
Abstract
Managing the complex care needs of seriously ill patients transitioning from hospital to home can have detrimental effects on family caregivers (FCG). Multi-component interventions tailored to FCG needs are most effective at reducing caregiver burden, distress, and depression. However, gaps exist in determining best methods to assess, document, and analyze intervention components for FCGs. Common methods used to capture patient data during transitions in care may not be appropriate or allowed for FCG needs. As such, we present a methodological approach for electronically capturing, reporting, and analyzing multiple intervention components. This approach uses a standardized terminology and pathway for tailoring intervention components in real time while evaluating intervention effects across time. We use examples from a randomized controlled trial to illustrate the benefits of the current approach for analyzing the effectiveness of multi-component interventions in the context of caregiving research.
• Identifies challenges for capturing data from family caregivers in the context of transitions in care. • Describes emerging study designs that aim to address the heterogeneity of family caregivers and the variability of unmet caregiver needs over the course of a care recipient’s illness.
• Provides a methodological approach for capturing data from multiple component interventions. • Provides an approach for assessing fidelity to the intervention and costs of intervention that may affect future scalability.What this paper adds
Applications of study findings
Hospitalized patients with serious illnesses typically have multi-faceted care plans at hospital discharge that require family caregivers’ (FCGs) support and effort. Family caregivers are often thrust into new responsibilities, including managing medical or nursing care, synthesizing information across multiple settings or providers, and organizing the logistics necessary for a successful transition from hospital to community care providers (Coleman, 2016). With a rapidly aging population in the United States with caregiving needs, attention to FCG interventions is increasing as is the recognition that the burden from these responsibilities affects patient and FCG health outcomes and FCGs’ ability to continue caregiving (Griffin et al., 2022; Hudson et al., 2020).
In spite of the increased recognition, evidence for FCG interventions improving the value of care transitions remains insufficient (Meulenbroeks et al., 2021). This evidence gap is congruent with low strength evidence found in FCG interventions aimed at reducing deleterious effects associated with being a FCG (Butler et al., 2020; Rouch et al., 2021) or at improving patient outcomes (Griffin et al., 2014, 2015). The best evidence to date suggests that multi-component and collaborative care interventions may improve intervention efficacy (Kamermayer et al., 2017; Scott, 2010), but questions remain about which components or combination of components are critical, and what the optimal dose of those components is. Tailoring interventions to meet unique FCG needs has also been cited as essential (Zarit, 2018), but effective tailoring is challenging, due to the heterogeneity of caregiving experience, capacity to provide care, personal health, and caregiving requirements (Bakas et al., 2014).
To address these gaps and challenges, researchers need to diversify the types of study designs they use (Zarit, 2018). While traditional randomized controlled trials (RCTs) test the efficacy and safety of intervention components, adaptive designs, such as Sequential, Multiple Assignment, Randomized Trials (SMART) can test combinations of effective intervention components, doses, and exposures that address individual needs and responses. SMART designs provide a rigorous approach for determining intervention efficacy and can facilitate adoption into routine practice (Lavori & Dawson, 2014; Lei et al., 2012; Mohr et al., 2015; Zarit, 2018).
Whether using RCTs or SMARTs, structuring data collection in ways to help bridge the evidence gaps is critical. In caregiving research, there is a paucity of data collection methodologies that can capture the fluctuation of FCGs needs over time as care recipients’ conditions change or FCGs adjust to transitions in care (Murphy et al., 2007). Data collection methodologies need to be adaptable, yet also foster measurement precision and reliability. In studies examining care transitions, one common approach is to document within the patient’s electronic health record (EHR). However, if the research focus is on the FCG rather than the patient, documentation of FCG needs may not be appropriate or allowed in the patient’s or FCG’s EHR. Moreover, FCG needs documented in the patient EHR are usually in narrative format, unstructured, and relate primarily to patient rather than FCG needs. Family caregiver studies may also be conducted in community or home settings that are not linked to either a patient’s or FCG’s EHR.
