
Abstract
Literature on the association between ageism and falling among older adults is limited. Using data from the nationwide cross-sectional SABE (Salud, Bienestar y Envejecimiento) Colombia Survey in 2015 with 18,875 participants aged ≥60 years living in the communities, the study aims to evaluate the association between perceived ageism within the family, neighborhood, health services, and public services, and recurrent falling. Participants had a mean age of 69.2 ± 7.1; 56.1% were female. Recurrent falling prevalence was 15%, and experiencing any ageism was 10%. Multivariable logistic regression analyses showed higher odds of recurrent falling for any ageism (OR = 1.81, 95% CI 1.61–2.02, p < .0001). High depressive symptoms mediated 10.1% of the association between any ageism and recurrent falling, followed by low instrumental activities of daily living (9.7%) and multimorbidity (9.3%). Current findings open new areas of gerontological research by expanding the risk factors for falling among older adults to include ageism perceptions.
• Perceived ageism is associated with common intrinsic risk factors for falling. • Perceived ageism is independently associated with recurrent falling. • High depressive symptoms, low instrumental activities of daily living, and multimorbidity mediate the relationship between ageism and falls.
• Early management of ageism at various levels might help to prevent falls. • Ageism represents a form of the stigma-discrimination complex affecting physical and psychological health among older adults. • Future research is necessary on why certain types of ageism are related to a higher risk of falls.What this paper adds
Applications of study findings
Introduction
Ageism is defined as “a process of systematic stereotyping and discrimination against people because they are old” (Butler, 1975). Discrimination is an expression of oppression where a “dominant group benefits from systematic abuse, exploitation and injustice directed toward a subordinate group” (Johnson & Johnson, 2000), as are stigma and prejudice (Pascoe & Smart Richman, 2009). Stigma refers to when a negative and inferior response, such as negative attitudes (prejudice) or behaviors (discrimination), is generated toward personnel with particular characteristics (Sibley & Barlow, 2017); this has also been called stigma-discrimination complex (Campo-Arias & Herazo, 2015) or stigma complex (Pescosolido & Martin, 2015). Ageism can act both consciously and unconsciously, and includes three dimensions: cognitive (e.g., stereotypes), affective (e.g., prejudice), and behavioral dimension (e.g., discrimination). It can be expressed at the individual, social, institutional, and cultural levels (Marques et al., 2020), and target others or oneself through self-stigma (Ayalon & Tesch-Römer, 2017). Ageism will gain importance due to its impact on physical, mental, and social well-being, especially among disadvantaged groups (WHO, 2021).
Falls are a geriatric syndrome par excellence due to their high prevalence, multifactorial etiology, and high risk of disability and mortality (Formiga, 2009). Falls are the leading cause of unintentional injury worldwide (Reyes-Ortiz et al., 2020), and since the frequency of falls increases with age and frailty, about one-third of older adults fall annually in the community (Reyes-Ortiz et al., 2005; WHO, 2007). Currently, there is more awareness and efforts to reduce the risk of falls among older people; however, most are aimed at improving intrinsic factors such as balance, equilibrium, gait, and medications, and extrinsic factors such as reducing environmental risk factors (Guirguis-Blake et al., 2018; WHO, 2007). Despite these efforts, there is evidence that deaths from falls have increased by 30% in the last decade (Castle, 2019).
Ageism in the form of a stigma-discrimination complex is a chronic stressor that can contribute to poor mental and physical health outcomes in older adults (Burnes et al., 2019; Chen & Yang, 2014; Han & Richardson, 2015; Lee & Bierman, 2019; Pearlin, 1989; Reyes-Ortiz et al., 2023; Shippee et al., 2019; Stokes, 2019). The stress process model proposes multiple interrelated pathways by which ageism affects mental and physical well-being: 1) Self-esteem, 2) loneliness, and 3) physical health. Experiences of ageism may create perceptions of diminished value as community members, negatively impacting self-esteem and perceived worth and status as an individual. Therefore, ageism may affect mental health with frequent relapses (Shippee et al., 2019; Stokes, 2019), and accentuate feelings of loneliness and isolation familiar with growing older. Consequently, poor mental health undermines physical health through deleterious health behaviors and inadvertent distractions or neglect of self-care that increase the risk of falling.
Castle (2019) proposed that ageism can influence poor self-awareness of the risk of falls or postural control. However, no studies show falling episodes associated directly with ageism. In one study, ageism was associated with self-reported frailty (Zora et al., 2022). By contrast, satisfaction with aging was found to be a possible protective mechanism against falls (Ayalon, 2016).
Thus, we hypothesized that perceived age discrimination (ageism) would be associated with falling and explained in three ways. First, ageism may affect mental and physical health in older adults, making them frail (Zora et al., 2022), and would be associated with common risk factors for falling such as higher depressive symptoms, multimorbidity, poor memory, or poor functional status (Jehu et al., 2021; Li et al., 2023). Second, ageism as a stigma-discrimination complex and chronic stressor may make an older adult susceptible to falling independently from usual fall risk factors and other potential confounding factors (Castle, 2019). Third, common risk factors for falling might mediate the relationship between ageism and recurrent falling. Since 2.5 million Colombians are aged 65 and older, and life expectancy is increasing (Gómez et al., 2009), the study aimed to evaluate the association between ageism and falls among older adults in Colombia.
