
Abstract
Background
Care transitions are frequent among patients with dementia. This study aimed to estimate the impact of continuity of care (COC) on successful community discharge after hospitalization.
Methods
National Veterans Health Administration data linked to Medicare claims in fiscal years 2014–2015. Community-dwelling older veterans with dementia with an acute hospitalization were included (n = 31,648). COC was measured by the Bice-Boxerman Continuity of Care (BBC) index (0–1). Association of COC before hospitalization on successful community discharge was examined separately among veterans discharged to the community directly and through post-acute care facilities.
Results
Veterans with a 0.1 higher BBC were 4.6% (p = .06) more likely to have successful direct community discharge; but BBC had no demonstrable effect when discharge was through post-acute care facilities.
Conclusion
Better COC may have impact at improving successful direct community discharge, although the effect is small and the type I error rate (statistical significance) was 6%.
Introduction
Between 30% and 48% of community-dwelling patients with dementia are hospitalized each year (Toseland et al., 1999; Zhao et al., 2008). Readmissions and nursing home admissions after hospital stays are frequent among older adults with dementia (Callahan et al., 2012, 2015), and some have been shown to be unnecessary or preventable (Callahan et al., 2012; Jencks et al., 2009). Successful hospital discharge to community (community discharge not followed by unplanned rehospitalization, nursing home admission or death) is likely to be associated with better patient satisfaction, lower cost and better quality of care. Aligned with this concept, the Centers for Medicare and Medicaid Services (CMS) established the Hospital Readmission Reduction Program in October 2012 to address the high rates of hospital readmissions. In 2016, CMS also included successful discharge to the community from skilled nursing facility as one of its publicly reported quality measures (Abt Associates, 2016). In the Veterans Health Administration (VHA), Patient-Aligned Care Team (PACT; Veterans Affairs (VA) medical homes) was established in 2014 and a measure of rehospitalization was added to the Veteran Integrated Service Networks Directors’ annual performance plan (U.S. General Accounting Office, 2019). However, to the best of our knowledge, the concept of successful community discharge following hospitalization (regardless of discharge destination) for community residing patients has not been studied.
Policymakers and healthcare systems have pointed to the integral role that primary care can play in preventing hospital readmissions (Meyers & Brady, 2020). One of the tenets of primary care is continuity of care (COC), the extent to which a patient seeks care from the same provider, reflecting greater provider knowledge of patients, greater commitment to their care, and more trust (Starfield, 1992). Continuity of care may be especially important in the care for persons with dementia, who are mostly cared for within primary care (Boustani et al., 2007). Complexity of conditions and long duration of illness of patients with dementia require ongoing knowledge of their medical and psychosocial conditions. Recent healthcare reforms promote COC through the Patient Protection and Affordable Care Act’s support of Patient-Centered Medical Home (2007), development of accountable care organization (2017), and VHA PACT(2014). Better COC has been found to be related to lower hospitalization rates (Katz et al., 2015; Lei et al., 2020; Maciejewski et al., 2014; Nelson, Sun, et al., 2014); but, to our knowledge, no study had examined its relationship to post-acute outcomes. Current interventions to reduce hospital readmissions focus on timely follow-up after home discharge (Brooke et al., 2014; Hernandez et al., 2010; Jackson et al., 2015); but little attention has been given to COC prior to hospitalization. This study aimed to fill these knowledge gaps by investigating the impact of COC prior to hospitalization on successful hospital discharge.
This study focused on veterans with dementia due to the significant efforts in VHA to improve COC and limit rehospitalization. Moreover, the decades-long system-wide use of electronic health records forms an important back-bone to good, continuous primary care (U.S. Department of Veterans Affairs, 2021). This study also addressed a methodological challenge in studying the impact of COC on successful community discharge which results from unobserved or unrecorded health confounders such as severity of dementia (i.e., endogeneity). We hypothesized that veterans with higher COC prior to hospitalization were more likely to have successful discharge to the community after hospitalization.
Design and Methods
Data Source
Many older veterans use both VA and other healthcare options, primarily Medicare; thus, our study data included data from both sources (Lei et al., 2018). We used VHA Office of Geriatrics & Extended Care Data Analysis Center (GECDAC) Core Files in Fiscal Years (FYs) 2014–2015 which merge VHA (enrollment and residential information and VHA provided and purchased inpatient and outpatient records/claims) and Medicare (enrollment and claims) data at the veteran level using VA’s Scrambled Social Security Number (Dally et al., October 2018). We used the GECDAC Residential History File, which aggregates VHA and Medicare utilization and Minimum Data Set resident assessments from community living centers, state veterans homes, and community nursing homes to track veterans through healthcare locations (Intrator et al., 2011). Veteran’s residential information, updated quarterly, was obtained from the VHA Planning Systems Support Group data. VHA staff data and Medicare Carrier claims were used to identify providers by their National Provider Identification and specialty. Population and market characteristics were obtained by linking veterans’ residential information to 2015 U.S. Census data and 2014 Area Health Resource Files.