We propose an approach for structuring, documenting, and reporting complex, multi-component, FCG interventions that can foster effective evaluation across a heterogeneous population. We draw from experiences implementing this approach in a current RCT being conducted in four Midwestern hospitals with FCGs in three states. Study details are described elsewhere (Holland et al., 2020). Briefly, the RCT’s purpose was to test a nurse-led, multi-component care transitions intervention on the health and well-being of FCGs living in rural or underserved areas and caring for a person who received a palliative care consultation while hospitalized. Using a care pathway, nurse interventionists developed an individualized care plan with/for FCGs by identifying caregiving and personal health problems, assessing problem severity, and creating an intervention scheme to address the identified problems. Care plans were re-assessed routinely over the course of the 8-weeks intervention to address new, emerging, and resolved problems.
Using a standardized approach for documentation, we assessed unmet FCG needs, documented each intervention component delivered to address those needs, and tracked changes in needs and intervention responses over time. This approach provided a mechanism to manage study data and monitor intervention fidelity. It offered an alternative to collecting structured data in spreadsheets or databases or unstructured data (e.g., field notes, narrative notes, charting notes) that require a post-hoc, in-depth content analysis to assess the intervention, dose, and association with outcomes in complex interventions. We were able to capture process data, including time and costs attributable to the intervention, and potential operability challenges, such as internet reliability. Our approach allowed assessment of intervention fidelity and efficacy, tailoring and adaptability, and informed potential challenges to consider in moving from intervention research to implementation into routine care and services.
Documenting and Analyzing Complex, Multi- Component Interventions
