
Abstract
Acculturation and racial discrimination have been independently associated with physical function limitations in immigrant and United States (U.S.)-born populations. This study examined the relationships among acculturation, racial discrimination, and physical function limitations in N = 165 African immigrant older adults using multiple linear regression. The mean age was 62 years (SD = 8 years), and 61% were female. Older adults who resided in the United States for 10 years or more had more physical function limitations compared with those who resided here for less than 10 years (b = −2.62, 95% confidence interval [CI] = [–5.01, –0.23]). Compared to lower discrimination, those with high discrimination had more physical function limitations (b = −2.51, 95% CI = [–4.91, –0.17]), but this was no longer significant after controlling for length of residence and acculturation strategy. Residing in the United States for more than 10 years is associated with poorer physical function. Longitudinal studies with large, diverse samples of African immigrants are needed to confirm these associations.
Introduction
With aging, older adults often develop physical function limitations (poor physical function) and disabilities, including an inability to walk, cook, or bathe (Verbrugge & Jette, 1994; World Health Organization & U.S. National Institute of Aging, 2011). The loss of the ability to participate in daily activities for older adults is typically a consequence of chronic diseases such as diabetes and hypertension, psychosocial factors, and a variety of other causes (Howrey et al., 2015; Stuck et al., 1999). Acculturation and racial discrimination—two psychosocial factors associated with immigration and minority status—are known risk factors for poor physical function in immigrant older adults and U.S.-born minorities, respectively (Gubernskaya et al., 2013; Walker et al., 2016). Physical function limitations have significant implications for poor health outcomes, including poor quality of life and mortality (Barile et al., 2012; Bentley et al., 2013; Koroukian et al., 2016). Poor physical function is associated with preventable health care expenses related to nursing home admissions, increased hospitalizations, and the use of long-term care services (Alecxih, 2010). Current studies provide very limited information on the burden of physical function limitations in African and Black immigrant older adults.
By 2060, 45% of U.S. older adults will belong to a racial/ethnic minority group (Mather et al., 2015, 2019). The growth of the African immigrant population serves as an important contributor to this trend. In 2015, there were 2.1 million African immigrants in the U.S. with Africans having the fastest growth rate from 2000 to 2013 among immigrants (Anderson, 2017). Currently, 19% of African immigrants are older than 55 years (U.S. Census Bureau & American Community Survey, 2014), and the number of older adults granted permanent residency in the U.S. is rising (Baugh & Witsman, 2017). Although it is essential to plan for the long-term care needs of this growing population, the prevalence of physical function limitations in older African immigrants in the U.S. is unknown, as reported rates in Black older adults range from 38.5% to 79% (Dallo et al., 2015; Melvin et al., 2014; Nkimbeng et al., 2019). In a study that disaggregated Black immigrants, the prevalence of physical function limitations in African immigrants was 3.6% (Elo et al., 2008). However, this sample was much younger (mean age of 39 years) than the older adult population with a high prevalence of physical limitations.
Migration and post migration processes—especially acculturation—present unique challenges for poor physical function in older adults. Acculturation is the process of cultural and psychological changes that occur when an individual migrates to a new environment (Berry, 1992, 2005; Gubernskaya et al., 2013; Lum & Vanderaa, 2010). It can impact changes in health behaviors such as diet and physical activity (Allen et al., 2014). Higher fat intake, lower consumption of fruits and vegetables, and increased intake of fast foods are some of the dietary changes that immigrants may engage in (Allen et al., 2014; Okafor et al., 2014; Tseng et al., 2015), which can impact chronic diseases. Proxy measures of acculturation (e.g., length of residence, age of migration, and naturalization status) indicate that greater acculturation is associated with physical function limitations (Gubernskaya et al., 2013; Ro & Gee, 2012; Wakabayashi, 2010). Although proxy measures are often measured in national surveys to decrease participant burden (Alegria, 2009), they may not fully capture the nuances of the acculturation process. Multidimensional theories and measures such as Berry’s (1992, 2005) acculturation theory may offer in-depth understanding of this process in immigrants.
