., 2006). These studies have relied on small samples of service-connected, hospitalized patients and have not provided comparisons with the nonveteran population. We build on this limited work by assessing, for veterans and nonveterans, the overall prevalence of falls as well as whether fall risk is influenced by respondents’ physical activity levels. Specifically, the aim of this study was to compare risks of noninjurious falls (NIFs) and fall-related injuries (FRIs) for the broader (service-connected and nonconnected) veteran and nonveteran populations, including whether risks differed according by physical activity status and across age categories. With this approach, our findings will provide clinicians with novel insights into falls and fall risk factors for a large but previously unexplored older adult population. Given the disabilities that are strongly associated with veteran status, we hypothesized a priori that veterans would have higher overall risk for NIFs and FRIs than nonveterans, especially at older ages when relative disparities in functional status might expand between these groups. We also hypothesized a priori that, after adjusting for health and functional status, veterans would be more protected from falls due to physical activity given their service-related histories of physical fitness that may result in greater intensity and efficacy of physical activities (Littman et al., 2009).
Research Design
Data Sources and Study Population
This was a retrospective secondary data analysis using national survey data. Prior work examining veterans has typically used claims data for veterans treated by the Veterans Healthcare Administration (VHA), a population (~6 million) representing just 30% of all veterans who use VHA care annually (National Center for Veterans Analysis and Statistics, 2017). These veterans, often eligible for the health benefit from the U.S. Department of Veterans Affairs (VA) through a service-connected disability, are a unique subset of the overall veterans’ population (approximately 40% of all veterans are VA-enrolled; Congressional Research Service, 2014). Reliance on VA claims means that studies on broader veterans’ population (for whom claims in the VA system or Medicare data are not typically available) are limited. To address this gap, we assessed patient-level information from the 2006–2014 waves of the biennial Health and Retirement Study (HRS). The HRS is a nationally representative survey with sociodemographic, economic, health, functional, and social status, insurance, and veteran status information for older adults. Eligible HRS respondents are interviewed approximately each 2 years by telephone.
Our initial sample included 54,845 observations for HRS respondents. We excluded observations without complete information and those that were not connected to an adjacent survey wave (to include lagged variables, which are described below). For instance, we excluded a 2010 observation if the same respondent did not also have survey information from either of 2008 or 2012. This left us with a final analytic data set of 48,643 observations, including both veteran and nonveteran respondents ages 65 years and older, representing 14,831 unique respondents. This resulted in a pooled data set in which respondents could contribute more than one observation if they were involved in multiple HRS survey waves—for instance, for an individual aged 74 and 76 years in two adjacent surveys. This approach makes maximal use of the available data in the surveys, increasing sample size by employing these person-waves (Margolis & Verdery, 2017).
We constructed two study cohorts using HRS data—one for veterans and one for nonveterans. To identify individuals with veteran status, we used responses to the question, “Have you ever served in the active military of the United States?” as has been done previously (Gould et al., 2015; Taylor et al., 2015). We also identified physical activity levels using responses to two HRS questions about how often respondents take part in each of moderate and vigorous physical activities. Using these responses, we constructed a dichotomous variable indicating whether respondents reported having regularly engaged (once per week or more) in either of moderate or vigorous physical activity. Moderate physical activities included gardening, walking at a moderate pace, stretching exercises, and home repairs; vigorous physical activity included jogging, swimming, tennis, and heavy housework.
Primary Outcomes
Self-reported NIFs and FRIs were the primary outcomes examined. Specifically, respondents were asked whether or not, in the time since their previous interview (or in the prior 2 years, for those respondents interviewing for the first time with the HRS), they had fallen. Those responding “Yes” were considered to have had a fall. Respondents with FRIs were identified by identifying those individuals who answered “Yes” when asked whether, in that fall, they had injured themselves seriously enough to need medical attention. Respondents answering “No” to having required medical attention were coded as having had an NIF.
Other Variables
The Disablement Process model suggests that falls can result from a pathway reflecting chronic conditions, functional limitations, and other impairments (Verbrugge & Jette, 1994). In addition, access to care (e.g., co-payments for medical treatment for FRIs) and respondents’ propensity to self-report an NIF or FRI might influence observed fall patterns. Because of potential differences in these disablement process, access to care, and propensity for self-report factors among veterans and nonveterans, we included representative characteristics that could proxy for these factors in risk-adjusted models. Demographic measures (age measured in 5-year bands, sex, race/ethnicity, educational level, and marital status that are known to predict FRI reporting accuracy; Hoffman et al., 2018) were obtained from the HRS, as were economic indicators (household income and wealth, Medicaid status that could reflect access to care, such as co-payments for medical treatment), and health and functional status indicators that could confound observed relationships between veteran status, physical activity, and fall risk (Deandrea et al., 2010; Schwartz et al., 2008; Sennerby et al., 2009; Tinetti et al., 1995). Health and functional status indicators included activities of daily living (ADL, a count of 0–5 limitations), instrumental ADL (IADL, a count of 0–3 limitations), counts of chronic conditions and depressive symptoms, and self-reported health (with dummy variables for very good or excellent health and for good health, with a reference category of fair or poor health). All time-varying variables (e.g., age, income, ADL) were lagged by one survey wave (~2 years) to account for potential reverse causality. To create lagged variables, we measured predictor variables in the wave prior to (wave t − 1) the one in which the fall outcome was measured (wave t), before pooling all waves of data. We did not use lagged data from earlier survey waves (e.g., wave t − 2) if information from the prior wave was missing.