Included in our standardized approach is an electronic platform for documentation and utilization of a standardized terminology, both of which allow for documenting, monitoring, and analyzing intervention strategies. In this study, our electronic platform was Nightingale Notes (Champ Software, Mankato, Minnesota, USA), a cloud-based EHR. Nightingale Notes utilizes the Omaha System, a research-based taxonomy that provides a standardized terminology and approach for assessment of patient problems, documentation of services, and evaluation of health and social problems (Holland et al., 2017; Martin et al., 2011). This system is most commonly used by public health agencies to document and track public health interventions, but less commonly used for research.
The Omaha System includes established care pathways, or structured types of care planning that can be utilized for specific problems in clinical or public health practice. Clinicians who follow pathways more consistently adhere to best practices (Martin, 2005; Moreo et al., 2017). In multi-component interventions, pathways can help guide interventionists toward protocols for identified problems and to determine which interventions should be used. They also assure that best practices are used for assessment and care planning.
Caregiver Pathways for Identified Problems, Intervention Categories*, Intervention Targets, and Interventionist Guidance.
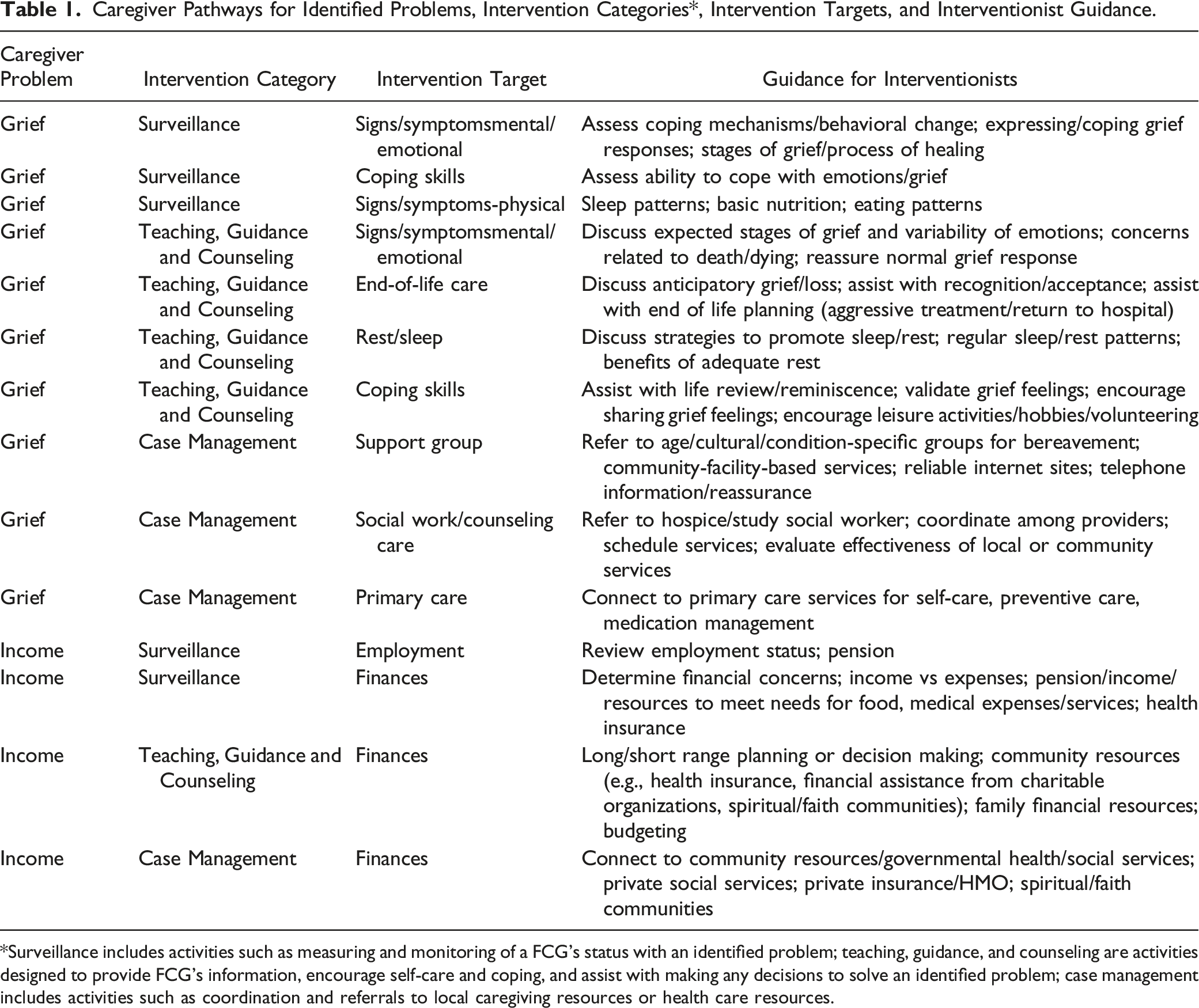
*Surveillance includes activities such as measuring and monitoring of a FCG’s status with an identified problem; teaching, guidance, and counseling are activities designed to provide FCG’s information, encourage self-care and coping, and assist with making any decisions to solve an identified problem; case management includes activities such as coordination and referrals to local caregiving resources or health care resources.
Documenting and Reporting Adaptations by Interventionists
Using a documentation system with standardized terminology allows for interventionists to evaluate how a study participant’s unmet needs (e.g., self-care, patient care) change over time (Holland et al., 2014). Having standardized terminology and taxonomy allows for consistency in how problems and outcomes are defined and assessed. Clearly and accurately documenting study participant problems, use of interventions, and subsequent outcomes in a structured format allows researchers and the interventionists to compare changes in intervention components across predetermined categories both in real time for individual participants and at the study’s conclusion for the study sample.