Racial discrimination is associated with poor physical function and poor health in Blacks and other racial/ethnic minorities. Racial discrimination is differential treatment based on race or other inadequately justified factors that disadvantages a racial group (Blank et al., 2004; U.S. Equal Employment Opportunity Commission, n.d.). Studies link it to medical conditions such as diabetes, hypertension, and emotional health outcomes such as diabetic distress (Pascoe & Richman, 2009; I. C. Williams et al., 2020). Research shows perceived discrimination is associated with poor cognitive and physical function in older adults in Europe (Shankar & Hinds, 2017). In the U.S., racial discrimination correlates with physical function limitations in older African American women (Walker et al., 2016). Longer length of residence in the U.S.(acculturation) is associated with increased perception of racial discrimination in immigrants (Brondolo et al., 2015). Discrimination, especially in the context of acculturation, remains yet to be explored in the African immigrant population.
The growing burden of chronic diseases in adult African immigrants may impact future physical function in this population. According to a breadth of studies, hypertension prevalence ranges from 8.3% to 40% (Commodore-Mensah et al., 2018; Njeru et al., 2016; Sewali et al., 2015), diabetes prevalence from 34.6% to 65.5% (Commodore-Mensah et al., 2018; Njeru et al., 2016; Obisesan et al., 2016), and obesity prevalence from 5.4% to 55% (Commodore-Mensah, Matthie, et al., 2017; Njeru et al., 2016; O’Connor et al., 2014; Sewali et al., 2015). These are all risk factors for physical function limitations in older adults (Stuck et al., 1999).
In this study, we examined the relationship among acculturation, discrimination, and physical function in African immigrant older adults. Using a multidimensional measure of acculturation, we examined acculturation strategies of older African immigrants and how these strategies impact physical function. We hypothesized that those who are more acculturated and have greater experiences of discrimination also have more physical function limitations. Although, there are some studies of physical function in African Americans and other U.S.-born older adults, ethnic and cultural differences between U.S.-born older adults and African immigrants can impact health behaviors and subsequently differential health outcomes. An understanding of these unique risk factors of poor physical function can inform tailored health interventions for African immigrant older adults in the U.S.
Method
Study Design and Sample
To leverage recruitment efforts in a difficult to reach population, this study drew on data from two concurrent studies in the Baltimore-Washington Metropolitan area. Inclusion criteria were as follows: (a) ≥50 years, (b) born in Africa, (c) ability to communicate in English, (d) lived in the United States for ≥6 months, (e) Black race, (f) cognitively intact from the six-item screener (Callahan et al., 2002), and (g) have ≥1 mobility limitation based on National Health Interview Survey Mobility questions (National Center for Health Statistics, 2016). The first study, which began in 2017 and is currently ongoing, is an epidemiological study to examine the overall health of African immigrant adults. In total, 76 participants from this study are included in this analysis. The second study examined physical function in older African immigrants. Researchers enrolled 89 participants from February 2018 to March 2019. Researchers employed the same instruments to measure all study variables in both studies, and data collectors were shared across both studies. An academic institutional review board (IRB) approved the study protocols.
The convenience sampling approach and community recruitment methods were the same for both studies (Commodore-Mensah et al., 2019). Researchers recruited participants through community-based organizations, word of mouth, and social media. Data collection events at community-based organizations occurred after leadership approval and IRB approval of that recruitment site. In Study 1, some potential participants with the study link completed the survey on a computer or smart mobile device, and consent information was included at the start of the online survey. Survey completion was considered consent for these participants. Participants who were screened by phone for Study 2 had the choice to have the survey mailed to them with a prepaid return envelope or participate via home data collection. Home data collection was scheduled at a convenient time for the participant. Trained research assistants obtained oral informed consent from in-person, and phone participants using an IRB-approved consent script. All participants completed a survey with items from the measures discussed below. About 80% of study research assistants were African immigrants.
Measures
Physical function
The study outcome was physical function limitations, which we measured with the Patient-Reported Outcomes Measurement Information System Physical Function short form (PROMIS PF 10a). This scale assessed the degree of difficulty in doing daily functional activities such as bending, climbing stairs, carrying groceries, and bathing (Rose et al., 2014). Data were collected on the paper version of the PROMIS PF 10a scale, and scores were transformed to T scores using the short form conversion tables (Rose et al., 2014). The U.S. population’s mean T score is 50, with a standard deviation of 10. Higher PROMIS-PF10a T scores represent better function.