Methods
Setting
This is a secondary analysis of anonymous data from the SABE (Salud, Bienestar y Envejecimiento) Colombia Study: a 2015 cross-sectional survey assessing the health, aging, and well-being of community-dwelling older adults in urban and rural areas across the country of Colombia. Participants provided written informed consent in the original study (Gomez et al., 2016).
Design
Sampling was developed using a multistage random cluster sampling technique with stratification of the units, and details are provided elsewhere (Gomez et al., 2016). The survey was administrated orally and face-to-face in Spanish. Participants were included if they were 60 years of age or older, could communicate with the research team, and provided written informed consent. Individuals were identified at the beginning of the interview if they had a total score <13 in the Mini-Mental State Examination (MMSE; Folstein et al., 1975). For these individuals with moderate to severe cognitive impairment, a proxy interview was performed. Participants with responses by proxies (17.5%, n = 4690) were excluded from our current analysis since they were not asked questions about age discrimination; 129 had missing values, resulting in 18,875 older individuals in the sample.
Measures
Outcome
The outcome variable for this study was falling, which was assessed by asking the patient these questions: “Have you fallen in the last 12 months?” A positive response was followed by “How many times have you fallen?” According to the number of falls, binary recurrent falls were defined as ≥2 versus 0–1 falls, using the total sample (Hung et al., 2017). Because recurrent fallers (≥2 falls) are usually frail and at higher risk for morbidity and death (Bartoch et al., 2020; Curran-Groome et al., 2020; Jehu et al., 2021), compared to those with 0–1 falls, we chose recurrent falling for the primary analyses. We also categorized falling as 0, 1 or ≥2 falls for multinomial analyses, using partial samples.
Primary Independent Variable
The leading independent variable was the history of age discrimination or ageism, assessed by the set of 4 questions that were asked of the older person in a separate room if they lived with someone: Have you felt unfair treatment for being an older adult or for your age by 1) Other people in the neighborhood? 2) Your family? 3) When going to health services? 4) When requesting public services? The answers to each question include never, sometimes, or always. Due to small percentages for the always answer, we dichotomized these answers as “No” (never = 0) versus “Yes” (sometimes or always = 1) and created a variable with any category of the above. We also defined a total score ranging from 0 to 3, with categories of ageism types (neighborhood, family, health services, and public services) as 0 (never), 1, 2, or ≥3. An additional age discrimination question from the survey was taken from the scale reasons for everyday discrimination and modified from the Williams et al. (1997) and Krieger et al. (2005) discrimination scales: Have you felt everyday rejected or discriminated against because of your age? Named everyday ageism: No (= 0) or Yes (= 1).
Covariates
Sociodemographic variables included age (years), gender (male or female), marital status (married or unmarried), and socioeconomic status (1 = low/low, 2 = low, 3 = medium-low, 4 = medium, and 5 = medium/high and high).
Poor vision was defined as when a person reported having regular, bad, or very bad (vs. good or very good) with either near or far vision regardless of glasses use. Depressive symptoms were measured by the geriatric depression scale (GDS; scores from 0 to 15; high depressive symptoms were defined as ≥6) (Yesavage et al., 1982). This scale has shown high reliability with an internal consistency of α = .78 in older Colombians (Gómez-Angulo & Campo-Arias, 2011) as well in this study, α = .66. Cognitive function was assessed by self-rated memory (excellent, very good, good, fair, or poor) and was dichotomized as poor (fair and poor categories = 1) and good (other categories = 0). In our sample, self-rated memory was negatively correlated with the MMSE (r = −.15). We used self-rated memory instead of the MMSE since the discrimination questions were not asked for participants with MMSE scores<13. Psychotropic medications were defined as using sleeping medications, tranquilizers, or sedatives.
Functional status was evaluated using a Lawton scale for Instrumental Activities of Daily Living (IADL) (Lawton & Brody, 1969). The Lawton scale includes six activities (using the telephone, taking medications, managing finances, preparing meals, shopping, and using transportation), and the score ranges from 0 to 6, with higher scores signifying higher functional status. Low IADL was defined as ≤5.
Medical conditions assessed include hypertension, diabetes, coronary heart disease, arthritis, stroke, chronic pulmonary obstructive disease, or non-skin cancer. Respondents were asked: “Has a doctor or a nurse told you that you have…?” for each previously listed condition. These conditions were counted from 0 to 7. Multimorbidity was defined as having ≥2 medical conditions (code = 1) versus 0–1 (code = 0). Low walking speed was defined as <.8 m/sec.
Statistical Analysis
Distribution of Participants Characteristics, SABE Colombia Study 2015.