In the example shown in Figure 1, reports of the interventionists’ strategies can elucidate if teaching FCGs about coping skills has modified grief over time and can inform interventionists if additional efforts or different interventions are needed. An illustrative example is how interventionists modified their guidance in FCG self-care during the Coronavirus 2019 pandemic (COVID-19). Prior to the pandemic, interventionists emphasized the importance of social support and maintaining contact with family and friends to address unmet FCG needs. The pandemic created an urgent need to teach and guide FCGs about balancing the benefits of social support with the risks of viral transmission, especially during post-hospital discharge when infection precautions are paramount. Likewise, interventionists were able to make modifications to their teaching and guidance on social support and grief when visitor restrictions imposed by hospitals and other healthcare facilities affected FCG’s care for the terminally ill and, with death, disruptions in funeral rites. By using data to recognize changes in FCG problems, interventionists could initiate discussions of expected stages of grief and variability of emotions to assist FCGs towards a more effective grief response (Holland et al., 2021). Example of graph monitoring improvements (assessed from 0–5) in knowledge and behavior to manage grief over time among FCGs who received nurse-guided intervention for grief.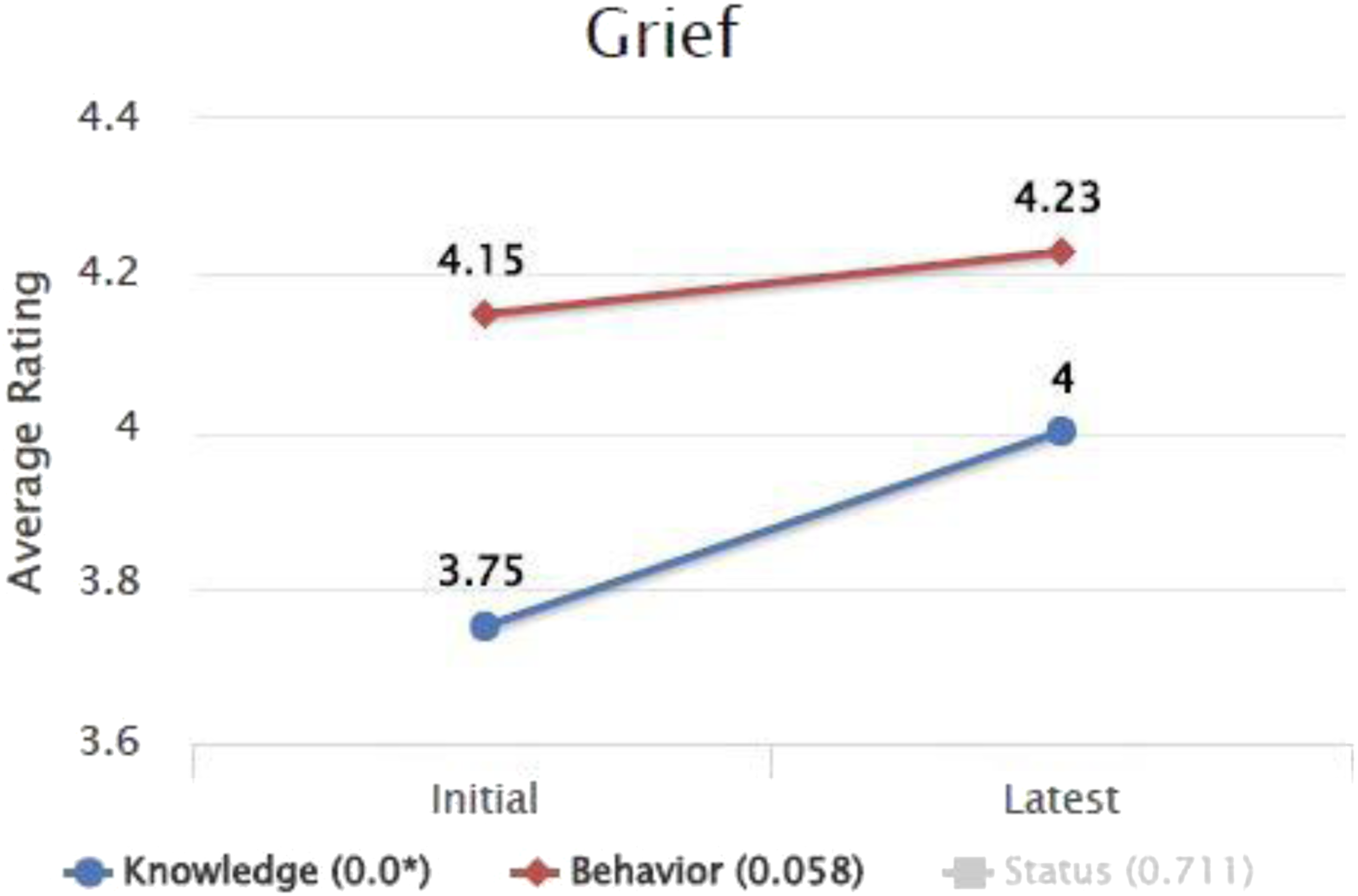
Capturing Time and Costs Efficiently
Using an electronic documentation system allows for more efficient study management. It allowed us to document average time spent with each participant during the intervention and time interventionists spent documenting intervention efforts. Consistent documentation can be used for assessing overall costs of the intervention, return on investment, and cost/benefit analyses. Researchers can calculate and monitor time and costs per intervention strategy. In addition, because there is standardized terminology and depth of information on each intervention target, researchers can analyze which need or cluster of unmet needs requires the greatest intervention time. These data provide essential information about the value propositions if healthcare systems were to adopt and implement a FCG intervention.