Statistical Analysis
We first compared respondent characteristics, including demographic, health and functional status, physical activity status, and fall outcomes by veteran status, using t tests and chi-square tests for continuous and categorical data and two-tailed significance cut-offs at p < .05. Next, we examined each of our study questions using multivariable logistic regression models with separate sets of models for each of the two outcome variables, NIFs and FRIs. To account for potential loss of precision in model estimates due to repeated observations of individuals in multiple surveys, we used cluster-robust standard errors in all models. In sensitivity checks, we reestimated models using generalized estimating equations (GEEs) with independent working correlation structures (Heagerty & Comstock, 2013). Model standard errors and p values were nearly identical when using GEEs; therefore, we report results from logistic regression models.
First, we assessed whether the odds of falling (NIFs and FRIs) varied according to veteran status. Next, in the second set of models, we explored the role of age in the veterans–falls relationship, by introducing an interaction term, Age × Veteran, into the original model. In a third set of models, we explored the role of physical activity in the veterans–falls relationship, by introducing a separate interaction term, Activity Level × Veteran, into the original model. Finally, we introduced a triple interaction, Age × Activity Level × Veteran, to the original model to assess whether the veterans–falls association varied simultaneously by age and physical activity levels.
To facilitate interpretation of model results, given the difficulty in interpreting interaction terms in logistic regression models (Norton et al., 2018), we used model estimates to compute predicted probabilities (or, “predicted risks”) using Stata’s postestimation margins command. These are probabilities of the outcome for each category of the exposure (veteran status) while averaging over the remaining covariates. For instance, for the second set of models examining fall risk by veteran status and age, we allowed the predictions to vary across ages 65 to 90 years, in 5-year increments (e.g., 30% vs. 31% risk of a fall for a veteran compared with a nonveteran at age 65 years). Finally, given that 97% of veterans were male, and men were less likely than women to have an FRI (8.4% vs. 13.5%), we ran sensitivity analyses where we included interaction terms between the predictors of interest and a male dummy variable as well ran stratified models in which we only examined male respondents. In an additional sensitivity analysis, we used an alternative categorization of regular physical activity, indicated by more than once per week (as opposed to at least weekly) of moderate or vigorous physical activity.
This study was determined to be not regulated by the University of Michigan Institutional Review Board.
Results
Unadjusted—Sociodemographics
We identified 11,841 (24.3%) veteran and 36,710 (75.7%) nonveteran observations. Substantial sociodemographic and health differences were observed (Table 1), including sex (97.4% of veterans were men, compared with 22.6% of nonveterans, p < .001). Veterans had higher education levels (28% vs. 18% with ≥college degrees, p < .001) and were more often married (78.2% vs. 56.3%, p < .001) and of non-Hispanic White race/ethnicity (85.9% vs. 74.0%, p < .001). Veterans reported better health (42.4% vs. 38.2% in very good/excellent health, p < .001), but more M (SD) chronic conditions, 1.7 (1.2) vs. 1.5 (1.1), p < .001.
Descriptive Statistics of Older Adults (≥65 Years), by Veteran Status, 2006–2014 (N = 48,643).
