
Abstract
This study explored nursing home social services directors’ interest in pursuing trauma-informed care (TIC) training, and individual and organizational characteristics associated with their interest. Data from the 2019 National Nursing Home Social Services Directors Survey, a national cross-sectional survey, were used. Measures sought information on participants’ interest in TIC training, sociodemographic characteristics, and characteristics of employing nursing homes. Descriptive statistics and multivariate binary logistic regression analyses were used. Of the 924 respondents, 880 (95.2%) were included in the analysis. Most (71.7%) expressed high interest in TIC training. Younger age, fewer years of nursing home social services experience, being degreed and licensed in social work, and being a person of color were associated with greater odds of high interest in TIC training. Neither nursing home ownership nor social services staffing ratio was significantly associated with interest in TIC training. As policy requires TIC in nursing homes, these findings present a first step towards understanding implementation.
• Social services workers play essential roles in behavioral health and the implementation of trauma-informed care (TIC) in nursing homes, yet not all social services workers are interested in training in TIC. • Individual characteristics are associated with interest in training, so nursing homes should find ways to ensure all social services workers receive appropriate training on TIC. • This paper adds considerations for nursing homes, who are now required to implement TIC, on the preparedness of their behavioral health workforce for implementation.
• Social services directors of all backgrounds should themselves receive training in TIC to allow them to provide or coordinate TIC implementation in their nursing homes. • Nursing home leadership should promote TIC training for social services directors and staff who can be instrumental in introducing and maintaining a TIC perspective in interactions with residents, families • More research is needed to detail the necessary preparedness and effectiveness of social services directors for TIC.What this paper adds
Applications of study findings
Introduction
Over 15,000 nursing homes provide long-term care to almost 1.4 million older Americans (Harris-Kojetin et al., 2019) each year. Ninety-five percent of these organizations receive funding through Medicare and/or Medicaid (Harris-Kojetin et al., 2019). The Centers for Medicare and Medicaid Services’s (CMS) Requirements for Participation, updated in 2016, provide minimum standards to ensure residents “attain or maintain the highest practicable physical, mental, and psychosocial well-being” (Behavioral Health Services, 2016). This update added emphasis on behavioral health care by requiring nursing homes to provide trauma-informed care (TIC). Trauma-informed care acknowledges the widespread prevalence of potentially traumatic experiences in the population, and seeks to provide health and social services in ways that do not retraumatize clients, or in the case of nursing homes, residents, thus relieving distress. Although no one’s discipline is solely responsible for providing TIC, as key providers of behavioral health services in nursing homes, social services directors often bring these initiatives to fruition and optimize care. However, they themselves may not have the knowledge needed to assist with TIC, given disparate educational preparation. It is critical, then, to broaden the understanding of social services directors’ interest in pursuing training in this area.
Trauma and Trauma-Informed Care
Although TIC has reached consensus on viewing trauma in a psychological context, there exists an abundance of definitions in varying degrees of alignment. For instance, the American Psychiatric Association (2013) conceptualizes trauma solely within the pathological context of posttraumatic stress disorder as the exposure to actual or threatened death, serious injury, or sexual violence alongside the presentation of various symptoms (Posttraumatic Stress Disorder). Alternatively, the Centers for Disease Control, 2022 endorses a developmental view by focusing on trauma events constituting adverse childhood experiences (e.g., abuse and neglect, household instability, and parental separation) may extend into adulthood (What Are Adverse Childhood Experiences?). Finally, the Substance Abuse and Mental Health Services Administration (SAMHSA, 2014) broadens these previous definitions by referring to harmful or otherwise threatening events or circumstances with lasting negative impacts on an individual’s functioning or well-being (What Is Trauma?). Although these potentially competing definitions may complicate the streamlined operationalization of trauma in research, the emphasis in TIC is not so much to arbitrate traumatic experiences, as it is to address their effects on individuals in need of care.