Risk factors
Acculturation
Acculturation was measured with length of residence in the U.S. and the modified Psychological Acculturation Scale (PAS; Tropp et al., 1999). Length of residence is a continuous self-reported number of years each participant resided in the U.S. This variable was dichotomized as <10 years or ≥10 years, as is the norm in many immigrant studies (Commodore-Mensah et al., 2016; Gubernskaya et al., 2013). The PAS measures changes that may occur during the acculturation process with questions such as “which group(s) of people do you feel the most comfortable?” and “In what culture do you feel confident you know how to act?” Responses are Likert-type scale ranging from 1 = “totally disagree” to 5 = “totally agree.” This scale has strong psychometric properties (Tropp et al., 1999) and has been used with African immigrants. Internal consistency in this sample was 0.81. The PAS questions were divided into two dimensions—one for the U.S. and the other for country of origin—and mean scores are calculated for each dimension. Scores were later categorized to form four acculturation strategies according to Berry’s theory. Berry’s theory of acculturation delineates four strategies to describe the uptake of new country culture and characteristics in comparison to the loss of country of origin culture (Berry, 1992, 2005). Individuals can adapt by adopting one of four acculturation strategies. They can become (a) assimilationist (abandoning the old cultural identity and adopting the new culture completely), (b) integrationist (maintaining both cultures), (c) separationist (not engaging in the new culture), or (d) marginalist (neither engaging in the old or new cultures). The separationist strategy in this study is called traditionalist (Commodore-Mensah, Ukonu, et al., 2017). Mean scores for each dimension were the basis of categorizing study participants according to one of the four acculturation strategies. Specifically, high scores on both dimensions (≥3) were categorized as integrationists, whereas high scores for the United States (≥3) and low scores for country of origin (<3) were assimilationists. High scores on the country of origin (≥3) and low scores for the United States (<3) were traditionalists, and low scores for both dimensions (<3) were categorized as marginalists. In this sample, only two participants were categorized into the assimilationist and marginalist categories, respectively. Therefore, our analysis presents a comparison of only the integrationist and traditionalist strategies and excludes these four participants because inferential analyses cannot be conducted with these.
Discrimination
Discrimination was measured with the Everyday Discrimination Scale (EDS; Williams D. R. et al., 1997; Williams D. R., 2012). This scale has nine items that assess experiences of discrimination during everyday activities. Questions include “You are treated with less courtesy than other people are,” “You are treated with less respect than other people are,” or “You are threatened or harassed.” Responses are rated categorically as 0 = Never, 1 = Rarely, 2 = Sometimes, and 3 = Often. Total scores for the nine discrimination items were highly skewed. Therefore, responses were dichotomized into high discrimination—as described by Mays and Cochran (2001) and Pérez et al. (2008)—if participants reported “sometimes or often” on one or more of the scale items, and low discrimination otherwise. The internal consistency of this scale in this sample was alpha = .86.
Covariates
Covariates in this study included sociodemographic characteristics and health conditions. Sociodemographic characteristics included age, sex, level of education, marital status, income, employment status, health insurance, and migration reason. Age was continuous years of life, whereas sex was binary (male or female), and health insurance was binary (yes or no). Education level was measured in categories of the highest level of education and technical training completed, whereas marital status was categorized by participant’s reported marital status. Household income was measured with categories ranging from US$0 to US$120,000 in US$10,000 increments, but it was later collapsed to US$40,000 increments for analyses. Employment status and migration reasons were categorized as reported by participants. We also reported where data were collected for each participant with categories of the recruitment source. Health conditions assessed in this study include diabetes, hypertension, and depressive symptoms. Responses were obtained for whether participants have ever been diagnosed with diabetes or hypertension. Depressive symptoms were measured with the Patient Health Questionnaire (PHQ-8; Kroenke et al., 2009). All data were self-reported.
Data Analysis
We used means (SD) and proportions to summarize continuous and categorical variables, respectively. To examine the unadjusted and adjusted relationships among acculturation, discrimination, and physical function, we fitted univariable and multivariable linear regression analyses. Three unique models were examined, which include physical function and (a) acculturation strategy, (b) length of residence, and (c) discrimination. In addition, we examined the relationships between discrimination and physical function after controlling for acculturation strategy and length of residence. Covariates included in each model were chosen based on literature review of their association with physical function limitations and stepwise model building. Diagnostic plotting of residuals versus continuous covariates and residuals versus fitted values was employed to evaluate violations of linearity and homoscedasticity assumptions; the assumptions appeared well met. Sensitivity analyses were conducted to address outlier influence and evaluate the robustness of findings to different definitions of independent and outcome variables (e.g., creating categories for continuous variables, using higher/lower cutoff scores), and imputation of missing data for key variables. More sensitivity analyses were conducted for complete data only (n = 127) and controlling for the study that recruited each participant (see online appendix). These analyses showed similar direction for the relationship among length of residence, acculturation strategy, discrimination, and physical function. Analyses were conducted in Stata 15 I/C (StataCorp, 2017).