Study Cohort
Veterans with dementia were identified from VHA and Medicare face-to-face inpatient and outpatient claims with ICD-9-CM codes for dementia diagnoses in a VHA sanctioned list (046xx, 290xx, 291.2, 292.82, 294xx, and 331xx), and from VHA pharmacy and Medicare part D prescriptions with medications commonly used to treat dementia (donepezil, galantamine, rivastigmine, and memantine) (Alzheimer’s Association, 2020). Veterans with dementia were identified as those with ≥1 inpatient or ≥2 outpatient diagnoses or with 1 outpatient diagnosis and ≥1 medication prescription in FYs 2007–2014.
The study cohort (Figure 1) included veterans with dementia ≥66 years old who had any acute inpatient medical or surgical hospitalization from the community between October 2014 to August 2015 with only the first hospitalization in this period included (n = 54,322; index hospitalization). We excluded veterans who were not enrolled in Medicare (n = 569) or who were enrolled in Medicare Advantage due to incomplete data (n = 5902). We excluded veterans continually in nursing home for >90 days in FY 2014 (considered to not be community dwelling; n = 1172) and with <3 selected outpatient visits because the COC measure was less reliable with few visits (n = 5515) (Nelson, Sun, et al., 2014). We further excluded veterans who died in hospital (n = 2191) or died after discharge to post-acute care (PAC) facilities (nursing homes and rehabilitation centers; n = 2141). Veterans who were discharged to community with outpatient hospice were also excluded as death was expected (n = 1727) and veterans who were discharged to nursing homes for long-term care (>90 days; n = 2570). Finally, we excluded veterans residing in Puerto-Rico and the Virgin-Islands for consistency with our other studies (n = 887). The final cohort included 23,331 veterans who were discharged to the community directly and 8317 veterans who were first discharged to a PAC facility and then to the community. Study cohort and successful discharge to the community, Note. FY, fiscal year; PAC, post-acute care; NH, nursing home.a If the veteran has multiple acute hospitalization in FY 2015, the first acute hospitalization is identified as the index hospitalization.b Post-acute care facilities include nursing home and rehabilitation hospital.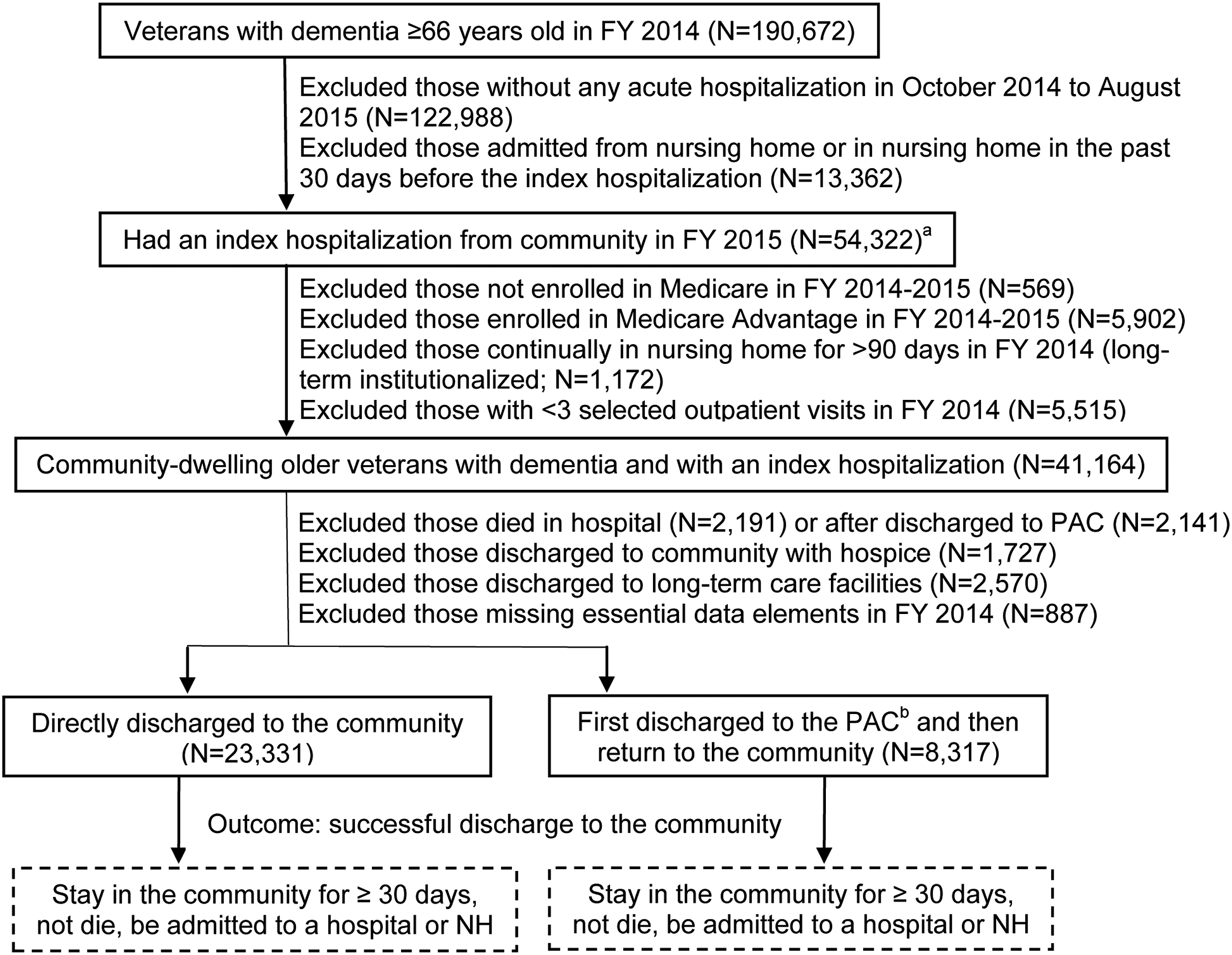
Variables
COC
Continuity of care was measured by the Bice-Boxerman Continuity of Care (BBC) index (Amjad et al., 2016; Chen & Cheng, 2016; Cheng & Chen, 2014; Hussey et al., 2014; Johnston & Hockenberry, 2016), reflecting the relative ratio of the veteran’s total visits to distinct providers. BBC measured the dispersion of care across various providers. The BBC ranges from zero (each visit involves a different provider) to one (all visits are to the same provider) with higher scores indicating better COC. In constructing the BBC within 1 year prior to the index hospitalization, we included outpatient evaluation and management visits during the time window, defined by Berenson-Eggers Type of Service codes M1A, M1B, M4A, M5B, M5C, M5D, and M6 (Hussey, et al., 2014; Johnston & Hockenberry, 2016). In addition, we counted only visits to providers most likely to be involved in outpatient management of veterans with dementia: primary care providers (physicians with general, family, internal, preventive and geriatric medicine, nurse practitioner, and physician assistant) and dementia-related specialists (neurologist, psychiatrist, psychologist and social worker). We only included veterans with at least 3 selected visits. Examples of BBC are provided in Supplementary Table 1.
Successful discharge to the community
We adapted the CMS’ definition of successful discharge to the community from skilled nursing facility (Abt Associates, 2016). Community discharge after hospitalization were considered successful if during the 30 subsequent days the veteran did not die, was not readmitted to a hospital for an unplanned inpatient stay, and was not admitted to a nursing home (Figure 1). We applied Research Triangle Institute’s modified version of the CMS’ Planned Readmission Algorithm to identify the unplanned readmission after index hospitalization (Smith et al., 2015).