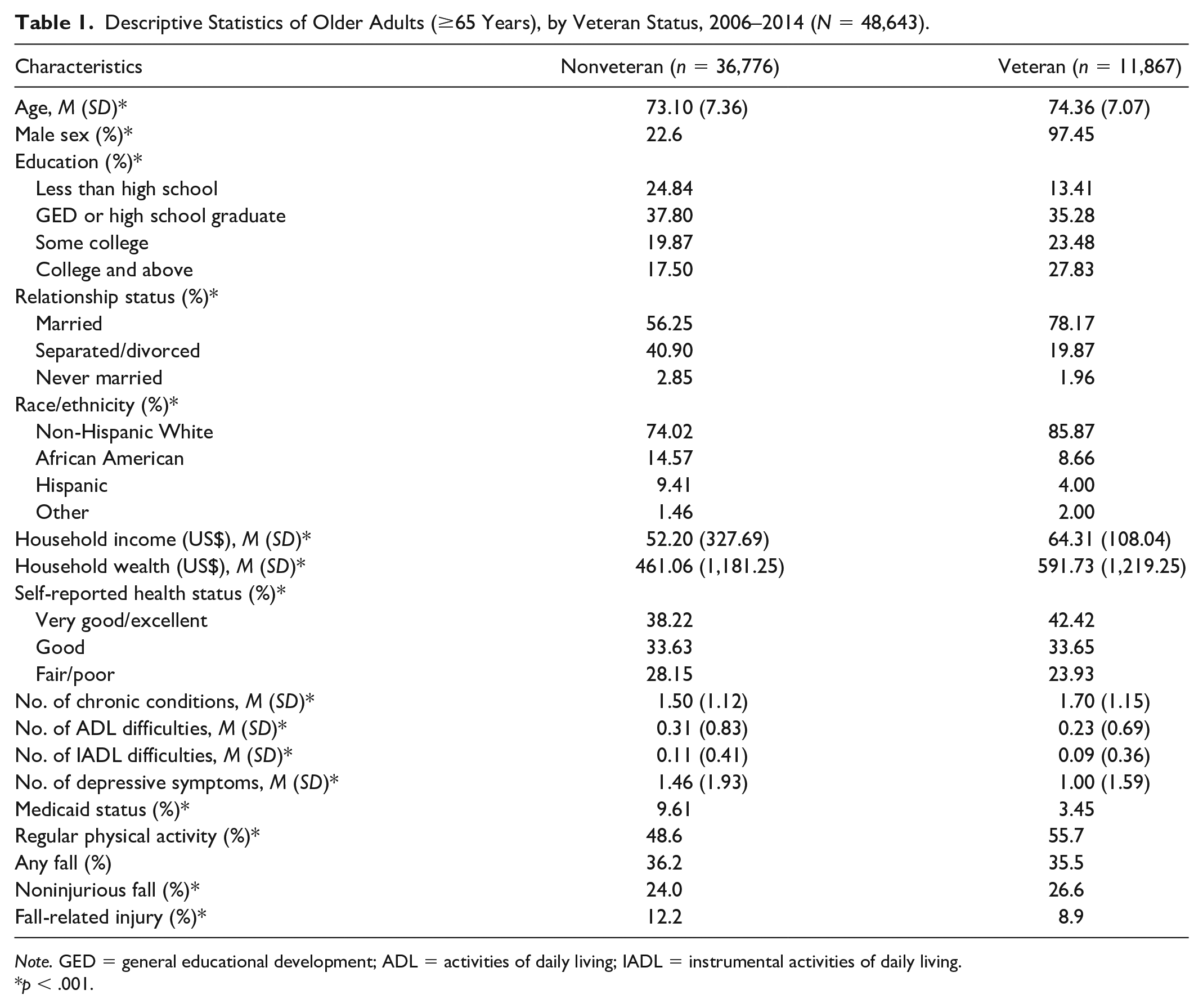
Note. GED = general educational development; ADL = activities of daily living; IADL = instrumental activities of daily living.
p < .001.
Unadjusted—Physical Activity and Falls
As shown in Table 1, compared with nonveterans, veterans were more regularly physically active overall (55.7% vs. 48.6%, p<.001) as well as across each of the three age categories: 64.3% vs. 56.0% in the 65 to 74 (p < .001), 59.3% vs. 50.6% in the 75 to 84 (p < .001), and 50.3% vs. 38.5% in the ≥85 (p < .001) age group (Figure 1).
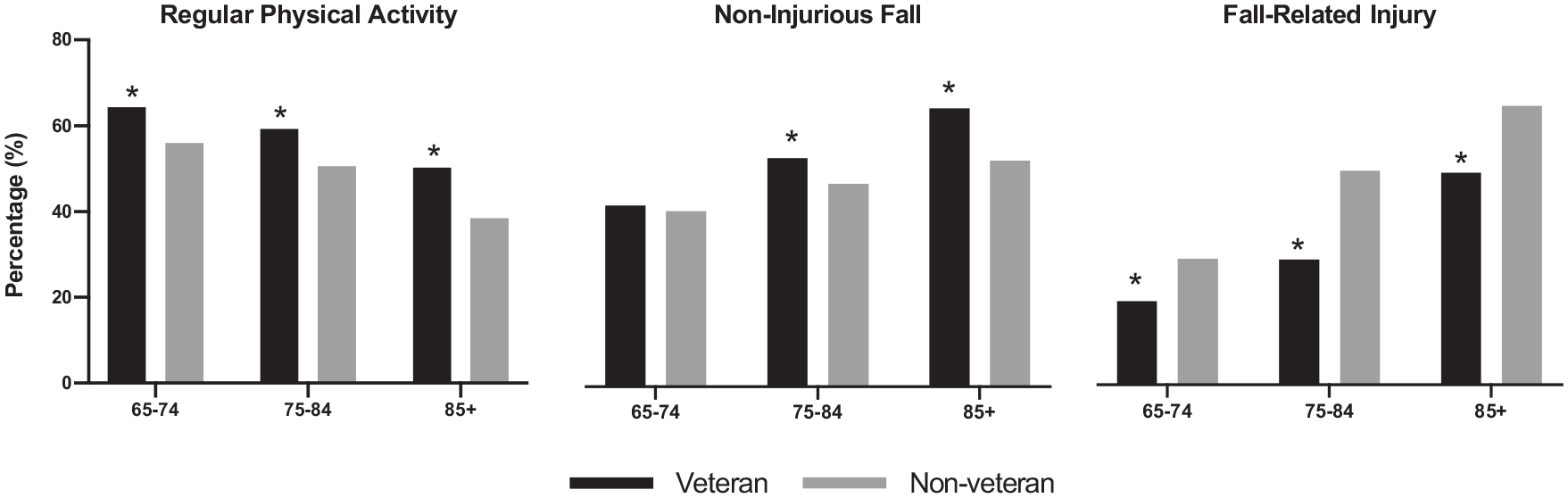
Unadjusted percentages of older adults (≥65 years) engaging in regular physical activity and reporting noninjurious falls and fall-related injury, by age, 2006–2014.