Around 70% of adults report having been exposed to traumatic events (Benjet et al., 2016). Such exposure can have deleterious and lasting effects on both physical and mental health (SAMHSA, 2014). Moreover, new traumas that occur in later life may compound pre-existing trauma histories (Maschi et al., 2013), exacerbating the risks confronting older adults. Care systems that interface with older adults may themselves present risks for late-life trauma exposure. Nursing homes, in particular, may promote re-traumatization through hierarchical power structures relegating residents to positions of decreased agency. Re-traumatization also may occur when care practices may threaten residents’ sense of security, such as through physical restraints or negative interpersonal experiences with staff (Robins et al., 2005).
Centers for Medicare and Medicaid Services introduced TIC to address pre-existing trauma in long-term care and to reduce the risks of new trauma resulting from care (Behavioral Health Services, 2016). Trauma-informed care is a strengths-based approach that foregrounds knowledge of trauma in the provision of health care allowing effective responses to existing trauma histories and decreasing the risk of re-traumatization (Hopper et al., 2010; SAMHSA, 2014). Trauma-informed care uses a collaborative model that recognizes individuals as experts in their care (Hopper et al., 2010). Organizations subscribing to TIC require that staff espouse a holistic understanding of trauma and are prepared to consider the role of trauma in the way services are received (SAMHSA, 2014).
Social Workers as Providers of Trauma-Informed Care in Long-Term Care
Trauma’s standing as a behavioral health issue aligns with social workers’ professional training and scope of practice (Council on Social Work Education [CSWE], 2018). Social workers are trained to approach behavioral health from a systems framework, using person-in-environment and life course perspectives. The concordance between this approach and trauma theory (Kusmaul & Anderson, 2018) suggests that social workers are well equipped to lead efforts integrating TIC into clinical practice (Levenson, 2017). Research has shown that nursing home social workers occupy important roles in delivering behavioral health care (Bern-Klug et al., 2018) and are instrumental in optimizing residents’ health (Kane, 2015).
However, disparity in social services directors’ training may result in disparities in preparedness for TIC. Nursing homes provide social work services through (a) qualified social workers, (b) social work paraprofessionals, and (c) interdisciplinary care teams that include social workers (Roberts & Bowblis, 2017). Although degreed and licensed social workers may be the most adequately prepared to respond to behavioral health needs, policy standards invite flexibility. For instance, nursing homes must staff qualified social workers only if they contain 121 beds or more (Administration, 2016), meaning that the 70% of CMS-certified nursing homes with fewer than 121 beds (Bern-Klug et al., 2021) are not required to staff qualified social workers.
This proviso further stipulates that “qualified social workers” need not hold a degree in social work (Administration, 2016). The 2016 Final Rule (Requirements for Long Term Care Facilities, 2016) revision further de-professionalized nursing home social work (Bern-Klug et al., 2016, 2018) by expanding the list of related fields that qualify. This expansion may contribute to decreased quality of care (Steketee et al., 2017) by increasing the number of nursing homes wherein social services staff are not degreed in social work. Thus, although the training social workers receive uniquely positions them to respond to trauma-related needs (CSWE, 2018), only 37% of nursing home social services directors are degreed and licensed in social work (Bern-Klug et al., 2021), meaning that the level of TIC offered to residents may vary.
The Current Study
The 2016 Final Rule (Requirements for Long Term Care Facilities, 2016) mandating the inclusion of TIC was the largest federal nursing home policy change since 1987 (Bern-Klug et al., 2016). However, research has not yet explored nursing home social services directors’ preparedness in implementing these policy changes, particularly insofar as TIC. In response, the current study addressed the following research questions (RQs):
Method
Design
This cross-sectional study used data from the 2019 National Nursing Home Social Services Directors Survey. Based on a similar study from 2006, the 2019 National Nursing Home Social Services Directors Survey sought a nationally representative sample of nursing home social services directors to describe this workforce at the national level and to examine their occupational responsibilities and training needs (Bern-Klug et al., 2021). The study used publicly available CMS Nursing Home Compare data, which contain the names and contact information for all nursing homes certified by Medicare and/or Medicaid as their sampling frame. In January 2019, Dr. Bern-Klug downloaded the December 2018 Annual File (Centers for Medicare & Medicaid Services, 2018), which was the most current version available at that time, and drew a simple random sample of 3650 of the 15,578 total nursing homes (23.4%).