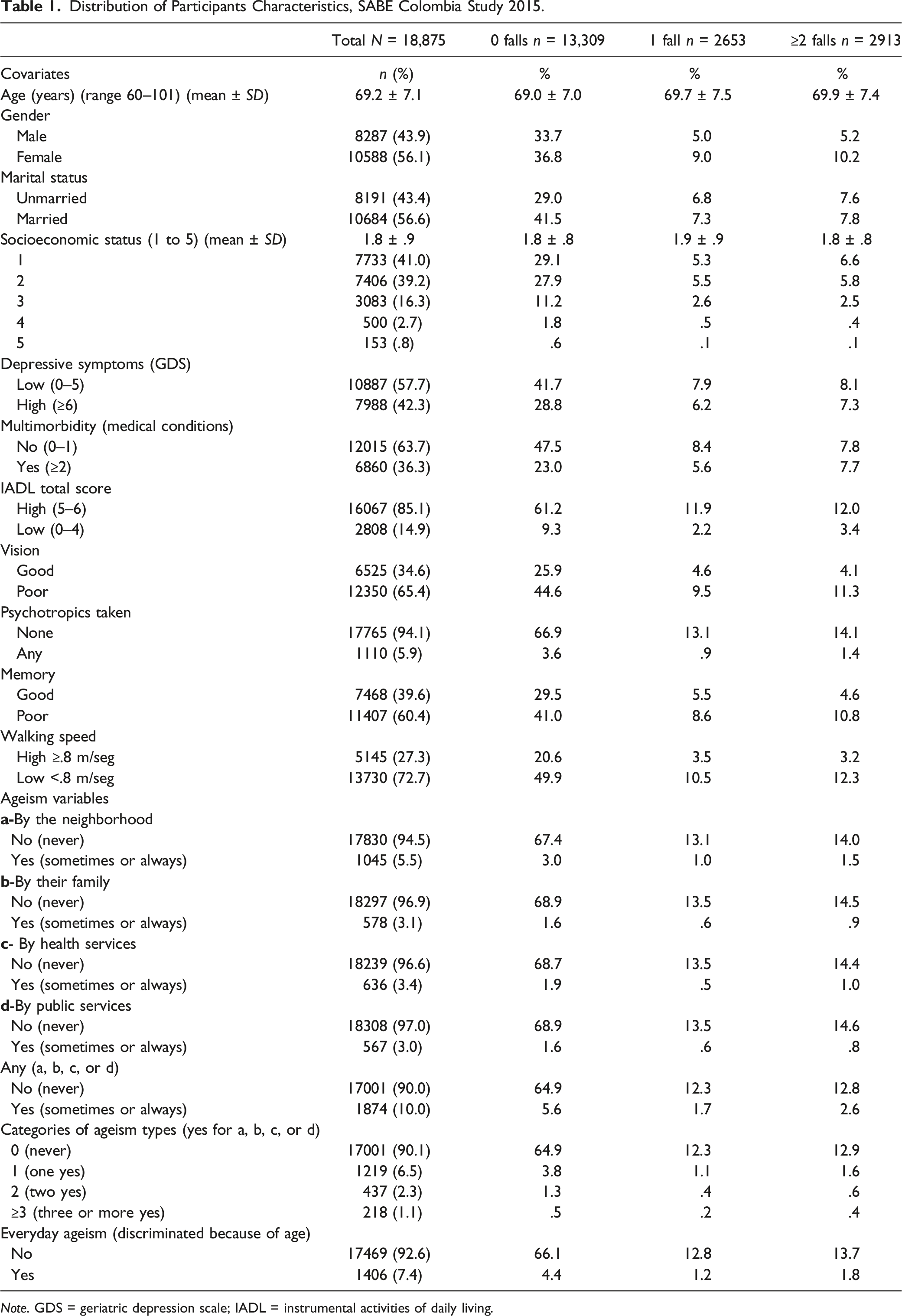
Note. GDS = geriatric depression scale; IADL = instrumental activities of daily living.
Bivariate Logistic Regression Analyses, Associations of Recurrent Falling and Ageism With Other Variables.
