
Abstract
One in four older adults has Behavioral Health (BH) concerns, and over 63% are not receiving services. Older adults living in the community depend on the aging network for home- and community-based services and care managers are critical providers in this network. However, most care managers' current education and training are inadequate to care for older adults with BH needs. This study evaluated the effectiveness of training on the perceived self-efficacy of care managers working with older adults with BH needs. The study used a quasi-experimental design with a pre- and post-test approach and convenience sampling (n = 90). We found a significant difference in mean self-efficacy scores, from pre-test (M = 62.31, SD = 10.11) to post-test (M = 65.88, SD = 7.40) related to working with clients with mental health problems. In addition, we found a significant difference between the mean pre-test (M = 59.81, SD = 10.68) and post-test score (M = 65.60, SD = 9.85) related to working with clients with substance use problems.
• This study begins to fill a gap in research on training as an intervention to improve mental health services among older adults. • We found that The BU CADER training course increased the mean self-efficacy score among care managers working with older adults with mental health and substance use problems. • This study makes significant contributions regarding the impact of training to increase self-efficacy.
• The findings from this study have important implications for the role of care managers and the provision of mental health services for older adults. • Care managers who work with older adults represent a valuable workforce within the aging care network and can help meet the critical needs of older adults living in the community. • The training could be delivered to providers in the aging networks. As the study revealed, past training in mental health and/or substance use issues was not a predictor of higher perceived self-efficacy, which suggests that even newly employed staff with previous training may benefit from the course.What this paper adds
Applications of study findings
Introduction
The older adult population is projected to grow, with an estimated one in five being over the age of 65 in the United States (US) by 2030 (U.S. Census Bureau, 2020a). Older adults 65 years of age and over often experience chronic conditions associated with age and a higher incidences of behavioral health problems [BH] (the term BH is used to describe both mental health and substance use) (Institute of Medicine, [IOM], 2012, Maresova et al., 2019) compared to younger populations, with one in four older adults experiencing some mental disorders, such as depression and anxiety. In addition, behavioral health issues among older adults are associated with negative outcomes, including increased emotional distress, mortality, suicide, hospitalization, and nursing home placement, as well as higher healthcare costs (Brown & Wolf, 2018; Kunik et al., 2017; Kułak-Bejda et al., 2021). However, an estimated 63% of older adults with BH issues do not receive the needed services (Pan American Health Organization, n.d; Byers et al., 2012; Mongelli et al., 2020). This need for behavioral health services among older adults, combined with the growing, aging U.S. population is concerning given that the number of trained BH providers is insufficient to meet the demand (Everett, 2019; Substance Abuse and Mental Health Services Administration [SAMHSA], 2019).
About 97% of older adults in the U.S. live at home (U.S. Census Bureau, 2020b), and the majority depend on the aging network such as Aging Services Access Points (ASAPs) for community-based long-term support (Roberts et al., 2018). ASAP’s are private non-profit agencies with governing boards that serve and represent 51% of people age 60 and older. ASAPs were established under Chapter 19A of Massachusetts General Laws (Mass.Gov, 2022) and are equivalent to what is nationally known as Area Agencies on Aging (AAA).
Older adults living in the community are at higher risk of institutionalization when their behavioral health needs are unmet (Tilly, 2016). As Baby Boomers continue to age and require services, the aging network will significantly influence the health, mental health, and overall well-being of this population (Muttillo, 2019). Although systems are in place to provide referrals to behavioral health services, they may not always be available, particularly for those who cannot leave their homes. Additionally, a lack of geriatric behavioral health providers could also prevent older adults from accessing services (Kunik et al., 2017). Therefore, there is a documented need for community-based, evidence-based, and innovative services to address the mental health needs of aging adults (Kunik et al., 2017; SAMHSA, 2019, Executive Office of Elder Affairs, 2018–2021-2025 plan).