Results
Demographic Characteristics of the Sample
The mean age was 62 years (SD = 8 years), and 61% were female (Table 1). Overall, 60% of the data were collected at community-based organizations that serve African immigrants. And, 58% migrated to join other family members, 61% had lived here for 10 years or more, and 50% migrated before the age of 50 years. Overall, 29% of participants had a bachelor’s degree or higher. The majority (54%) of the sample had hypertension, and 29% had diabetes. The average functional limitation T score was 45, indicating that the physical function of this sample was 5 points lower than the general adult population T score. The majority of participants in both studies had lived in the United States for 10 years and acculturated through the integrationist strategy. There was no difference in the level of discrimination (see online appendix), but participants in Study 1 were older and had lower physical function scores.
Characteristics of African Immigrant Older Adults With Physical Function Limitations.
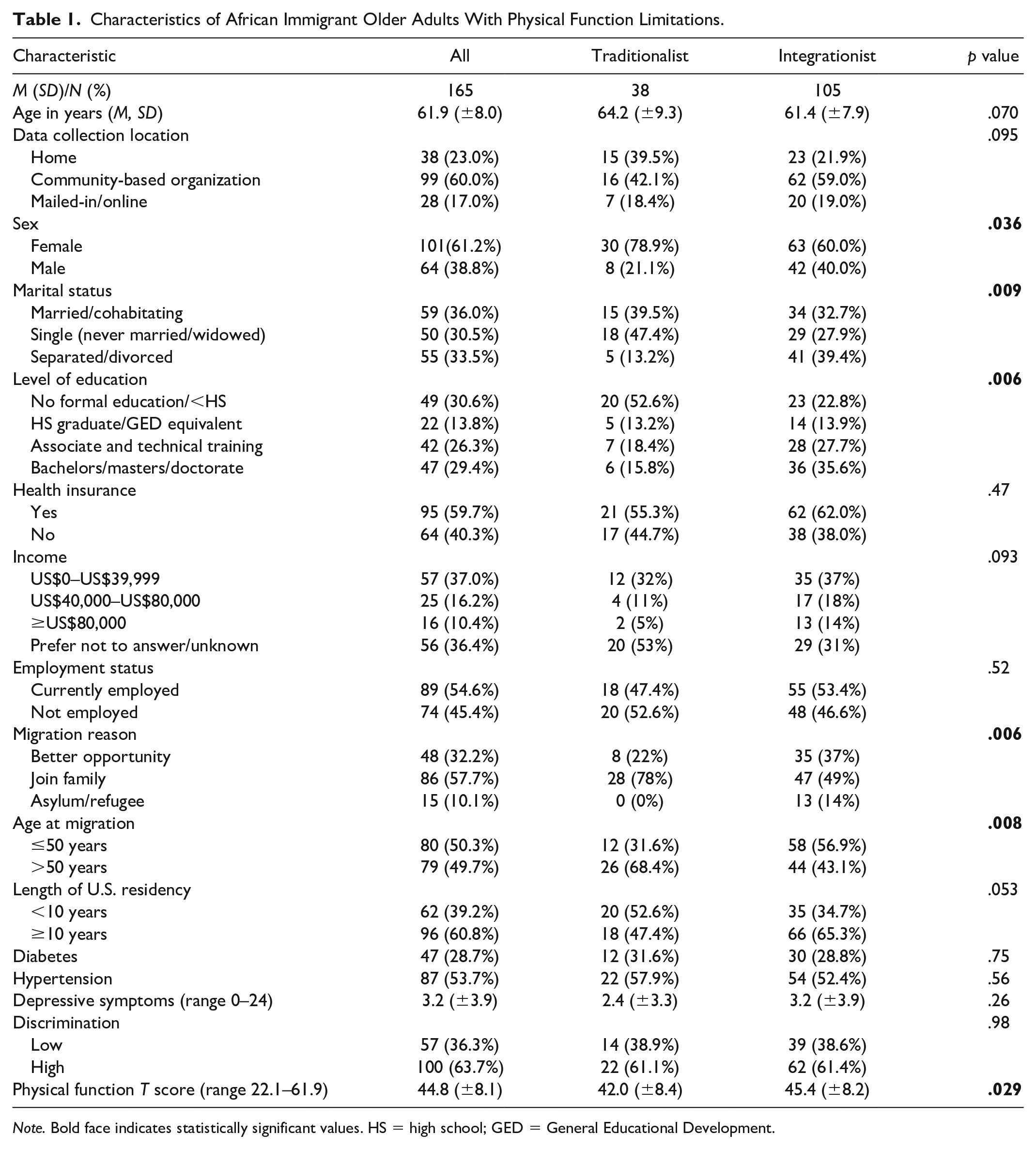
Note. Bold face indicates statistically significant values. HS = high school; GED = General Educational Development.