We modeled each of the reasons of unsuccessful community discharge (30-day unplanned rehospitalization, nursing home admission, and mortality) and also combined them as a single dichotomous outcome. We separately modeled the impact of COC on successful discharge to the community among veterans who were discharged to the community directly and those who were first discharged to a PAC facility (e.g., skilled nursing facility or rehabilitation center) and then returned to the community since the two cohorts might be different in terms of health status and healthcare needs (Nguyen et al., 2015). Last, we constructed a binary indicator for any primary care visits within 14 days after community discharge (directly or through PAC) as an intermediate outcome to test the underlying mechanism that COC might impact successful community discharge.
Covariates
We adjusted for potential confounders of successful community discharge including socio-demographics (age, gender, race, and marital status), socio-economic variables (priority group, rurality, Medicaid eligibility status, and median household income in the ZIP code area where the Veteran resided), and market characteristics (number of active physicians, nursing home beds and hospital beds per 1000 population in the county) in FY 2014. Priority group is determined by service-connected disabilities and income and determines VHA benefit coverage (U.S. Department of Veterans Affairs, 2018). Baseline (in FY 2014) health risk factors included years living with dementia, JEN Frailty Index to determine the risk of long-term institutionalization (Kinosian et al., 2018), 34 comorbidity indicators to adjust for illness burden (Lei et al., 2018), and enrollment in Geriatric PACT and Home-based Primary Care PACT for veterans with complex medical needs. We also included total number of visits (to primary care providers, dementia-related specialists and other specialists) as a measure of severity of conditions, baseline acute hospitalization (Rudolph et al., 2010), and risk factors during index hospitalization (in FY 2015) including length of stay, an indicator for surgical procedures, and an indicator for intensive care unit use.
Instrumental variable
We used an instrumental variable approach to address the endogeneity of health and COC to estimate the impact of COC on successful discharge. The instrument was an indicator of a change in residence at a distance (longitude/latitude) of more than 10 miles in FY 2014 (4.3% of cohort; n = 1361). Veterans who moved more than 10 miles would likely need to change their “usual” providers, resulting in lower COC. We used 10 miles as the cut-off as such a distance is more likely to require discontinuation of care by previously visited providers and establishment of new provider relationships in the new community.
The instrumental variable approach also assumes that the instrument, the move, was not correlated with the outcome, successful community discharge, except through COC. This assumption would be invalidated if veterans moved due to worse health conditions which are likely to impact on the success of a subsequent hospital discharge, for example, a move for external social support which is also unobservable in administrative data. In addition, there should not be any mutual confounders between the instrument and outcomes through which the instrument might impact the outcomes. These conditions cannot be proven. However, we conducted some sensitivity analyses, as recommended in the literature (Ali et al., 2014; Valley et al., 2015). We checked the balance of observed risk factors and other baseline characteristics between veterans who moved more than 10 miles and those who did not and found that the majority were balanced (Supplementary Table 2). As recommended, we adjusted the instrumented model (stages 1 and 2) for the variables that were not balanced (Age [66–74], marital status, Medicaid, years living with dementia, JEN Frailty Index [0–2], number of visits to primary care providers and other specialists, substance dependence, and several mental health conditions) and performed analyses stratified by these variables.