In unadjusted comparisons, no overall differences in falls were observed (36.2% nonveterans vs. 35.5% veterans, p = .13; Table 1). However, as shown in Figure 1, there were differences according to type of fall. Veterans reported more NIFs (26.6% vs. 24.0%, p < .002), but fewer FRIs (8.9% vs. 12.3%, p < .001) overall (Figure 1). These patterns were consistent across age groups. Veterans had more NIFs in the 75 to 84 (29.3% vs. 26.0%, p < .001) and ≥85 (35.7% vs. 29.0%, p < .001) age groups. They had fewer FRIs in each of the 65 to 74 (6.7% vs. 10.1%, p < .001), 75 to 84 (10.1% vs. 14.4%, p < .001) and ≥85 (17.2% vs. 22.4%, p < .001) age groups.
Adjusted Results: Veteran Status and Falls
As shown in Table 2, in multivariable analyses, after adjustment for all model covariates, no differences between veterans and nonveterans were observed overall in the odds of an NIF (odds ratio [OR] = 1.06; 95% confidence interval [CI] = [0.98, 1.16]; Model 1a) or an FRI (OR = 0.96; 95% CI = [0.86, 1.08]; Model 1b).
Odds of Self-Reported Falls, by Veteran Status, Age, and Physical Activity Level for U.S. Older Adults (≥65 Years), 2006–2014 (n = 48,643).
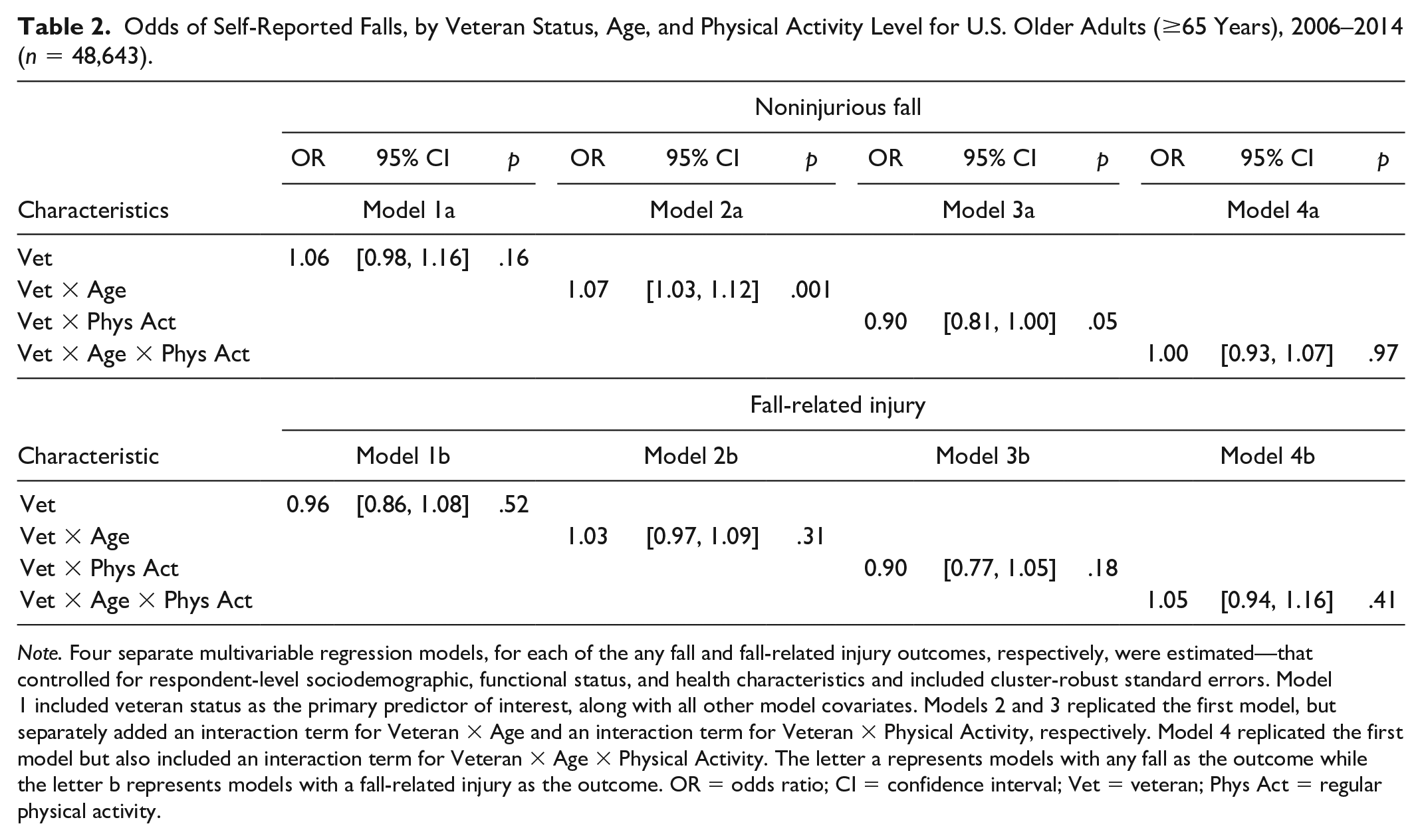
Note. Four separate multivariable regression models, for each of the any fall and fall-related injury outcomes, respectively, were estimated—that controlled for respondent-level sociodemographic, functional status, and health characteristics and included cluster-robust standard errors. Model 1 included veteran status as the primary predictor of interest, along with all other model covariates. Models 2 and 3 replicated the first model, but separately added an interaction term for Veteran × Age and an interaction term for Veteran × Physical Activity, respectively. Model 4 replicated the first model but also included an interaction term for Veteran × Age × Physical Activity. The letter a represents models with any fall as the outcome while the letter b represents models with a fall-related injury as the outcome. OR = odds ratio; CI = confidence interval; Vet = veteran; Phys Act = regular physical activity.