There is little guidance on what core knowledge is required for a workforce to address the complex behavioral health needs of older adults, or how much training is needed for the care managers working with this population (Hinrichsen et al., 2018; Lehmann et al., 2017). The complex interactions of behavioral health conditions with the physical, cognitive, and functional impairments common among older adults require a workforce with specific competencies and the ability to operate within a larger care team (Institute of Medicine, 2012). Hence, Kunik et al. (2017) and the Substance Abuse Mental Health Service Administration (SAMHSA) (2016) recommend training non-licensed providers to assess, screen, and deliver behavioral health services for older adults.
Care managers are healthcare professionals who serve as patient advocates to support, guide, and coordinate care for patients, families, and caregivers as they navigate their health and wellness journeys, and in the aging network, can help meet the demand for behavioral health services for older adults. (Case Management Society of America, n.d). In the aging network, a care manager acts as the broker for service delivery between the client and the services needed (Mass.gov, 2020). In ASAPs in the state of MA, the required qualifications for care managers include BA/BS in social work, human services or a related field. An Associates Degree with significant relevant work experience may be substituted for a portion of degree (Agespan, n.d; Mystic Valley Elder Services, n.d; Springwell Elder Services, n.d. and other); hence, their education and training may not prepare them to work with an older adults’ complex behavioral health needs (Joo et al., 2019). However, if properly trained, care managers can provide supportive behavioral health services to older adults living in the community (BU-CADER, 2017b).
Confidence in job performance or perceived self-efficacy influences self-development, adaptation, and performance outcomes (Bandura, 2012; Jiang et al., 2018). Hence, researchers suggest that non-licensed professionals should not just focus on clinical skills but also competence and confidence in their ability to perform a job (Kunik et al., 2017). Research in this field is important and timely because the population of older adults is growing, the percentage of this population with BH needs is increasing and access to services for these BH needs is limited, so it is important to have care managers trained and confident in their ability to work with this population with this need.
This study was grounded in Social Cognitive Theory (SCT). SCT includes the constructs of self-efficacy and behavioral capabilities that have been documented as important for improving work performance and increasing motivation over time (Consiglio et al., 2016). People with high perceived self-efficacy are more likely to engage in tasks that are challenging, expend effort, persist until they overcome difficulties, and perform at higher levels than those with low perceived self-efficacy (Bandura, 1997).
The purpose of this study was to investigate the impact of a training intervention on perceived self-efficacy among care managers working with older adults with behavioral health needs. The overarching research question was: To what extent does participation in a training intervention on behavioral health increase the perceived self-efficacy of care managers working with older adults with behavioral health needs? The study had two aims. The first was to evaluate the effectiveness of a training intervention on the perceived self-efficacy of care managers working with older adults with behavioral health issues. We hypothesized that perceived self-efficacy would be higher at post-test compared to pre-test. Due to the lack of research on improving self-efficacy through past training, the second objective was to examine differences in perceived self-efficacy training intervention between care managers with prior behavioral health training (pre-test–post-test) compared to care managers without prior behavioral health training.
Methods
We used a quasi-experimental study design with pre-test–post-tests. The dependent variable was self-efficacy, and the independent variable was the training intervention. The intervention for the study was a behavioral Health in Aging online course created by the Center for Aging and Disability Education and Research (CADER) at Boston University School of Social Work. The CADER Mental Health in Aging training has demonstrated positive outcomes for competency-based learning (skills and knowledge) for both non-licensed and licensed health and social service professionals (CADER, 2017a, 2017b, 2017c). However, to our knowledge, it has not been assessed for effectiveness in increasing perceived self-efficacy. The research study took place at one of the 25 Aging Services Access Points [ASAP] in Massachusetts.
To ensure treatment compliance, training was provided with both asynchronous and synchronous components as described in the training manual. As the study was conducted during COVID-19, the synchronous component was conducted via Zoom although synchronous training can also take place in person. BU CADER provides an in-person training manual to accompany the online training that has clear content for discussions and case vignettes for role-playing, which allowed participants to receive informative feedback and guided modeling. The online course and in-person training manual are available through BU CADER and can be easily replicated for use by other researchers and trainers.