Comparison of Sample Characteristics by Acculturation Strategy
Almost two thirds of this sample used the integrationist acculturation strategy. In unadjusted analyses, there were significant differences in sample characteristics by acculturation strategy. These included sex, marital status, level of education, migration reason, age at migration, and physical function score (p < .05 for all). Specifically, more people categorized as traditionalist had less than high school or no formal education. The majority of participants who were classified as traditionalists migrated to the U.S. after the age of 50 years.
Acculturation and Physical Function
Older adults who had resided in the U.S. for more than 10 years had more physical function limitations than their counterparts who had immigrated more recently. After adjusting for covariates, older adults who had resided in the U.S. for more than 10 years had a 2.6-point lower physical function score compared with those who had resided in the U.S. below 10 years (b = −2.62, 95% CI = [–5.01, –0.23]), indicating that individuals who had resided in the U.S. for more than 10 years had poorer function (Table 2). Participants categorized as traditionalists had significantly poorer physical function (T score = 42, SD = 8.4) compared with integrationist (T score = 45.4, SD = 8.2). After controlling for covariates, integrationist had a 0.02 higher T score (b = 0.02, 95% CI = [–2.76, 2.80]) compared with traditionalist, but this was not statistically significant (Table 2).
Relationship Between Length of U.S. Residence and Physical Function (n = 154), and Relationship Between Acculturation Strategies and Physical function (N = 139).
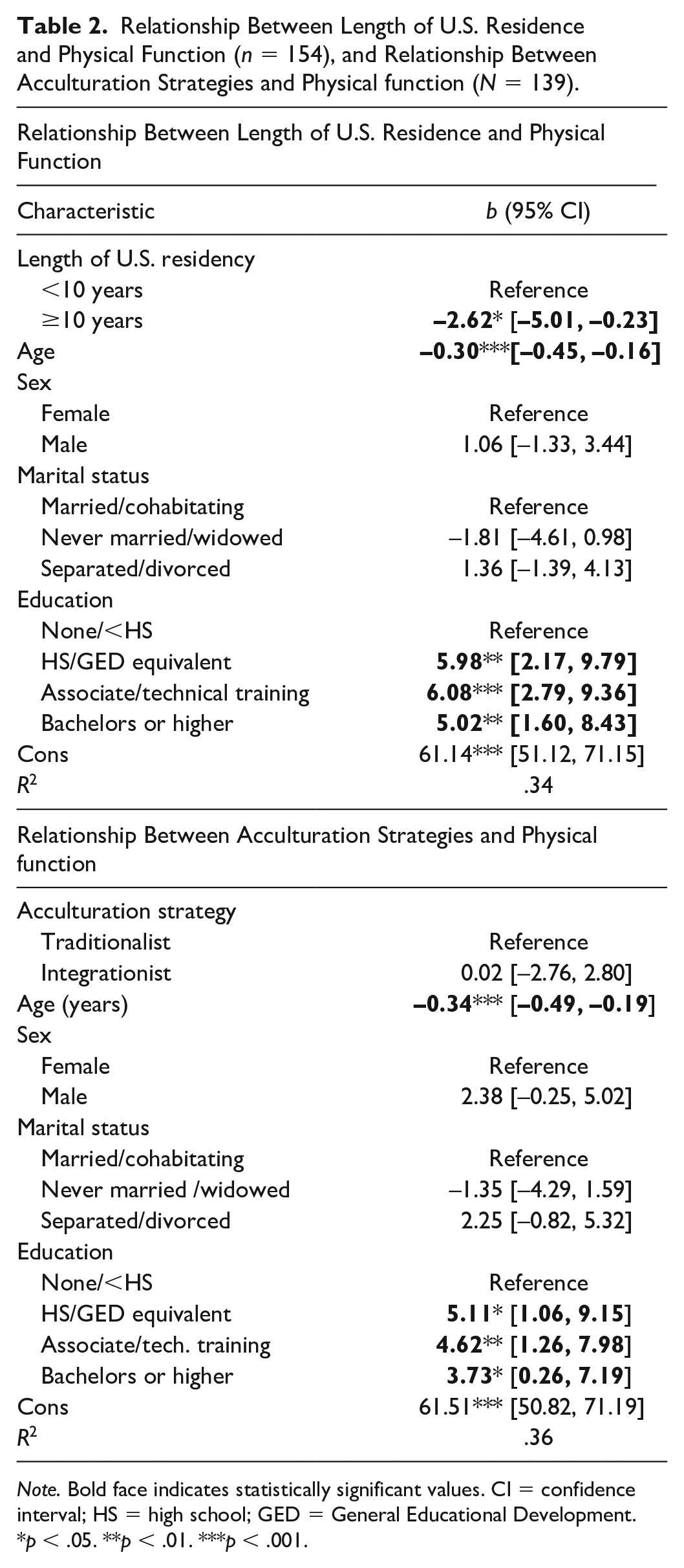
Note. Bold face indicates statistically significant values. CI = confidence interval; HS = high school; GED = General Educational Development.
p < .05. **p < .01. ***p < .001.
Discrimination and Physical Function