Adjusted Results: Age and Fall Outcomes, by Veteran Status
In multivariable analyses, for each 5-year increase in age, the odds increased more for more veterans compared with nonveterans for NIFs (OR = 1.07, 95% CI = [1.03, 1.12]) but not for FRIs (OR = 1.03, 95% CI = [0.97, 1.09]; Table 2, Models 2a, 2b).
To facilitate interpretation of these model interaction terms, we computed predicted probabilities to illustrate differences in fall risks across age groups. As shown in Figure 2, although similar at ages 65 to 69 years (21.5% vs. 22.8%), the risks of an NIF were greater for veterans compared with nonveterans at older ages (28.2% vs. 25.5% at ages 80–84; 30.7% vs. 26.4% at ages 85–89), even after controlling for a number of potential fall risk factors. This translated to ([28.2 − 25.5] / 25.5=) 11% and ([30.7 − 26.4] / 26.4=) 16% risk differences for NIFs at these oldest age groups.
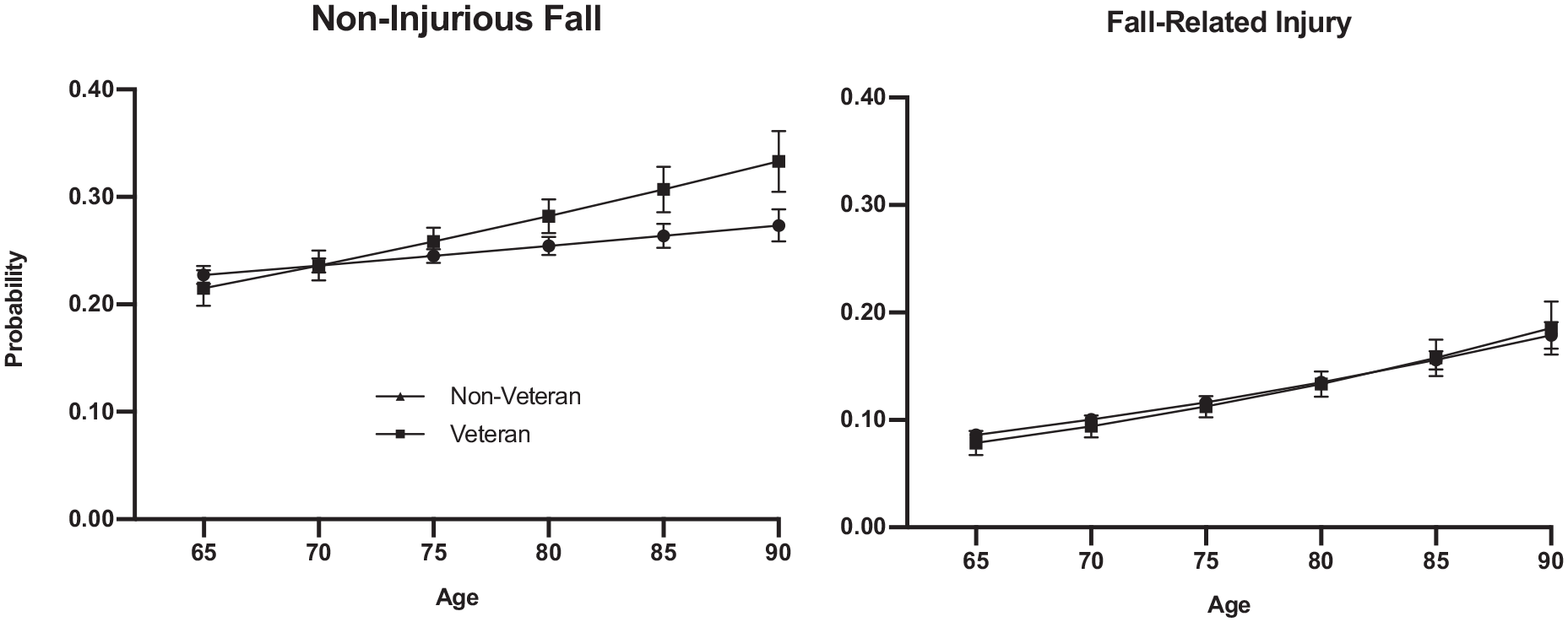
Probability of a noninjurious fall and fall-related injury by veteran status and age among older Americans, 2006–2014 Health and Retirement Study.