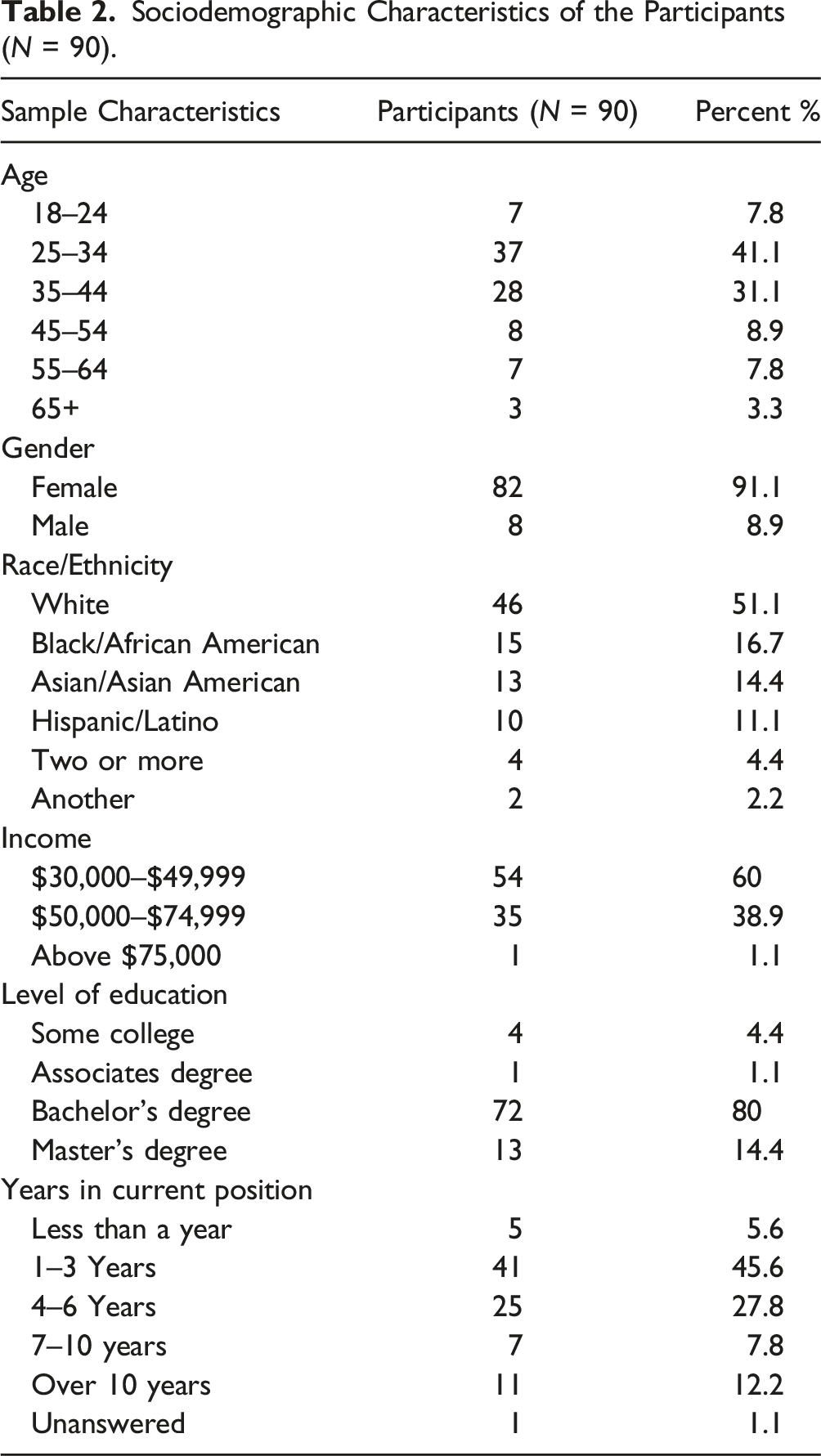
The target population for the study was care managers who work at the ASAP with older adults aged 60 and over. Convenience sampling was used for the study. We conducted a Power analysis for a paired sample t-test, with a desired sample size of 83. At the time of recruitment, there were 104 care managers who were eligible to participate in the study, however, due to staff turnover only 90 participants participated. Fourteen care managers had left the agency.