Sampling Procedures
Recruitment occurred in the spring of 2019. Researchers called selected nursing homes to assess study eligibility. For inclusion in the study, nursing homes needed to employ at least one social services staff person at least part-time. Additional nursing homes were excluded if (a) they were actively hiring social services staff, (b) their social services director was on leave, (c) their phone number was disconnected or incorrect, (d) they did not answer the recruitment phone call after three attempts, or (e) their calls went directly to voicemail. Using these criteria, 583 (16.0%) nursing homes were eliminated, leaving 3067 nursing homes.
Based on the information obtained from the phone calls, the research team emailed a link to the Qualtrics survey to social services directors for whom they had an email address. If no email address was provided or if there was no response to the email, they mailed the social services directors a paper questionnaire containing a study identification number and a postage-paid return envelope. Participants provided electronic or written informed consent. Participation was not compensated.
A total of 924 of the invited 3067 social services directors returned surveys (response rate = 30.1%). We excluded 12 surveys (1.3%) for not meeting the ≥50% threshold for survey completion based on responses to all items. Following inspection of the remaining 912 cases, we employed listwise deletion to account for missing data (n = 32, 3.5%; Graham, 2009) across five key measures (range = 1.0%–1.4% missing per variable), producing the final analytic sample size (N = 880 [Qualtrics: n = 493, 56.0%; paper: n = 387, 44.0%]). The Human Subjects Office at [Affiliation] approved all study procedures.
Participant Characteristics
Participant Characteristics.
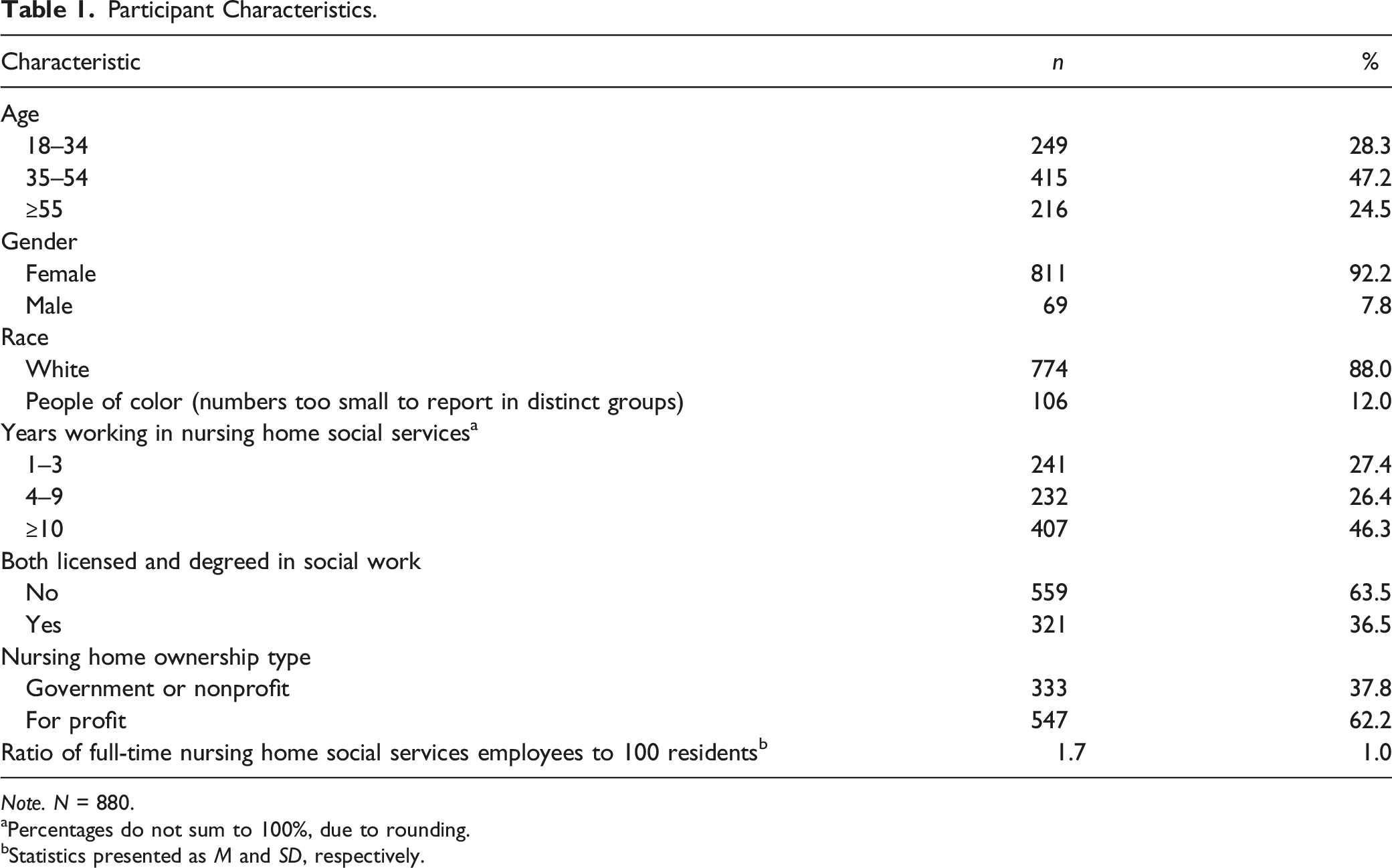
Note. N = 880.
aPercentages do not sum to 100%, due to rounding.
bStatistics presented as M and SD, respectively.
Questionnaire
The questionnaire participants completed contained 185 items, assessing the extent to which participants’ respective social services department addressed 46 different tasks (Bern-Klug et al., 2021) outlined by the National Association of Social Workers and the Veteran’s Health Administration. Although unavailable for paper questionnaires, Qualtrics-based questionnaire completion lasted an average of 45 minutes. Data derived from paper surveys were double entered to enhance accuracy (Barchard & Verenikina, 2013).
Measures