Enhancing Intervention Fidelity
A documentation system can also enhance fidelity to a study protocol, which can improve the interpretability of study findings and facilitate translation into practice. Using this system, we created precise reports to monitor fidelity to the intervention, which could then rapidly identify potential protocol deviations. Challenges to intervention fidelity can provide a better understanding of adaptations needed to integrate into clinical practice. Our study intervention, for example, was designed for delivery via video visits. The use of video allows the interventionist to pick-up visual cues that are unavailable from phone calls (Holland et al., 2014). Some encounters, however, were by phone or in-person due to FCG circumstances, changes in the care recipient’s condition, and COVID-19. By reporting the delivery modality of each intervention encounter with FCGs, the study team was able to determine the frequency of non-video visits, their context, and allow for examination of whether other delivery modes affected intervention quality. Because we conducted the study during COVID-19, we were further able to document the increased use and acceptability of video visits.
Challenges
Changing documentation practices from the typical review of a patient’s symptoms and conditions in hospital/clinic narrative notes to a holistic focus on FCG well-being using a structured note can require a concerted shift in perspective. Interventionists experienced a learning curve when they began documenting in the system. We provided training, weekly review of documentation, and then additional training and support when necessary. While narrative notes provide for more open-ended discussion of problems and interventions clinically, they are challenging for research purposes. Finally, purchasing a standardized system may be difficult for small studies, but for larger studies, the efficiency for analysis and methodological rigor it affords can be invaluable.
Conclusion
There is increased recognition of caregiving on patient and FCGs’ well-being and the role FCGs’ have for successful transitional care after hospital discharge (Coleman & Roman, 2015). Most FCG interventions are manualized and tailored to the needs of FCGs, but lack rigorous documentation and reporting of the intervention components, thus limiting our ability to determine which components are efficacious and if ordering and dose affect the efficacy. We suggest a potential approach for addressing this critical gap is documenting and analyzing unmet needs over time, thus providing a system to disentangle the benefits of complex interventions that target FCGs. Using standardized language to assure consistency across interventionists, this approach is time efficient, flexible enough to include multiple intervention components, and allows for time, costs, and process measures to be captured. By using a standardized documentation system, researchers can maintain a research record for the FCG that is independent of both the FCG and patient’s EHRs, comparable across FCGs, and allows for flexibility to structure, document and analyze research intervention components and evaluate their effectiveness.
Footnotes
Acknowledgments
The authors wish to acknowledge Jodie Cogswell and Meghan Ryan for their assistance with this manuscript and to the family caregiver participants in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is funded by the National Institutes of Health, National Institute of Nursing Research - NIH-NINR R01NR016433.
IRB Statement
This manuscript does not include participant data; however, the reflections presented in this paper are based on a study that does include participant data. The study protocol was reviewed and approved by The Mayo Clinic Institutional Review Board (17–005188).