Statistical Analyses
We used a Probit model and an instrumental variable Probit model to estimate the impact of BBC within 1 year before the index hospitalization and other covariates in FY 2014 on the community discharge outcomes in FY 2015. This approach addresses the problem of reverse causality that could arise by modeling BBC and successful hospital discharge in the same year (Johnston & Hockenberry, 2016; Maciejewski et al., 2014). We multiplied the BBC score by 10 to estimate the impact of 0.1-unit BBC increments on successful community discharge (Nyweide et al., 2013).
Since Probit model coefficients cannot be interpreted in terms of the outcome probability change due to one-unit increment in BBC scores, we reported the marginal effect and used bootstraping with 500 replications to generate 95% confidence intervals (CIs); draws were made at the VA medical center (n = 140) to deal with clustering.
To deal with the imbalances of age, marital status, Medicaid status, years living with dementia, JEN Frailty Index, substance use disorder, mental health conditions, and number of visits on the instrument, we performed sensitivity analyses stratified by these variables to rule out an association of move with outcomes, which would invalidate the instrumental variable assumption. We also conducted a sensitivity analysis excluding veterans with assisted living residence identified in Medicare part B claims (Thomas et al., 2018), as a move to assisted living may signal worsened health conditions. We further tested the validity of the instrumental variable by modeling only veterans who had any change in residence and still using a move by more than 10 miles as the instrument to rule out an association of move with outcomes because veterans who moved and those who did not may have different outcome distributions. We tested other cut-offs for the instrument (change in residence by more than 5 miles [6.1%] and change in residence by more than 15 miles [3.3%]) since we were concerned about the variability of the instrument. We performed sensitivity analyses using a BBC measure of only primary care visits (continuity of primary care), excluding visits by dementia-related specialists to test the possibility that BBC was unnecessarily lower for veterans referred to a dementia-related specialist. Finally, we tested the sensitivity to the selection of BBC as the measure of COC by using a density measure of COC, the Usual Provider of Care (UPC) measure (Katz et al., 2014; Katz et al., 2015), which reflects the proportion of veteran’s total visits to the most frequently visited provider. We reported results using a statistical significance level with p-values of <0.1 due to the complex instrumental variable design, the great number of covariates in the models, and the low prevalence of move which might limit the power of the instrumental variable analysis. All statistical analyses were conducted using Stata version 15.1 (StataCorp).
Results
Summary Statistics of Variables of Interest.
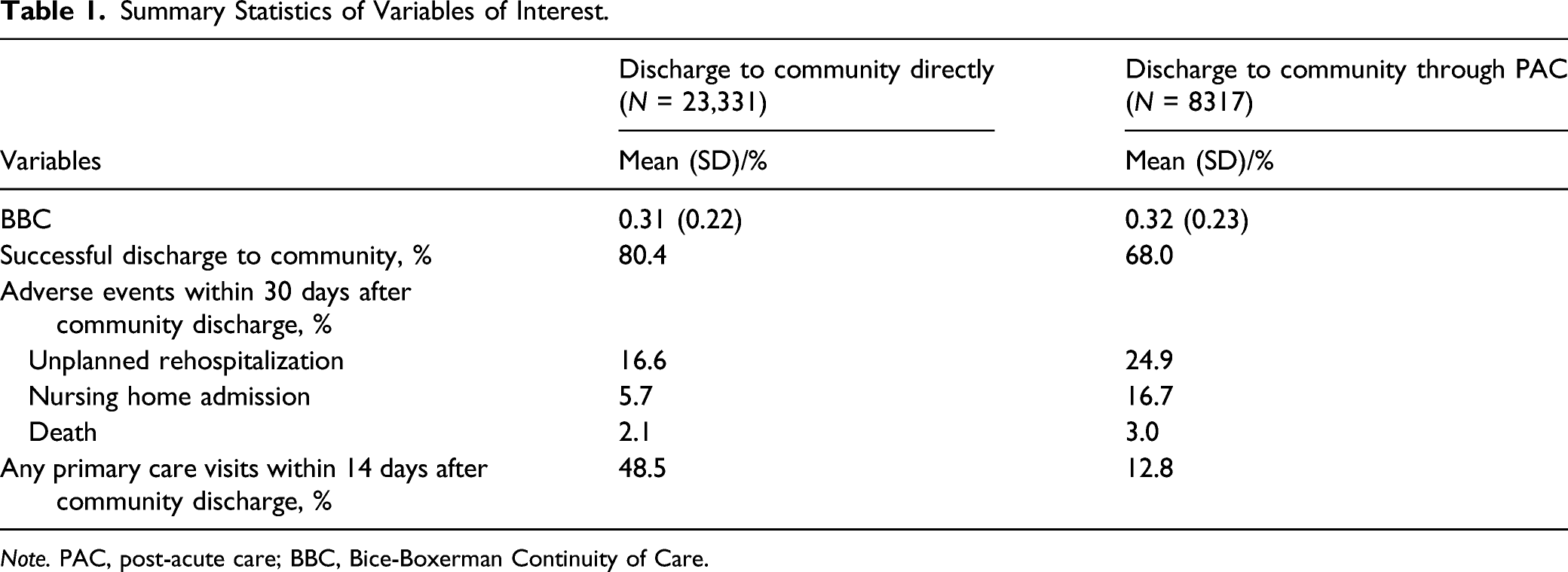
Note. PAC, post-acute care; BBC, Bice-Boxerman Continuity of Care.