All measures consisted of researcher-constructed single items.
Dependent Variable
Independent Variables
Individual characteristics were self-reported by participants, and included age, gender, race, years working in nursing home social services, and a composite variable assessing social work degree and licensure status. All were collected as categorical variables. Small cell sizes prompted further collapsing age (18–34, 35–54, ≥55), race (White, people of color), and years working in nursing home social services (1–3, 4–9, ≥10). As no participants endorsed a gender outside of male or female, gender was treated dichotomously. Participants indicated their highest level of education and whether they were licensed or certified in social work, but it was unclear how useful these responses were, as many respondents without social work degrees indicated they were certified or licensed (some states allow non-degreed social workers to be certified). To address these data inconsistencies, we computed a composite social work degree–license variable from individual variables assessing whether participants (a) had a Bachelor of Social Work degree, and/or (b) had a Master of Social Work degree, and (c) were licensed or certified to practice social work.
Organizational characteristics included nursing home ownership type and the ratio of full-time nursing home social services employees to residents. Nursing home ownership type was drawn from the December 2018 Annual File (Centers for Medicare & Medicaid Services, 2018). This variable was dichotomized (not-for-profit
Analytic Strategy
We conducted all analyses in IBM SPSS (Version 25), using a two-tailed p value of .05. Univariate statistics were conducted to describe the sample and to answer RQ1. Bivariate and multivariate analyses were employed to answer RQ2 and RQ3 in unadjusted and adjusted frameworks, respectively.
Unadjusted bivariate analyses included a series of Pearson chi-square tests of independence (age, gender, race, years working in nursing home social services, license and degree status, nursing home ownership type) and an independent samples t test (ratio of full-time nursing home social services employees to residents). We fit a multivariate binary logistic regression to test the adjusted associations between social services directors’ interest in pursuing TIC training and the aforementioned independent variables. Analytic assumptions for multivariate binary logistic regression (Mertler & Vannatta Reinhart, 2017, Chapter 11) were verified.