Case Manager Personal Efficacy Scale.
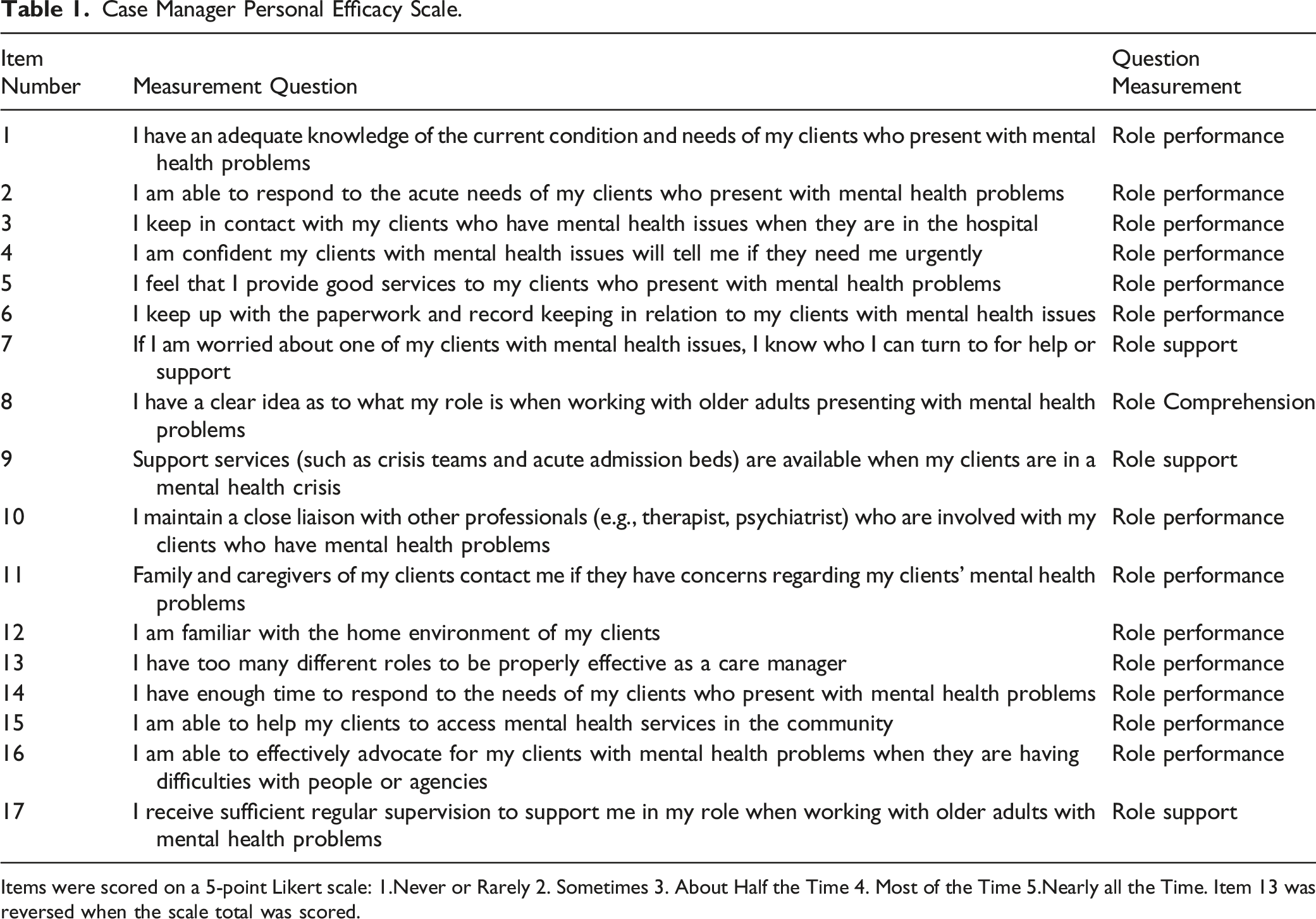
Items were scored on a 5-point Likert scale: 1.Never or Rarely 2. Sometimes 3. About Half the Time 4. Most of the Time 5.Nearly all the Time. Item 13 was reversed when the scale total was scored.