Descriptive Statistics of Baseline Characteristics (N = 31,648).
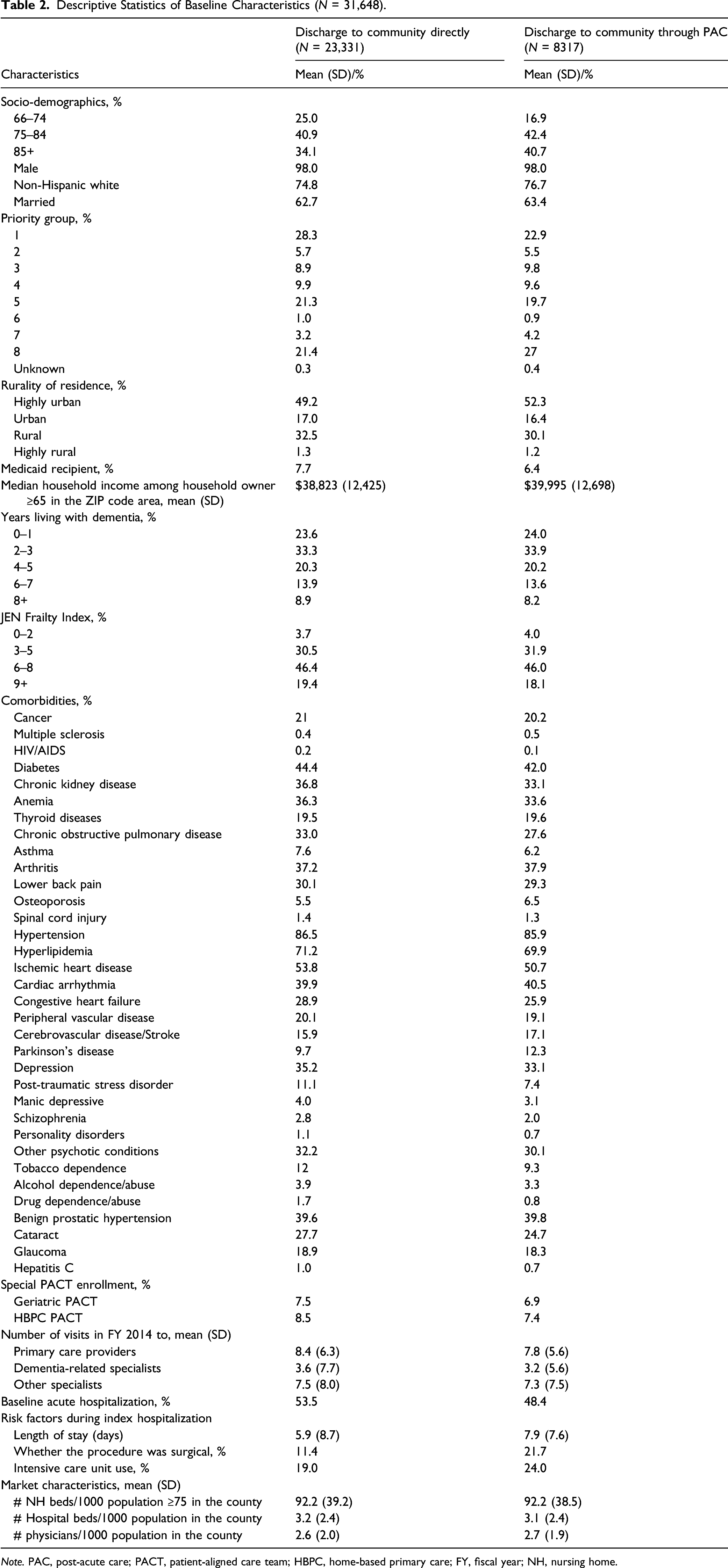
Note. PAC, post-acute care; PACT, patient-aligned care team; HBPC, home-based primary care; FY, fiscal year; NH, nursing home.
Continuity of Care and Successful Discharge to Community.