Results
How Interested Are Nursing Home Social Services Directors in Pursuing TIC Training?
Descriptive results indicated that 71.7% (n = 631) of the sample expressed high interest in pursuing TIC training (moderate interest: n = 255, strong interest: n = 376). Conversely, 28.3% (n = 249) of the sample expressed low interest in pursuing TIC training (no interest: n = 104, minor interest: n = 145).
Which Individual and Organizational Characteristics Are Significantly Associated With Nursing Home Social Services Directors’ Interest in Pursuing TIC Training?
Bivariate
Bivariate Analyses of Interest in Pursuing Trauma-Informed Care Training.
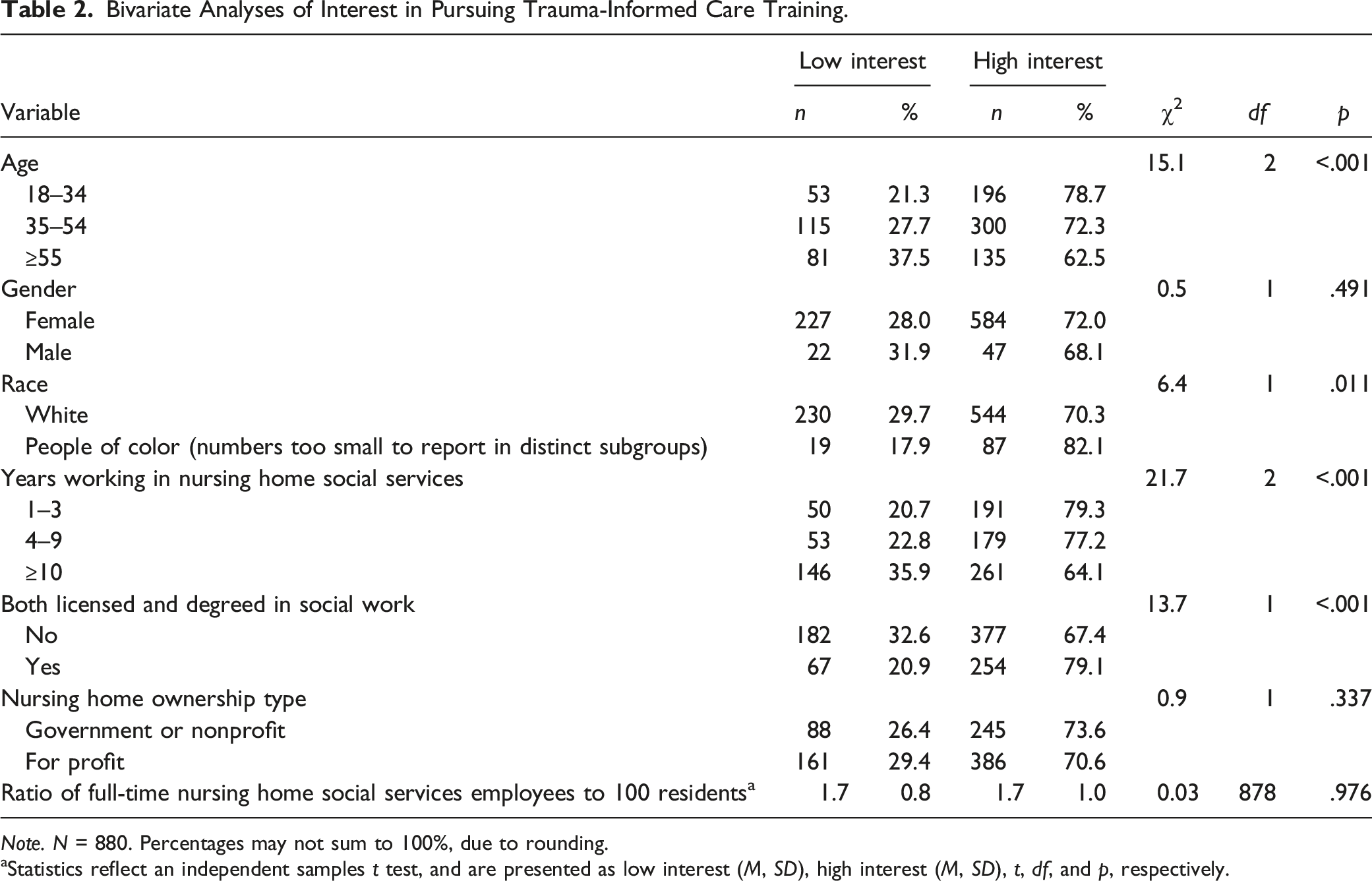
Note. N = 880. Percentages may not sum to 100%, due to rounding.