Adjusted Results: Physical Activity and Fall Outcomes, by Veteran Status
In multivariable analyses, when comparing by physical activity status, both veterans and nonveterans benefited from physical activity. However, there was evidence that veterans benefited more in terms of avoiding NIFs (OR = 0.90, 95% CI = [0.81, 1.00]), but not FRIs (OR = 0.90, 95% CI = [0.77, 1.05]; Table 2, Models 3a, 3b). Predicted probabilities are plotted in Figure 3, which illustrates that, among inactive respondents, the risk of an NIF was higher (28.8% vs. 26.4%) for veterans compared with nonveterans; however, among active respondents, the risk of an NIF was similar for veterans compared with nonveterans (22.9% vs. 22.6%). This translated to a marginal risk reduction in NIFs of 2.5 percentage points (p = .005) for veterans, or approximately 10% decrease in NIF risk, but no change in risk (0.5 percentage points, p = .36) for nonveterans, when engaged versus not engaged in regular physical activity.
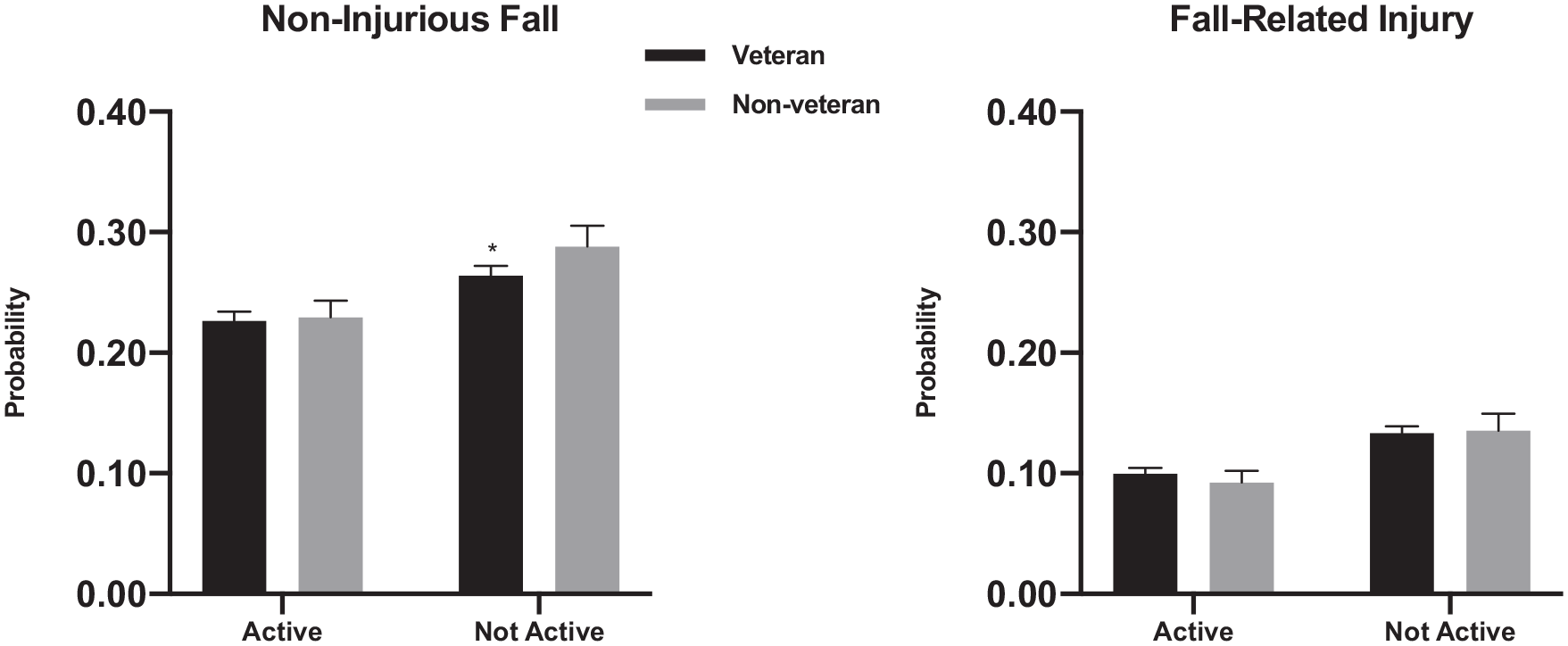
Probability of a noninjurious fall and fall-related injury by veteran status and regular physical activity status among older Americans, 2006–2014 Health and Retirement Study.