Data Analysis
Data analysis was conducted using the Statistical Package for the Social Sciences [SPSS] (Field, 2013). A dependent sample t-test was conducted to test if mean differences in self-efficacy exist between pre-test and post-test. The assumption of normality was examined with a one-sample Shapiro-Wilk test (Wah & Razali, 2011). The paired samples t-test also assumed homogeneity of variances on the difference between pre-test and post-test. To test this assumption, a Levene’s test for equality of variance was conducted (Levene, 1960). To examine aim 2, an independent sample t-test was conducted to assess if differences in perceived self-efficacy exist among participants who had previous behavioral health training. A Power Analysis for a paired sample t-test was conducted in G*Power to determine a sufficient sample size using an alpha of 0.05, a power of 0.80, a medium effect size (dz = 0.5), and two tails (Faul et al., 2013). Based on the aforementioned assumptions, the desired sample size was 83.
Results
Sociodemographic Characteristics of the Participants (N = 90).
Mean Self-Efficacy Scores From Pre to Post-Test Among Participants Who Work With Older Adults With Mental Health and Substance Use Problems.

Differences in Mean Self-Efficacy Scores for Participants With Previous Mental Health Certification.

Differences in Mean Self-Efficacy Scores for Participants With a Previous Mental Health Course.

Differences in Mean Self-Efficacy Scores for Participants With Previous Substance Use Certification.

Differences in Mean Self-Efficacy Scores for Participants With Previous Substance Use Course.

We found no statistically significant difference in self-efficacy scores between participants with previous mental health certification compared to those with no previous mental health certification t (53) = −0.231, p = .818.
We found no statistically significant difference in the self-efficacy score for participants working with older adults who presented with mental health between participants who had previous mental health certification t (53) = −0.231, p = .818 as displayed in Table 4, and between participants who had taken a previous mental health course and those who had not t (45) = 1.197, p = .237 as displayed in Table 5.
Similarly, there was no statistically significant difference in the self-efficacy scores between participants who had a previous certification in substance use disorder compared to those who had not t (38.6) = 1.397, p = .171 as displayed in Table 6.
However, we found a statistically significant difference in the self-efficacy score for participants who work with older adults who presented substance use compared to participants who had a previous course in substance use disorder relative to those who had not (t (51) = 2.03, p = .048) as displayed in Table 7. These results suggest that participants with a previous course in substance use disorder during their undergraduate or graduate education (M = 67.43, SD = 9.54) reported significantly higher self-efficacy scores than participants who had not (M = 59.30, SD = 9.90).
Discussion
The purpose of the study was to determine the extent to which participation in a training intervention on behavioral health increases the perceived self-efficacy of care managers working with older adults with behavioral health needs to intervene and provide support.
Results of this study provide evidence that BU CADER’s online Mental Health in Aging course positively influenced the perceived self-efficacy of care managers working with older adults. Specifically, we found a significant difference in the mean self-efficacy score at the post-test compared with the pre-test. The findings from this study have important implications for the role of care managers and the provision of mental health services for older adults. The demand for behavioral health services for older adults is estimated to increase in the future. At the same time, the supply of trained providers is insufficient to meet the projected demand (Flaherty & Bartels, 2019; Satiani et al., 2018). Care manager may be able to help meet the demand for mental health services for older adults living in the community. In addition, the findings highlight the importance of blended training that offers both in-person and virtual platforms and allows for opportunities for vicarious learning, which is a strong predictor of self-efficacy (Bandura, 1986). These results also align with Mencl et al. (2012), who noted that successful performance increases self-efficacy, enhancing the learning and performance of new skills and leading to further efficacy and an increase in confidence.