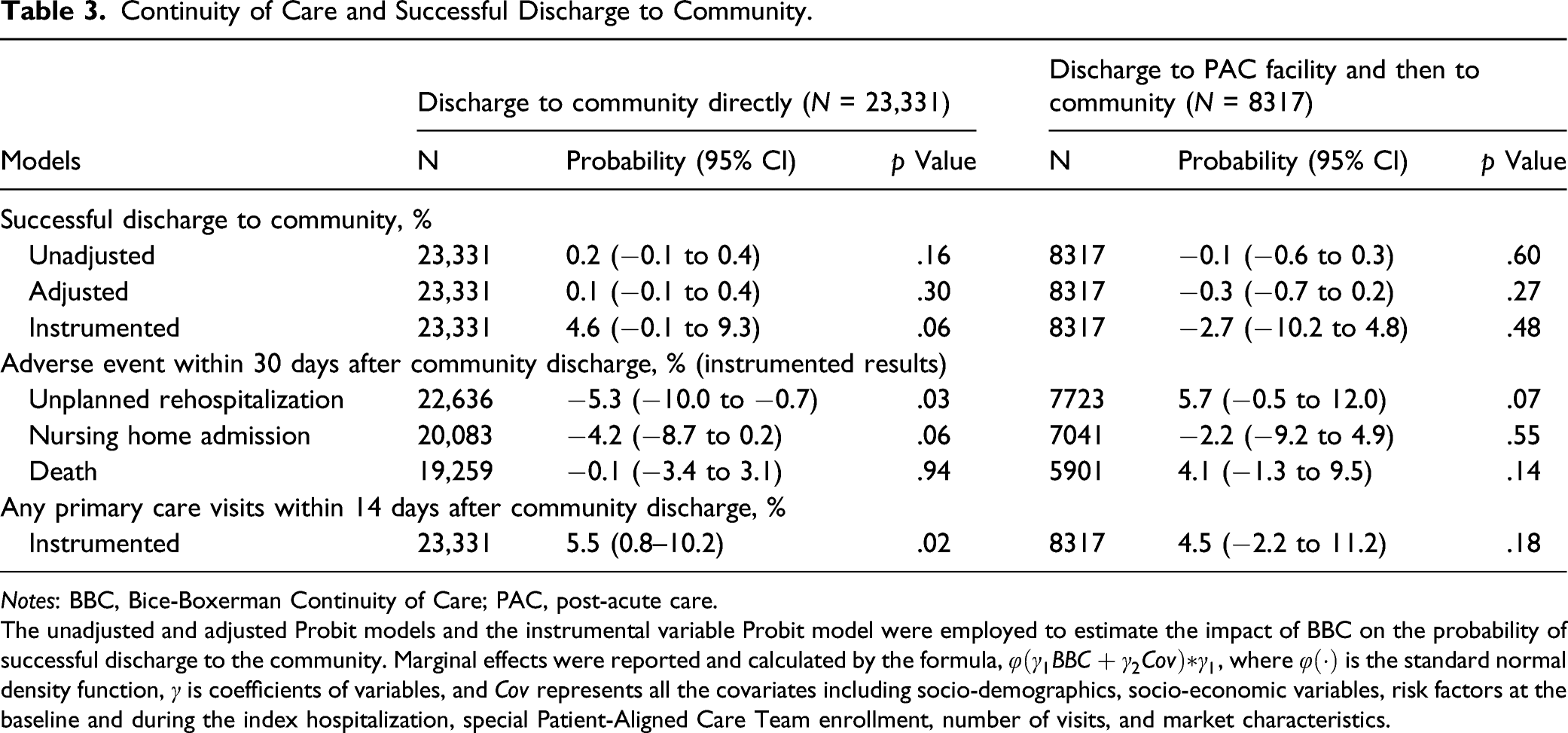
Notes: BBC, Bice-Boxerman Continuity of Care; PAC, post-acute care.
The unadjusted and adjusted Probit models and the instrumental variable Probit model were employed to estimate the impact of BBC on the probability of successful discharge to the community. Marginal effects were reported and calculated by the formula,
A move by more than 10 miles was highly correlated with lower COC (partial F1,23258 = 54, p < 0.01; Supplementary Table 3), indicating that it was a strong instrument. We confirmed that the instrumental variable approach was necessary as the Durbin-Wu-Hausman test of endogeneity was significant for the instrumental variable model (p < 0.1), indicating that standard multivariate regression would result in biased estimates compared with instrumented results. Instrumental variable estimates were much larger than multivariate regression estimates, indicating that the endogeneity arising from unobserved confounders led to an underestimation of the impact of COC on successful discharge to the community. Henceforth, we report only on instrumented results.
When discharged to community directly, veterans with a 0.1 higher BBC were 5.3% (p = .03) less likely to have unplanned rehospitalization and 4.2% (p = .06) less likely to have nursing home admission, but were no more or less likely to die (Table 3). When discharged to community through PAC, veterans with higher BBC were no more or less likely to have nursing home admission or to die, but were 5.7% more likely to have unplanned rehospitalization (p = .07). When discharged to community directly, veterans with a 0.1 higher BBC were 5.5% (p = .02) more likely to have any primary care visits within 14 days of discharge; but BBC had no demonstrable effect when discharge was through PAC.
Sensitivity Analysis—Continuity of Care and Successful Discharge to the Community.