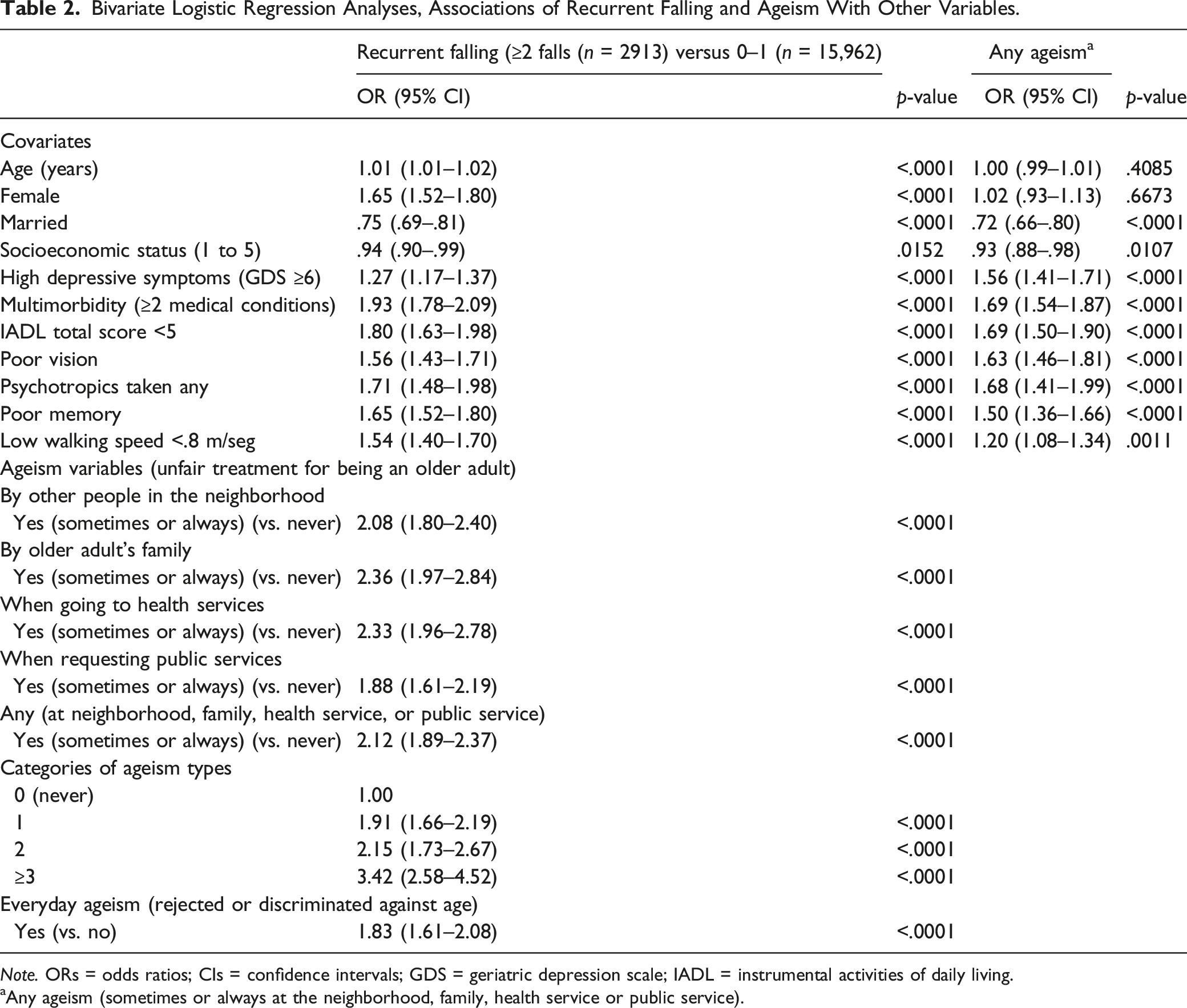
Note. ORs = odds ratios; CIs = confidence intervals; GDS = geriatric depression scale; IADL = instrumental activities of daily living.
aAny ageism (sometimes or always at the neighborhood, family, health service or public service).
Logistic Regression Analyses for Any Ageism Predicting Falls.
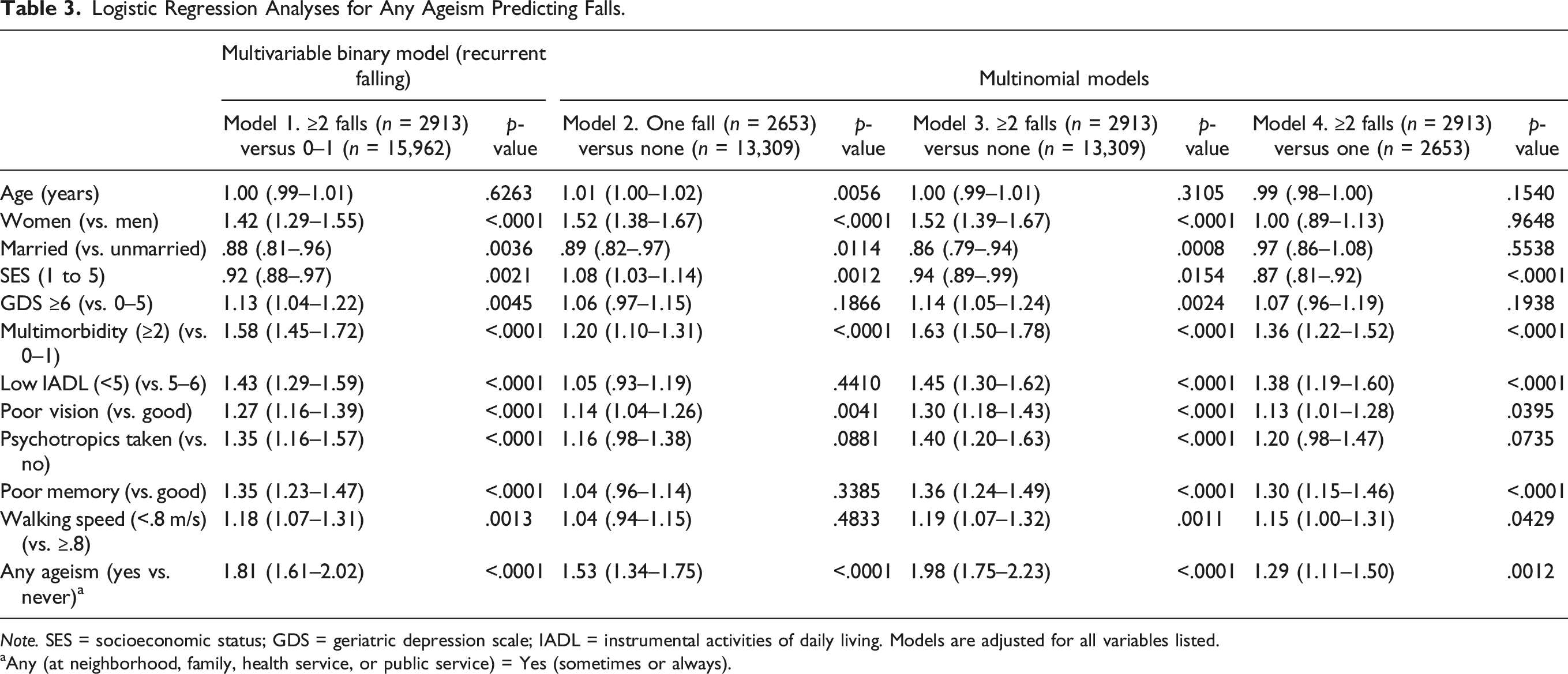
Note. SES = socioeconomic status; GDS = geriatric depression scale; IADL = instrumental activities of daily living. Models are adjusted for all variables listed.