The results of the second research aim indicated that at baseline (pre-test) and after the training (post-test), there was no difference in the self-efficacy scores of those participants who had previously completed a previous mental health course or certification relative to those who had not. Most prior research related to earlier training experiences focused on past performance. This work might help explain why there were no significant differences in the self-efficacy scores of participants with and without previous mental health training. Although self-efficacy plays a role in training (Bandura, 1986; Salas et al., 2012), past performance, as opposed to training, is considered a strong predictor of self-efficacy (Bandura, 1986, 2006). Hence, the need for blended trainings like the BU CADER training that focuses on modeling and immediate feedback. Data on training has shown that a blended instructional methodology can increase self-efficacy and job performance (Dziuba et al., 2004; McPherson & Barnett, 2006; Vermillion, 2019) by allowing learners to apply the concepts learned in the classroom to real-world scenarios (Kenney & Newcombe, 2011). Blended learning is defined as a hybrid of in-person and online learning that includes the conveniences of online courses without the complete loss of face-to-face instruction (Roval & Jordan, 2004). To our knowledge, no other training has utilized a blended training to study the effectiveness of this modality in increasing perceived self-efficacy of care managers working in the aging network.
To help meet the growing need for behavioral health services among older adults, care managers can play a critical role in shaping older adults' behavioral health service delivery trajectory. However, e-training will be essential to help them develop the self-efficacy necessary to provide supportive mental health services. Though BU CADER’s Mental Health in Aging online course was designed to increase knowledge, skills, and values in key practice areas with older adults, the blended learning model of the training may have allowed for vicarious experiences and enacted mastery, both of which have been shown to increase self-efficacy (Mathieu et al., 1993; Sullivan & Mahalik, 2000). Similarly, targeted training interventions have previously been found to improve self-efficacy in nurses (Moon & Hyun, 2019; Crawford, 2021) and other health care providers (Mickan et al., 2019; Tsuei, 2017). Care managers who work with older adults represent a valuable workforce within the aging network, and can help meet the critical needs of older adults living in the community. This study makes significant contributions regarding the impact of training to increase self-efficacy as such; continuous training is necessary, and employers cannot rely on past training or coursework. Instead, staff have to be provided with experiential training opportunities that allow them to use keep using the skills on the job.
Study Limitations
The main limitation of the present study is the quasi-experimental design. A lack of comparison group and randomization could contribute to insufficient control of important confounding variables (Shadish et al., 2002). Additionally, any changes observed in the outcome might be due to factors other than the intervention, that is, participants’ previous experience, other trainings related to mental health and substance at the time of intervention or having a good supervisor. In addition, researchers have suggested that participants report positive feedback after attending a training, hence self-report measurement could impact the post-survey results (Little et al., 2020). As such, future studies should include a control group and assess the effectiveness of the BU CADER’s training course in relation to another training course or conduct a within-subject withdrawal design which would increase the validity of the study.
Much of the prior research has focused on care managers and the delivery of social services. However, as the care manager role evolves, this will lead to a demand for confident care managers who are competent in working with older adults with behavioral health issues; therefore, further research is required to help determine how this critical workforce can overcome the current gaps in behavioral health service delivery.
Another limitation of this study concerns the sampling frame. The study was conducted at one of 25 Aging Services Access Points (ASAP) in Massachusetts, and results might not be generalizable to care managers in other ASAPs throughout Massachusetts and beyond.
Conclusion
To our knowledge, this is the first study to evaluate the effectiveness of the BU CADER training on increasing self-efficacy in care managers working in the aging networks. This study begins to fill a gap in research related to training as an intervention to improve behavioral health services among older adults. We found that the BU CADER training course increased the mean self-efficacy score among care managers working with older adults with mental health and substance use problems. The training could be delivered to providers in the aging network who are already working with the older adult population. As the study revealed, past certification or courses in mental health was not a predictor of higher perceived self-efficacy, which suggests that even newly employed staff with previous training may benefit from the course. To ensure sustainability, the training course should be made available to all care managers within the aging network and part of new hires orientation training.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board
Approval for this study was obtained by the Simmons University’s Institutional Review Board. IRB number 21-027.
HIPAA
Consent was obtained from all participants and personal information was deidentified.