aStatistics reflect an independent samples t test, and are presented as low interest (M, SD), high interest (M, SD), t, df, and p, respectively.
Multivariate
Multivariate Binary Logistic Regression Classification Table.
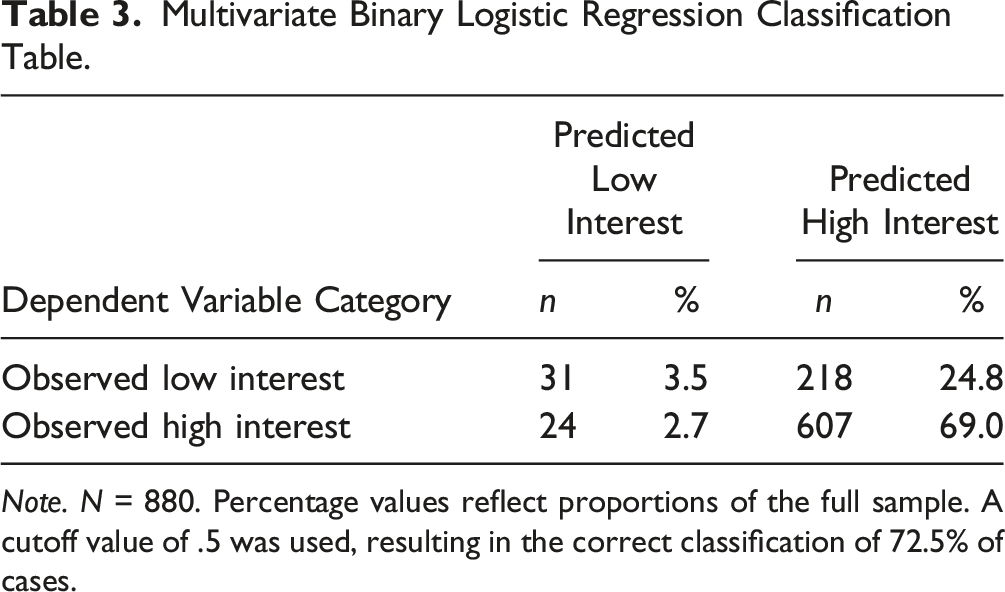
Note. N = 880. Percentage values reflect proportions of the full sample. A cutoff value of .5 was used, resulting in the correct classification of 72.5% of cases.
Multivariate Binary Logistic Regression Results of High Interest in Pursuing Trauma-Informed Care Training.