Discrimination was not statistically significantly associated with poor physical function in univariable analyses. However, after adjusting for age, sex, marital status, education, health insurance, and employment status, participants with high levels of discrimination had significantly poorer physical function (2.5-point lower T score) compared with those with low discrimination (b = −2.51, 95% CI = [–4.84, –0.17]; Table 3). When length of residence and acculturation strategies were controlled, discrimination coefficients became nonsignificant.
Relationship Between Discrimination and Physical Function.
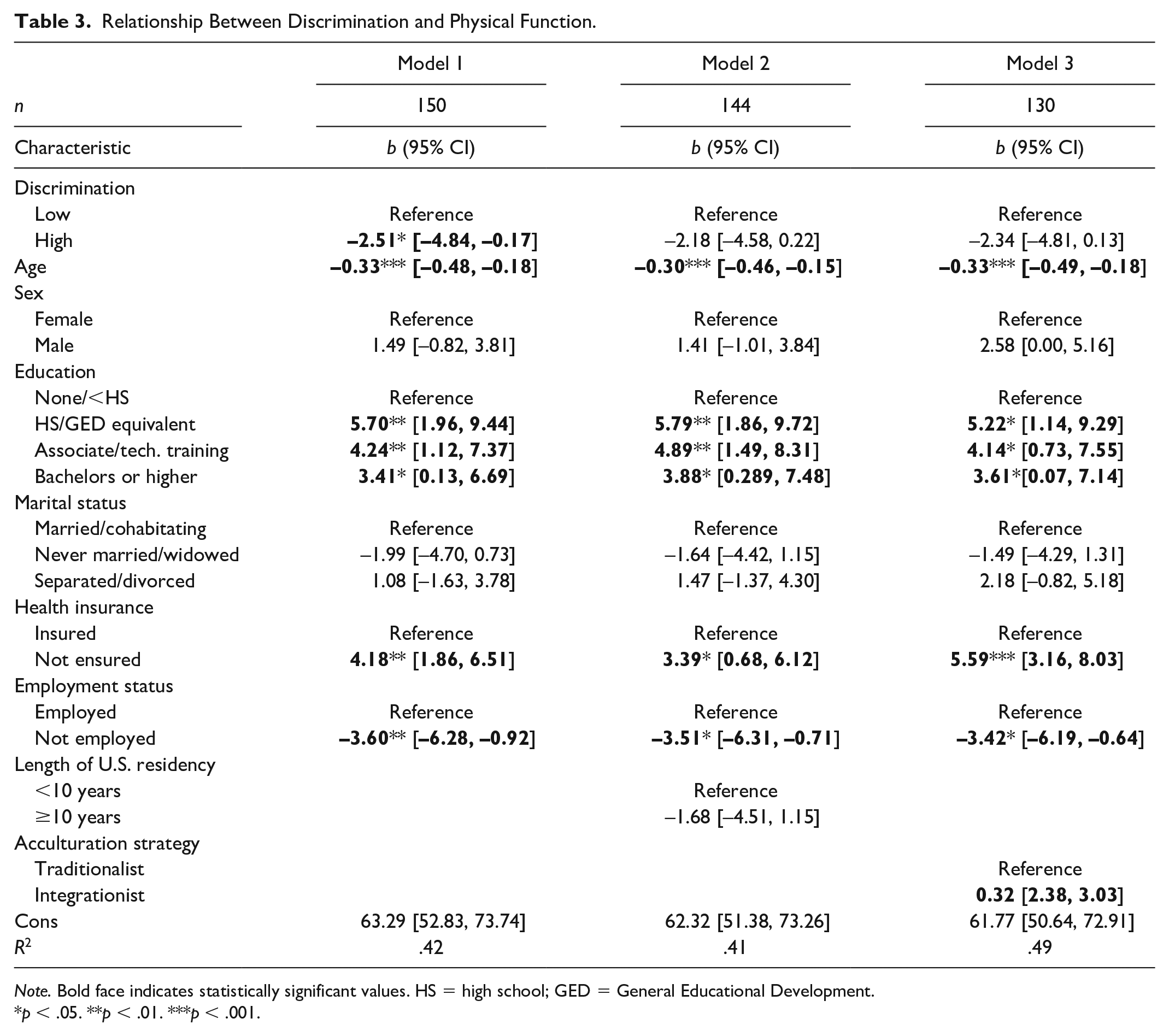
Note. Bold face indicates statistically significant values. HS = high school; GED = General Educational Development.
p < .05. **p < .01. ***p < .001.
Discussion
The purpose of this study was to examine the relationship among acculturation, discrimination, and physical function in African immigrant older adults. In this sample, participants primarily adopted the integrationist acculturation strategy (identified equally with the African and American cultures), and in univariable analyses, it was linked to better function compared with the traditionalist strategy (only identifying with country of origin culture). From the adjusted analyses, the integrationist strategy was not related to poorer physical function (better function). Therefore, our acculturation strategy hypothesis was not supported but length of residence as a proxy for acculturation was supported, as those who had resided in the country for more than 10 years had more physical function limitations.
Although limited, studies of acculturation strategies in African and older immigrants reveal similar patterns noted in this study. A recent study also found that the majority of younger African immigrants (M age = 49.5 years) were integrationists (Commodore-Mensah, Ukonu, et al., 2017). Similar to our sample, Jang and colleagues (2007) found that Korean immigrant older adults classified as traditionalist had poorer functional and mental