Adjusted Results: Physical Activity, Age, and Fall Outcomes, by Veteran Status
There were no significant differences in the fall–veteran relationship by age according to physical activity status (Table 2, Models 4a, 4b), after controlling for respondent characteristics.
Sensitivity Analyses
When we included interaction terms in each of the models testing for whether results varied according to male sex, the coefficients were in the direction of reduced risk of the outcomes for males versus females, but none of the terms were statistically significant (e.g., the interaction of Male × Physical Activity × Veteran’s Status for the FRI Outcome had an OR of 0.58, p = .18; results available upon request). When we ran stratified analyses only including male respondents, increasing age was no longer statistically significantly associated with increased NIFs for veterans, although the magnitude of the coefficient was similar (OR = 1.04, 95% CI = [0.98, 1.10]; Supplemental Table S1). The marginal effect of the Veteran Status × Physical Activity Term was also slightly smaller and nonsignificant. All other findings remained unchanged. We also used an alternative definition of regular physical activity (more than once per week) and found that veterans were more highly active than nonveterans (11% vs. 10%, p < .001); also, veterans no longer had greater benefits from physical activity compared with nonveterans in an adjusted model.
Discussion
In this study of veterans and fall risk, we had three novel findings. First, veterans had 11% more noninjurious but 28% fewer injurious falls than nonveterans. Put into context, were rates lowered to those of the group with lowest risk, we estimate that there would be 750,000 fewer veterans with NIFs and 1 million fewer nonveterans with FRIs each 2 years. Second, the risk of an NIF increased more with age for veterans than nonveterans, with a 10% to 15% greater relative risk for the oldest old veterans. Third, physical activity was protective against an NIF for veterans but not for nonveterans, with a ~10% lower risk for veterans engaging in at least 1 day per week of moderate or vigorous physical activity. Collectively, these results are indicative of a U.S. older veterans’ population of more active older individuals who are more exposed to less serious fall risks than other older Americans.
In one of the few prior studies on veterans and falls, Quigley et al. (2006) observed a positive correlation between fall risk scores and age for 1,810 older veterans treated in VA nursing home. The current study extends existing knowledge of veterans and falls, showing that veterans have more NIFs (especially at older ages) but fewer serious injuries from falls that are associated with morbidity, institutionalization, and even death (Burns & Kakara, 2018; Hartholt et al., 2019; Kuehn, 2018). Because falls without injuries do not present these same threats to health and independence as FRIs and given the myriad health benefits to older adults of more active lifestyles (even if slightly increasing fall risk), these veterans’ fall patterns may illustrate a worthwhile trade-off between safety and independence.
Previous researchers have shown that regular physical activity is generally effective in preventing falls (Cauley et al., 2013; Finnegan et al., 2019; Gregg et al., 2000; Quach & Burr, 2016; Sherrington et al., 2017), but have also cautioned that the risks of falling can increase for highly active individuals (Orwoll et al., 2018). A recent Cochrane systematic review (Sherrington et al., 2019) also suggests that decreases in risk of up to 25% can be obtained through physical exercise programs. This study’s finding of a 10% overall reduced risk of NIFs is consistent with this prior work, in that veterans may have more active lifestyles that incur moderate risks for minor falls while avoiding more serious injury; at the same time, as veterans age, the relative benefits for veterans compared with nonveterans of such regular activity no longer appear to overcome certain intrinsic (health and functioning-related) risks for falling.
Military service itself may provide an explanation for this unique fall profile. Physical fitness and regular fitness tests are prerequisites for active-duty members (Littman et al., 2009), and veterans may retain these health habits into later life. For this reason, the intensity and frequency of regular physical activity may be different for veterans and nonveterans, even among those who report regular engagement in such activity; this was supported in our data, as more veterans than nonveterans reported being in the most active category. Furthermore, when we compared the benefits of regular activity when only assessing highly active respondents (more than once per week of activity), we no longer observed relative fall risk benefits for veterans.
Our study has several limitations. First, self-reported data on falls can be unreliable or incomplete (Hoffman et al., 2018), resulting in conservative estimates of fall prevalence. However, unless reporting bias varies by veteran status over time, this is unlikely to substantially alter our findings. In prior work using the HRS and linked Medicare data, we observed that accuracy of self-reports of an FRI was generally higher for women compared with men and for those with more compared with fewer functional limitations or chronic conditions. However, by controlling for these factors in our models, these factors should not have influenced our risk-adjusted fall estimates. To the extent that residual risk remained after risk adjustment, it is possible that falls may have been underreported by veterans to the extent they were healthier than nonveterans (perhaps at younger ages), but relatively overreported as their health declined. However, given model risk-adjustment and the opposite directions of these gender and health-related reporting biases for the two cohorts, these reporting issues should have had a limited effect on our reported outcomes.