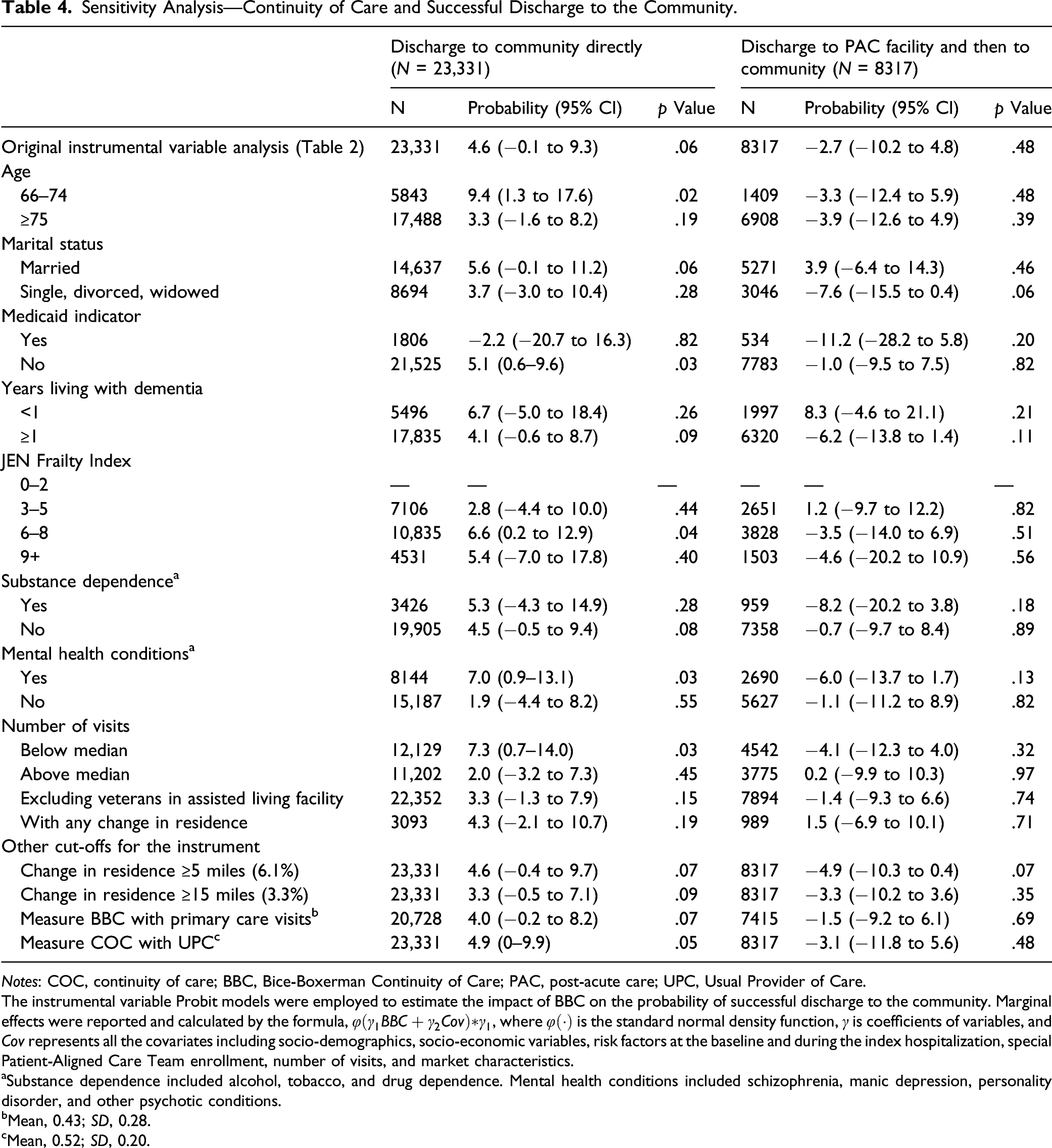
Notes: COC, continuity of care; BBC, Bice-Boxerman Continuity of Care; PAC, post-acute care; UPC, Usual Provider of Care.
The instrumental variable Probit models were employed to estimate the impact of BBC on the probability of successful discharge to the community. Marginal effects were reported and calculated by the formula,
aSubstance dependence included alcohol, tobacco, and drug dependence. Mental health conditions included schizophrenia, manic depression, personality disorder, and other psychotic conditions.
bMean, 0.43; SD, 0.28.
cMean, 0.52; SD, 0.20.
Consistent with the main results, among veterans with community discharge through PAC, BBC had no impact on the probability of successful discharge except among unmarried veterans and with the instrument defined by a change in residence of ≥5 miles.
Discussion and Implications
Using an instrumental variable method this study showed that among veterans with dementia discharged from hospital directly to the community, those with better COC were more likely to be discharged successfully. This result is statistically significant at the 6% level, indicating that there might be 6% chance of a type I error. To provide some perspective of the magnitude of the impact of the change in COC, if veterans in the first quartile of the BBC (<0.16) improved to the median quartile (<0.27), the model estimates that the likelihood of successful direct hospital discharge would increase by 5.1%. Among those discharged to the community through PAC, better COC was not associated with successful community discharge.
Among veterans discharged directly to the community, better COC was associated with a lower likelihood of 30-day unplanned rehospitalization and nursing home admission. These results are consistent with the literature that better COC was associated with lower hospitalization rate (Katz et al., 2015; Lei et al., 2020; Maciejewski et al., 2014; Nelson, Sun, et al., 2014) and lower nursing home utilization (Lei et al., 2021). COC in primary care settings prior to hospitalization may have impacted successful community discharge due to better follow-up by primary care after community discharge by a team knowledgeable of the patient’s conditions that may be more able to provide comprehensive care, addressing patients’ clinical and socio-emotional needs following hospital discharge. Among the study cohort, veterans with higher BBC scores before the index hospitalization were more likely to have any primary care visits within 14 days of discharge, consistent with practice guideline reported to help prevent unplanned rehospitalizations (Brooke et al., 2014; Hernandez et al., 2010; Jackson et al., 2015). By FY 2015, programs to reduce readmissions such as the CMS Hospital Readmission Reduction Program (since FY 2013), and the VHA PACT medical homes (since FY 2014) were established and had initiated programs to limit admissions or readmissions (Boccuti & Casillas, 2015; Nelson, Helfrich, et al., 2014). Many of these programs targeted increased post hospitalization follow-ups by primary care clinicians (Rosland et al., 2013), with uptake more likely among providers to veterans with better COC (Dreiher et al., 2012). Consistent with the literature, COC had no impact on 30-day mortality after hospital discharge (Nyweide et al., 2013). Death within 30 days of inpatient discharge, among a population that does not receive hospice care is likely to be unexpected, thus it is unlikely that COC might play a role in limiting it.