health outcomes compared with their integrationist counterparts (Jang et al., 2007). However, cluster analyses of a different sample of Korean immigrant older adults revealed that the majority were moderately bicultural (greater orientation to Korean culture than American culture) was the predominant acculturation strategy (Rhee, 2019). Although it was not significant in our adjusted models, in the univariable comparison, traditionalists had significantly poorer physical function compared with integrationists. In a multistate sample of Korean older adults, greater American acculturation was associated with improved functions; however, this finding became nonsignificant after adjusting for gender (Choi et al., 2020). Larger studies with diverse samples are needed to fully understand how different acculturation strategies impact functional health outcomes in immigrant older adults.
Length of residence as a proxy measure of acculturation was related to more physical function limitations in this sample. Greater adoption of U.S. culture is considered higher acculturation (Schwartz et al., 2010), and it is assumed that with longer residence, there are more opportunities to adopt more aspects of U.S. culture. Limited research in African immigrants show that longer residence in the U.S. is linked with poor health outcomes. Analyses of data from the National Health Interview Survey (1997–2005) reveal that longer length of U.S. residency for African immigrants was related to greater odds of being overweight (Oza-Frank & Venkat Narayan, 2010). In a study of Ghanaian and Nigerian immigrants, longer residence in the United States was associated with greater odds of cardiovascular disease risk factors (Commodore-Mensah, Ukonu, et al., 2017). However, analyses of 5 years of the National Health Interview Surveys showed that recently immigrated (lived in the country for <12 months) foreign-born Black older adults had the highest proportion of poor physical function (Nkimbeng et al., 2019).