Second, we examined adults ages 65 years and older, so were unable to assess whether there were additional protective effects from physical activity for younger veterans. The HRS does not ask about fall history for respondents younger than age 65 years, however, and the majority of falls among Americans occur after age 65 years. Third, because men are less likely to fall (Deandrea et al., 2010) and also report higher levels of physical activity compared with women (Azevedo et al., 2007; Koeneman et al., 2011), our results could reflect the predominantly male makeup of the veterans’ cohort (Gould et al., 2015; Taylor et al., 2015). Our data were somewhat consistent with this explanation, as 56% of men compared with 47% of women in the study were regularly active, and men also reported better overall health and fewer functional limitations compared with women. Moreover, in stratified analyses only including male respondents, we no longer observed absolute risk increases for a fall with increasing age or regular physical activity, for veterans compared with nonveterans. However, absolute risk differences in stratified models are dependent on baseline fall risks (which varied for male veterans and nonveterans). To ascertain relative differences in model relationships between men and women, it is more appropriate to use interaction terms (Sun et al., 2010), as significant findings in subgroup analyses can be due to differences in subgroup sample compositions or due to chance. When we examined relative effects across subgroups by sex, by including interaction terms in each model, we did not observe significant interactions. Therefore, we did not observe strong evidence that fall risk–related relative differences between veterans and nonveterans were due to sex compositional differences in the two cohorts. Future work should more fully examine this question.
Finally, our physical activity measure was less granular that the U.S. Department of Health and Human Services’s (2008) recommended activity levels for older adults. However, a sensitivity analysis we included was able to demonstrate differences between respondents at the highest activity levels and those with more modest regular activity—suggesting that the relative benefits of regular physical activity for veterans compared with nonveterans were most likely due to veterans being more active exercisers.
These limitations notwithstanding, our observation that veterans’ fall profile represents a classic trade-off between activity and safety can inform clinical practice for veterans the broader U.S. older adult population. First, for the oldest old veterans who are on a trajectory of increased falls, many (perhaps six in 10) are unlikely to have access to care through the VA; clinicians outside the VA may be unfamiliar with the unique risks of this cohort, however, and therefore may not optimally understand how to help veterans address changing, complex trade-offs between mobility and safety as veterans age.
More broadly, the findings support the need for patient-centered support to better understand and address trade-offs associated with falls, so that older adults do not simply avoid activity due to a fear of falling (Delbaere et al., 2004; Painter et al., 2012). A patient-centered approach will recognize the heterogeneity among older individuals in terms of fall risk and physical activity levels, and provide individual-specific plans accordingly (Tuvemo Johnson et al., 2016). On one hand, greater activity levels for older adults can improve functioning and the likelihood of longer-term independence, even as it presents more opportunities for trips, stumbles, and minor falls (Growdon et al., 2017; Tinetti & Kumar, 2010); conversely, sedentary behavior can counterintuitively prevent falls (by restricting opportunities for falling), even as it harms longer-term functioning and autonomy. Therefore, aiming for no falls is not necessarily an optimal strategy, if the goal is older adult autonomy. To this end, it is concerning that half of the respondents did not regularly engage in physical activity given the protective benefits for falls and for overall older adult health (Sparling et al., 2015).
On the other hand, the nearly 10% reduced risk of falls for veterans who regularly exercised has clinical meaningfulness. According to recent work, home-based exercise programs largely tested in clinical trials have obtained ~25% fall risk reductions among older adults (Sherrington et al., 2019); that more than one third of that risk reduction was observed in the general veteran population without clinical intervention is impressive. Put another way, given the costs of widespread, community-based interventions and challenges of getting individuals to take-up exercise, it might cost billions of dollars to obtain similar results in the nonveteran population. Therefore, better understanding why veterans are able to engage in and benefit from exercise could help bolster broader prevention efforts.
Future work should further explore whether physical activity in this broader veterans’ population confers lasting health benefits in terms of functional independence beyond falls, such as differences in nursing home entry, support from informal caregivers, and acute and long-term care health care expenditures. It may be that early accumulation of health capital can explain later life habits that influence fall risk; measures of health capital and identification strategies to separate selection effects of veterans’ cohorts will be needed to pursue such analyses.
Conclusion
Collectively, veterans have a unique risk profile that appears to reflect an active population. Compared with other older adults, veterans have more minor falls but fewer injurious ones, which is consistent with a largely male, highly active, and relatively healthy population. However, veterans’ fall risk increases with age, a change in risk that is not offset by increased physical activity, suggesting that clinical efforts should help older veterans manage the complex trade-offs between maintaining independence through active lifestyles while ensuring their safety in older ages.
Supplemental Material
Supplemental_Appendix – Supplemental material for Physical Activity and Falls Among a National Cohort of Older Veterans
Supplemental material, Supplemental_Appendix for Physical Activity and Falls Among a National Cohort of Older Veterans by Dan Marciniak, Neil B. Alexander and Geoffrey J. Hoffman in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by University of Michigan Institutional Review Board (No. HUM00176834).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: G.J.H. is supported by the University of Michigan Older Americans Independence Center Research Education Core (AG024824) and University of Michigan Pepper Center pilot (AG024824).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.