Among veterans discharged to the community through PAC, better COC in primary care settings was not associated with successful community discharge. Veterans with dementia who were first discharged to PAC facilities before returning to the community were older and received more aggressive procedures (e.g., more surgical procedures and intensive care unit use in this study) and thus might have more adverse outcomes regardless of COC before the index hospitalization than those discharged to the community directly. It is also unclear whether following their PAC stay they were more likely to need care by other specialists and not consult with their usual care. Thus, better COC before an index hospitalization may have been less meaningful for them following discharge from PAC. In addition, it is unclear whether and how a patient’s primary care provider(s) or dementia-related specialist(s) are “kept in the loop” about the patient’s health status when they were transitioned to a PAC facility and then discharged from it, primarily if not all the care was provided in VA facilities which have a comprehensive electronic medical record. Last, quality of PAC may contribute to their outcomes after discharge (Neuman et al., 2014). Quality of transition care from nursing homes was only established after 2015 with CMS establishing the claim-based quality measures in 2016 (Abt Associates, 2016), and payment sanctions later, and VHA reporting these measures for its Community Living Centers in 2019 (U.S. General Accounting Office, 2019).
There are several limitations to this study. First, this study focused primarily on male veterans making generalizations to the US population difficult. Exclusion of veterans with less than 3 outpatient visits, who may have less healthcare utilization, also limits the generalizability of our findings. Second, claim-based measures of COC do not measure the quality of care provided in the community and may not reflect patient-provider relationships. However, studies have shown that better COC was associated with better communication (Katz et al., 2014). Third, we could not measure severity of dementia, but we did control for years living with dementia which is likely to be related to dementia severity (Piccininni et al., 2005).
Fourth, we did not have informal caregiver information, which could be a potential confounder because veterans with dementia who have appropriate caregiver support may be more likely to have better COC or veterans might move closer to caregivers who may help arrange the discharge. We conducted sensitivity analyses stratified by marital status, which might be an indicator for social support, with consistent findings among married veterans. Fifth, the instrument was unbalanced on several risk and socio-economic characteristics (age, marital status, Medicaid, years living with dementia, JEN Frailty Index, number of visits, substance use disorder, and several mental health conditions), which might violate the assumption that a move should not be correlated with the outcomes. However, those who moved more than 10 miles were younger, more likely to be unmarried, newly diagnosed with dementia, with lower JEN Frailty Index, and had less outpatient visits (Supplementary Table 2), which indicate the move might not be due to worsen health conditions except for those who were newly diagnosed with dementia and might be more related to the change of family structure and socio-economic status. The sensitivity analyses stratified by these variables resulted in estimates that aligned with the sign of the estimates in the main findings although estimates were not significant in some strata. Another limitation of the instrument is that the low prevalence of move by more than 10 miles (4.3% of the study cohort) might limit the power of the instrumental variable analysis. Six, while we adjusted for many confounders in the analysis, veterans with better COC may have been different from those with worse COC in other unobserved ways when admitted to the hospital.
Last, beginning in 2010, VHA implemented PACTs widely; however, the BBC measure of COC does not distinguish fragmented care from coordinated multidisciplinary team care. For example, if the patient was seen by more than one member of the team, his or her care would be measured as less continuous using the BBC. In addition, in team-based organizations, provider’s multiple team membership might have deleterious effects on treating complex patients (Crawford et al., 2019). Future studies should investigate how to measure COC in teams and whether that continuity is reflected in patient outcomes such as successful hospital discharge.
In conclusion, among community-dwelling older veterans living with dementia, those discharged directly back to the community who had better COC in the year prior to the hospitalization may have impact at improving successful community discharge. These results provide empirical support for efforts to improve COC as a means to reduce transitions after hospitalization.
Supplemental Material
sj-pdf-1-jag-10.1177_07334648211051867 – Supplemental Material for Continuity of Care and Successful Hospital Discharge of Older Veterans With Dementia
Supplemental Material, sj-pdf-1-jag-10.1177_07334648211051867 for Continuity of Care and Successful Hospital Discharge of Older Veterans With Dementia by Lianlian Lei, Shubing Cai, Yeates Conwell, Richard H. Fortinsky and Orna Intrator in Journal of Applied Gerontology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is done as part of the doctoral thesis work at University of Rochester Department of Public Health Sciences and University of Rochester provided financial stipend for doctoral students during the first 2 years in the program.
Informed Consent
University of Rochester (RSRB00072110) and the Department of Veteran Affairs Syracuse VA Medical Center (1251562-6) Institutional Review Board approved this study
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.