aAny (at neighborhood, family, health service, or public service) = Yes (sometimes or always).
Multivariable Logistic Regression Analyses for Ageism Types Categories and Everyday Ageism Predicting Falls.
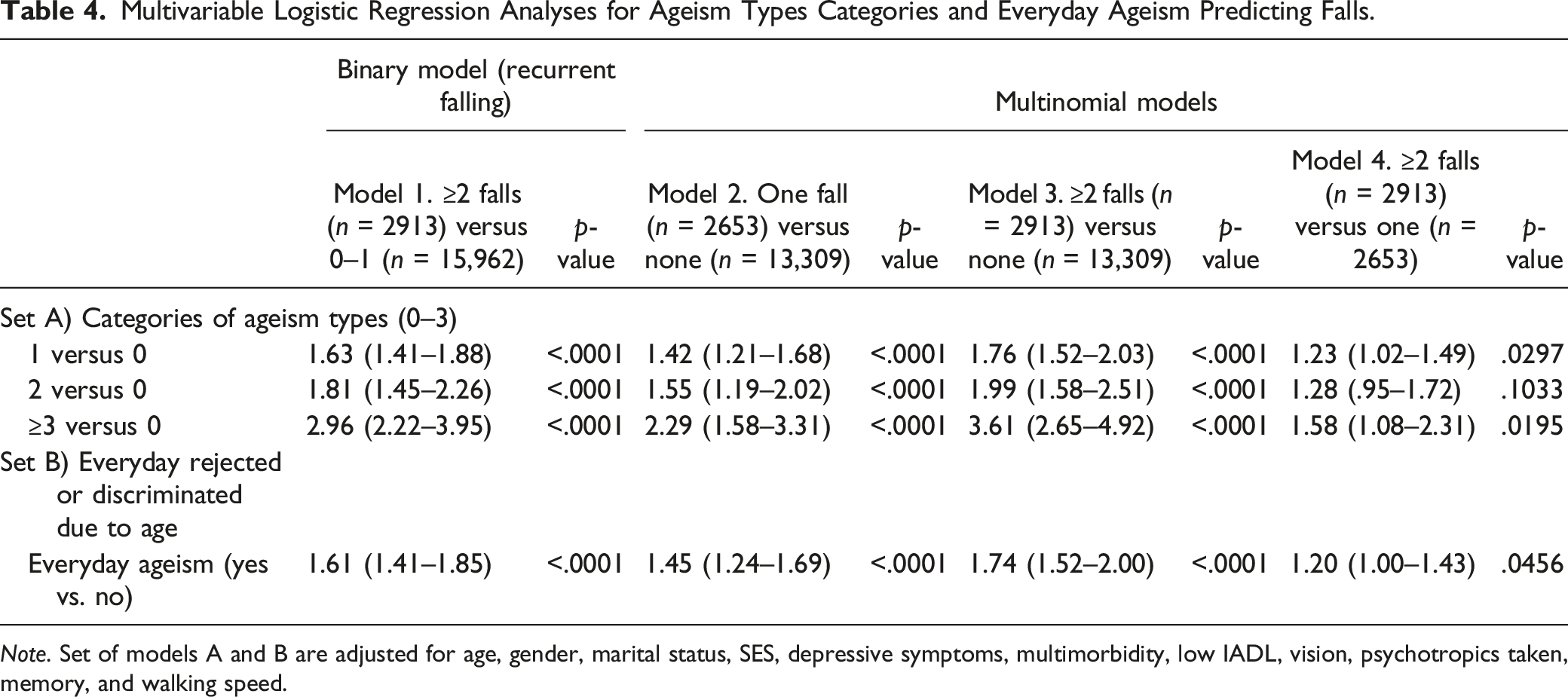
Note. Set of models A and B are adjusted for age, gender, marital status, SES, depressive symptoms, multimorbidity, low IADL, vision, psychotropics taken, memory, and walking speed.