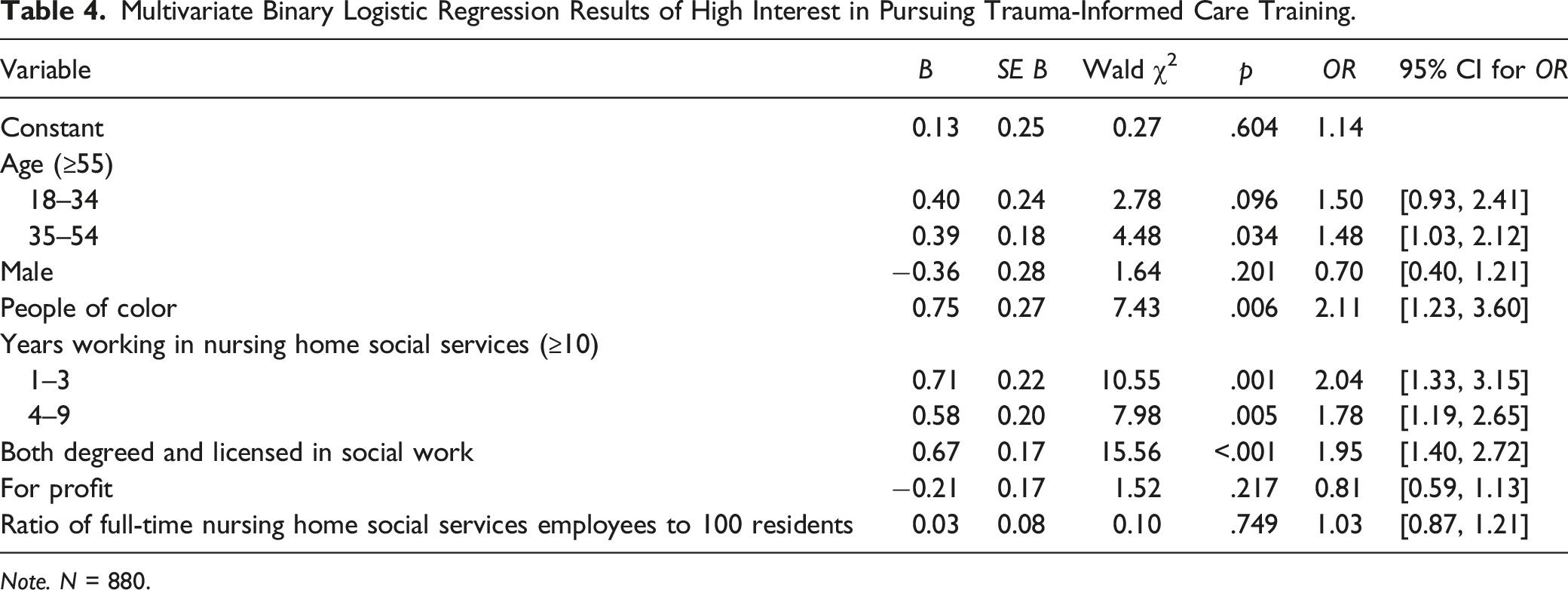
Note. N = 880.
Discussion
This study examined nursing home social services directors’ interest in pursuing TIC training in the context of individual and organizational characteristics. Federal regulations require nursing homes to implement TIC. In many nursing homes, this responsibility would fall to the social services department, because of its relationships to psychosocial care. It is important for nursing home residents who may have past traumatic experiences and are vulnerable to new trauma, to receive care in an environment that understands and practices trauma-informed care. Social services workers have behavioral health services responsibilities in nursing homes, and thus have the potential to play key roles in TIC implementation. We found that the majority of the social services directors in our study expressed a high interest in pursuing TIC training. The directors’ individual characteristics better predicted respondents’ interest in pursuing TIC training than the characteristics of the organizations for which they worked. Without further information, we can view this interest in TIC training in one of two ways: (a) an interest in training reveals a lack of sufficient previous training and/or (b) an interest in training recognizes the importance of TIC, thus, prompting a desire for increased information.
Not all nursing home social services directors are social workers, because regulations do not require them to be. Our results found that participants who were both degreed and licensed in social work had significantly higher odds of expressing a high interest pursuing TIC training. This finding was expected because of the emphasis on behavioral health within social work training (Kusmaul & Anderson, 2018; Levenson, 2017). In this sense, nursing home social services directors who are both degreed and licensed in social work may be better candidates to incorporate CMS’s trauma-related initiatives into clinical care than those who meet CMS’s standards for “qualified social workers” despite lacking degrees and licenses in social work (Requirements for Long Term Care Facilities, 2016). We recommend that the requirements for social work training for nursing home social workers be strengthened, and that beyond that, nursing homes choose to hire degreed social workers because their training contributes to behavioral health care.