Discrimination experiences were significantly associated with poorer physical function in analyses with 150 participants but became nonsignificant in reduced samples. In a study with 120 middle-age older adult women in the U.S., greater experiences of racial discrimination were related to poorer function (Walker et al., 2016). Research on the relationship between racial discrimination and physical function in older adults is limited, but prior studies have examined the relationship between perceived racial discrimination and a number of chronic diseases. Racial discrimination was associated with diabetes, hypertension, and depression, which are current risk factors for poor physical function (Lewis et al., 2015; Pascoe & Richman, 2009; D. R. Williams & Mohammed, 2009).
There is some evidence to suggest that acculturation may impact the perception of discrimination in immigrants. Greater length of residence (proxy measure of acculturation) in the U.S. is associated with greater cultural racism (racial discrimination; Case & Hunter, 2014). In Norway, skin-tone discrimination was associated with acculturation in African immigrants, where discrimination from Whites was associated with lower uptake of Norwegian culture and discrimination from Africans was associated with decrease upkeep of African culture (Kunst & Phillibert, 2018). In this study, the relationship between discrimination and physical function was attenuated after adjusting for the length of residence and acculturation strategies, but the point estimate remained large, which is suggestive of precision loss. Post hoc analyses did not reveal any significant interaction effects. Further research with larger and more representative samples can provide a clear understanding of these interactive relationships.
This study has a few limitations. First, the African immigrant older adults in this sample were primarily from five countries, and the majority of them were currently living in the Baltimore-Washington Metropolitan area. These results might not reflect the health of all African immigrants in the U.S. Second, this study presents results from cross-sectional analyses. This makes it impossible to establish temporality and causality. Also, acculturation strategies were assessed at one time point; participants may transition between acculturation strategies with time in the U.S. or interaction with other factors, such as living in an ethnic enclave. Third, study data were collected through self-report, which may be influenced by social desirability bias during interviews and/or recall bias in self-administered surveys. Fourth, due to financial constraints, this study only included English speaking participants; therefore, the results might not reflect the experiences of non-English speaking older African immigrants.
Conclusion
To the best of our knowledge, this was the first study to examine physical function in African immigrant older adults in the U.S. African immigrant older adults who had resided in the United States for ≥10 years had worse physical functions compared with newer immigrants. More studies with large diverse samples of African adults (individuals from more African countries and different regions of the U.S.) using longitudinal designs are needed to explore how various acculturation strategies may impact experiences of discrimination and physical function with time in the U.S. In addition, qualitative studies can help provide in-depth understanding of the acculturation process, and may inform identification and description of which cultural practices and health behaviors are changing in immigrants. Greater understanding of this process can facilitate targeting of health interventions to enhance uptake and maintenance of health promoting behaviors. Poor physical function is prevalent in older adults and is costly, but it is also modifiable. Health care providers should assess and refer participants for treatment during routine appointments. In addition to physical and occupational therapy assessment and treatment, innovative interventions such as the Community Aging in Place Advancing Better Living for Elders (CAPABLE) that are also cost saving are potential treatment approaches (Ruiz et al., 2017; Szanton et al., 2019). Finally, all participants in this sample have at least one mobility limitation: a precursor to poor physical function (Verbrugge & Jette, 1994); health policies are needed to ensure timely assessment and treatment of poor physical function in older adults.
Supplemental Material
sj-pdf-1-jag-10.1177_0733464820977608 – Supplemental material for Longer Residence in the United States is Associated With More Physical Function Limitations in African Immigrant Older Adults
Supplemental material, sj-pdf-1-jag-10.1177_0733464820977608 for Longer Residence in the United States is Associated With More Physical Function Limitations in African Immigrant Older Adults by Manka Nkimbeng, Yvonne Commodore-Mensah, Jacqueline L. Angel, Karen Bandeen-Roche, Roland J. Thorpe, Hae-Ra Han, Peter J. Winch and Sarah L. Szanton in Journal of Applied Gerontology
Footnotes
Acknowledgements
The authors thank the participants for generously sharing their time and experiences for the purpose of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Robert Wood Johnson Foundation Health Policy Research Scholar program, the National Institute on Aging (NIA# 1F31AG057166-01), and the Johns Hopkins Institute for Clinical and Translational Research (ICTR) which is funded in part by Grant Number TL1 TR001078 from the National Center for Advancing Translational Sciences (NCATS), a component of the National Institutes of Health (NIH) and NIH Roadmap for Medical Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of the Robert Wood Johnson Foundation, Johns Hopkins ICTR, NCATS or NIH.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.