Mediating Variables in the Association Between Any Ageism and Recurrent Falling. a
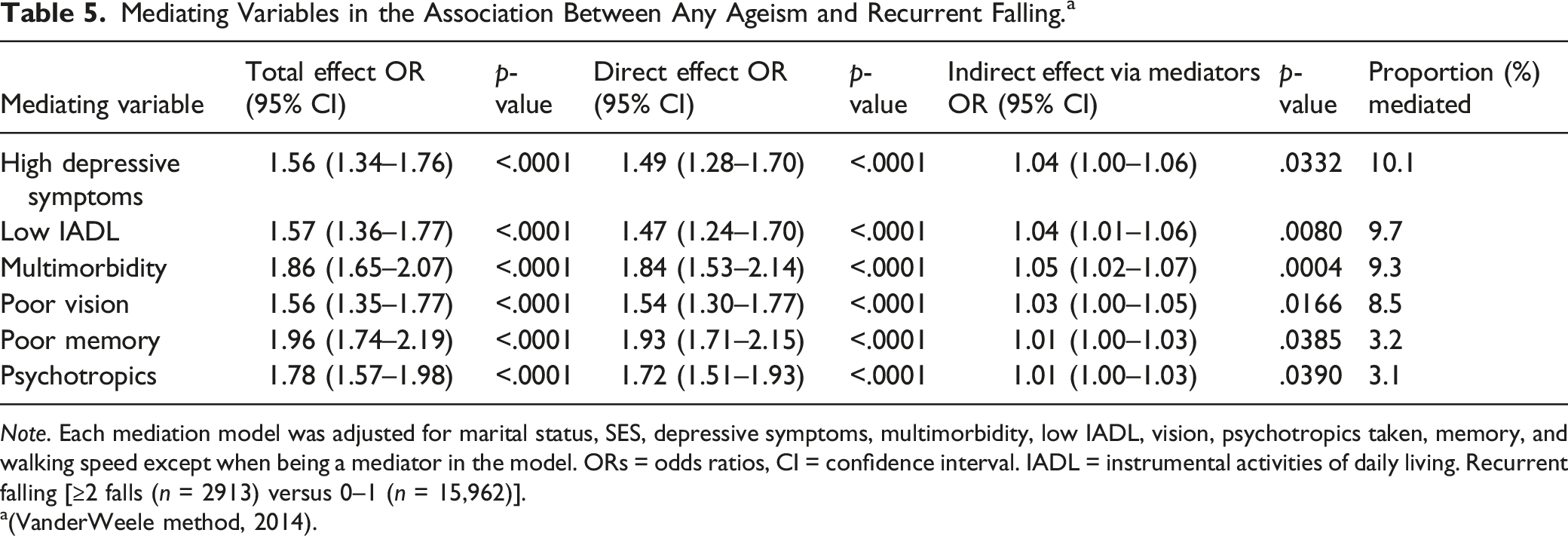
Note. Each mediation model was adjusted for marital status, SES, depressive symptoms, multimorbidity, low IADL, vision, psychotropics taken, memory, and walking speed except when being a mediator in the model. ORs = odds ratios, CI = confidence interval. IADL = instrumental activities of daily living. Recurrent falling [≥2 falls (n = 2913) versus 0–1 (n = 15,962)].
Results
Study participants were between 60 and 101 years old (mean = 69.3 ± 7.2), and 56.1% were female. Ten percent of participants have experienced any ageism perception in the neighborhood, family, health service, or public service. Fourteen percent (n = 2653) had fallen once, and 15.4% (n = 2913) fell twice or more during the previous year (Table 1).
In bivariate logistic regression analyses (Table 2), variables consistently associated with higher odds for recurrent falling were ageism variables and covariates such as female gender, high depressive symptoms, multimorbidity, poor vision, poor memory, low IADL score, low walking speed, and psychotropics use. By contrast, being married and having higher socioeconomic status (SES) were associated with lower odds of recurrent falling. Classical risk factors for falling were associated with increased odds for any ageism measure; these include high depressive symptoms, multimorbidity, low IADL score, poor vision, psychotropics use, poor memory, and low walking speed. By contrast, being married and having a higher SES were associated with lower odds for any ageism.