We found that participants who were younger and participants who were newer to working in nursing home social services reported higher interest in pursuing TIC training. We suspect that these findings may be related to recent trends: TIC has enjoyed increased educational (Boel-Studt et al., 2022) and clinical (Bruce et al., 2018) attention as of late. Thus, this age-related interest may reflect broader awareness of trauma in recent years and thus of the potential benefits of implementing TIC in nursing homes.
As the strongest relationship identified in our model, results also revealed that people of color (in this case, participants identifying as a race other than White) showed significantly higher interest in pursuing TIC training than participants identifying as White. It is possible that this increased interest is related to the greater trauma experienced by people of color in the United States due to overt racism and microaggressions (Sullivan et al., 2021), and higher rates of PTSD experienced by adults and older adults in some visible minority groups (Davison et al., 2021). Considered in conjunction with age, this finding indicates that TIC interest varies by some—but not all (e.g., gender)—sociodemographic characteristics. More research is needed to explicate the processes underlying these differential findings.
The finding that neither of the organizational characteristics we considered was associated with interest in TIC training was unexpected. Ownership status consistently is associated with nursing home quality (Shippee et al., 2020). We suspect that ownership status may be associated with person-centered culture, which may influence how successful a facility is at implementing TIC, but it was not associated with individual social services directors’ interest in TIC training. The ratio of social services staff to residents considers the fact that there may be differences in staffing at nursing homes above or below the “120-bed rule” regulation, but also was not associated with social services director interest in TIC.
Limitations
Findings should be considered with respect to study limitations. First, our study’s cross-sectional design precludes inferring causal mechanisms. Additionally, despite the study’s probability sampling approach and the finding that the study sample resembled the population sample (Bern-Klug et al., 2021), our low response rate (30.1%) may subject our results to nonresponse bias. Furthermore, the self-report data collection mechanism, coupled with the growing attention to TIC, may have biased participants’ responses through social desirability. Finally, our model fit was questionable (Mertler & Vannatta Reinhart, 2017, Chapter 11) and the Nagelkerke-R2 was low, indicating other factors may play stronger roles in TIC training pursuit interest. The survey did not contain all the items we would have liked to consider. For example, we did not have the data to calculate staffing ratios separately for long-term care versus subacute residents, which can significantly impact the time available for training.
Conclusion and Implications
This study is one piece of a larger effort regarding TIC implementation in nursing homes. An important part of actualizing this implementation includes supporting those charged with deploying emerging initiatives through education and training. Social services directors may be tapped to provide organization-wide education on TIC. If they lack knowledge in this area, their employing nursing homes may miss a key link in their TIC implementation. To this end, ongoing coaching could help organizations address concerns that arise as new, trauma-informed cultures are implemented.
Trauma theory posits that traumatic experiences affect individuals long-term by disrupting their development. TIC is important in nursing homes due to commonly shared experiences in late life, such as life review. From a theoretical perspective, it would be important to understand the impacts of TIC on older adults and their developmental experiences in nursing homes. To do so requires increased knowledge about TIC implementation, as well as advances in measurement.
There are many questions that remain regarding TIC implementation in nursing homes, such as, “to what extent are certified nursing homes providing TIC training to their staff?” “Who on staff is responsible for the training?” “What support is available to the staff responsible for training?” “How effective is the training?” “Have nursing homes altered their policies and procedures to better reflect TIC perspectives?” “Who or what led to the changes?” “How can we strengthen TIC in nursing homes?” Beyond that, future research should consider specific roles social services directors play in TIC implementation and the types of organizational supports, both internal and external, which foster these roles. Additionally, given that these data were collected prior to the rise of COVID-19, just weeks after the TIC requirement went into place, it is likely that many nursing homes had not begun TIC implementation. Thus, future research should also consider these roles with respect to the unique trauma confronting nursing home residents posed by COVID-19.
Footnotes
Author’s Note
IRB/Human Subjects approval was provided by the University of Iowa’s Human Subjects Office, IRB # 201810727.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for 2019 National Nursing Home Social Services Directors Survey data collection was provided by the Retirement Research Foundation for Aging to Mercedes Bern-Klug, PhD, MSW, FGSA at the University of Iowa.