Multivariable binary logistic regression analyses showed that recurrent falling (≥2 falls vs. 0–1) was significantly associated with: 1) Table 3, Model 1, any ageism (Model 1, OR = 1.81, 95% CI 1.61–2.02); 2) Table 4, Model 1, set A, having 1 type of ageism, 2 types or ≥3 types of ageism versus none (Model 2, OR = 1.63, 95% CI 1.41–1.88; OR = 1.81 95% CI 1.45–2.26; OR = 2.96 95% CI 2.22–3.95, respectively); and 3) Table 4, Model 1, set B, everyday ageism (Model 3, OR = 1.61, 95% CI 1.41–1.85). In addition, female gender, high depressive symptoms, multimorbidity, low IADL score, low walking speed, poor vision, and poor memory were also independently associated with higher odds of recurrent falling. Higher SES and being married were associated with lower odds of recurrent falling. In Table 4, Model 1, set A, when increasing the number of types of ageism (1, 2, or ≥3 compared to 0) increases the odds for recurrent falling (OR = 1.63; OR = 1.81; and OR = 2.96, respectively). In Table 4, Model 1 set B, everyday ageism was also associated with increased odds for recurrent falling (OR = 1.61).
In multinomial logistic regression analyses in Table 3 showed that falls (Model 2: one vs. none, Model 3: ≥2 falls vs. none, and Model 4: ≥2 falls vs. one) were also associated with any ageism (OR = 1.53; OR = 1.98; and OR 1.29, respectively). In addition, in Table 4, Model 1 set A, increasing the number of types of ageism (1, 2 or ≥3 compared to 0) increases the odds for falls (especially in Models 2 [OR = 1.42; OR = 1.55; and OR = 2.29], and 3 [OR = 1.76; OR = 1.99; and OR = 3.61], respectively). In Table 4, Model 1 set B, everyday ageism was also associated with increased odds for falls (especially in Models 2 [OR = 1.45] and 3 [OR = 1.74]).
The mediation analyses showed that high depressive symptoms explained the most significant proportion of the association between any ageism and recurrent falling (10.1%), followed by low IADL (9.7%), multimorbidity (9.3%), poor vision (8.5%), poor memory (3.2%), and psychotropics (3.1%). Walking speed was not a mediator. In sensitivity analyses, additional mediation analyses, we used ≥2 falls versus 0 as the falling outcome. We found that multimorbidity explained the higher proportion for mediation of the association between any ageism and falling (10.0%), followed by depressive symptoms (9.6%), low IADL (9.4%), poor vision (8.2%), and psychotropics (3.1%).
Discussion
We conducted a secondary analysis of a national cross-sectional study to evaluate the relationship between ageism and falls among older adults. We found that any ageism as a single exposure (ageism perceived by the neighborhood, family of the older adult, health services, or access to public services
Previously, Castle (2019) proposed that ageism, by affecting awareness of fall risk and resistance to behavioral change, may put older adults at a higher risk for falling. As far as we know, the association between ageism and recurrent falling is a new finding in literature. Based on our results and other related literature, this association has several potential explanations.
Our results justify, in part, the stress process model hypothesis, where perceived ageism is equivalent to chronic exposure to psychosocial trauma. Ageism is a stressful process, and some studies have shown that inflammation stress markers partially mediate the relationship between self-perception of aging and longevity (Levy & Bavishi, 2018). Thus, ageism can have negative consequences on a person’s physical and mental well-being (Burnes et al., 2019; Chen & Yang, 2014; Lee & Bierman, 2019; Pearlin, 1989; Shippee et al., 2019; Stokes, 2019), which may be related to poor self-awareness of fall risk. Our findings support those negative physical and mental consequences. Other reasons include embodied cognition and stereotype threat, where stereotypes once focused on “other” older people are now applied and become relevant to oneself (Castle, 2019; Costello & Bloesch, 2017; Levy, 2009); the perceived stress can, therefore, affect balancing dual tasks that require attention such as talking while walking (Castle, 2019; Holtzer et al., 2017; Swift et al., 2017). Additionally, others have found a relationship between chronic exposure to positive stereotypes and an increase in variables related to physical health, such as gait speed (Hausdorff et al., 1999), and even this increase has been comparable with people who participate in programs of rigorous exercise (Alexander, 1996). There is evidence of the relationship between satisfaction with aging as a possible protective mechanism against falls (Ayalon, 2016). All these previous studies agree in part with our results such as the mediation findings. For example, ageism is associated with both high depressive symptoms and recurrent falling, with high depressive symptoms as the mediator; this explains part of the pathway between ageism and recurrent falling. Similarly, it is happening with other mediators such as low IADL score, multimorbidity, poor vision, poor memory, and psychotropic use.
A striking finding was that age discrimination is associated with common risk factors for falls, which at the same time are markers for frailty (Reyes-Ortiz et al., 2022). Since those who experience stigma/discrimination by age are more likely to be frail (Zora et al., 2022), this can explain why their risk of falling increases. Previous studies have linked poor health and dependency with ageism (Pascoe & Smart Richman, 2009), and a recent systematic review concluded that self-directed age discrimination is mainly determined by the health status of older adults (Marques et al., 2020). We consider the explanation of this relationship to be bidirectional; on the one hand, older people with poor health or frailty are more likely to be discriminated against (Mudge & Hubbard, 2018) for reasons such as greater dependency, cost, or complexity in care in health. On the other hand, the fact that older adults being discriminated against due to their age can have harmful effects on health and poor well-being has been widely described in previous studies (Chang et al., 2020). We suggest, based on our findings, that it could even lead to frailty (Zora et al., 2022). By contrast, positive self-perceptions of aging have been associated with better physical performance among older adults (Nilsson et al., 2021).
The scope of the relationship between falling and ageism in Latin America is difficult to establish as evidence from large-scale older adult surveys assessing ageism is limited in these countries. However, previous population-based studies in the city of Bogota, or at the country level in Ecuador and Colombia reported an association between falling and psychological trauma related to a history of abuse (Reyes-Ortiz et al., 2018), polyvictimization (Reyes-Ortiz et al., 2021) or discrimination measures (childhood discrimination, everyday discrimination, and recent situations for discrimination) (Reyes-Ortiz et al., 2022). Similarly to our study, the Ecuador study showed a mediation effect of depressive symptoms on the relationship between polyvictimization (two or more types of abuse) and recurrent falling (Reyes-Ortiz et al., 2021).
This study allows us to have specific data on perceived ageism in Colombia and the Latin America region; being one of the first to provide this information, it is a basis for future studies. The prevalence of perceived ageism in our study is only 10%. Although the reported prevalence of discrimination has varied among the countries of the European Union, our findings were like their average, where 11% of the 62-year-old participants frequently experienced discrimination due to their age (van den Heuvel & van Santvoort, 2011). By contrast, according to the World Value Survey, which included 57 countries, about 60% reported that older adults did not receive the respect they deserved (Inglehart et al., 2014). Also, in England, a survey including persons over 52 years reported that 36.8% of respondents aged 65 and older experienced age discrimination (Rippon et al., 2014). However, we still need to consider underreporting in the perception of ageism in our study (WHO, 2021).
Regarding sociodemographic factors, studies have described that ageism increases with age (Rippon et al., 2014). However, our study found no significant association with this factor. We explain this difference in the first place because we do not rule out reporting bias in our sample, which we believe can be justified by the socially tolerated nature of age discrimination that may exist in countries with lower educational levels and the fact that older adults may minimize the importance of age discrimination (WHO, 2021). Some authors have considered that this may lead to it being overlooked as a form of stigma or discrimination (North & Fiske, 2012). On the other hand, disparities exist between developing or less developed countries compared to certain Western countries like the United States. As developing countries may prioritize economic growth and physical infrastructure, there may be limited resources allotted to social programs to recognize the negative impact of or to address ageism.
In the multivariable analysis, we found an association between recurrent falls and female gender, like the European Union countries’ analysis (van den Heuvel & van Santvoort, 2011). Other studies have also reported similar findings on how multimorbidity, dependency in instrumental activities, poor health status and functionality reflected in low gait speed, poor vision, and memory were independently associated with recurrent falls (WHO, 2007). Unlike other factors, such as being married and having high SES, which were related to a lower risk of having recurrent falls, data have been reported in previous studies (van den Heuvel & van Santvoort, 2011; Rippon et al., 2014).
Our findings have potential implications in gerontology. One or several types of ageism exposures reflect psychological trauma at a similar level to several types of abuse or lifetime discrimination that may have late health consequences in older adults as recurrent falling that is a marker of frailty (Jehu et al., 2021; Reyes-Ortiz et al., 2018, 2022; Zora et al., 2022). Indeed, the issue is intricated, where ageism, a frequent stigma-discrimination complex, is associated with the fall’s syndrome. From a gerontological perspective, it could merit further attention from those who assess and care for older adults.
This study has some limitations. The study’s cross-sectional nature did not allow us to determine causality or the direction of the relationship. Also, considering that the survey was conducted in Colombia, the impact of ageism may vary compared to other countries due to different cultural perceptions of aging and family structures. In addition, retrospective recall in the data collection may have caused recall bias. However, our study has some strengths. We showed that several types of ageism are associated with falling, a common and complex geriatric syndrome. Our findings support that repetitive ageism episodes throughout a person’s life may have later consequences, such as falling episodes.
Conclusion
Ageism as a single exposure or gradient was independently associated with falling among older adults. Ageism was also related to common risk factors for falling. In addition, several of those risk factors were found to mediate the relationship between ageism and falling. Previous research has not considered perceived ageism experiences as consequential in the pathway to falling. Our findings open new gerontological research areas by expanding the risk factors to ageism exposure and perception that should be considered to understand the risk of falling among older adults. In clinical practice, addressing ageism and acting over potential modifiable mediators such as depressive symptoms, low functional status, and comorbidities may help to decrease the impact of ageism on falling.
Footnotes
Author’s Note
Preliminary findings of this work were presented as a poster/abstract at the Florida Geriatrics Society Annual Meeting on Sept 11-12, 2021 in Marco Island, FL.
Author Contributions
All authors: 1-Made a substantial contribution to the concept and design of the work and interpretation of data; 2- Drafted the article and revised it critically for content; approved the version to be published; and 3 = Have participated sufficiently in the work to take public responsibility for appropriate portions of the content. Dr Reyes-Ortiz acquired and analyzed the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.